Intensive care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(3):274-283
DOI 10.5935/0103-507X.20150032
To systematically review the main methods for nutritional risk assessment used in critically ill cancer patients and present the methods that better assess risks and predict relevant clinical outcomes in this group of patients, as well as to discuss the pros and cons of these methods according to the current literature.
The study consisted of a systematic review based on analysis of manuscripts retrieved from the PubMed, LILACS and SciELO databases by searching for the key words “nutritional risk assessment”, “critically ill” and “cancer”.
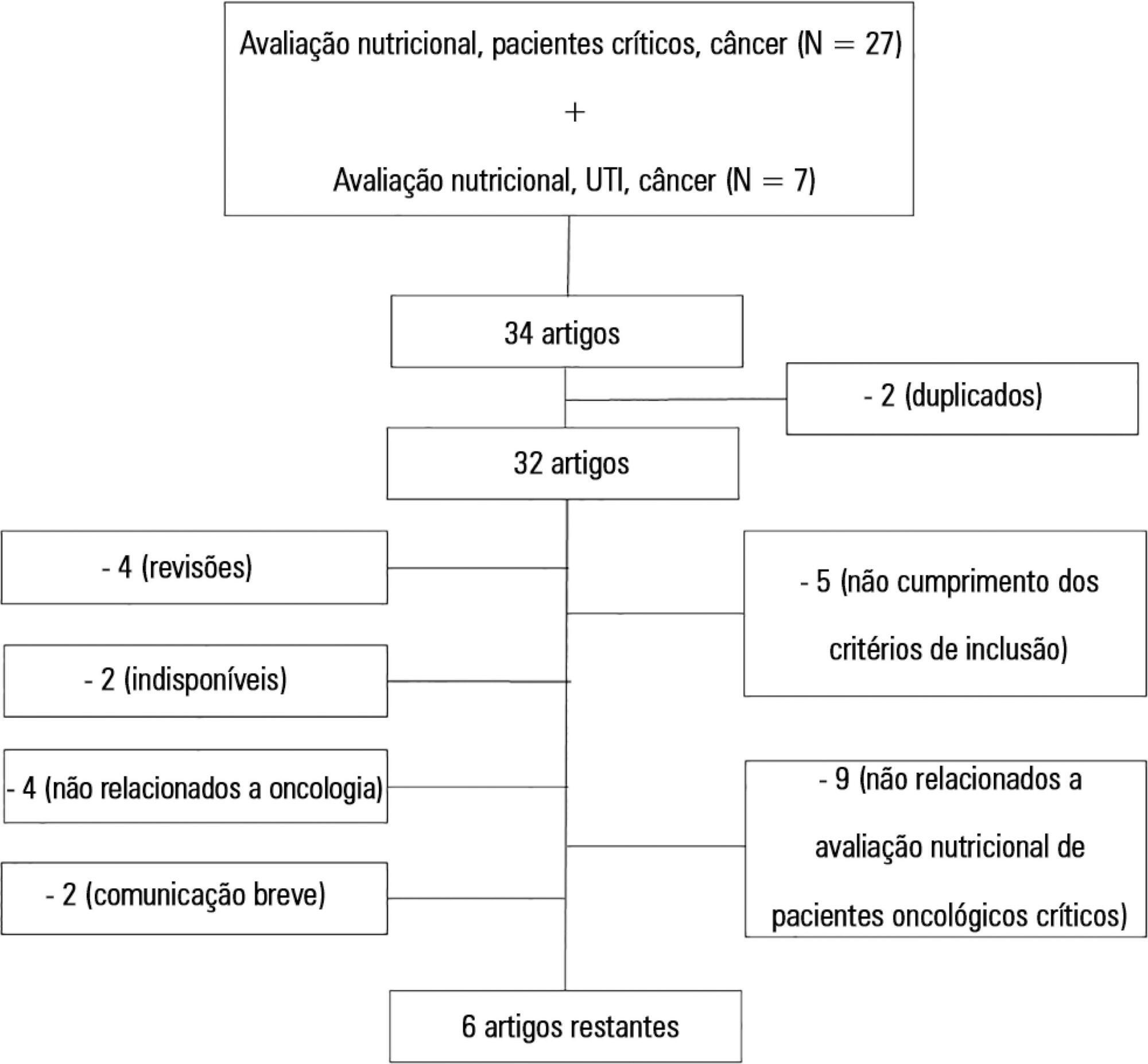
Only 6 (17.7%) of 34 initially retrieved papers met the inclusion criteria and were selected for the review. The main outcomes of these studies were that resting energy expenditure was associated with undernourishment and overfeeding. The high Patient-Generated Subjective Global Assessment score was significantly associated with low food intake, weight loss and malnutrition. In terms of biochemical markers, higher levels of creatinine, albumin and urea were significantly associated with lower mortality. The worst survival was found for patients with worse Eastern Cooperative Oncologic Group - performance status, high Glasgow Prognostic Score, low albumin, high Patient-Generated Subjective Global Assessment score and high alkaline phosphatase levels. Geriatric Nutritional Risk Index values < 87 were significantly associated with mortality. A high Prognostic Inflammatory and Nutritional Index score was associated with abnormal nutritional status in critically ill cancer patients. Among the reviewed studies that examined weight and body mass index alone, no significant clinical outcome was found.
None of the methods reviewed helped to define risk among these patients. Therefore, assessment by a combination of weight loss and serum measurements, preferably in combination with other methods using scores such as Eastern Cooperative Oncologic Group - performance status, Glasgow Prognostic Score and Patient-Generated Subjective Global Assessment, is suggested given that their use is simple, feasible and useful in such cases.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):274-283
DOI 10.5935/0103-507X.20150032
To systematically review the main methods for nutritional risk assessment used in critically ill cancer patients and present the methods that better assess risks and predict relevant clinical outcomes in this group of patients, as well as to discuss the pros and cons of these methods according to the current literature.
