-
Editorial
Research networks and their contribution to the quality of critical care
Rev Bras Ter Intensiva. 2014;26(2):77-78
Abstract
EditorialResearch networks and their contribution to the quality of critical care
Rev Bras Ter Intensiva. 2014;26(2):77-78
DOI 10.5935/0103-507X.20140012
Views1Over the past few years, the intensive care field in our country has increased in terms of both volume and quality. There is now a huge community of healthcare professionals in more than 2,500 intensive care units throughout the country.() This dissemination of our specialty has also been associated with an increased interest in research […]See moreViews1

Abstract
EditorialResearch networks and their contribution to the quality of critical care
Rev Bras Ter Intensiva. 2014;26(2):77-78
DOI 10.5935/0103-507X.20140012
Views1Over the past few years, the intensive care field in our country has increased in terms of both volume and quality. There is now a huge community of healthcare professionals in more than 2,500 intensive care units throughout the country.() This dissemination of our specialty has also been associated with an increased interest in research […]See more -
Editorial
Research networks and clinical trials in critical care in Brazil: current status and future perspectives
Rev Bras Ter Intensiva. 2014;26(2):79-80
Abstract
EditorialResearch networks and clinical trials in critical care in Brazil: current status and future perspectives
Rev Bras Ter Intensiva. 2014;26(2):79-80
DOI 10.5935/0103-507X.20140013
Views0Scientific CommitteeAlexandre Biasi Cavalcanti, Felipe Dal-Pizzol, Fernando Augusto Bozza, Flávia Ribeiro Machado, Glauco Adrieno Westphal, Jorge Ibrain Figueira Salluh, Leandro Utino Taniguchi, Luciano César Pontes de Azevedo, Ludhmila Abrahão Hajjar, Márcio Soares, Suzana Margareth Ajeje Lobo, Thiago Costa Lisboa[…]See moreViews0Abstract
EditorialResearch networks and clinical trials in critical care in Brazil: current status and future perspectives
Rev Bras Ter Intensiva. 2014;26(2):79-80
DOI 10.5935/0103-507X.20140013
Views0Scientific CommitteeAlexandre Biasi Cavalcanti, Felipe Dal-Pizzol, Fernando Augusto Bozza, Flávia Ribeiro Machado, Glauco Adrieno Westphal, Jorge Ibrain Figueira Salluh, Leandro Utino Taniguchi, Luciano César Pontes de Azevedo, Ludhmila Abrahão Hajjar, Márcio Soares, Suzana Margareth Ajeje Lobo, Thiago Costa Lisboa[…]See more -
Editorial
Sedation and memories in critical care
Rev Bras Ter Intensiva. 2014;26(2):81-82
Abstract
EditorialSedation and memories in critical care
Rev Bras Ter Intensiva. 2014;26(2):81-82
DOI 10.5935/0103-507X.20140014
Views0Sedation strategies in intensive care units (ICU) have changed over the past decade towards daily wake-up calls, less sedation and even no sedation.(–) Furthermore, new ventilatory modes were designed to promote better patient synchrony with the ventilator and fewer sedation requirements. It is well known that the strategies used to reduce sedation reduce the length […]See moreViews0Abstract
EditorialSedation and memories in critical care
Rev Bras Ter Intensiva. 2014;26(2):81-82
DOI 10.5935/0103-507X.20140014
Views0Sedation strategies in intensive care units (ICU) have changed over the past decade towards daily wake-up calls, less sedation and even no sedation.(–) Furthermore, new ventilatory modes were designed to promote better patient synchrony with the ventilator and fewer sedation requirements. It is well known that the strategies used to reduce sedation reduce the length […]See more -
Commentary
The use of hypothermia and outcome post cardiopulmonary resuscitation in 2014
Rev Bras Ter Intensiva. 2014;26(2):83-85
Abstract
CommentaryThe use of hypothermia and outcome post cardiopulmonary resuscitation in 2014
Rev Bras Ter Intensiva. 2014;26(2):83-85
DOI 10.5935/0103-507X.20140015
Views0THE PASTIn animal trials clinical outcome and histopathological damage of the brain tissue due to hypoxia after cardiac arrest was found to be reduced by mild therapeutic hypothermia.(,)The clinical milestone trials in 2002 also have found mild therapeutic hypothermia at 32°-34 °C for 12-24 hours to be neuroprotective in treatment of the post-cardiac arrest syndrome.(–) […]See moreViews0Abstract
CommentaryThe use of hypothermia and outcome post cardiopulmonary resuscitation in 2014
Rev Bras Ter Intensiva. 2014;26(2):83-85
DOI 10.5935/0103-507X.20140015
Views0THE PASTIn animal trials clinical outcome and histopathological damage of the brain tissue due to hypoxia after cardiac arrest was found to be reduced by mild therapeutic hypothermia.(,)The clinical milestone trials in 2002 also have found mild therapeutic hypothermia at 32°-34 °C for 12-24 hours to be neuroprotective in treatment of the post-cardiac arrest syndrome.(–) […]See more -
Commentary
Use of antipsychotics for the treatment of intensive care unit delirium
Rev Bras Ter Intensiva. 2014;26(2):86-88
Abstract
CommentaryUse of antipsychotics for the treatment of intensive care unit delirium
Rev Bras Ter Intensiva. 2014;26(2):86-88
DOI 10.5935/0103-507X.20140016
Views0Intensivists are faced on a daily basis with patients suffering from delirium, which causes them and their loved ones considerable distress and predicts for those patients worse outcomes, including dementia and death. With the use of routine screening tools delirium is now identified in patients previously thought to be still under the effects of sedation, […]See moreViews0Abstract
CommentaryUse of antipsychotics for the treatment of intensive care unit delirium
Rev Bras Ter Intensiva. 2014;26(2):86-88
DOI 10.5935/0103-507X.20140016
Views0Intensivists are faced on a daily basis with patients suffering from delirium, which causes them and their loved ones considerable distress and predicts for those patients worse outcomes, including dementia and death. With the use of routine screening tools delirium is now identified in patients previously thought to be still under the effects of sedation, […]See more -
Special Article
Brazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views6See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
Views6Abstract
Special ArticleBrazilian recommendations of mechanical ventilation 2013. Part I
Rev Bras Ter Intensiva. 2014;26(2):89-121
DOI 10.5935/0103-507X.20140017
Views6See morePerspectives on invasive and noninvasive ventilatory support for critically ill patients are evolving, as much evidence indicates that ventilation may have positive effects on patient survival and the quality of the care provided in intensive care units in Brazil. For those reasons, the Brazilian Association of Intensive Care Medicine (Associação de Medicina Intensiva Brasileira – AMIB) and the Brazilian Thoracic Society (Sociedade Brasileira de Pneumologia e Tisiologia – SBPT), represented by the Mechanical Ventilation Committee and the Commission of Intensive Therapy, respectively, decided to review the literature and draft recommendations for mechanical ventilation with the goal of creating a document for bedside guidance as to the best practices on mechanical ventilation available to their members. The document was based on the available evidence regarding 29 subtopics selected as the most relevant for the subject of interest. The project was developed in several stages, during which the selected topics were distributed among experts recommended by both societies with recent publications on the subject of interest and/or significant teaching and research activity in the field of mechanical ventilation in Brazil. The experts were divided into pairs that were charged with performing a thorough review of the international literature on each topic. All the experts met at the Forum on Mechanical Ventilation, which was held at the headquarters of AMIB in São Paulo on August 3 and 4, 2013, to collaboratively draft the final text corresponding to each sub-topic, which was presented to, appraised, discussed and approved in a plenary session that included all 58 participants and aimed to create the final document.
