Intensive care units Archives - Page 5 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
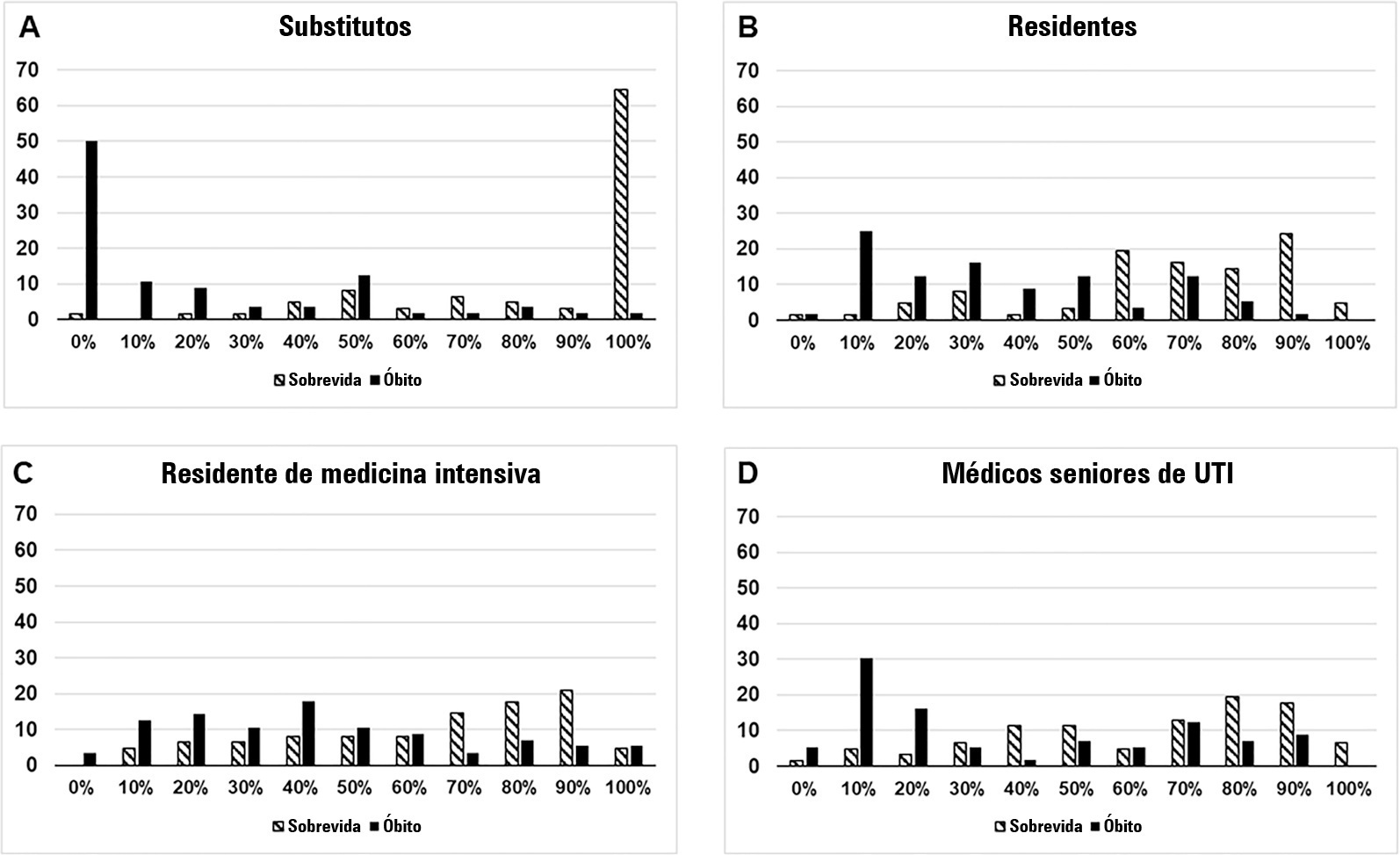
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
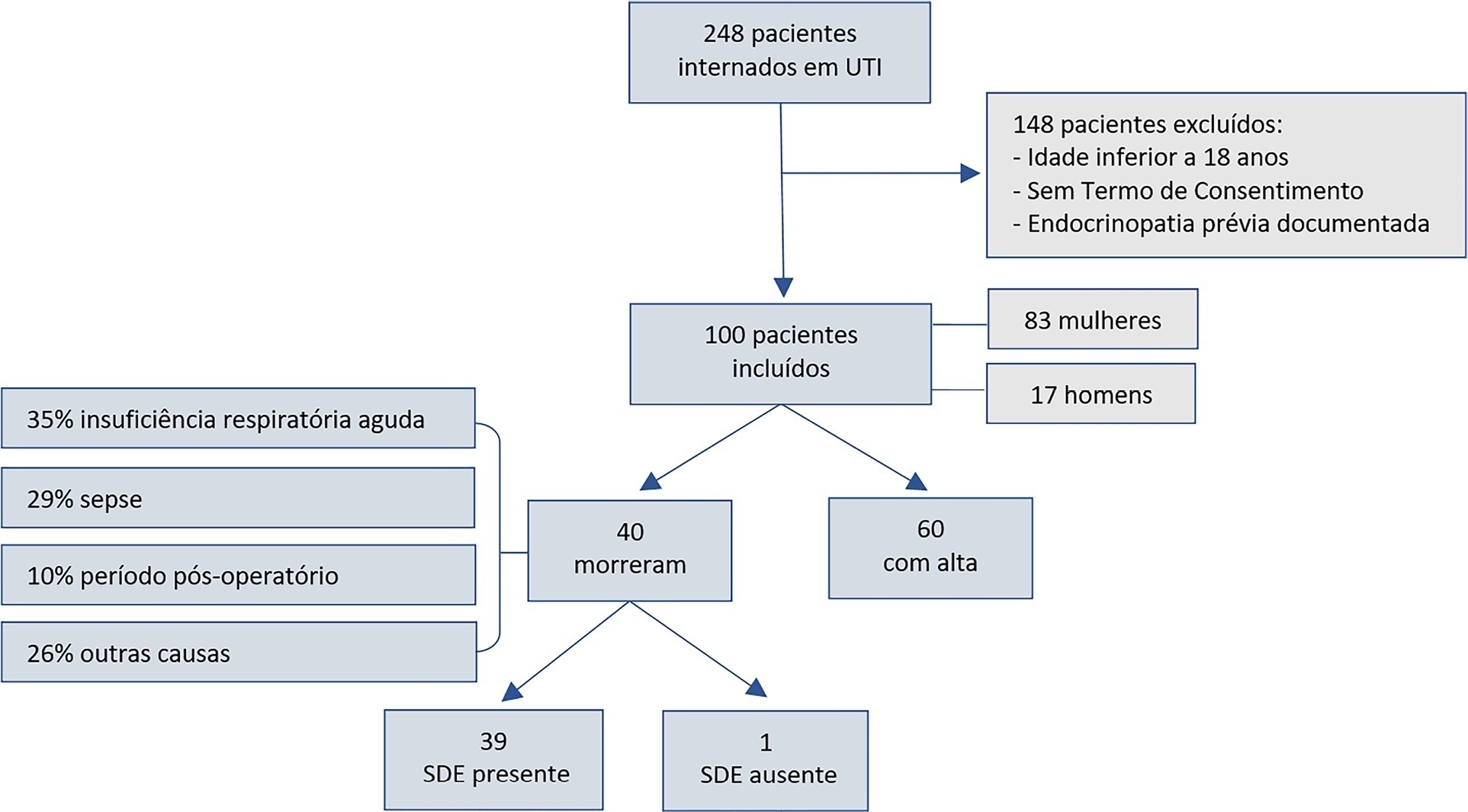
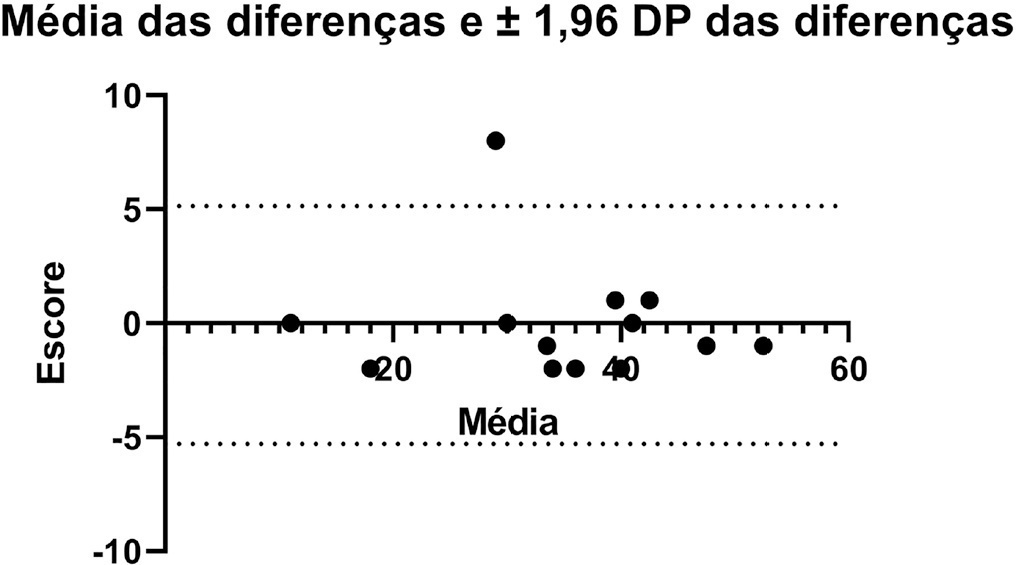
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):262-271
DOI 10.5935/0103-507X.20220024-en
To assess euthyroid sick syndrome as a prognostic factor in patients in the intensive care unit; to detect factors that may affect mortality; and to develop an equation to calculate death probability.
This was a longitudinal, observational, nonconcurrent cohort study developed in the intensive care unit of Fundação Santa Casa de Misericórdia do Pará. One hundred adults with no prior documented endocrinopathy were submitted to a 20mL blood sample collection for the measurement of thyroid stimulating hormone, free tetraiodothyronine, free triiodothyronine and reverse triiodothyronine.
Most patients were female, aged 20 to 29 years. Most patients who died were older (median age of 48 years), and euthyroid sick syndrome was present in 97.5% of them. Euthyroid sick syndrome was related to death, comorbidities, age and length of stay in the intensive care unit (median of 7.5 days).