The study consisted of a systematic review based on analysis of manuscripts retrieved from the PubMed, LILACS and SciELO databases by searching for the key words “nutritional risk assessment”, “critically ill” and “cancer”.
Only 6 (17.7%) of 34 initially retrieved papers met the inclusion criteria and were selected for the review. The main outcomes of these studies were that resting energy expenditure was associated with undernourishment and overfeeding. The high Patient-Generated Subjective Global Assessment score was significantly associated with low food intake, weight loss and malnutrition. In terms of biochemical markers, higher levels of creatinine, albumin and urea were significantly associated with lower mortality. The worst survival was found for patients with worse Eastern Cooperative Oncologic Group - performance status, high Glasgow Prognostic Score, low albumin, high Patient-Generated Subjective Global Assessment score and high alkaline phosphatase levels. Geriatric Nutritional Risk Index values < 87 were significantly associated with mortality. A high Prognostic Inflammatory and Nutritional Index score was associated with abnormal nutritional status in critically ill cancer patients. Among the reviewed studies that examined weight and body mass index alone, no significant clinical outcome was found.
None of the methods reviewed helped to define risk among these patients. Therefore, assessment by a combination of weight loss and serum measurements, preferably in combination with other methods using scores such as Eastern Cooperative Oncologic Group - performance status, Glasgow Prognostic Score and Patient-Generated Subjective Global Assessment, is suggested given that their use is simple, feasible and useful in such cases.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):376-382
DOI 10.5935/0103-507X.20150063
To evaluate the serum concentrations of vitamin D and their variations in patients with severe sepsis or septic shock and in control subjects upon admission and after 7 days of hospitalization in the intensive care unit and to correlate these concentrations with the severity of organ dysfunction.
This case-control, prospective, observational study involved patients aged > 18 years with severe sepsis or septic shock paired with a control group. Serum vitamin D concentrations were measured at inclusion (D0) and on the seventh day after inclusion (D7). Severe deficiency was defined as vitamin D levels < 10ng/ml, deficiency as levels between 10 and 20ng/ml, insufficiency as levels between 20 and 30ng/ml, and sufficiency as levels ≥ 30ng/mL. We considered a change to a higher ranking, together with a 50% increase in the absolute concentration, to represent an improvement.