-
Original Article
Sedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
Abstract
Original ArticleSedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
Views0See moreObjective:
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
Methods:
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants’ clinical records; the data relative to the participants’ memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
Results:
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
Conclusion:
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Views0Abstract
Original ArticleSedation and memories of patients subjected to mechanical ventilation in an intensive care unit
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
Views0See moreObjective:
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
Methods:
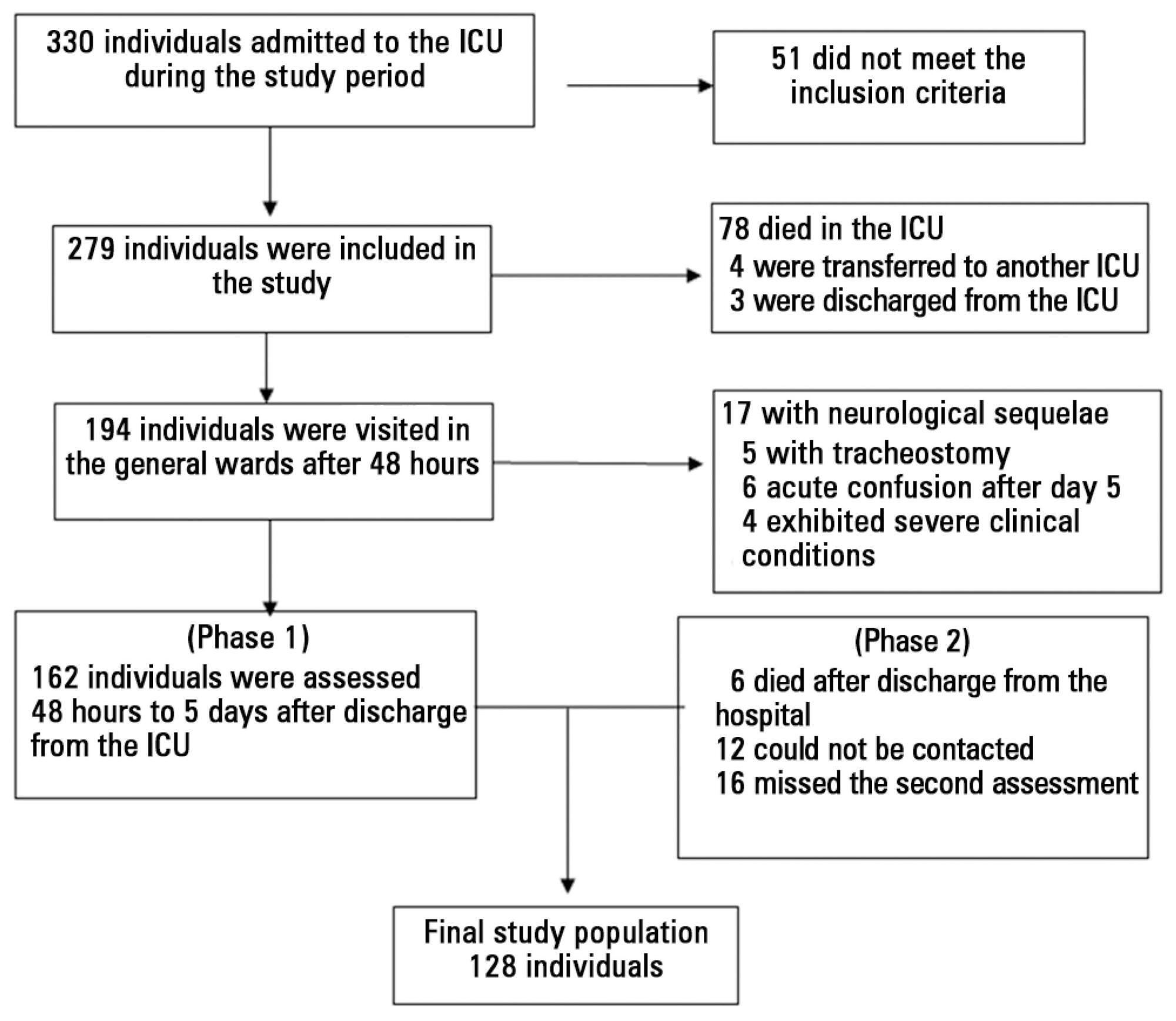
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants’ clinical records; the data relative to the participants’ memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
Results:
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
Conclusion:
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
-
Original Articles
Inflammatory and perfusion markers as risk factors and predictors of critically ill patient readmission
Rev Bras Ter Intensiva. 2014;26(2):130-136
Abstract
Original ArticlesInflammatory and perfusion markers as risk factors and predictors of critically ill patient readmission
Rev Bras Ter Intensiva. 2014;26(2):130-136
DOI 10.5935/0103-507X.20140019
Views0Objective:
To assess the performance of central venous oxygen saturation, lactate, base deficit, and C-reactive protein levels and SOFA and SWIFT scores on the day of discharge from the intensive care unit as predictors of patient readmission to the intensive care unit.
Methods:
This prospective and observational study collected data from 1,360 patients who were admitted consecutively to a clinical-surgical intensive care unit from August 2011 to August 2012. The clinical characteristics and laboratory data of readmitted and non-readmitted patients after discharge from the intensive care unit were compared. Using a multivariate analysis, the risk factors independently associated with readmission were identified.
Results:
The C-reactive protein, central venous oxygen saturation, base deficit, and lactate levels and the SWIFT and SOFA scores did not correlate with the readmission of critically ill patients. Increased age and contact isolation because of multidrug-resistant organisms were identified as risk factors that were independently associated with readmission in this study group.
Conclusion:
Inflammatory and perfusion parameters were not associated with patient readmission. Increased age and contact isolation because of multidrug-resistant organisms were identified as predictors of readmission to the intensive care unit.
Keywords:C-reactive proteinLactatePatient readmissionPatient readmission/economicsPatient safetyrisk factorsSee moreViews0Abstract
