Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Ederlon Rezende"
We found (15) results for your search.Abstract
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Currently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):255-261
DOI 10.1590/S0103-507X2009000300004
Currently, aging of the population is a widespread global phenomenon. Therefore, the assessment of prognosis in elderly patients is needed. This study aims to identify risk factors in a population of elderly patients admitted in the intensive care unit METHODS: A prospective study in the intensive care unit of a general tertiary hospital was carried out for five months. Patients with 65 years or more of age, who stayed in the intensive care unit for 24 hours or more were included and those at the-end-of-life, patients readmitted to intensive care unit during the same hospital stay were excluded. RESULTS: In this study 199 patients were involved, with a mean age of 75.4±6.8 years, and 58.8% were female. Mortality was 57.3%. The mean APACHE II, SOFA, MODS and Katz index (assessment of daily activities) were respectively 20.0±5.8, 6.8±3.9, 2.4±1.9 and 5.3±1.6. Most patients were postoperative 59.3% and 41.6% were under invasive mechanical ventilation. At regression analysis, the independent determinants of higher mortality were: older age (76.9±6.7 years death versus 73.3±6.5 years discharge, P<0.001, OR=1.08, CI 95% 1.01-1. 16), the Katz index (4.9±1.9 deaths versus 5.7±0.9 discharge, p=0.001, OR=0.66, CI 95% 0.45-0.98), hyperglycemia (158.1±69.0 death versus 139.6±48.5 discharge p=0.041; OR=1.02; CI 95% 1.01-1.03) and need for mechanical ventilation at admission to the intensive care unit (57.0% death versus 20.5% discharge p <0.001, OR=3.57, CI 95% 1.24-10.3). CONCLUSION: Elderly patients admitted to the intensive care unit that have difficulties in performing daily activities, hyperglycemia and who are under invasive mechanical ventilation had a worse hospital prognosis.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
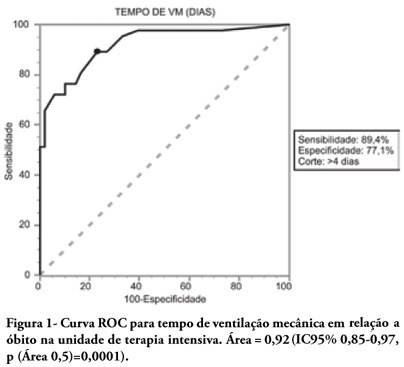
OBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 - patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):262-268
DOI 10.1590/S0103-507X2009000300005
OBJECTIVES: To describe the population of aged as compared to young patients under mechanical ventilation and to analyze the mortality risk factors of this group in an intensive care unit. METHODS: This was a prospective observational trial in patients over 18 years of age, admitted in an intensive care unit and under mechanical ventilation, during one year. Patients were divided into two groups according to age: Group 1 - patients over 65 years old; and Group 2, 65 years old or younger. RESULTS: eighty one mechanic ventilation patients were included, 62 aged and 18 younger, mean ages from aged was 76 years, while in the younger it was 56 years. As compared to the control, aged patients had longer mechanic ventilation time , higher intensive care unit and hospital mortality: 63.1% versus 26.3% and 74.2% versus 47.4% (P<0.05), respectively. In addition, the aged under mechanic ventilation had increased desintubation failures, difficult ventilatory weaning and deaths directly related to respiratory dysfunction. The mechanic ventilation time was an independent risk factor for death in the intensive care unit in aged patients (OR= 2.7, p=0.02). The area under the ROC curve of mechanic ventilation about intensive care unit death was 0.92 (95% CI 0.85-0.97, p (area 0.5)=0.0001), cutoff point of 4 days, sensitivity 89.4% and specificity 77.1%. CONCLUSIONS: Mechanic ventilation patients over 65years of age have a worse prognosis than the younger, and the longer the mechanic ventilation time, the higher will be intensive care mortality.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):360-365
DOI 10.1590/S0103-507X2006000400007
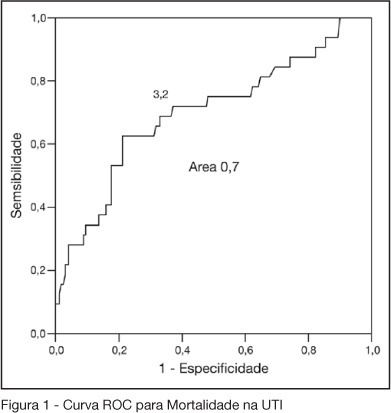