The main limitation of this study is the fact that it was conducted in a reference hospital for maternal and child care; therefore, there was a greater number of female patients and, consequently, a sampling bias existed. However, opportune measurement of free and reverse triiodothyronine levels in critical patients and application of the proposed equation are suggested.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):295-299
DOI 10.5935/0103-507X.20220028-en
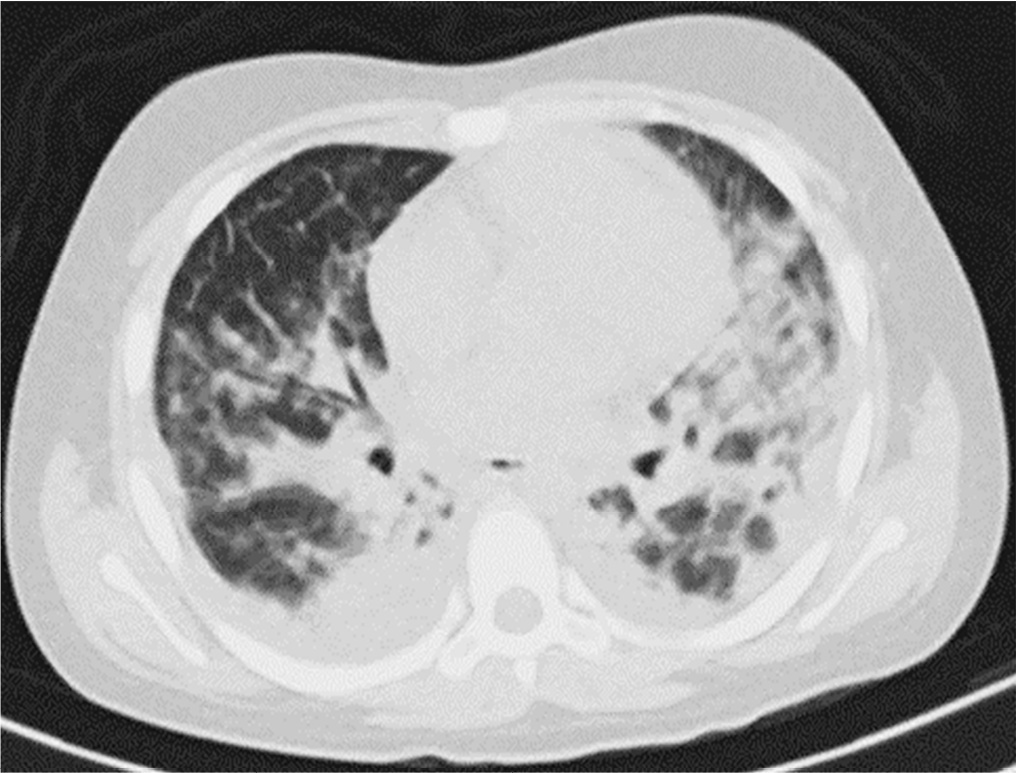
Posterior reversible encephalopathy syndrome is a rare clinical and radiological syndrome characterized by vasogenic edema of the white matter of the occipital and parietal lobes, which are usually symmetrical, resulting from a secondary manifestation of acute dysfunction of the posterior cerebrovascular system. We describe a case of posterior reversible encephalopathy syndrome secondary to SARS-CoV-2 infection in a 9-year-old boy who developed acute hypoxemic respiratory failure and required assisted mechanical ventilation. The child developed multisystem inflammatory syndrome, and he was monitored in the pediatric intensive care unit and was provided mechanical ventilation and vasoactive agents for hemodynamic support. Additionally, he developed pulmonary and extrapulmonary clinical manifestations along with neuropsychiatric manifestations that required close follow-up and were verified using brain magnetic resonance imaging for timely intervention. Currently, there are few reports of children with posterior reversible encephalopathy syndrome associated with multisystem inflammatory syndrome.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):295-299