Original ArticlesInflammatory and perfusion markers as risk factors and predictors of critically ill patient readmission
Rev Bras Ter Intensiva. 2014;26(2):130-136
DOI 10.5935/0103-507X.20140019
Views0Objective:
To assess the performance of central venous oxygen saturation, lactate, base deficit, and C-reactive protein levels and SOFA and SWIFT scores on the day of discharge from the intensive care unit as predictors of patient readmission to the intensive care unit.
Methods:
This prospective and observational study collected data from 1,360 patients who were admitted consecutively to a clinical-surgical intensive care unit from August 2011 to August 2012. The clinical characteristics and laboratory data of readmitted and non-readmitted patients after discharge from the intensive care unit were compared. Using a multivariate analysis, the risk factors independently associated with readmission were identified.
Results:
The C-reactive protein, central venous oxygen saturation, base deficit, and lactate levels and the SWIFT and SOFA scores did not correlate with the readmission of critically ill patients. Increased age and contact isolation because of multidrug-resistant organisms were identified as risk factors that were independently associated with readmission in this study group.
Conclusion:
Inflammatory and perfusion parameters were not associated with patient readmission. Increased age and contact isolation because of multidrug-resistant organisms were identified as predictors of readmission to the intensive care unit.
Keywords:C-reactive proteinLactatePatient readmissionPatient readmission/economicsPatient safetyrisk factorsSee more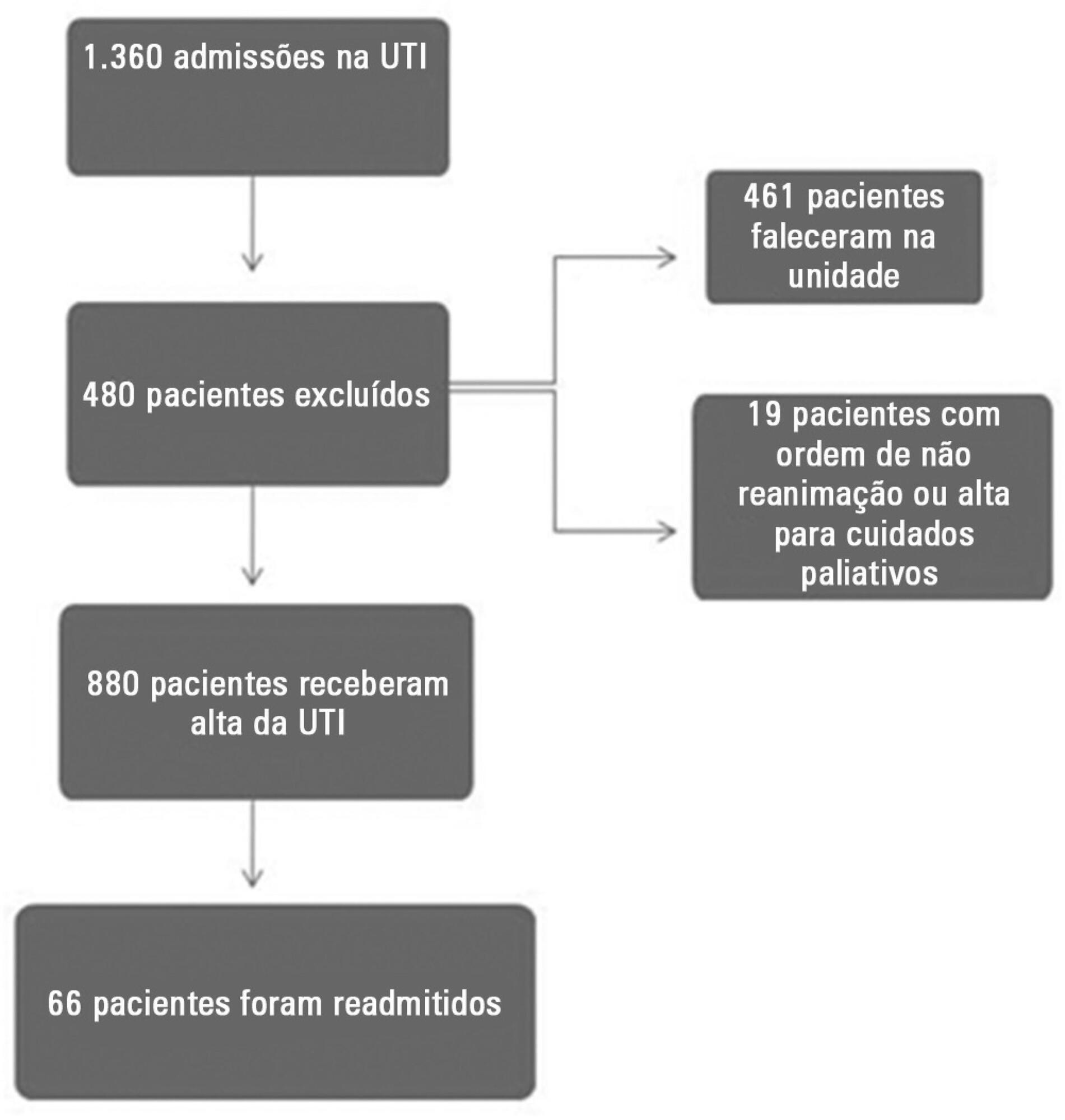
-
Original Article
Ventilatory weaning practices in intensive care units in the city of Cali
Rev Bras Ter Intensiva. 2014;26(2):137-142
Abstract
Original ArticleVentilatory weaning practices in intensive care units in the city of Cali
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
Views0See moreObjective:
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
Methods:
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
Results:
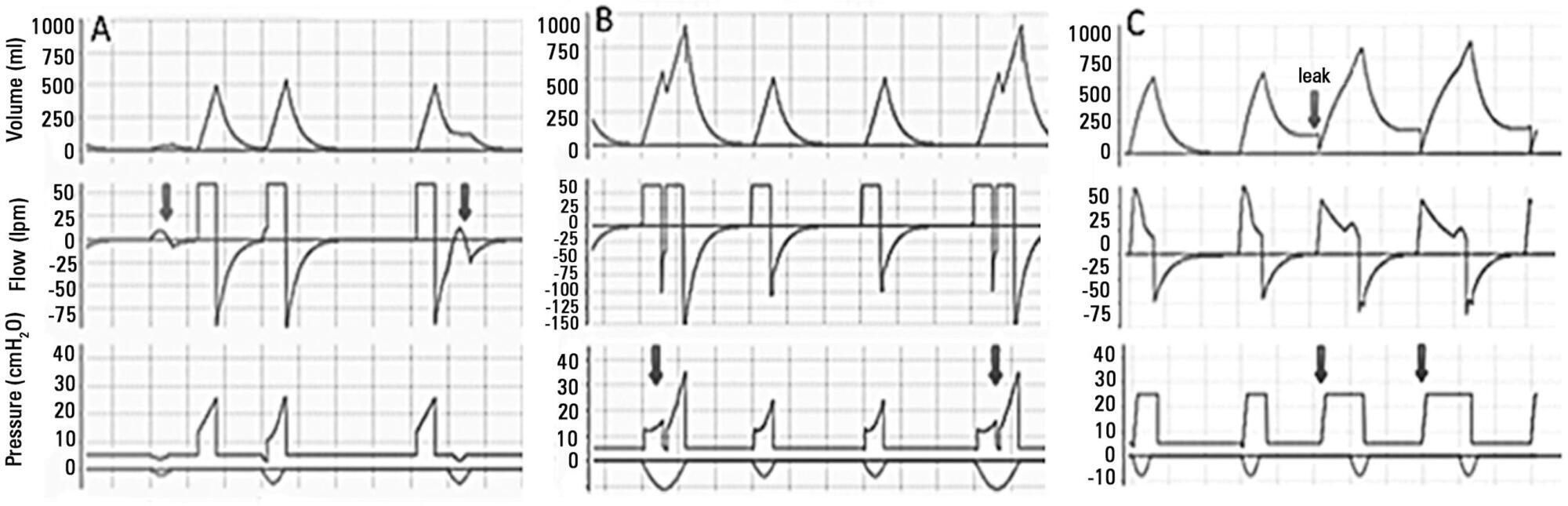
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
Conclusion:
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
Views0Abstract
Original ArticleVentilatory weaning practices in intensive care units in the city of Cali
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
Views0See moreObjective:
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
Methods:
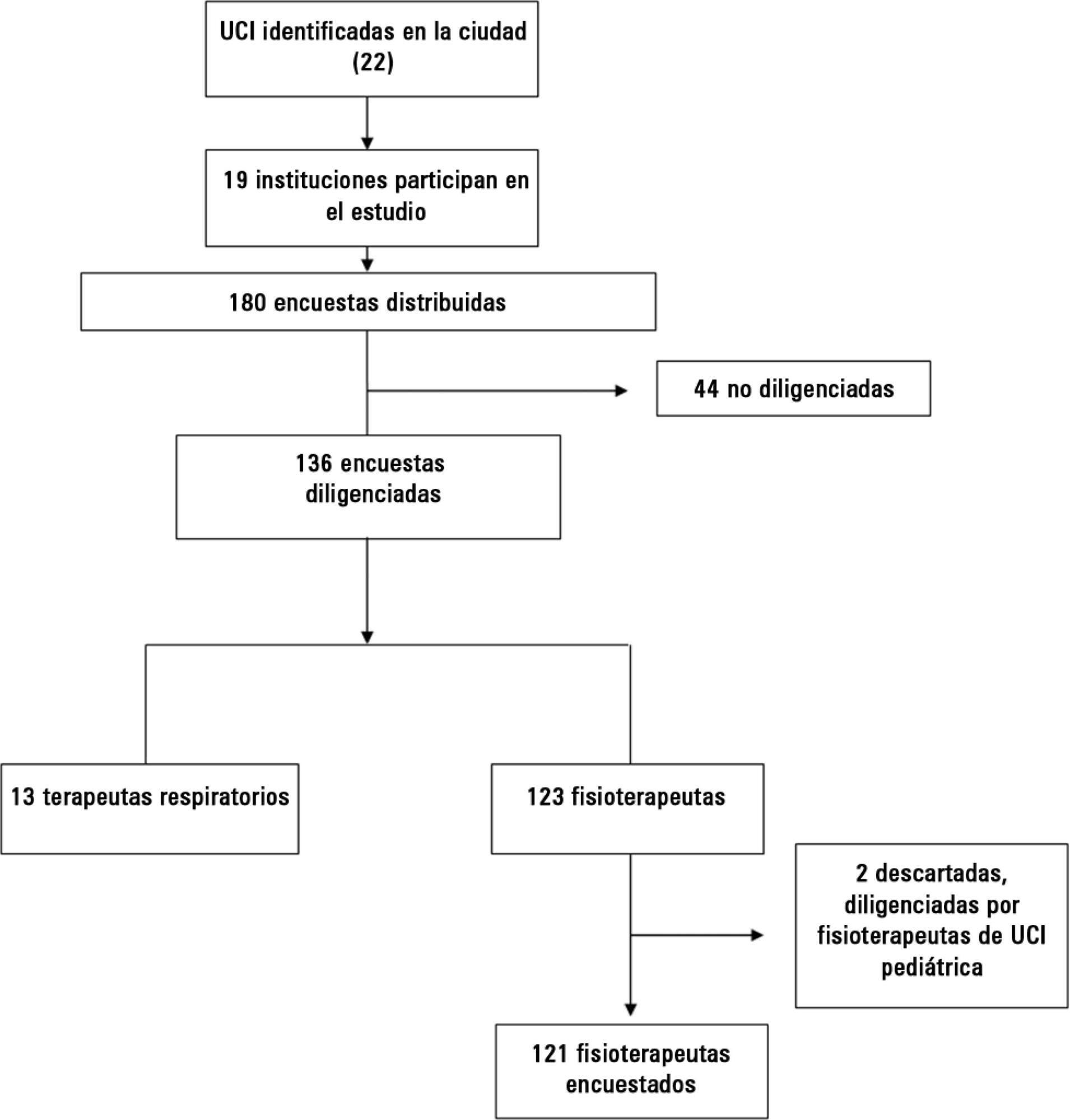
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
Results:
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
Conclusion:
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
-
Original Articles
Fractional excretion of potassium in the course of acute kidney injury in critically ill patients: potential monitoring tool?
Rev Bras Ter Intensiva. 2014;26(2):143-147
Abstract
Original ArticlesFractional excretion of potassium in the course of acute kidney injury in critically ill patients: potential monitoring tool?
