-
Original Articles
Is the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
Abstract
Original ArticlesIs the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
DOI 10.5935/0103-507X.20140001
Views1Objective:
To evaluate the satisfaction of the intensive care unit staff with a computerized physician order entry and to compare the concept of the computerized physician order entry relevance among intensive care unit healthcare workers.
Methods:
We performed a cross-sectional survey to assess the satisfaction of the intensive care unit staff with the computerized physician order entry in a 30-bed medical/surgical adult intensive care unit using a self-administered questionnaire. The questions used for grading satisfaction levels were answered according to a numerical scale that ranged from 1 point (low satisfaction) to 10 points (high satisfaction).
Results:
The majority of the respondents (n=250) were female (66%) between the ages of 30 and 35 years of age (69%). The overall satisfaction with the computerized physician order entry scored 5.74±2.14 points. The satisfaction was lower among physicians (n=42) than among nurses, nurse technicians, respiratory therapists, clinical pharmacists and diet specialists (4.62±1.79 versus 5.97±2.14, p<0.001); satisfaction decreased with age (p<0.001). Physicians scored lower concerning the potential of the computerized physician order entry for improving patient safety (5.45±2.20 versus 8.09±2.21, p<0.001) and the ease of using the computerized physician order entry (3.83±1.88 versus 6.44±2.31, p<0.001). The characteristics independently associated with satisfaction were the system's user-friendliness, accuracy, capacity to provide clear information, and fast response time.
Conclusion:
Six months after its implementation, healthcare workers were satisfied, albeit not entirely, with the computerized physician order entry. The overall users’ satisfaction with computerized physician order entry was lower among physicians compared to other healthcare professionals. The factors associated with satisfaction included the belief that digitalization decreased the workload and contributed to the intensive care unit quality with a user-friendly and accurate system and that digitalization provided concise information within a reasonable time frame.
Keywords:Attitude of health personnelHealth care surveysJob satisfactionMedical order entry systemPhysician practice patternsSee moreViews1

Abstract
Original ArticlesIs the ICU staff satisfied with the computerized physician order entry? A cross-sectional survey study
Rev Bras Ter Intensiva. 2014;26(1):1-6
DOI 10.5935/0103-507X.20140001
Views1Objective:
To evaluate the satisfaction of the intensive care unit staff with a computerized physician order entry and to compare the concept of the computerized physician order entry relevance among intensive care unit healthcare workers.
Methods:
We performed a cross-sectional survey to assess the satisfaction of the intensive care unit staff with the computerized physician order entry in a 30-bed medical/surgical adult intensive care unit using a self-administered questionnaire. The questions used for grading satisfaction levels were answered according to a numerical scale that ranged from 1 point (low satisfaction) to 10 points (high satisfaction).
Results:
The majority of the respondents (n=250) were female (66%) between the ages of 30 and 35 years of age (69%). The overall satisfaction with the computerized physician order entry scored 5.74±2.14 points. The satisfaction was lower among physicians (n=42) than among nurses, nurse technicians, respiratory therapists, clinical pharmacists and diet specialists (4.62±1.79 versus 5.97±2.14, p<0.001); satisfaction decreased with age (p<0.001). Physicians scored lower concerning the potential of the computerized physician order entry for improving patient safety (5.45±2.20 versus 8.09±2.21, p<0.001) and the ease of using the computerized physician order entry (3.83±1.88 versus 6.44±2.31, p<0.001). The characteristics independently associated with satisfaction were the system's user-friendliness, accuracy, capacity to provide clear information, and fast response time.
Conclusion:
Six months after its implementation, healthcare workers were satisfied, albeit not entirely, with the computerized physician order entry. The overall users’ satisfaction with computerized physician order entry was lower among physicians compared to other healthcare professionals. The factors associated with satisfaction included the belief that digitalization decreased the workload and contributed to the intensive care unit quality with a user-friendly and accurate system and that digitalization provided concise information within a reasonable time frame.
Keywords:Attitude of health personnelHealth care surveysJob satisfactionMedical order entry systemPhysician practice patternsSee more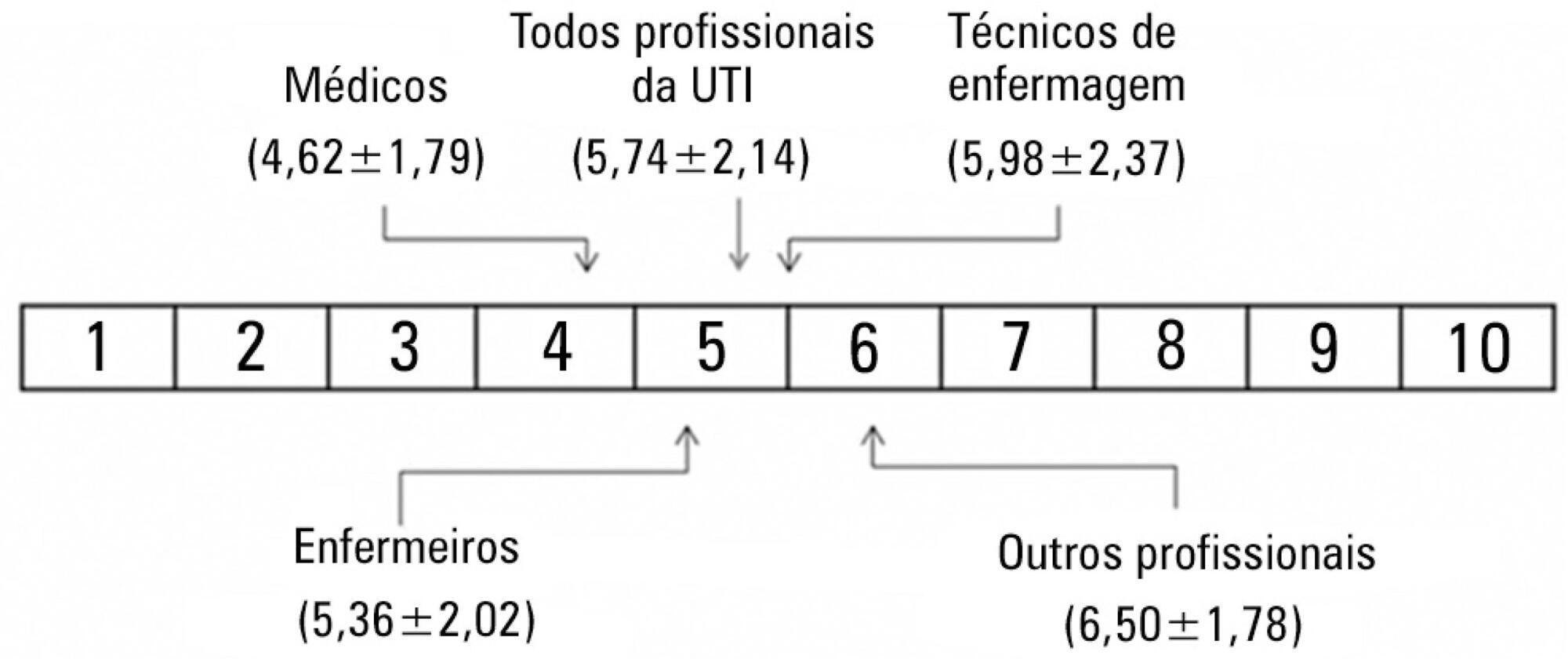
-
Original Articles
Impact of a continuous education program on the quality of assistance offered by intensive care physiotherapy
Rev Bras Ter Intensiva. 2014;26(1):7-13
Abstract
Original ArticlesImpact of a continuous education program on the quality of assistance offered by intensive care physiotherapy
Rev Bras Ter Intensiva. 2014;26(1):7-13
DOI 10.5935/0103-507X.20140002
Views0Objective:
To evaluate the role of quality indicators and adverse events registering in the quality assessment of intensive care physiotherapy and to evaluate the impact of implementing protocolized care and professional training in the quality improvement process.