DOI 10.5935/0103-507X.20220028-en
Posterior reversible encephalopathy syndrome is a rare clinical and radiological syndrome characterized by vasogenic edema of the white matter of the occipital and parietal lobes, which are usually symmetrical, resulting from a secondary manifestation of acute dysfunction of the posterior cerebrovascular system. We describe a case of posterior reversible encephalopathy syndrome secondary to SARS-CoV-2 infection in a 9-year-old boy who developed acute hypoxemic respiratory failure and required assisted mechanical ventilation. The child developed multisystem inflammatory syndrome, and he was monitored in the pediatric intensive care unit and was provided mechanical ventilation and vasoactive agents for hemodynamic support. Additionally, he developed pulmonary and extrapulmonary clinical manifestations along with neuropsychiatric manifestations that required close follow-up and were verified using brain magnetic resonance imaging for timely intervention. Currently, there are few reports of children with posterior reversible encephalopathy syndrome associated with multisystem inflammatory syndrome.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
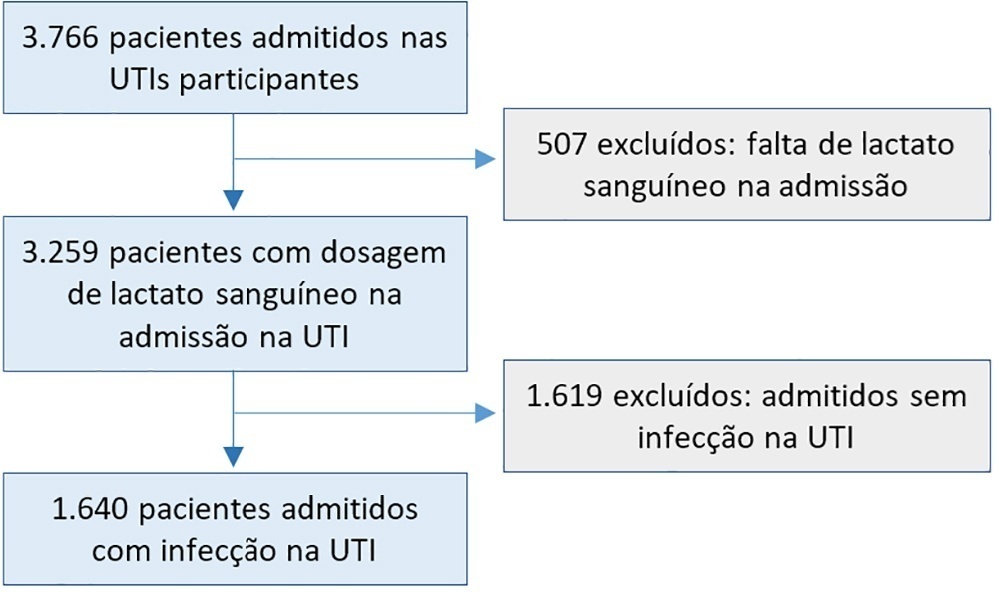
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 - 3.9mmol/L), moderate (4.0 - 9.9mmol/L) or severe (> 10mmol/L).