Rev Bras Ter Intensiva. 2014;26(2):143-147
DOI 10.5935/0103-507X.20140021
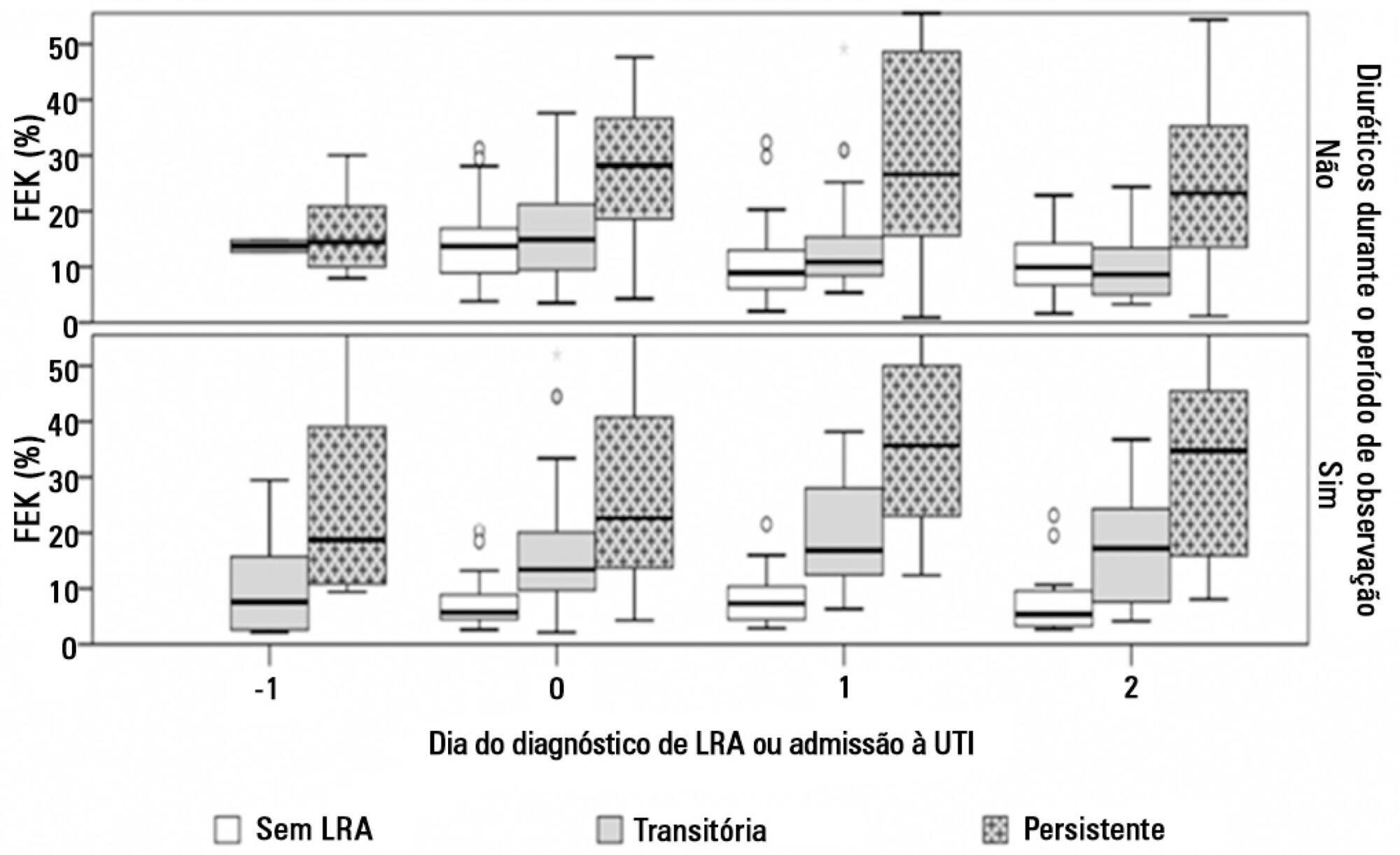
Views0See moreObjective:
To evaluate the behavior of fractional excretion of potassium in the course of acute kidney injury in critically ill patients.
Methods:
As part of a larger study in which we have evaluated blood and urinary parameters in the course of acute kidney injury, 168 patients were included. Blood and urine samples were collected daily until the removal of the urinary catheter or the initiation of renal replacement therapy. We describe the evolution of fractional excretion of potassium based on whether acute kidney injury was diagnosed, its duration (transient or persistent) and its severity (creatinine-based Acute Kidney Injury Network – AKIN stage). The diagnostic performance of fractional excretion of potassium in predicting the duration of acute kidney injury and the need for renal replacement therapy on the day of acute kidney injury diagnosis was also evaluated.
Results:
Fractional excretion of potassium was significantly higher in persistent acute kidney injury compared to transient acute kidney injury on the day of acute kidney injury diagnosis (24.8 vs. 13.8%, p<0.001). Both groups had the median fractional excretion of potassium increasing in the two days preceding the acute kidney injury diagnosis. Patients without acute kidney injury had stable low fractional excretion of potassium values. The fractional excretion of potassium was fairly accurate in predicting persistent acute kidney injury (area under the curve: 0.712; 95% confidence interval: 0.614-0.811; p<0.001) on the day of acute kidney injury diagnosis. The area under the curve was 0.663 (95% confidence interval: 0.523-0.803; p=0.03) for renal replacement therapy. The fractional excretion of potassium increased with maximum AKIN stage reached, in both transient and persistent acute kidney injury.
Conclusion:
Sequential fractional excretion of potassium assessment appears to be useful in critically ill patients at risk for acute kidney injury.
Views0Abstract
Original ArticlesFractional excretion of potassium in the course of acute kidney injury in critically ill patients: potential monitoring tool?
Rev Bras Ter Intensiva. 2014;26(2):143-147
DOI 10.5935/0103-507X.20140021
Views0See moreObjective:
To evaluate the behavior of fractional excretion of potassium in the course of acute kidney injury in critically ill patients.
Methods:
As part of a larger study in which we have evaluated blood and urinary parameters in the course of acute kidney injury, 168 patients were included. Blood and urine samples were collected daily until the removal of the urinary catheter or the initiation of renal replacement therapy. We describe the evolution of fractional excretion of potassium based on whether acute kidney injury was diagnosed, its duration (transient or persistent) and its severity (creatinine-based Acute Kidney Injury Network – AKIN stage). The diagnostic performance of fractional excretion of potassium in predicting the duration of acute kidney injury and the need for renal replacement therapy on the day of acute kidney injury diagnosis was also evaluated.
Results:
Fractional excretion of potassium was significantly higher in persistent acute kidney injury compared to transient acute kidney injury on the day of acute kidney injury diagnosis (24.8 vs. 13.8%, p<0.001). Both groups had the median fractional excretion of potassium increasing in the two days preceding the acute kidney injury diagnosis. Patients without acute kidney injury had stable low fractional excretion of potassium values. The fractional excretion of potassium was fairly accurate in predicting persistent acute kidney injury (area under the curve: 0.712; 95% confidence interval: 0.614-0.811; p<0.001) on the day of acute kidney injury diagnosis. The area under the curve was 0.663 (95% confidence interval: 0.523-0.803; p=0.03) for renal replacement therapy. The fractional excretion of potassium increased with maximum AKIN stage reached, in both transient and persistent acute kidney injury.
Conclusion:
Sequential fractional excretion of potassium assessment appears to be useful in critically ill patients at risk for acute kidney injury.
-
Original Articles
Sepsis in intensive care unit patients with traumatic brain injury: factors associated with higher mortality
Rev Bras Ter Intensiva. 2014;26(2):148-154
Abstract
Original ArticlesSepsis in intensive care unit patients with traumatic brain injury: factors associated with higher mortality
Rev Bras Ter Intensiva. 2014;26(2):148-154
DOI 10.5935/0103-507X.20140022
Views0Objective:
Patients with traumatic brain injury are particularly susceptible to sepsis, which may exacerbate the systemic inflammatory response and lead to organ dysfunction. The influence of clinical variables on the mortality of intensive care unit patients with traumatic brain injury and sepsis was investigated.
Methods:
The present investigation was a retrospective study involving 175 patients with traumatic brain injury who were treated in a period of 1 year at a reference hospital for trauma and who had sepsis, severe sepsis, or septic shock. Demographic and clinical data were obtained, and the SOFA score was calculated at the time sepsis was found and after 72 hours.
Results:
There was a predominance of young men with severe traumatic brain injury, multiple head injuries, sepsis with a pulmonary focus, prolonged hospital stay, and high mortality (37.7%). Circulatory and respiratory failure had a high incidence, but renal and coagulation failure were less frequent, and liver failure was not observed. After logistic regression, the presence of septic shock and respiratory failure 72 hours after the sepsis diagnosis was associated with higher mortality, with an odds ratio of 7.56 (95%CI=2.04-27.31, p=0.0024) and 6.62 (95%CI=1.93-22.78, p=0.0027), respectively. In addition, there was a higher mortality among patients who had no organ failure on D1 but who developed the condition after 72 hours of sepsis and in those patients who already had organ failure at the time sepsis was diagnosed and remained in this condition after 72 hours.
Conclusion:
Septic shock and progressive organ (particularly respiratory) dysfunction increases the mortality of patients with traumatic brain injury and sepsis.
Keywords:craniocerebral traumaIntensive care unitsMultiple organ failureRespiratory distress syndrome, adultSepsisSeptic shockSee moreViews0Abstract
Original ArticlesSepsis in intensive care unit patients with traumatic brain injury: factors associated with higher mortality
Rev Bras Ter Intensiva. 2014;26(2):148-154
DOI 10.5935/0103-507X.20140022
Views0Objective:
Patients with traumatic brain injury are particularly susceptible to sepsis, which may exacerbate the systemic inflammatory response and lead to organ dysfunction. The influence of clinical variables on the mortality of intensive care unit patients with traumatic brain injury and sepsis was investigated.