Methods:
A prospective before-after study was designed to assess 15 indicators of the quality of care. Baseline compliance and adverse events were collected before and after the implementation of treatment protocols and staff training.
Results:
Eighty-nine patients admitted, being 48 in the pre-intervention period and 41 in the post-intervention period with a total of 1246 and 1191 observations respectively. Among the indicators related to the global population, there was a significant improvement in chest x-ray control, multidisciplinary rounds and shift changes as well as in compliance with these decisions. Indicators related to the population under mechanical ventilation, obtained by direct observation at bedside, showed a significant improvement in the compliance with the tidal volume of 6-8mL/Kg, plateau pressure <30cmH2O, adequate mechanical ventilation alarm setting, mechanical ventilation humidification control, adequate humidification line exchange and orotracheal tube position. Among the mechanical ventilation indicators collected through the physiotherapy records, there was significantly improved compliance with the predicted tidal volume registry and cuff pressure registry. There was a significant reduction in the number of adverse events. There was no impact on intensive care unit mortality, length of stay, duration of mechanical ventilation and ventilator-free days.
Conclusion:
It is possible to measure the quality of physiotherapy care using indicators of quality control. The implementation of care protocols and training of the professionals can improve team performance.
Keywords:Education, continuingIndicators of health serviceIntensive carePhysical therapy modalitiesQuality improvementQuality managementRespiratory therapySee moreViews0Abstract
Original ArticlesImpact of a continuous education program on the quality of assistance offered by intensive care physiotherapy
Rev Bras Ter Intensiva. 2014;26(1):7-13
DOI 10.5935/0103-507X.20140002
Views0Objective:
To evaluate the role of quality indicators and adverse events registering in the quality assessment of intensive care physiotherapy and to evaluate the impact of implementing protocolized care and professional training in the quality improvement process.
Methods:
A prospective before-after study was designed to assess 15 indicators of the quality of care. Baseline compliance and adverse events were collected before and after the implementation of treatment protocols and staff training.
Results:
Eighty-nine patients admitted, being 48 in the pre-intervention period and 41 in the post-intervention period with a total of 1246 and 1191 observations respectively. Among the indicators related to the global population, there was a significant improvement in chest x-ray control, multidisciplinary rounds and shift changes as well as in compliance with these decisions. Indicators related to the population under mechanical ventilation, obtained by direct observation at bedside, showed a significant improvement in the compliance with the tidal volume of 6-8mL/Kg, plateau pressure <30cmH2O, adequate mechanical ventilation alarm setting, mechanical ventilation humidification control, adequate humidification line exchange and orotracheal tube position. Among the mechanical ventilation indicators collected through the physiotherapy records, there was significantly improved compliance with the predicted tidal volume registry and cuff pressure registry. There was a significant reduction in the number of adverse events. There was no impact on intensive care unit mortality, length of stay, duration of mechanical ventilation and ventilator-free days.
Conclusion:
It is possible to measure the quality of physiotherapy care using indicators of quality control. The implementation of care protocols and training of the professionals can improve team performance.
Keywords:Education, continuingIndicators of health serviceIntensive carePhysical therapy modalitiesQuality improvementQuality managementRespiratory therapySee more -
Original Articles
Augmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
Abstract
Original ArticlesAugmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
DOI 10.5935/0103-507X.20140003
Views8Objective:
An augmented renal clearance has been described in some groups of critically ill patients, and it might induce sub-optimal concentrations of drugs eliminated by glomerular filtration, mainly antibiotics. Studies on its occurrence and determinants are lacking. Our goals were to determine the incidence and associated factors of augmented renal clearance and the effects on vancomycin concentrations and dosing in a series of intensive care unit patients.
Methods:
We prospectively studied 363 patients admitted during 1 year to a clinical-surgical intensive care unit. Patients with serum creatinine >1.3mg/dL were excluded. Creatinine clearance was calculated from a 24-hour urine collection. Patients were grouped according to the presence of augmented renal clearance (creatinine clearance >120mL/min/1.73m2), and possible risk factors were analyzed with bivariate and logistic regression analysis. In patients treated with vancomycin, dosage and plasma concentrations were registered.
Results:
Augmented renal clearance was present in 103 patients (28%); they were younger (48±15 versus 65±17 years, p<0.0001), had more frequent obstetric (16 versus 7%, p=0.0006) and trauma admissions (10 versus 3%, p=0.016) and fewer comorbidities. The only independent determinants for the development of augmented renal clearance were age (OR 0.95; p<0.0001; 95%CI 0.93-0.96) and absence of diabetes (OR 0.34; p=0.03; 95%CI 0.12-0.92). Twelve of the 46 patients who received vancomycin had augmented renal clearance and despite higher doses, had lower concentrations.
Conclusions:
In this cohort of critically ill patients, augmented renal clearance was a common finding. Age and absence of diabetes were the only independent determinants. Therefore, younger and previously healthy patients might require larger vancomycin dosing.
Keywords:CreatinineMetabolic clearance rateSepsis/drug therapyVancomycin/pharmacokineticsVancomycin/therapeutic useSee moreViews8Abstract
Original ArticlesAugmented renal clearance in critically ill patients: incidence, associated factors and effects on vancomycin treatment
Rev Bras Ter Intensiva. 2014;26(1):13-20
DOI 10.5935/0103-507X.20140003
Views8Objective:
An augmented renal clearance has been described in some groups of critically ill patients, and it might induce sub-optimal concentrations of drugs eliminated by glomerular filtration, mainly antibiotics. Studies on its occurrence and determinants are lacking. Our goals were to determine the incidence and associated factors of augmented renal clearance and the effects on vancomycin concentrations and dosing in a series of intensive care unit patients.
Methods:
We prospectively studied 363 patients admitted during 1 year to a clinical-surgical intensive care unit. Patients with serum creatinine >1.3mg/dL were excluded. Creatinine clearance was calculated from a 24-hour urine collection. Patients were grouped according to the presence of augmented renal clearance (creatinine clearance >120mL/min/1.73m2), and possible risk factors were analyzed with bivariate and logistic regression analysis. In patients treated with vancomycin, dosage and plasma concentrations were registered.