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 - 0.72), which increased to 0.71 (95%CI 0.68 - 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 - 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):154-162
DOI 10.5935/0103-507X.20220010-en
To evaluate the influence of patient characteristics on hyperlactatemia in an infected population admitted to intensive care units and the influence of hyperlactatemia severity on hospital mortality.
A post hoc analysis of hyperlactatemia in the INFAUCI study, a national prospective, observational, multicenter study, was conducted in 14 Portuguese intensive care units. Infected patients admitted to intensive care units with a lactate measurement in the first 12 hours of admission were selected. Sepsis was identified according to the Sepsis-2 definition accepted at the time of data collection. The severity of hyperlactatemia was classified as mild (2 - 3.9mmol/L), moderate (4.0 - 9.9mmol/L) or severe (> 10mmol/L).
In a total of 1,640 patients infected on admission, hyperlactatemia occurred in 934 patients (57%), classified as mild, moderate and severe in 57.0%, 34.4% and 8.7% of patients, respectively. The presence of hyperlactatemia and a higher degree of hyperlactatemia were both associated with a higher Simplified Acute Physiology Score II, a higher Charlson Comorbidity Index and the presence of septic shock. The lactate Receiver Operating Characteristic curve for hospital mortality had an area under the curve of 0.64 (95%CI 0.61 - 0.72), which increased to 0.71 (95%CI 0.68 - 0.74) when combined with Sequential Organ Failure Assessment score. In-hospital mortality with other covariates adjusted by Simplified Acute Physiology Score II was associated with moderate and severe hyperlactatemia, with odds ratio of 1.95 (95%CI 1.4 - 2.7; p < 0.001) and 4.54 (95%CI 2.4 - 8.5; p < 0.001), respectively.
Blood lactate levels correlate independently with in-hospital mortality for moderate and severe degrees of hyperlactatemia.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 - 1.78] and 1.34 [1.0 - 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 - 154.43] and 47.79 [11.41 - 200.25], respectively); with a p < 0.05 for all results.
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):166-175
DOI 10.5935/0103-507X.20220011-en
To assess whether scales of physical functional performance and the surprise question (“Would I be surprised if this patient died in 6 months?”) predict life support limitations and mortality in critically ill nonsurgical patients.
We included 114 patients admitted from the Emergency Department to an intensive care unit in this prospective cohort. Physical functional performance was assessed by the Palliative Prognostic Score, Karnofsky Performance Status, and the Katz Activities of Daily Living scale. Two intensivists responded to the surprise question.