BACKGROUND AND OBJECTIVES: One of the greatest challenges found by the intensivists in their daily activities is tissue hipoperfusion control. Blood lactate is generally accepted as a marker of tissular hypoxia and several studies have demonstrated good correlation between blood lactate and prognosis during shock and resuscitation. The aim of this study was to evaluate the clinical utility of arterial blood lactate as a marker of morbidity and mortality in critically ill patients in the post-operative period of high risk non-cardiac surgeries. METHODS: Prospective and observational cohort study realized in an ICU of a tertiary hospital during a four month period. Demographic data of the patients submitted to high risk surgeries were collected, besides arterial lactate measures and number and type of complications in the post-operative period. To the statistic analysis was considered as significant a p < 0.05. The predictive ability of the indexes to differentiate survivors from non-survivors was tested using ROC curves. Lenght of ICU stay estimation where calculated by Kaplan Meier method. RESULTS: Were included 202 patients. 50.2% were female and their mean age was 66.5 ± 13.6 years. APACHE II score was 17.4 ± 3.0 and the median of MODS score was 4 (2-6). Median lenght of surgeries was 4h (3-6h). 70.7% of the surgeries were elective ones. ICU and hospital mortality were 15.6% and 33.7%, respectively. The best lactate value to discriminate mortality was 3.2 mmol/L, with sensitivity of 62.5%, specificity of 78.8% and an area under the curve of 0.7. 62.5% of patients with lactate > 3.2 did not survive versus 21.2% of survivors (OR = 2.95 IC95% 1.98- 4.38, p < 0.0001). ICU lenght of stay was greater when > 3.2 mmol/L (log rank 0.007) lactate. CONCLUSIONS: High risk patients submitted to non cardiac surgeries and admitted to the ICU with hiperlactatemia, defined as an arterial lactate > 3.2 mmol/L, are prone to a longer ICU lenght of stay and to die.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):360-365
DOI 10.1590/S0103-507X2006000400007
BACKGROUND AND OBJECTIVES: One of the greatest challenges found by the intensivists in their daily activities is tissue hipoperfusion control. Blood lactate is generally accepted as a marker of tissular hypoxia and several studies have demonstrated good correlation between blood lactate and prognosis during shock and resuscitation. The aim of this study was to evaluate the clinical utility of arterial blood lactate as a marker of morbidity and mortality in critically ill patients in the post-operative period of high risk non-cardiac surgeries. METHODS: Prospective and observational cohort study realized in an ICU of a tertiary hospital during a four month period. Demographic data of the patients submitted to high risk surgeries were collected, besides arterial lactate measures and number and type of complications in the post-operative period. To the statistic analysis was considered as significant a p < 0.05. The predictive ability of the indexes to differentiate survivors from non-survivors was tested using ROC curves. Lenght of ICU stay estimation where calculated by Kaplan Meier method. RESULTS: Were included 202 patients. 50.2% were female and their mean age was 66.5 ± 13.6 years. APACHE II score was 17.4 ± 3.0 and the median of MODS score was 4 (2-6). Median lenght of surgeries was 4h (3-6h). 70.7% of the surgeries were elective ones. ICU and hospital mortality were 15.6% and 33.7%, respectively. The best lactate value to discriminate mortality was 3.2 mmol/L, with sensitivity of 62.5%, specificity of 78.8% and an area under the curve of 0.7. 62.5% of patients with lactate > 3.2 did not survive versus 21.2% of survivors (OR = 2.95 IC95% 1.98- 4.38, p < 0.0001). ICU lenght of stay was greater when > 3.2 mmol/L (log rank 0.007) lactate. CONCLUSIONS: High risk patients submitted to non cardiac surgeries and admitted to the ICU with hiperlactatemia, defined as an arterial lactate > 3.2 mmol/L, are prone to a longer ICU lenght of stay and to die.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
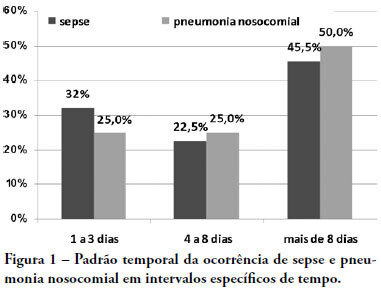
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):376-384
DOI 10.1590/S0103-507X2008000400010