Results:
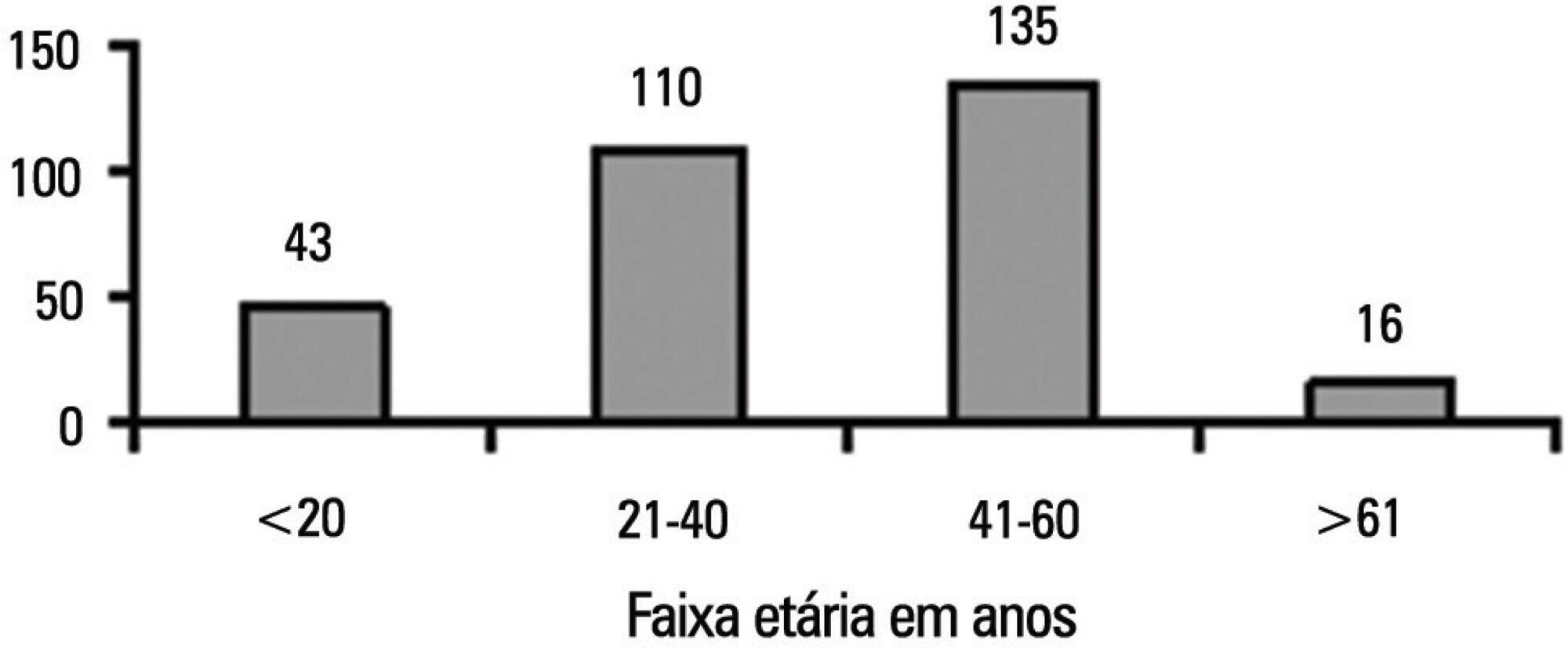
Augmented renal clearance was present in 103 patients (28%); they were younger (48±15 versus 65±17 years, p<0.0001), had more frequent obstetric (16 versus 7%, p=0.0006) and trauma admissions (10 versus 3%, p=0.016) and fewer comorbidities. The only independent determinants for the development of augmented renal clearance were age (OR 0.95; p<0.0001; 95%CI 0.93-0.96) and absence of diabetes (OR 0.34; p=0.03; 95%CI 0.12-0.92). Twelve of the 46 patients who received vancomycin had augmented renal clearance and despite higher doses, had lower concentrations.
Conclusions:
In this cohort of critically ill patients, augmented renal clearance was a common finding. Age and absence of diabetes were the only independent determinants. Therefore, younger and previously healthy patients might require larger vancomycin dosing.
Keywords:CreatinineMetabolic clearance rateSepsis/drug therapyVancomycin/pharmacokineticsVancomycin/therapeutic useSee more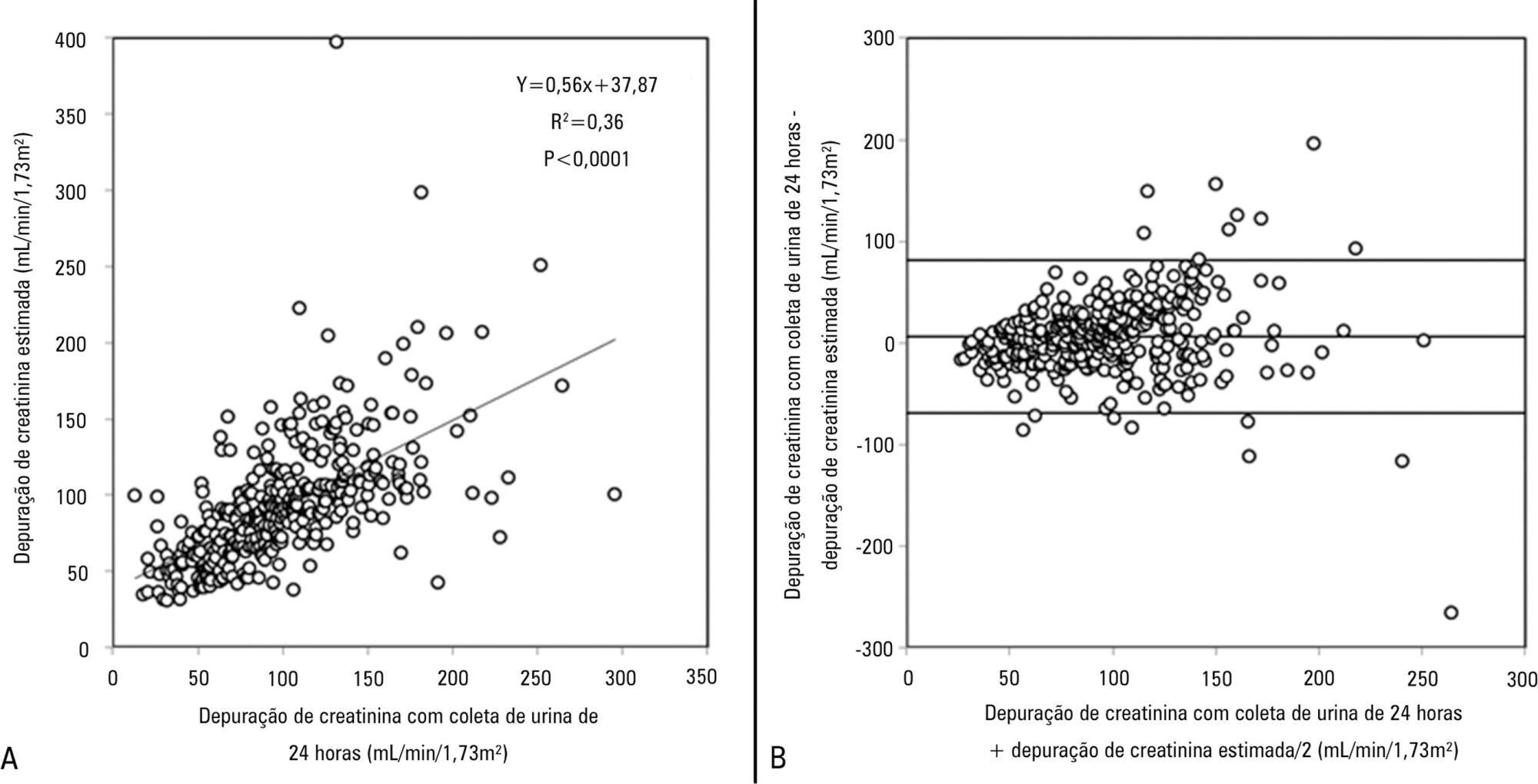
-
Original Articles
Profile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
Abstract
Original ArticlesProfile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
DOI 10.5935/0103-507X.20140004
Views0See moreObjective:
To characterize the profile of effective organ and tissue donors and to understand which organs and tissues were donated for transplantation.
Methods:
This was a quantitative, descriptive, exploratory, retrospective study that analyzed clinical data from 305 donors between January 2006 to December 2010. The data were then analyzed using descriptive analyses, generating frequency tables, measures of position (mean, minimum and maximum) and measures of dispersion (standard deviation) for data that was social and clinical in nature.