Methods:
The present investigation was a retrospective study involving 175 patients with traumatic brain injury who were treated in a period of 1 year at a reference hospital for trauma and who had sepsis, severe sepsis, or septic shock. Demographic and clinical data were obtained, and the SOFA score was calculated at the time sepsis was found and after 72 hours.
Results:
There was a predominance of young men with severe traumatic brain injury, multiple head injuries, sepsis with a pulmonary focus, prolonged hospital stay, and high mortality (37.7%). Circulatory and respiratory failure had a high incidence, but renal and coagulation failure were less frequent, and liver failure was not observed. After logistic regression, the presence of septic shock and respiratory failure 72 hours after the sepsis diagnosis was associated with higher mortality, with an odds ratio of 7.56 (95%CI=2.04-27.31, p=0.0024) and 6.62 (95%CI=1.93-22.78, p=0.0027), respectively. In addition, there was a higher mortality among patients who had no organ failure on D1 but who developed the condition after 72 hours of sepsis and in those patients who already had organ failure at the time sepsis was diagnosed and remained in this condition after 72 hours.
Conclusion:
Septic shock and progressive organ (particularly respiratory) dysfunction increases the mortality of patients with traumatic brain injury and sepsis.
Keywords:craniocerebral traumaIntensive care unitsMultiple organ failureRespiratory distress syndrome, adultSepsisSeptic shockSee more -
Original Articles
Adequacy of energy and protein balance of enteral nutrition in intensive care: what are the limiting factors?
Rev Bras Ter Intensiva. 2014;26(2):155-162
Abstract
Original ArticlesAdequacy of energy and protein balance of enteral nutrition in intensive care: what are the limiting factors?
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
Views0Objective:
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
Methods:
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
Results:
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Conclusion:
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Keywords:Critical careEnergy and protein balanceEnergy requiremententeral nutritionIntensive carenutrition therapyNutritional supportSee moreViews0Abstract
Original ArticlesAdequacy of energy and protein balance of enteral nutrition in intensive care: what are the limiting factors?
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
Views0Objective:
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
Methods:
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
Results:
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Conclusion:
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Keywords:Critical careEnergy and protein balanceEnergy requiremententeral nutritionIntensive carenutrition therapyNutritional supportSee more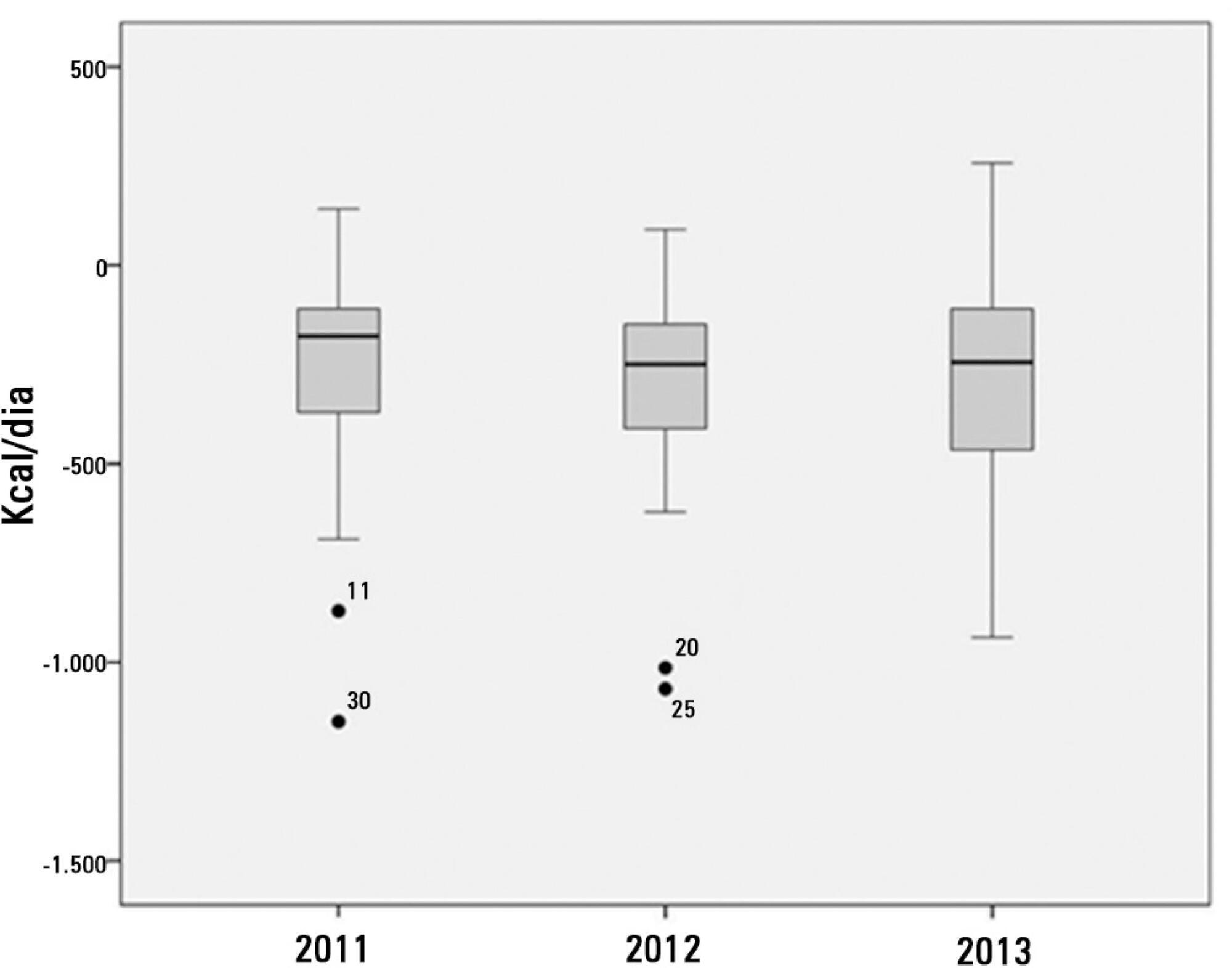
-
Original Articles
Comparative analysis between the alveolar recruitment maneuver and breath stacking technique in patients with acute lung injury
Rev Bras Ter Intensiva. 2014;26(2):163-168
Abstract
Original ArticlesComparative analysis between the alveolar recruitment maneuver and breath stacking technique in patients with acute lung injury
Rev Bras Ter Intensiva. 2014;26(2):163-168
DOI 10.5935/0103-507X.20140024
Views0Objective:
To compare the effectiveness of the alveolar recruitment maneuver and the breath stacking technique with respect to lung mechanics and gas exchange in patients with acute lung injury.
Methods:
Thirty patients were distributed into two groups: Group 1 – breath stacking; and Group 2 – alveolar recruitment maneuver. After undergoing conventional physical therapy, all patients received both treatments with an interval of 1 day between them. In the first group, the breath stacking technique was used initially, and subsequently, the alveolar recruitment maneuver was applied. Group 2 patients were initially subjected to alveolar recruitment, followed by the breath stacking technique. Measurements of lung compliance and airway resistance were evaluated before and after the use of both techniques. Gas analyses were collected before and after the techniques were used to evaluate oxygenation and gas exchange.
Results:
Both groups had a significant increase in static compliance after breath stacking (p=0.021) and alveolar recruitment (p=0.03), but with no significant differences between the groups (p=0.95). The dynamic compliance did not increase for the breath stacking (p=0.22) and alveolar recruitment (p=0.074) groups, with no significant difference between the groups (p=0.11). The airway resistance did not decrease for either groups, i.e., breath stacking (p=0.91) and alveolar recruitment (p=0.82), with no significant difference between the groups (p=0.39). The partial pressure of oxygen increased significantly after breath stacking (p=0.013) and alveolar recruitment (p=0.04), but there was no significant difference between the groups (p=0.073). The alveolar-arterial O2 difference decreased for both groups after the breath stacking (p=0.025) and alveolar recruitment (p=0.03) interventions, and there was no significant difference between the groups (p=0.81).
Conclusion:
Our data suggest that the breath stacking and alveolar recruitment techniques are effective in improving the lung mechanics and gas exchange in patients with acute lung injury.
Keywords:Breathing exercisesPhysical therapy modalitiesPositive-pressure respiration/methodsPulmonary gas exchangeRespiratory mechanicsSee moreViews0Abstract
Original ArticlesComparative analysis between the alveolar recruitment maneuver and breath stacking technique in patients with acute lung injury
Rev Bras Ter Intensiva. 2014;26(2):163-168
DOI 10.5935/0103-507X.20140024
Views0Objective:
To compare the effectiveness of the alveolar recruitment maneuver and the breath stacking technique with respect to lung mechanics and gas exchange in patients with acute lung injury.
Methods:
Thirty patients were distributed into two groups: Group 1 – breath stacking; and Group 2 – alveolar recruitment maneuver. After undergoing conventional physical therapy, all patients received both treatments with an interval of 1 day between them. In the first group, the breath stacking technique was used initially, and subsequently, the alveolar recruitment maneuver was applied. Group 2 patients were initially subjected to alveolar recruitment, followed by the breath stacking technique. Measurements of lung compliance and airway resistance were evaluated before and after the use of both techniques. Gas analyses were collected before and after the techniques were used to evaluate oxygenation and gas exchange.