OBJECTIVES: Due to the dramatic medical breakthroughs and an increasingly ageing population, the proportion of patients who are at risk of dying following surgery is increasing over time. The aim of this study was to evaluate the outcomes and the epidemiology of non-cardiac surgical patients admitted to the intensive care unit. METHODS: A multicenter, prospective, observational, cohort study was carried out in 21 intensive care units. A total of 885 adult surgical patients admitted to a participating intensive care unit from April to June 2006 were evaluated and 587 patients were enrolled. Exclusion criteria were trauma, cardiac, neurological, gynecologic, obstetric and palliative surgeries. The main outcome measures were postoperative complications and intensive care unit and 90-day mortality rates. RESULTS: Major and urgent surgeries were performed in 66.4% and 31.7% of the patients, respectively. The intensive care unit mortality rate was 15%, and 38% of the patients had postoperative complications. The most common complication was infection or sepsis (24.7%). Myocardial ischemia was diagnosed in only 1.9% of the patients. A total of 94 % of the patients who died after surgery had co-morbidities at the time of surgery (3.4 ± 2.2). Multiple organ failure was the main cause of death (53%). CONCLUSION: Sepsis is the predominant cause of morbidity in patients undergoing non-cardiac surgery. In this patient population, multiple organ failure prevailed as the most frequent cause of death in the hospital.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):49-55
DOI 10.1590/S0103-507X2011000100009
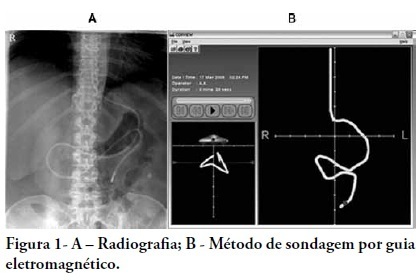
OBJECTIVE: Appropriate nutritional support is important to the outcomes of critically ill patients. However, a significant portion of these patients experience intestinal motility problems. Administration of enteral nutrition by means of tubes placed in the post-pyloric position has been suggested to improve the nutrition tolerance. The aim of this study was to compare the rate of successful post-pyloric placement using a real-time electromagnetic positioning device to the success rate using the conventional placement method. METHODS: This was a prospective, randomized and controlled study, conducted in a tertiary hospital over a period of three months. The patients were randomized to one of two groups: electromagnetically guided system group, whose patients underwent real-time monitoring of post-pyloric tube placement; or the control group, whose patients underwent tube placment using to the conventional blinded technique. The rates of successful post-pyloric placement and the procedure times were assessed and compared between the groups. RESULTS: Thirty-seven patients were enrolled, 18 in the electromagnetic group and 19 in the control group. The final tube position was evaluated using radiography. The electromagnetic guided group showed better success rates and shorter procedure times when compared to the control group. Additionally, in the electromagnetic guided group, higher pH values were found in the fluids aspirated from the probe, suggesting successful postpyloric placement. CONCLUSION: The electromagnetically guided method provided better placement accuracy than did the conventional technique.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):49-55
DOI 10.1590/S0103-507X2011000100009
OBJECTIVE: Appropriate nutritional support is important to the outcomes of critically ill patients. However, a significant portion of these patients experience intestinal motility problems. Administration of enteral nutrition by means of tubes placed in the post-pyloric position has been suggested to improve the nutrition tolerance. The aim of this study was to compare the rate of successful post-pyloric placement using a real-time electromagnetic positioning device to the success rate using the conventional placement method. METHODS: This was a prospective, randomized and controlled study, conducted in a tertiary hospital over a period of three months. The patients were randomized to one