Results:
There was an overall predominance of white (72%) and male (55%) individuals between the ages of 41 and 60 years (44%). The primary cause of brain death was cerebrovascular accident (55%). In the patient history, 31% of the patients were classified as overweight, 27% as hypertensive and only 4.3% as having diabetes mellitus. Vasoactive drugs were used in 92.7% of the donors, and the main drug of choice was noradrenaline (81.6%). Hyperglycemia and hypernatremia were diagnosed in 78% and 71% of the donors, respectively.
Conclusion:
Significant hemodynamic changes were found, and the results indicate that the use of vasoactive drugs was the main strategy used to control these changes. Furthermore, most donors presented with hyperglycemia and hypernatremia, which were frequently reported in association with brain death. The persistent nature of these findings suggests that the organ donors were inadequately maintained.
Views0Abstract
Original ArticlesProfile of effective donors from organ and tissue procurement services
Rev Bras Ter Intensiva. 2014;26(1):21-27
DOI 10.5935/0103-507X.20140004
Views0See moreObjective:
To characterize the profile of effective organ and tissue donors and to understand which organs and tissues were donated for transplantation.
Methods:
This was a quantitative, descriptive, exploratory, retrospective study that analyzed clinical data from 305 donors between January 2006 to December 2010. The data were then analyzed using descriptive analyses, generating frequency tables, measures of position (mean, minimum and maximum) and measures of dispersion (standard deviation) for data that was social and clinical in nature.
Results:
There was an overall predominance of white (72%) and male (55%) individuals between the ages of 41 and 60 years (44%). The primary cause of brain death was cerebrovascular accident (55%). In the patient history, 31% of the patients were classified as overweight, 27% as hypertensive and only 4.3% as having diabetes mellitus. Vasoactive drugs were used in 92.7% of the donors, and the main drug of choice was noradrenaline (81.6%). Hyperglycemia and hypernatremia were diagnosed in 78% and 71% of the donors, respectively.
Conclusion:
Significant hemodynamic changes were found, and the results indicate that the use of vasoactive drugs was the main strategy used to control these changes. Furthermore, most donors presented with hyperglycemia and hypernatremia, which were frequently reported in association with brain death. The persistent nature of these findings suggests that the organ donors were inadequately maintained.
-
Original Articles
Reaction time of a health care team to monitoring alarms in the intensive care unit: implications for the safety of seriously ill patients
Rev Bras Ter Intensiva. 2014;26(1):28-35
Abstract
Original ArticlesReaction time of a health care team to monitoring alarms in the intensive care unit: implications for the safety of seriously ill patients
Rev Bras Ter Intensiva. 2014;26(1):28-35
DOI 10.5935/0103-507X.20140005
Views0Objective:
To define the characteristics and measure the reaction time of a health care team monitoring alarms in the intensive care unit.
Methods:
A quantitative, observational, and descriptive study developed at the coronary care unit of a cardiology public hospital in Rio de Janeiro state (RJ). Data were obtained from the information collected on the patients, the monitoring used, and the measurement of the team’s reaction time to the alarms of multi-parameter monitors during a non-participatory field observation.
Results:
Eighty-eight patients were followed (49 during the day shift and 39 during the night shift). During the 40 hours of observation (20 hours during the day shift and 20 hours during the night shift), the total number of monitoring alarms was 227, with 106 alarms during the day shift and 121 during the night shift, an average of 5.7 alarms/hour. In total, 145 alarms unanswered by the team were observed, with 68 occurring during the day shift (64.15%) and 77 during the night shift (63.64%). This study demonstrated that the reaction time was longer than 10 minutes in more than 60% of the alarms, which were considered as unanswered alarms. The median reaction time of the answered alarms was 4 minutes and 54 seconds during the day shift and 4 minutes and 55 seconds during the night shift. The respiration monitoring was activated in only nine patients (23.07%) during the night shift. Regarding the alarm quality of these variables, the arrhythmia alarm was qualified in only 10 (20.40%) of the day-shift patients and the respiration alarm in four night-shift patients (44.44%).
Conclusion:
The programming and configuration of the physiological variables monitored and the parameters of alarms in the intensive care unit were inadequate; there was a delay and lack of response to the alarms, suggesting that relevant alarms may have been ignored by the health care team, thus compromising the patient safety.
Keywords:Clinical alarmsEquipament failureIntensive care unitsIntensive care/standardsMonitoring, physiologic/instrumentationPatient safetySee moreViews0Abstract
Original ArticlesReaction time of a health care team to monitoring alarms in the intensive care unit: implications for the safety of seriously ill patients
Rev Bras Ter Intensiva. 2014;26(1):28-35
DOI 10.5935/0103-507X.20140005
Views0Objective:
To define the characteristics and measure the reaction time of a health care team monitoring alarms in the intensive care unit.
Methods:
A quantitative, observational, and descriptive study developed at the coronary care unit of a cardiology public hospital in Rio de Janeiro state (RJ). Data were obtained from the information collected on the patients, the monitoring used, and the measurement of the team’s reaction time to the alarms of multi-parameter monitors during a non-participatory field observation.
Results:
Eighty-eight patients were followed (49 during the day shift and 39 during the night shift). During the 40 hours of observation (20 hours during the day shift and 20 hours during the night shift), the total number of monitoring alarms was 227, with 106 alarms during the day shift and 121 during the night shift, an average of 5.7 alarms/hour. In total, 145 alarms unanswered by the team were observed, with 68 occurring during the day shift (64.15%) and 77 during the night shift (63.64%). This study demonstrated that the reaction time was longer than 10 minutes in more than 60% of the alarms, which were considered as unanswered alarms. The median reaction time of the answered alarms was 4 minutes and 54 seconds during the day shift and 4 minutes and 55 seconds during the night shift. The respiration monitoring was activated in only nine patients (23.07%) during the night shift. Regarding the alarm quality of these variables, the arrhythmia alarm was qualified in only 10 (20.40%) of the day-shift patients and the respiration alarm in four night-shift patients (44.44%).
Conclusion:
The programming and configuration of the physiological variables monitored and the parameters of alarms in the intensive care unit were inadequate; there was a delay and lack of response to the alarms, suggesting that relevant alarms may have been ignored by the health care team, thus compromising the patient safety.