Results:
Both groups had a significant increase in static compliance after breath stacking (p=0.021) and alveolar recruitment (p=0.03), but with no significant differences between the groups (p=0.95). The dynamic compliance did not increase for the breath stacking (p=0.22) and alveolar recruitment (p=0.074) groups, with no significant difference between the groups (p=0.11). The airway resistance did not decrease for either groups, i.e., breath stacking (p=0.91) and alveolar recruitment (p=0.82), with no significant difference between the groups (p=0.39). The partial pressure of oxygen increased significantly after breath stacking (p=0.013) and alveolar recruitment (p=0.04), but there was no significant difference between the groups (p=0.073). The alveolar-arterial O2 difference decreased for both groups after the breath stacking (p=0.025) and alveolar recruitment (p=0.03) interventions, and there was no significant difference between the groups (p=0.81).
Conclusion:
Our data suggest that the breath stacking and alveolar recruitment techniques are effective in improving the lung mechanics and gas exchange in patients with acute lung injury.
Keywords:Breathing exercisesPhysical therapy modalitiesPositive-pressure respiration/methodsPulmonary gas exchangeRespiratory mechanicsSee more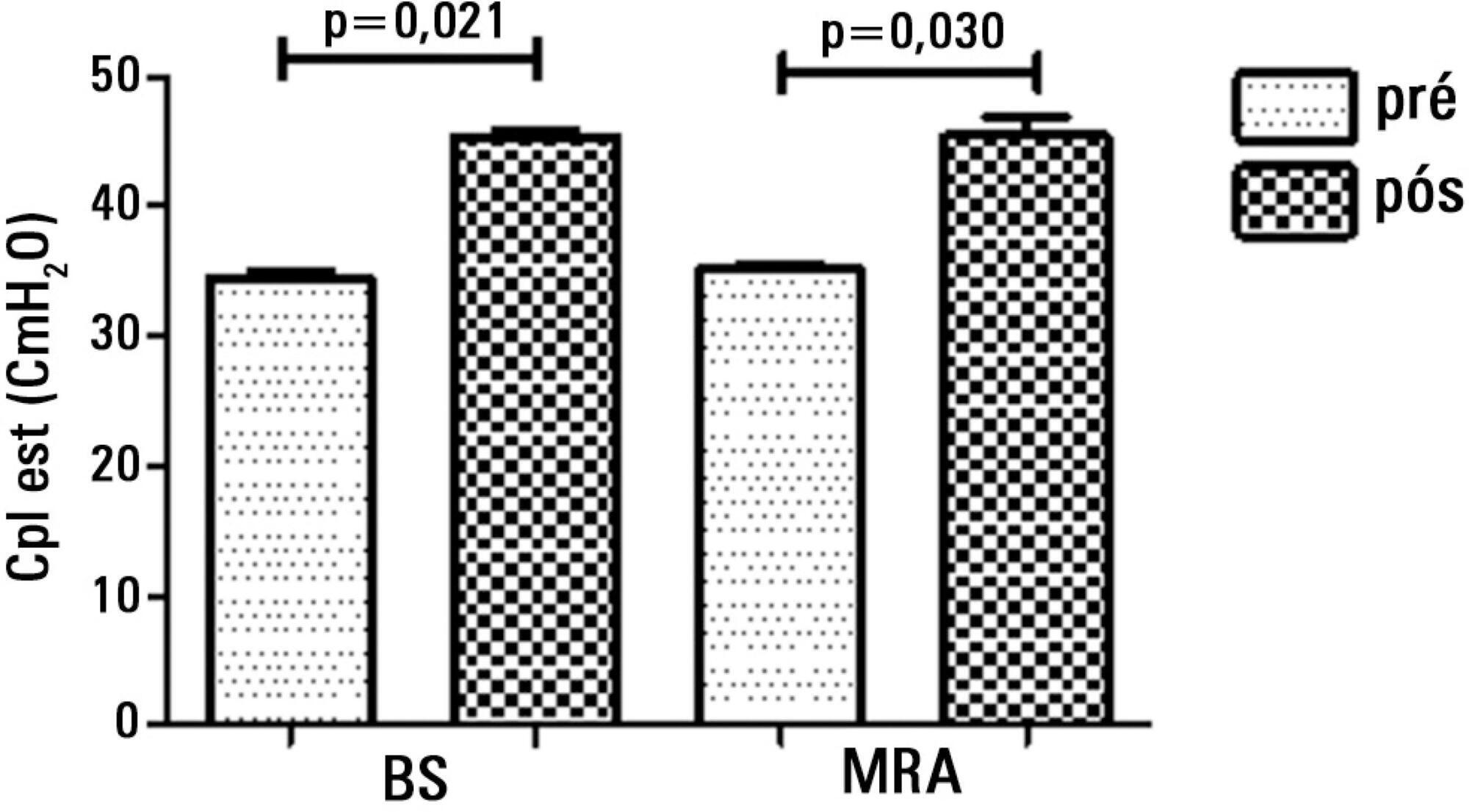
-
Original Articles
Influence of prone positioning on premature newborn infant stress assessed by means of salivary cortisol measurement: pilot study
Rev Bras Ter Intensiva. 2014;26(2):169-175
Abstract
Original ArticlesInfluence of prone positioning on premature newborn infant stress assessed by means of salivary cortisol measurement: pilot study
Rev Bras Ter Intensiva. 2014;26(2):169-175
DOI 10.5935/0103-507X.20140025
Views0Objective:
This study sought to assess the influence of prone positioning on the stress of newborn premature infants through the measurement of the salivary cortisol concentration and the evaluation of physiological and behavioral responses before and after changes in body positioning.
Methods:
Saliva samples were collected from newborn infants at two different times: the first (corresponding to the baseline) after a period of 40 minutes during which the infants were not subjected to any manipulation and were placed in the lateral or supine position, and the second 30 minutes after placement in the prone position. Variables including heart rate, respiratory rate, peripheral oxygen saturation, and the Brazelton sleep score were recorded before, during, and at the end of the period in the prone position.
Results:
The sample comprised 16 newborn premature infants (56.3% male) with a gestational age between 26 and 36 weeks, postnatal age between 1 and 33 days, birth weight of 935 to 3,050g, and weight at the time of intervention of 870 to 2,890g. During the intervention, six participants breathed room air, while the remainder received oxygen therapy. The median salivary cortisol concentration was lower in the prone position compared to baseline (0.13 versus 0.20; p=0.003), as was the median Brazelton sleep score (p=0.02). The average respiratory rate was lower after the intervention (54.88±7.15 versus 60±7.59; p=0.0004). The remainder of the investigated variables did not exhibit significant variation.
Conclusion:
Prone positioning significantly reduced the salivary cortisol level, respiratory rate, and Brazelton sleep score, suggesting a correlation between prone positioning and reduction of stress in preterm infants.
Keywords:Adrenal córtex/metabolismoHydrocortisone/analysisInfant newborn/metabolismInfant premature/metabolismIntensive care units, neonatalProne positionSaliva/analysisStress, physiologicalSee moreViews0Abstract
Original ArticlesInfluence of prone positioning on premature newborn infant stress assessed by means of salivary cortisol measurement: pilot study
Rev Bras Ter Intensiva. 2014;26(2):169-175
DOI 10.5935/0103-507X.20140025
Views0Objective:
This study sought to assess the influence of prone positioning on the stress of newborn premature infants through the measurement of the salivary cortisol concentration and the evaluation of physiological and behavioral responses before and after changes in body positioning.
Methods:
Saliva samples were collected from newborn infants at two different times: the first (corresponding to the baseline) after a period of 40 minutes during which the infants were not subjected to any manipulation and were placed in the lateral or supine position, and the second 30 minutes after placement in the prone position. Variables including heart rate, respiratory rate, peripheral oxygen saturation, and the Brazelton sleep score were recorded before, during, and at the end of the period in the prone position.
Results:
The sample comprised 16 newborn premature infants (56.3% male) with a gestational age between 26 and 36 weeks, postnatal age between 1 and 33 days, birth weight of 935 to 3,050g, and weight at the time of intervention of 870 to 2,890g. During the intervention, six participants breathed room air, while the remainder received oxygen therapy. The median salivary cortisol concentration was lower in the prone position compared to baseline (0.13 versus 0.20; p=0.003), as was the median Brazelton sleep score (p=0.02). The average respiratory rate was lower after the intervention (54.88±7.15 versus 60±7.59; p=0.0004). The remainder of the investigated variables did not exhibit significant variation.
Conclusion:
Prone positioning significantly reduced the salivary cortisol level, respiratory rate, and Brazelton sleep score, suggesting a correlation between prone positioning and reduction of stress in preterm infants.