We included 51 patients (26 with septic shock and 25 controls). The prevalence of vitamin D concentration ≤ 30ng/ml was 98%. There was no correlation between the serum concentration of vitamin D at D0 and the SOFA score at D0 or D7 either in the general population or in the group with septic shock. Patients with improvement in vitamin D deficiency had an improved SOFA score at D7 (p = 0.013).
In the population studied, patients with septic shock showed improvement in the serum concentrations of vitamin D on the seventh day compared with the controls. We also found a correlation between higher vitamin D concentrations and a greater decrease in the severity of organ dysfunction.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):376-382
DOI 10.5935/0103-507X.20150063
To evaluate the serum concentrations of vitamin D and their variations in patients with severe sepsis or septic shock and in control subjects upon admission and after 7 days of hospitalization in the intensive care unit and to correlate these concentrations with the severity of organ dysfunction.
This case-control, prospective, observational study involved patients aged > 18 years with severe sepsis or septic shock paired with a control group. Serum vitamin D concentrations were measured at inclusion (D0) and on the seventh day after inclusion (D7). Severe deficiency was defined as vitamin D levels < 10ng/ml, deficiency as levels between 10 and 20ng/ml, insufficiency as levels between 20 and 30ng/ml, and sufficiency as levels ≥ 30ng/mL. We considered a change to a higher ranking, together with a 50% increase in the absolute concentration, to represent an improvement.
We included 51 patients (26 with septic shock and 25 controls). The prevalence of vitamin D concentration ≤ 30ng/ml was 98%. There was no correlation between the serum concentration of vitamin D at D0 and the SOFA score at D0 or D7 either in the general population or in the group with septic shock. Patients with improvement in vitamin D deficiency had an improved SOFA score at D7 (p = 0.013).
In the population studied, patients with septic shock showed improvement in the serum concentrations of vitamin D on the seventh day compared with the controls. We also found a correlation between higher vitamin D concentrations and a greater decrease in the severity of organ dysfunction.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):7-13
DOI 10.5935/0103-507X.20140002
To evaluate the role of quality indicators and adverse events registering in the quality assessment of intensive care physiotherapy and to evaluate the impact of implementing protocolized care and professional training in the quality improvement process.
A prospective before-after study was designed to assess 15 indicators of the quality of care. Baseline compliance and adverse events were collected before and after the implementation of treatment protocols and staff training.
Eighty-nine patients admitted, being 48 in the pre-intervention period and 41 in the post-intervention period with a total of 1246 and 1191 observations respectively. Among the indicators related to the global population, there was a significant improvement in chest x-ray control, multidisciplinary rounds and shift changes as well as in compliance with these decisions. Indicators related to the population under mechanical ventilation, obtained by direct observation at bedside, showed a significant improvement in the compliance with the tidal volume of 6-8mL/Kg, plateau pressure <30cmH2O, adequate mechanical ventilation alarm setting, mechanical ventilation humidification control, adequate humidification line exchange and orotracheal tube position. Among the mechanical ventilation indicators collected through the physiotherapy records, there was significantly improved compliance with the predicted tidal volume registry and cuff pressure registry. There was a significant reduction in the number of adverse events. There was no impact on intensive care unit mortality, length of stay, duration of mechanical ventilation and ventilator-free days.
It is possible to measure the quality of physiotherapy care using indicators of quality control. The implementation of care protocols and training of the professionals can improve team performance.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):7-13
DOI 10.5935/0103-507X.20140002
To evaluate the role of quality indicators and adverse events registering in the quality assessment of intensive care physiotherapy and to evaluate the impact of implementing protocolized care and professional training in the quality improvement process.
A prospective before-after study was designed to assess 15 indicators of the quality of care. Baseline compliance and adverse events were collected before and after the implementation of treatment protocols and staff training.