of two groups: electromagnetically guided system group, whose patients underwent real-time monitoring of post-pyloric tube placement; or the control group, whose patients underwent tube placment using to the conventional blinded technique. The rates of successful post-pyloric placement and the procedure times were assessed and compared between the groups. RESULTS: Thirty-seven patients were enrolled, 18 in the electromagnetic group and 19 in the control group. The final tube position was evaluated using radiography. The electromagnetic guided group showed better success rates and shorter procedure times when compared to the control group. Additionally, in the electromagnetic guided group, higher pH values were found in the fluids aspirated from the probe, suggesting successful postpyloric placement. CONCLUSION: The electromagnetically guided method provided better placement accuracy than did the conventional technique.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
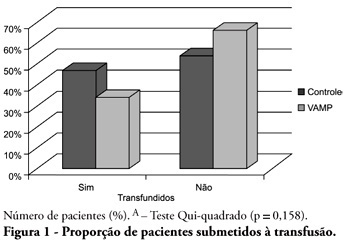
OBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups' transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):5-10
DOI 10.1590/S0103-507X2010000100003
OBJECTIVE: Anemia is common in severely ill patients, and blood sampling plays a relevant causative role. Consequently, blood transfusions are frequent an related to several complications. Trying to reduce the transfusion-related risk, minimizing blood loss is mandatory. Thus, this work aimed to evaluate a closed blood sampling system as a strategy to spare unnecessary blood losses and transfusions. METHODS: This was a prospective, randomized, controlled, multicenter, 6 months, clinical trial. The patients were assigned to either VAMP (Venous Arterial Blood Management Protection) group, using a closed blood sampling system, or control group. The groups' transfusion rate, as well as hemoglobin (Hb) and Hematocrit (Ht) changes were compared for 14 days. RESULTS: Were included 127 patients, 65 assigned to the control group, and 62 to VAMP. During the intensive care unit stay, both groups experienced both hemoglobin and hematocrit drops. However, when the final Ht and Hb were compared between the groups, a difference was identified with higher values in the VAMP group (p=0.03; p=0.006, respectively). No statistical difference was found for both groups transfusion rates, although the VAMP group had an absolute 12% blood transfusion reduction. CONCLUSION: The use of a closed blood sampling system was able to minimize blood count values changes, however failed to reduce transfusions rate.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):63-77
DOI 10.1590/S0103-507X2006000100012
BACKGROUND AND OBJECTIVES: Monitoring of vital functions is one of the most important tools in the management of critically ill patients. Nowadays is possible to detect and analyze a great deal of physiologic data using a lot of invasive and non-invasive methods. The intensivist must be able to select and carry out the most appropriate monitoring technique according to the patient requirements and taking into account the benefit/risk ratio. Despite the fast development of non invasive monitoring techniques, invasive hemodynamic monitoring using Pulmonary Artery Catheter still is one of the basic procedures in Critical Care. The aim was to define recommendations about clinical utility of basic hemodynamic monitoring methods and the Use of Pulmonary Artery Catheter. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty-five physicians and nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made based on 55 questions about the use of central venous pressure, invasive arterial pressure, pulmonary artery catheter and its indications in different settings. CONCLUSIONS: Evaluation of central venous pressure and invasive arterial pressure, besides variables obtained by the PAC allow the understanding of cardiovascular physiology that is of great value to the care of critically ill patients. However, the correct use of these tools is fundamental to achieve the benefits due to its use.