The proposed physical functional performance scores were significantly lower in patients with life support limitations and those who died during the hospital stay. A negative response to the surprise question was more frequent in the same subset of patients. Adjusted univariable analysis showed an increased odds ratio for life support limitations and death regarding the activities of daily living scale (1.35 [1.01 - 1.78] and 1.34 [1.0 - 1.79], respectively) and a negative response for the surprise question (42.35 [11.62 - 154.43] and 47.79 [11.41 - 200.25], respectively); with a p < 0.05 for all results.
All physical functional performance scales showed lower scores in nonsurvivors and patients with life support limitations. The activities of daily living score and the surprise question increased the odds of life support limitations and mortality in our cohort of nonsurgical intensive care unit patients admitted from the Emergency Department.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
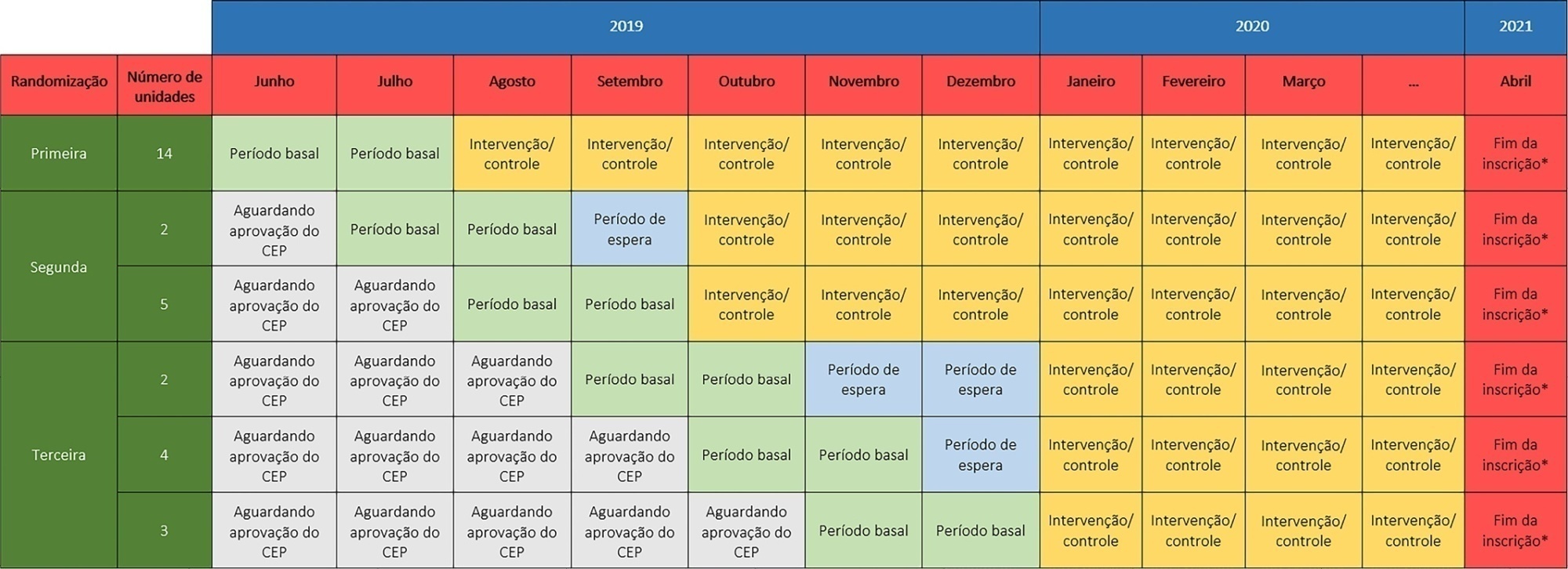
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 - 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 - 3) versus 5 (2 - 24) hours; p < 0.001].
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 - 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 - 3) versus 5 (2 - 24) hours; p < 0.001].
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.