Eighty-nine patients admitted, being 48 in the pre-intervention period and 41 in the post-intervention period with a total of 1246 and 1191 observations respectively. Among the indicators related to the global population, there was a significant improvement in chest x-ray control, multidisciplinary rounds and shift changes as well as in compliance with these decisions. Indicators related to the population under mechanical ventilation, obtained by direct observation at bedside, showed a significant improvement in the compliance with the tidal volume of 6-8mL/Kg, plateau pressure <30cmH2O, adequate mechanical ventilation alarm setting, mechanical ventilation humidification control, adequate humidification line exchange and orotracheal tube position. Among the mechanical ventilation indicators collected through the physiotherapy records, there was significantly improved compliance with the predicted tidal volume registry and cuff pressure registry. There was a significant reduction in the number of adverse events. There was no impact on intensive care unit mortality, length of stay, duration of mechanical ventilation and ventilator-free days.
It is possible to measure the quality of physiotherapy care using indicators of quality control. The implementation of care protocols and training of the professionals can improve team performance.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
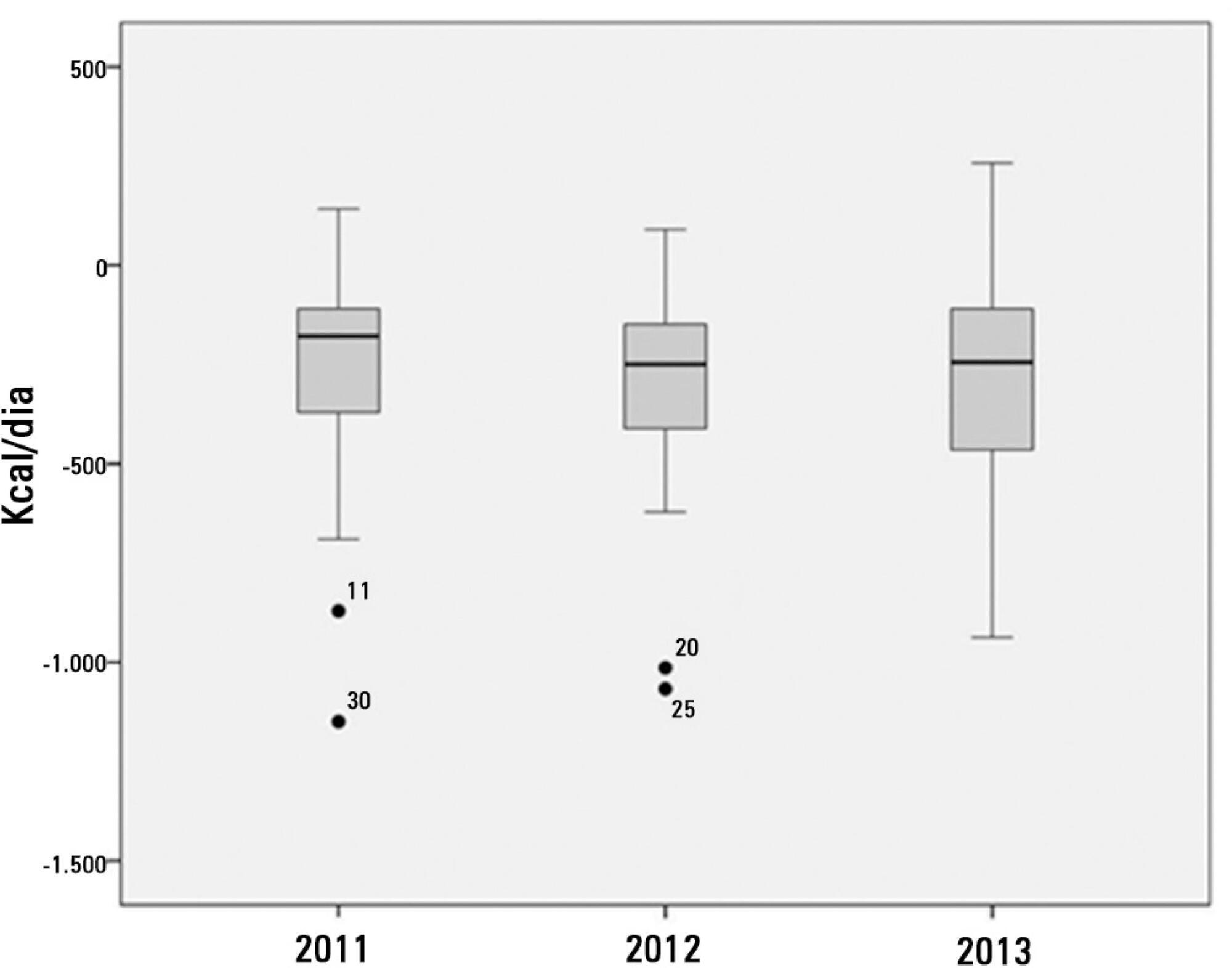
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):106-114
DOI 10.5935/0103-507X.20130021
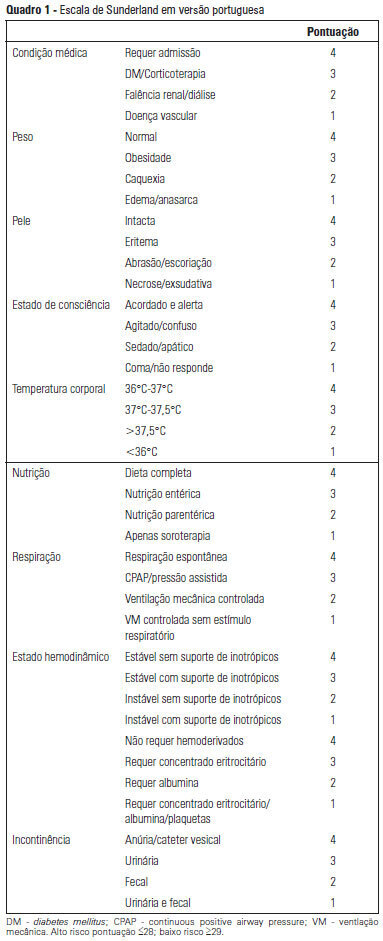
OBJECTIVE: To Translate into Portuguese and evaluate the measuring properties of the Sunderland Scale and the Cubbin & Jackson Revised Scale, which are instruments for evaluating the risk of developing pressure ulcers during intensive care. METHODS: This study included the process of translation and adaptation of the scales to the Portuguese language, as well as the validation of these tools. To assess the