Keywords:Clinical alarmsEquipament failureIntensive care unitsIntensive care/standardsMonitoring, physiologic/instrumentationPatient safetySee more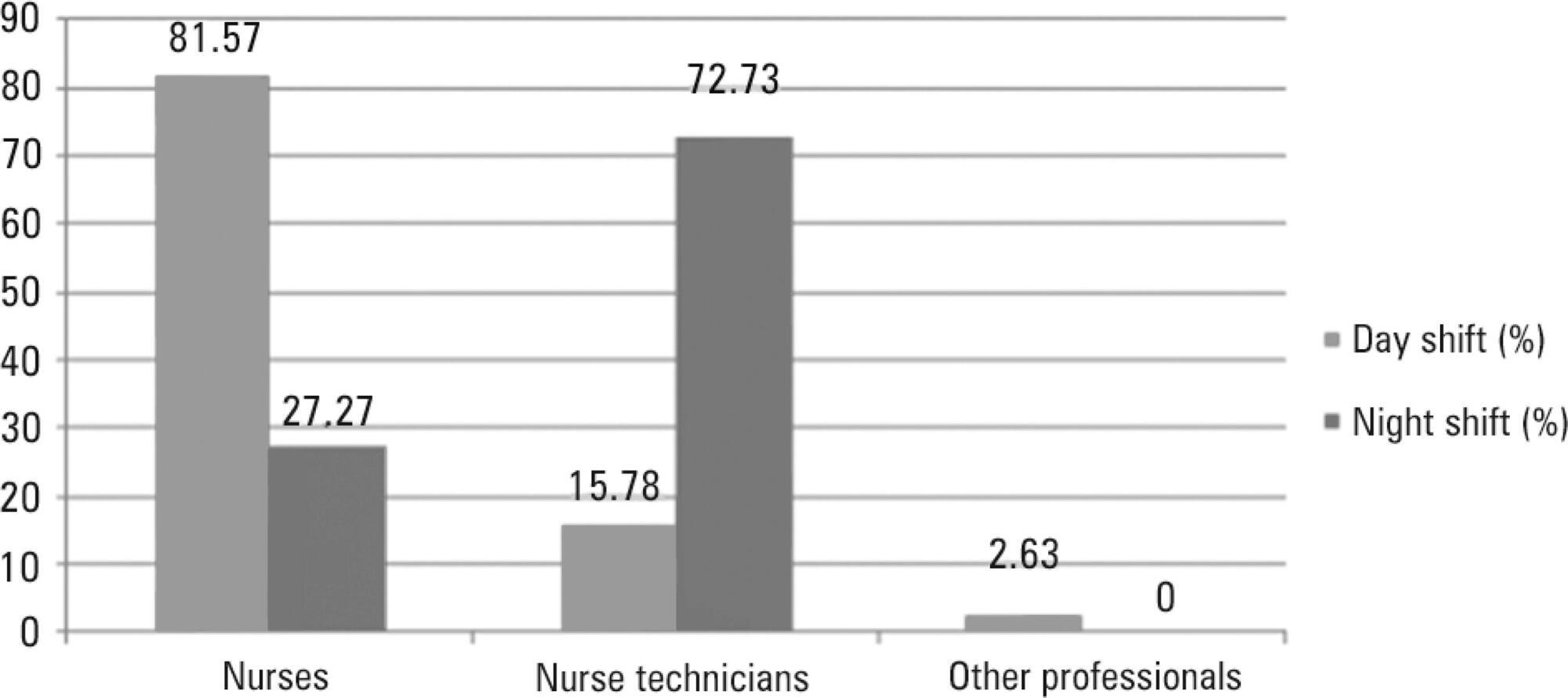
-
Original Articles
Use of scores to calculate the nursing workload in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):36-43
Abstract
Original ArticlesUse of scores to calculate the nursing workload in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):36-43
DOI 10.5935/0103-507X.20140006
Views0See moreObjective:
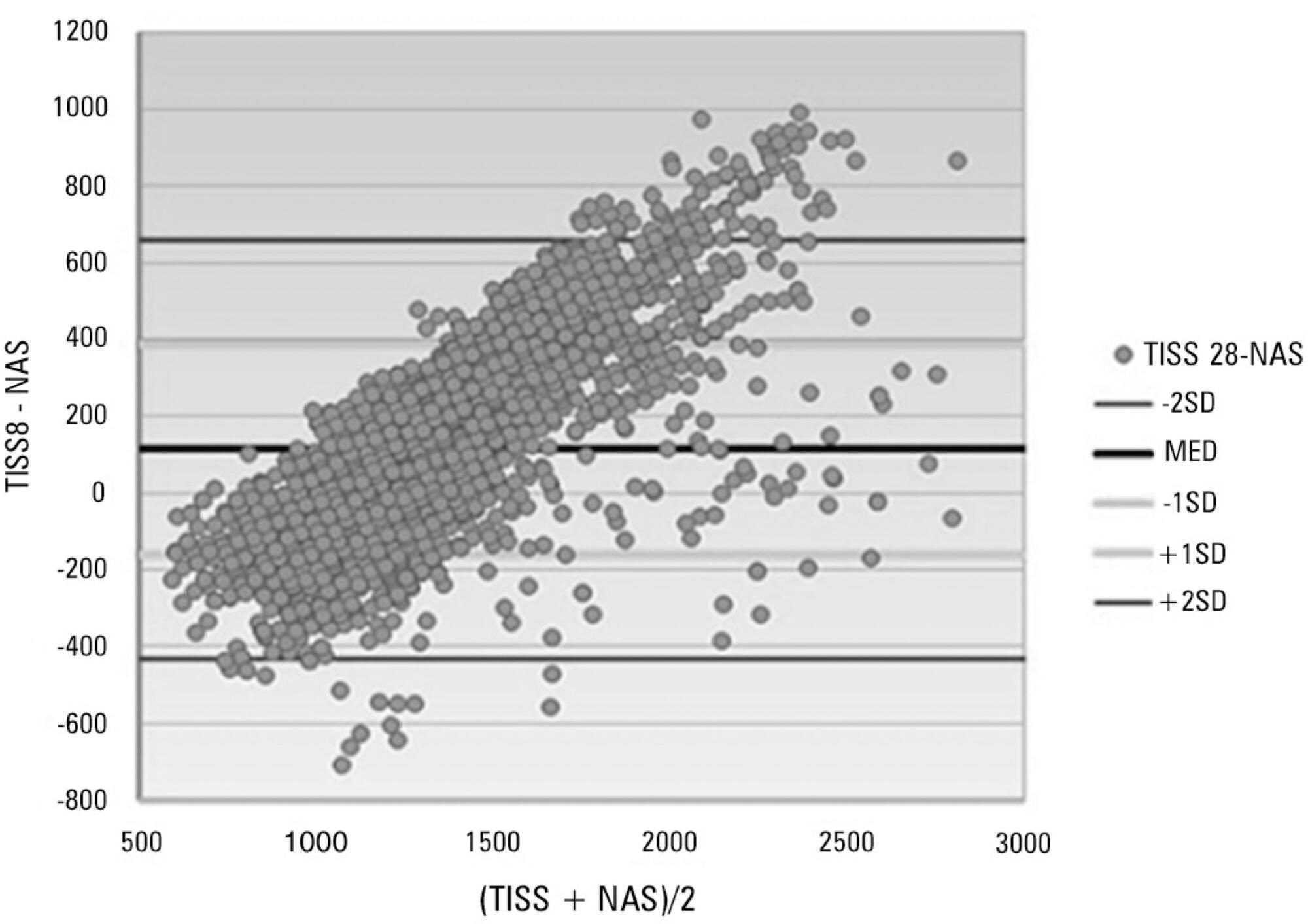
To assess the performance of the Nursing Activities Score in a pediatric intensive care unit, compare its scores expressed as time spent on nursing activities to the corresponding ones calculated using the Simplified Therapeutic Intervention Scoring System, and correlate the results obtained by both instruments with severity, morbidity and mortality.
Methods:
Prospective, observational, and analytical cohort study conducted at a type III general pediatric intensive care unit. The study participants were all the children aged 29 days to 12 years admitted to the investigated pediatric intensive care unit from August 2008 to February 2009.
Results:
A total of 545 patients were studied, which corresponded to 2,951 assessments. The average score of the Simplified Therapeutic Intervention Scoring System was 28.79±10.37 (915±330 minutes), and that of the Nursing Activities Score was 55.6±11.82 (802±161 minutes). The number of minutes that resulted from the conversion of the Simplified Therapeutic Intervention Scoring System score was higher compared to that resulting from the Nursing Activities Score for all the assessments (p<0.001). The correlation between the instruments was significant, direct, positive, and moderate (R=0.564).
Conclusions:
The agreement between the investigated instruments was satisfactory, and both instruments also exhibited satisfactory discrimination of mortality; for that purpose, the best cutoff point was 16 nursing hours/patient day.
Views0Abstract
Original ArticlesUse of scores to calculate the nursing workload in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):36-43
DOI 10.5935/0103-507X.20140006
Views0See moreObjective:
To assess the performance of the Nursing Activities Score in a pediatric intensive care unit, compare its scores expressed as time spent on nursing activities to the corresponding ones calculated using the Simplified Therapeutic Intervention Scoring System, and correlate the results obtained by both instruments with severity, morbidity and mortality.