Keywords:Adrenal córtex/metabolismoHydrocortisone/analysisInfant newborn/metabolismInfant premature/metabolismIntensive care units, neonatalProne positionSaliva/analysisStress, physiologicalSee more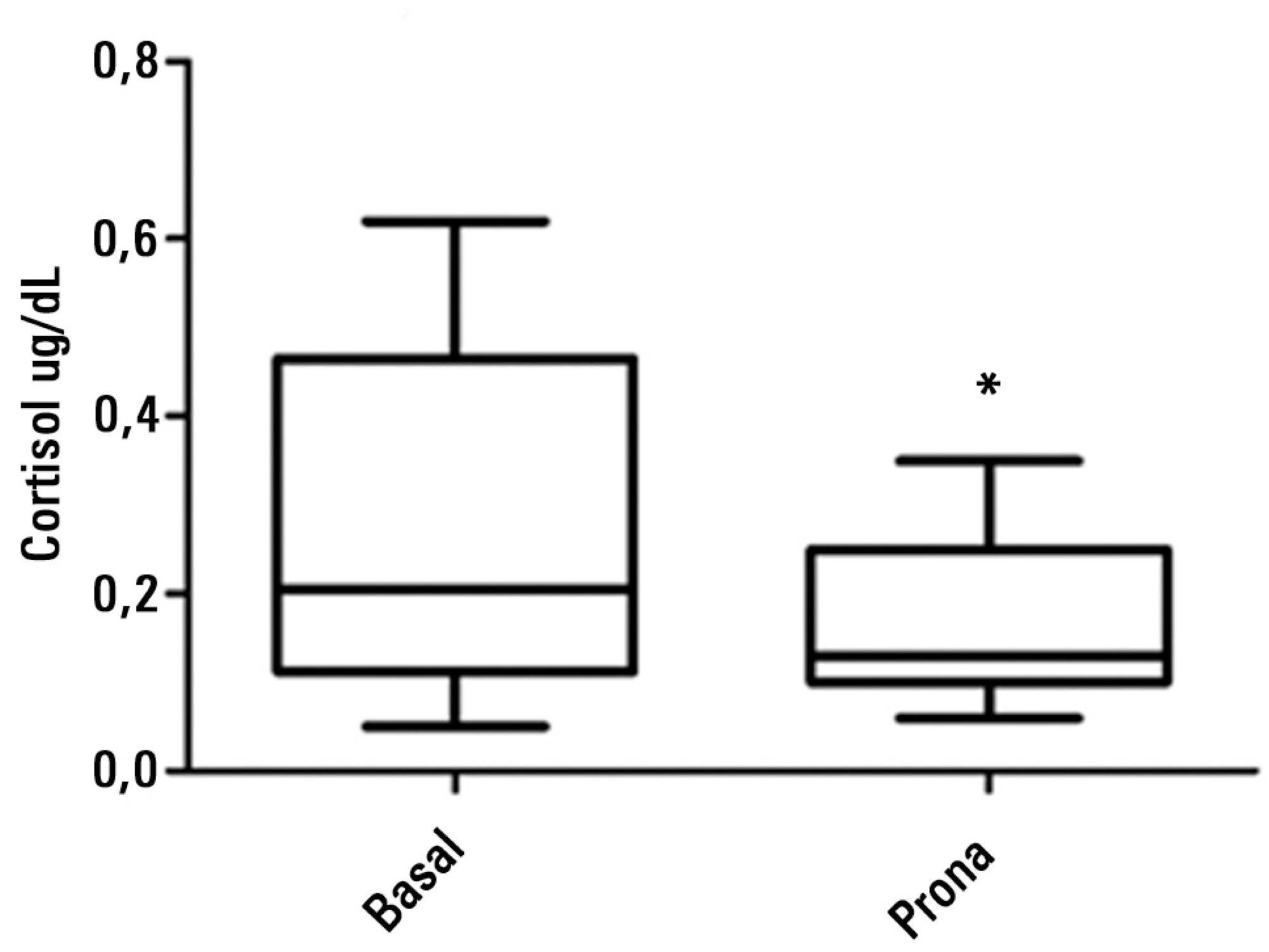
-
Review Articles
Antiphospholipid antibodies in critically ill patients
Rev Bras Ter Intensiva. 2014;26(2):176-182
Abstract
Review ArticlesAntiphospholipid antibodies in critically ill patients
Rev Bras Ter Intensiva. 2014;26(2):176-182
DOI 10.5935/0103-507X.20140026
Views0Antiphospholipid antibodies are responsible for a wide spectrum of clinical manifestations. Venous, arterial and microvascular thrombosis and severe catastrophic cases account for a large morbidly/mortality. Through the connection between the immune, inflammatory and hemostatic systems, it is possible that these antibodies may contribute to the development of organ dysfunction and are associated with poor short and long-term prognoses in critically ill patients. We performed a search of the PubMed/MedLine database for articles written during the period from January 2000 to February 2013 to evaluate the frequency of antiphospholipid antibodies in critically ill patients and their impact on the outcomes of these patients. Only eight original studies involving critically ill patients were found. However, the development of antiphospholipid antibodies in critically ill patients seems to be frequent, but more studies are necessary to clarify their pathogenic role and implications for clinical practice.
Keywords:Antibodies, antiphospholipidAntiphospholipid syndromeCatastrophic illnessCritical illnessIntensive care unitsMultiple organ failurePrognosisSee moreViews0Abstract
Review ArticlesAntiphospholipid antibodies in critically ill patients
Rev Bras Ter Intensiva. 2014;26(2):176-182
DOI 10.5935/0103-507X.20140026
Views0Antiphospholipid antibodies are responsible for a wide spectrum of clinical manifestations. Venous, arterial and microvascular thrombosis and severe catastrophic cases account for a large morbidly/mortality. Through the connection between the immune, inflammatory and hemostatic systems, it is possible that these antibodies may contribute to the development of organ dysfunction and are associated with poor short and long-term prognoses in critically ill patients. We performed a search of the PubMed/MedLine database for articles written during the period from January 2000 to February 2013 to evaluate the frequency of antiphospholipid antibodies in critically ill patients and their impact on the outcomes of these patients. Only eight original studies involving critically ill patients were found. However, the development of antiphospholipid antibodies in critically ill patients seems to be frequent, but more studies are necessary to clarify their pathogenic role and implications for clinical practice.
Keywords:Antibodies, antiphospholipidAntiphospholipid syndromeCatastrophic illnessCritical illnessIntensive care unitsMultiple organ failurePrognosisSee more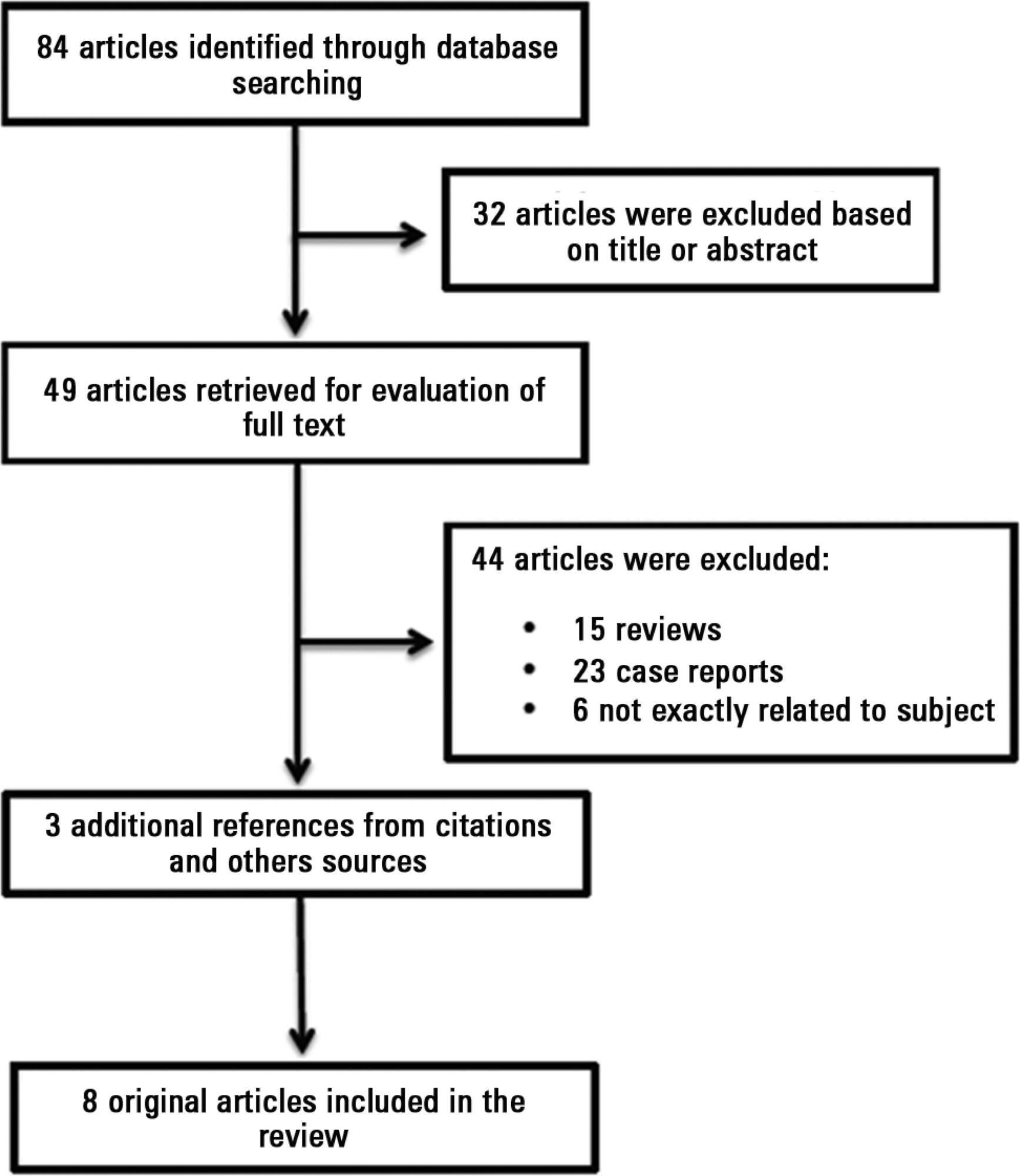
-
Estratégias de prevenção da lesão renal aguda em cirurgia cardíaca: revisão integrativa
Rev Bras Ter Intensiva. 2014;26(2):183-192
Abstract
Estratégias de prevenção da lesão renal aguda em cirurgia cardíaca: revisão integrativa
Rev Bras Ter Intensiva. 2014;26(2):183-192
DOI 10.5935/0103-507X.20140027
Views2See moreA lesão renal aguda é uma complicação frequente após cirurgia cardíaca, estando associada ao aumento de morbidade e mortalidade, e ao maior tempo de permanência em unidade de terapia intensiva. Considerando a alta prevalência e a associação da lesão renal aguda com o pior prognóstico, o desenvolvimento de estratégias de proteção renal torna-se indispensável, especialmente em pacientes com alto risco para o desenvolvimento de lesão renal aguda, como aqueles submetidos à cirurgia cardíaca, com o intuito de minimizar a incidência da lesão renal aguda no âmbito hospitalar, reduzindo, dessa forma, a alta morbimortalidade. A presente revisão integrativa teve por objetivo avaliar as evidências disponíveis na literatura sobre as intervenções mais eficazes na prevenção da lesão renal aguda em pacientes submetidos à cirurgia cardíaca. Para seleção dos artigos, utilizaram-se as bases de dados CINAHL e MedLine. A amostra desta revisão constituiu-se de 16 artigos. Após a análise dos artigos incluídos na revisão, os resultados dos estudos apontaram que apenas a hidratação com solução salina apresenta resultados consideráveis na prevenção de lesão renal aguda. As demais estratégias são controversas e necessitam de mais pesquisas para comprovar eficácia.