reliability, Cronbach alpha values of 0.702 to 0.708 were identified for the Sunderland Scale and the Cubbin & Jackson Revised Scale, respectively. The validation criteria (predictive) were performed comparatively with the Braden Scale (gold standard), and the main measurements evaluated were sensitivity, specificity, positive predictive value, negative predictive value, and area under the curve, which were calculated based on cutoff points. RESULTS: The Sunderland Scale exhibited 60% sensitivity, 86.7% specificity, 47.4% positive predictive value, 91.5% negative predictive value, and 0.86 for the area under the curve. The Cubbin & Jackson Revised Scale exhibited 73.3% sensitivity, 86.7% specificity, 52.4% positive predictive value, 94.2% negative predictive value, and 0.91 for the area under the curve. The Braden scale exhibited 100% sensitivity, 5.3% specificity, 17.4% positive predictive value, 100% negative predictive value, and 0.72 for the area under the curve. CONCLUSIONS: Both tools demonstrated reliability and validity for this sample. The Cubbin & Jackson Revised Scale yielded better predictive values for the development of pressure ulcers during intensive care.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):106-114
DOI 10.5935/0103-507X.20130021
OBJECTIVE: To Translate into Portuguese and evaluate the measuring properties of the Sunderland Scale and the Cubbin & Jackson Revised Scale, which are instruments for evaluating the risk of developing pressure ulcers during intensive care. METHODS: This study included the process of translation and adaptation of the scales to the Portuguese language, as well as the validation of these tools. To assess the reliability, Cronbach alpha values of 0.702 to 0.708 were identified for the Sunderland Scale and the Cubbin & Jackson Revised Scale, respectively. The validation criteria (predictive) were performed comparatively with the Braden Scale (gold standard), and the main measurements evaluated were