Methods:
Prospective, observational, and analytical cohort study conducted at a type III general pediatric intensive care unit. The study participants were all the children aged 29 days to 12 years admitted to the investigated pediatric intensive care unit from August 2008 to February 2009.
Results:
A total of 545 patients were studied, which corresponded to 2,951 assessments. The average score of the Simplified Therapeutic Intervention Scoring System was 28.79±10.37 (915±330 minutes), and that of the Nursing Activities Score was 55.6±11.82 (802±161 minutes). The number of minutes that resulted from the conversion of the Simplified Therapeutic Intervention Scoring System score was higher compared to that resulting from the Nursing Activities Score for all the assessments (p<0.001). The correlation between the instruments was significant, direct, positive, and moderate (R=0.564).
Conclusions:
The agreement between the investigated instruments was satisfactory, and both instruments also exhibited satisfactory discrimination of mortality; for that purpose, the best cutoff point was 16 nursing hours/patient day.
-
Original Articles
Performance of the Pediatric Index of Mortality 2 in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):44-50
Abstract
Original ArticlesPerformance of the Pediatric Index of Mortality 2 in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):44-50
DOI 10.5935/0103-507X.20140007
Views0Objective:
To assess the discrimination and calibration of the Pediatric Index of Mortality 2 in patients admitted to a pediatric intensive care unit.
Methods:
The study was conducted with a contemporary cohort from November 2005 to November 2006. Patients aged 29 days to 18 years were included in the study. Patients who died within 12 hours of admission and cases of readmission were excluded from the study. The performance of the Pediatric Index of Mortality 2 was assessed by means of the Hosmer-Lemeshow goodness-of-fit test, the standardized mortality ratio and the area under receiver operating characteristic (ROC) curve with 95% confidence interval. The significance level was established as 5%.
Results:
A total of 276 admissions to the pediatric intensive care unit were included in the analysis. The mortality rate was 14.13%, and the efficiency of admission 0.88%. The median age of the sample was 42.22 months, and most participants were male (60.1%). Most admissions were referrals from the emergency department. The mean duration of stay in pediatric intensive care unit was 6.43±5.23 days. Approximately 72.46% of admissions were for clinical reasons and exhibited an association with the outcome death (odds ratio: 2.9; 95%CI: 1.09-7.74; p=0.017). Calibration of the Pediatric Index of Mortality 2 with the chi-square statistic was 12.2686 (p=0.1396) in the Hosmer-Lemeshow goodness-of-fit test, and the standardized mortality ratio was 1.0. The area under the ROC curve assessing model discrimination was 0.778.
Conclusion:
Pediatric Index of Mortality 2 exhibited satisfactory performance.
Keywords:ChildIntensive care units, pediatricMortalityOutcomes assessment (Health care)Quality indicators, health careRisk assessmentSee moreViews0Abstract
Original ArticlesPerformance of the Pediatric Index of Mortality 2 in a pediatric intensive care unit
Rev Bras Ter Intensiva. 2014;26(1):44-50
DOI 10.5935/0103-507X.20140007
Views0Objective:
To assess the discrimination and calibration of the Pediatric Index of Mortality 2 in patients admitted to a pediatric intensive care unit.
Methods:
The study was conducted with a contemporary cohort from November 2005 to November 2006. Patients aged 29 days to 18 years were included in the study. Patients who died within 12 hours of admission and cases of readmission were excluded from the study. The performance of the Pediatric Index of Mortality 2 was assessed by means of the Hosmer-Lemeshow goodness-of-fit test, the standardized mortality ratio and the area under receiver operating characteristic (ROC) curve with 95% confidence interval. The significance level was established as 5%.
Results:
A total of 276 admissions to the pediatric intensive care unit were included in the analysis. The mortality rate was 14.13%, and the efficiency of admission 0.88%. The median age of the sample was 42.22 months, and most participants were male (60.1%). Most admissions were referrals from the emergency department. The mean duration of stay in pediatric intensive care unit was 6.43±5.23 days. Approximately 72.46% of admissions were for clinical reasons and exhibited an association with the outcome death (odds ratio: 2.9; 95%CI: 1.09-7.74; p=0.017). Calibration of the Pediatric Index of Mortality 2 with the chi-square statistic was 12.2686 (p=0.1396) in the Hosmer-Lemeshow goodness-of-fit test, and the standardized mortality ratio was 1.0. The area under the ROC curve assessing model discrimination was 0.778.
Conclusion:
Pediatric Index of Mortality 2 exhibited satisfactory performance.
Keywords:ChildIntensive care units, pediatricMortalityOutcomes assessment (Health care)Quality indicators, health careRisk assessmentSee more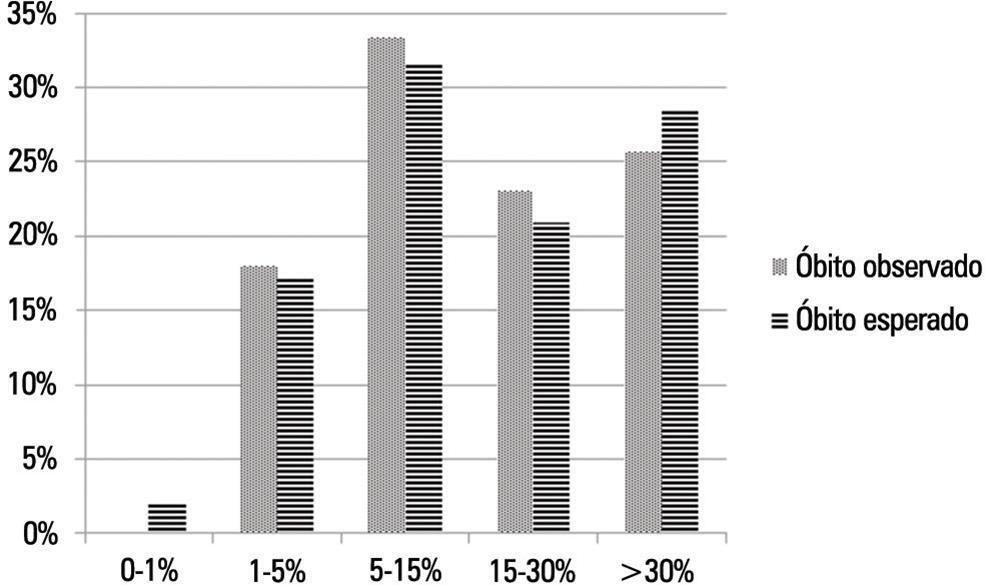
-
Original Articles
Predictors of extubation failure and reintubation in newborn infants subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2014;26(1):51-56
Abstract
Original ArticlesPredictors of extubation failure and reintubation in newborn infants subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2014;26(1):51-56
DOI 10.5935/0103-507X.20140008
Views0Objective:
To identify risk factors for extubation failure and reintubation in newborn infants subjected to mechanical ventilation and to establish whether ventilation parameters and blood gas analysis behave as predictors of those outcomes.
Methods:
Prospective study conducted at a neonatal intensive care unit from May to November 2011. A total of 176 infants of both genders subjected to mechanical ventilation were assessed after extubation. Extubation failure was defined as the need to resume mechanical ventilation within less than 72 hours. Reintubation was defined as the need to reintubate the infants any time after the first 72 hours.
Results:
Based on the univariate analysis, the variables gestational age <28 weeks, birth weight <1,000g and low Apgar scores were associated with extubation failure and reintubation. Based on the multivariate analysis, the variables length of mechanical ventilation (days), potential of hydrogen (pH) and partial pressure of oxygen (pO2) remained associated with extubation failure, and the five-minute Apgar score and age at extubation were associated with reintubation.