Views2Abstract
Estratégias de prevenção da lesão renal aguda em cirurgia cardíaca: revisão integrativa
Rev Bras Ter Intensiva. 2014;26(2):183-192
DOI 10.5935/0103-507X.20140027
Views2See moreA lesão renal aguda é uma complicação frequente após cirurgia cardíaca, estando associada ao aumento de morbidade e mortalidade, e ao maior tempo de permanência em unidade de terapia intensiva. Considerando a alta prevalência e a associação da lesão renal aguda com o pior prognóstico, o desenvolvimento de estratégias de proteção renal torna-se indispensável, especialmente em pacientes com alto risco para o desenvolvimento de lesão renal aguda, como aqueles submetidos à cirurgia cardíaca, com o intuito de minimizar a incidência da lesão renal aguda no âmbito hospitalar, reduzindo, dessa forma, a alta morbimortalidade. A presente revisão integrativa teve por objetivo avaliar as evidências disponíveis na literatura sobre as intervenções mais eficazes na prevenção da lesão renal aguda em pacientes submetidos à cirurgia cardíaca. Para seleção dos artigos, utilizaram-se as bases de dados CINAHL e MedLine. A amostra desta revisão constituiu-se de 16 artigos. Após a análise dos artigos incluídos na revisão, os resultados dos estudos apontaram que apenas a hidratação com solução salina apresenta resultados consideráveis na prevenção de lesão renal aguda. As demais estratégias são controversas e necessitam de mais pesquisas para comprovar eficácia.
-
Case Report
High-volume hemofiltration and prone ventilation in subarachnoid hemorrhage complicated by severe acute respiratory distress syndrome and refractory septic shock
Rev Bras Ter Intensiva. 2014;26(2):193-199
Abstract
Case ReportHigh-volume hemofiltration and prone ventilation in subarachnoid hemorrhage complicated by severe acute respiratory distress syndrome and refractory septic shock
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
Views0We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Keywords:acute respiratory distress syndromeCase reportsHemofiltration/methodsProne positionRespiration, artificialSeptic shockSubarachnoid hemorrhage/therapySee moreViews0Abstract
Case ReportHigh-volume hemofiltration and prone ventilation in subarachnoid hemorrhage complicated by severe acute respiratory distress syndrome and refractory septic shock
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
Views0We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Keywords:acute respiratory distress syndromeCase reportsHemofiltration/methodsProne positionRespiration, artificialSeptic shockSubarachnoid hemorrhage/therapySee more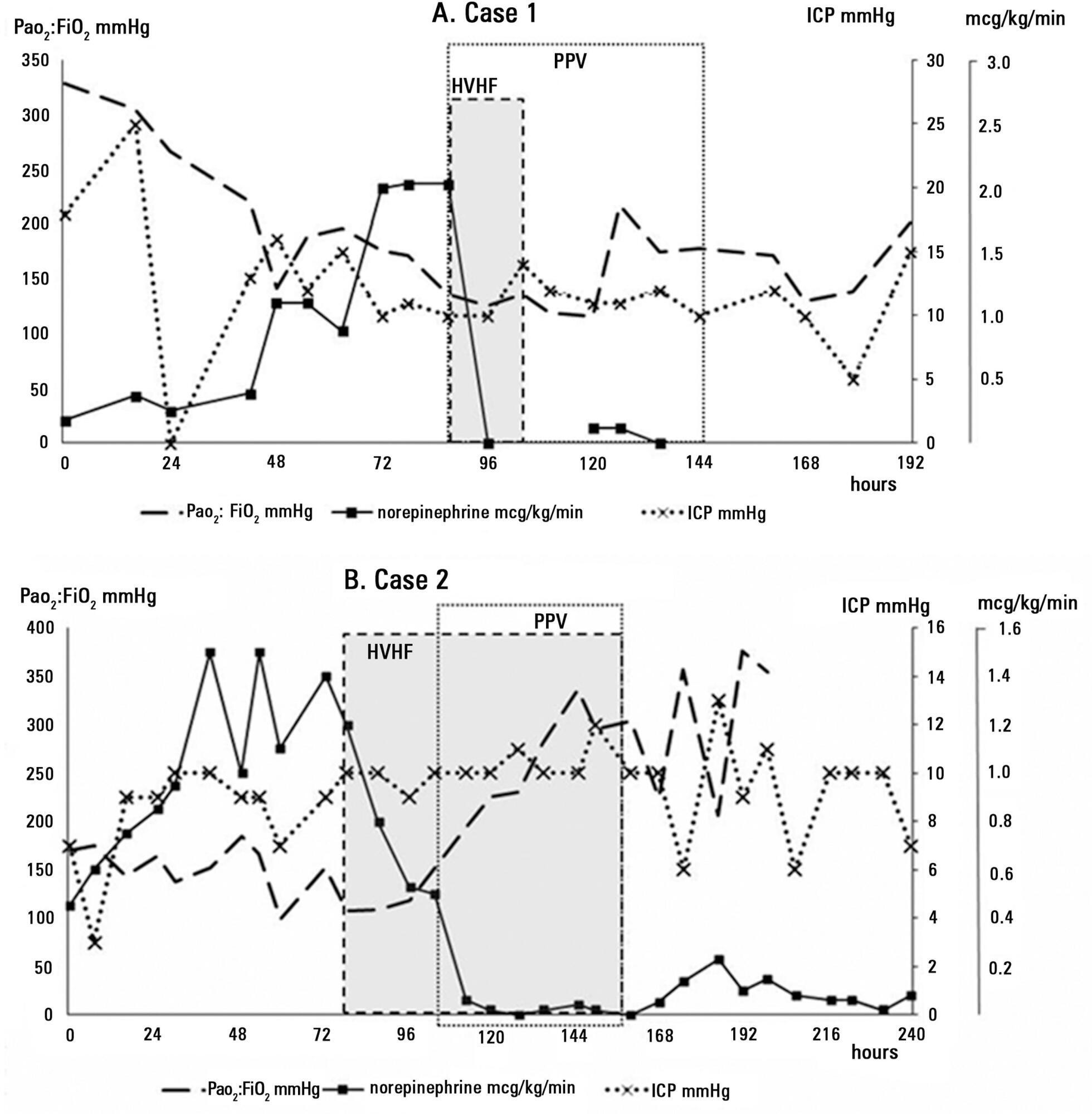
Volume Articles - Critical Care Science (CCS)