sensitivity, specificity, positive predictive value, negative predictive value, and area under the curve, which were calculated based on cutoff points. RESULTS: The Sunderland Scale exhibited 60% sensitivity, 86.7% specificity, 47.4% positive predictive value, 91.5% negative predictive value, and 0.86 for the area under the curve. The Cubbin & Jackson Revised Scale exhibited 73.3% sensitivity, 86.7% specificity, 52.4% positive predictive value, 94.2% negative predictive value, and 0.91 for the area under the curve. The Braden scale exhibited 100% sensitivity, 5.3% specificity, 17.4% positive predictive value, 100% negative predictive value, and 0.72 for the area under the curve. CONCLUSIONS: Both tools demonstrated reliability and validity for this sample. The Cubbin & Jackson Revised Scale yielded better predictive values for the development of pressure ulcers during intensive care.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):137-147
DOI 10.5935/0103-507X.20130025
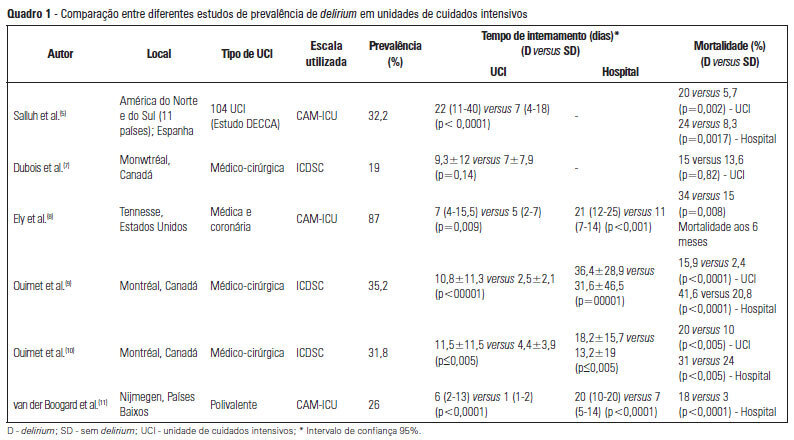
Delirium occurs in up to 80% of patients admitted to intensive care units. Although under-diagnosed, delirium is associated with a significant increase in morbidity and mortality in critical patients. Here, we review the main risk factors, clinical manifestations and preventative and therapeutic approaches (pharmacological and non-pharmacological) for this illness.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):137-147
DOI 10.5935/0103-507X.20130025
Delirium occurs in up to 80% of patients admitted to intensive care units. Although under-diagnosed, delirium is associated with a significant increase in morbidity and mortality in critical patients. Here, we review the main risk factors, clinical manifestations and preventative and therapeutic approaches (pharmacological and non-pharmacological) for this illness.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
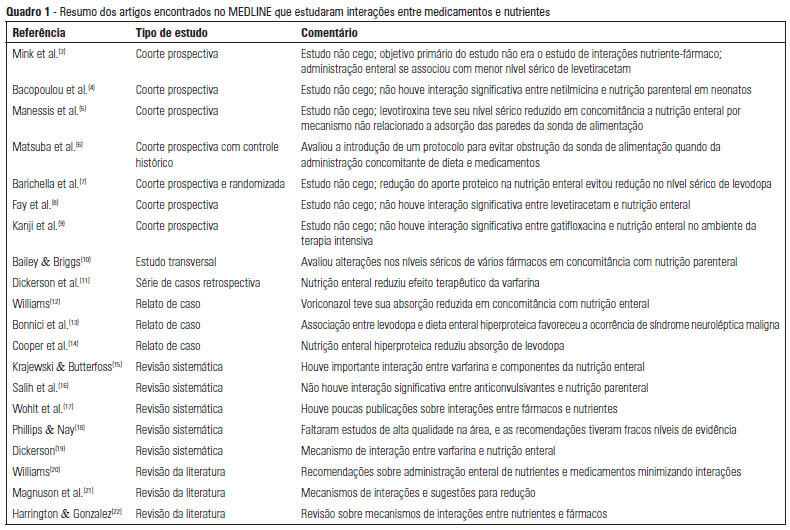
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)