Conclusion:
Low five-minute Apgar scores, age at extubation, length of mechanical ventilation, acid-base disorders and hyperoxia exhibited associations with the investigated outcomes of extubation failure and reintubation.
Keywords:InfantInfant, newbornIntubation, intratracheal/adverse effectsprematureRespiration, artificialTreatment failureVentilator weaning/adverse effectsSee moreViews0Abstract
Original ArticlesPredictors of extubation failure and reintubation in newborn infants subjected to mechanical ventilation
Rev Bras Ter Intensiva. 2014;26(1):51-56
DOI 10.5935/0103-507X.20140008
Views0Objective:
To identify risk factors for extubation failure and reintubation in newborn infants subjected to mechanical ventilation and to establish whether ventilation parameters and blood gas analysis behave as predictors of those outcomes.
Methods:
Prospective study conducted at a neonatal intensive care unit from May to November 2011. A total of 176 infants of both genders subjected to mechanical ventilation were assessed after extubation. Extubation failure was defined as the need to resume mechanical ventilation within less than 72 hours. Reintubation was defined as the need to reintubate the infants any time after the first 72 hours.
Results:
Based on the univariate analysis, the variables gestational age <28 weeks, birth weight <1,000g and low Apgar scores were associated with extubation failure and reintubation. Based on the multivariate analysis, the variables length of mechanical ventilation (days), potential of hydrogen (pH) and partial pressure of oxygen (pO2) remained associated with extubation failure, and the five-minute Apgar score and age at extubation were associated with reintubation.
Conclusion:
Low five-minute Apgar scores, age at extubation, length of mechanical ventilation, acid-base disorders and hyperoxia exhibited associations with the investigated outcomes of extubation failure and reintubation.
Keywords:InfantInfant, newbornIntubation, intratracheal/adverse effectsprematureRespiration, artificialTreatment failureVentilator weaning/adverse effectsSee more -
Original Articles
Availability of physical therapy assistance in neonatal intensive care units in the city of São Paulo, Brazil
Rev Bras Ter Intensiva. 2014;26(1):57-64
Abstract
Original ArticlesAvailability of physical therapy assistance in neonatal intensive care units in the city of São Paulo, Brazil
Rev Bras Ter Intensiva. 2014;26(1):57-64
DOI 10.5935/0103-507X.20140009
Views0Objective:
To describe the characteristics of physical therapy assistance to newborns and to provide a profile of physical therapists working in intensive care units in the city of São Paulo, Brazil.
Methods:
This cross-sectional study was conducted in every hospital in São Paulo city that had at least one intensive care unit bed for newborns registered at the National Registry of Health Establishments in 2010. In each unit, three types of physical therapists were included: an executive who was responsible for the physical therapy service in that hospital (chief-physical therapists), a physical therapist who was responsible for the physical therapy assistance in the neonatal unit (reference-physical therapists), and a randomly selected physical therapist who was directly involved in the neonatal care (care-physical therapists).
Results:
Among the 67 hospitals eligible for the study, 63 (94.0%) had a physical therapy service. Of those hospitals, three (4.8%) refused to participate. Thus, 60 chief-PTs, 52 reference-physical therapists, and 44 care-physical therapists were interviewed. During day shifts, night shifts, and weekends/holidays, there were no physical therapists in 1.7%, 45.0%, and 13.3% of the intensive care units, respectively. Physical therapy assistance was available for 17.8±7.2 hours/day, and each physical therapist cared for 9.4±2.6 newborns during six working hours. Most professionals had completed at least one specialization course.
Conclusion:
Most neonatal intensive care units in the city of São Paulo had physical therapists working on the day shift. However, other shifts had incomplete staff with less than 18 hours of available physical therapy assistance per day.
Keywords:Infant, newbornInfant, prematureIntensive care unitsPhysical therapy department, hospitalPhysical therapy modalitiesSee moreViews0Abstract
Original ArticlesAvailability of physical therapy assistance in neonatal intensive care units in the city of São Paulo, Brazil
Rev Bras Ter Intensiva. 2014;26(1):57-64
DOI 10.5935/0103-507X.20140009
Views0Objective:
To describe the characteristics of physical therapy assistance to newborns and to provide a profile of physical therapists working in intensive care units in the city of São Paulo, Brazil.
Methods:
This cross-sectional study was conducted in every hospital in São Paulo city that had at least one intensive care unit bed for newborns registered at the National Registry of Health Establishments in 2010. In each unit, three types of physical therapists were included: an executive who was responsible for the physical therapy service in that hospital (chief-physical therapists), a physical therapist who was responsible for the physical therapy assistance in the neonatal unit (reference-physical therapists), and a randomly selected physical therapist who was directly involved in the neonatal care (care-physical therapists).
Results:
Among the 67 hospitals eligible for the study, 63 (94.0%) had a physical therapy service. Of those hospitals, three (4.8%) refused to participate. Thus, 60 chief-PTs, 52 reference-physical therapists, and 44 care-physical therapists were interviewed. During day shifts, night shifts, and weekends/holidays, there were no physical therapists in 1.7%, 45.0%, and 13.3% of the intensive care units, respectively. Physical therapy assistance was available for 17.8±7.2 hours/day, and each physical therapist cared for 9.4±2.6 newborns during six working hours. Most professionals had completed at least one specialization course.
Conclusion:
Most neonatal intensive care units in the city of São Paulo had physical therapists working on the day shift. However, other shifts had incomplete staff with less than 18 hours of available physical therapy assistance per day.
Keywords:Infant, newbornInfant, prematureIntensive care unitsPhysical therapy department, hospitalPhysical therapy modalitiesSee more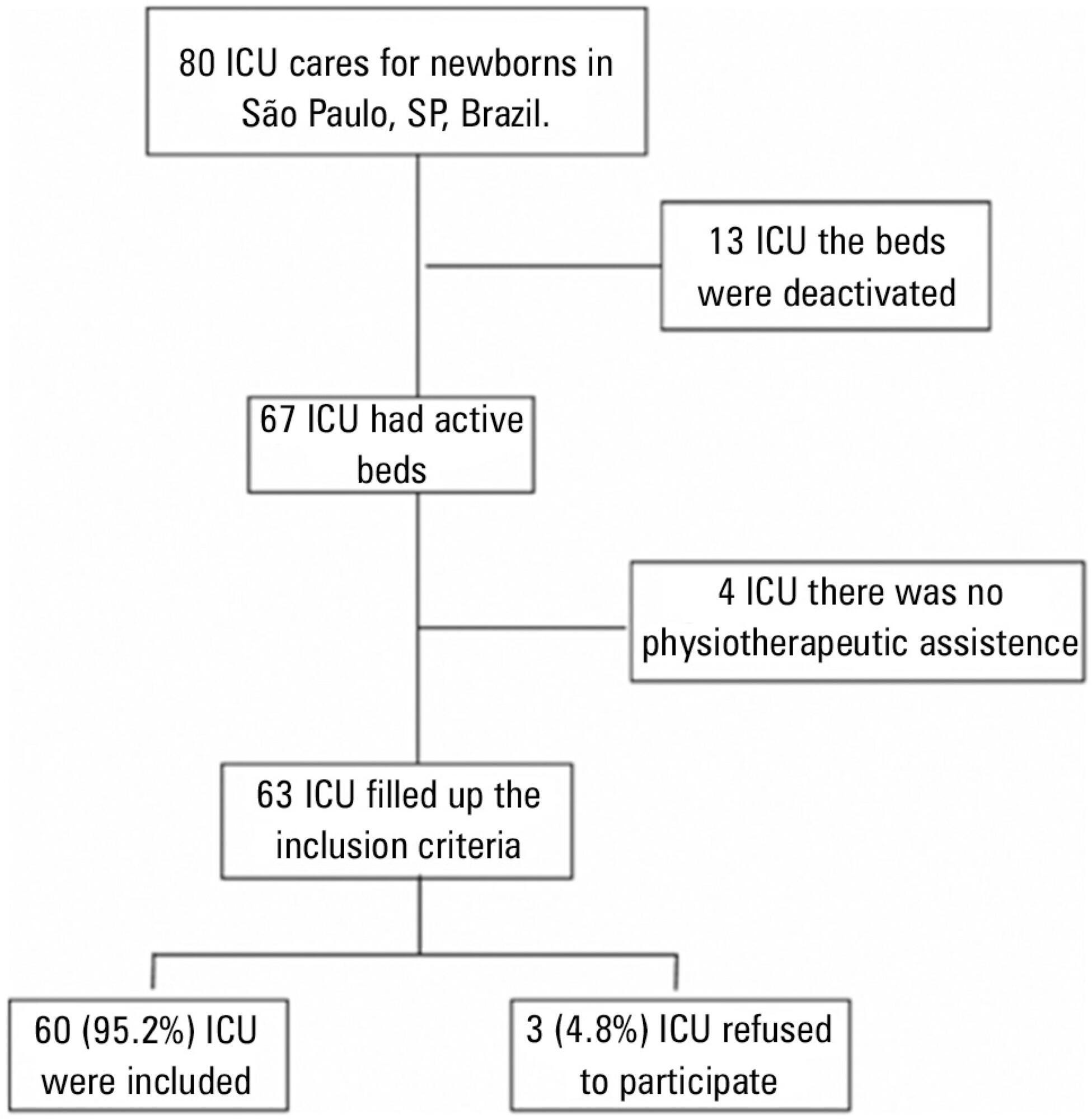
-
Original Articles
Impact of hospitalization in an intensive care unit on range of motion of critically ill patients: a pilot study
Rev Bras Ter Intensiva. 2014;26(1):65-70
Abstract
Original ArticlesImpact of hospitalization in an intensive care unit on range of motion of critically ill patients: a pilot study
Rev Bras Ter Intensiva. 2014;26(1):65-70
DOI 10.5935/0103-507X.20140010
Views0See moreObjective:
To evaluate the joint range of motion of critically ill patients during hospitalization in the intensive care unit.
Methods:
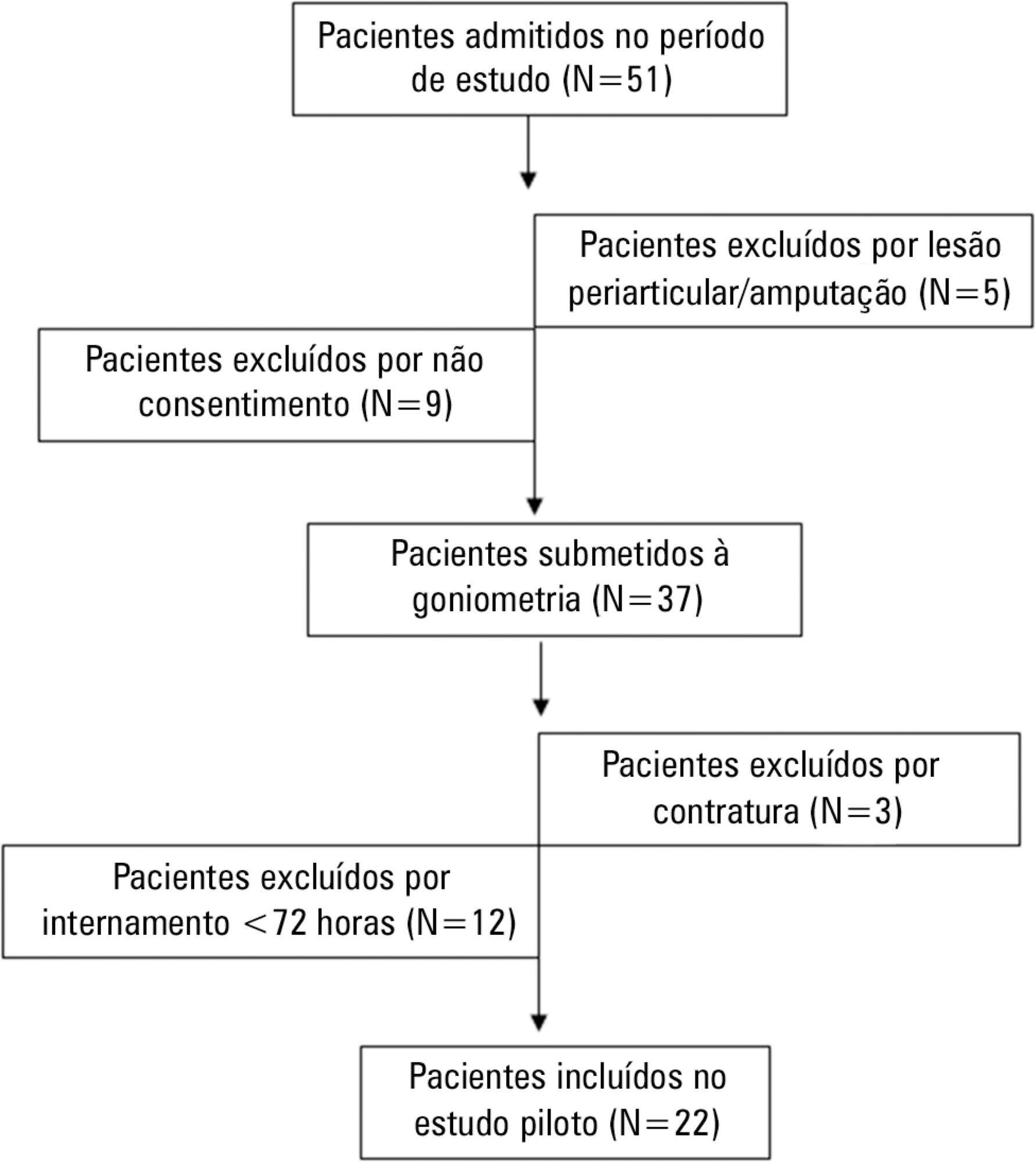
This work was a prospective longitudinal study conducted in a critical care unit of a public hospital in the city of Salvador (BA) from September to November 2010. The main variable evaluated was the passive joint range of motion. A goniometer was used to measure the elbows, knees and ankles at the time of admission and at discharge. All patients admitted in the period were included other than patients with length of stay <72 hours and patients with reduced joint range of motion on admission.
Results:
The sample consisted of 22 subjects with a mean age of 53.5±17.6 years, duration of stay in the intensive care unit of 13.0±6.0 days and time on mechanical ventilation of 12.0±6.3 days. The APACHE II score was 28.5±7.3, and the majority of patients had functional independence at admission with a prior Barthel index of 88.8±19. The losses of joint range of motion were 11.1±2.1°, 11.0±2.2°, 8.4±1.7°, 9.2±1.6°, 5.8±0.9° and 5.1±1.0°, for the right and left elbows, knees and ankles, respectively (p<0.001).
Conclusion:
There was a tendency towards decreased range of motion of large joints such as the ankle, knee and elbow during hospitalization in the intensive care unit.
Views0Abstract
Original ArticlesImpact of hospitalization in an intensive care unit on range of motion of critically ill patients: a pilot study
Rev Bras Ter Intensiva. 2014;26(1):65-70
DOI 10.5935/0103-507X.20140010
Views0See moreObjective:
To evaluate the joint range of motion of critically ill patients during hospitalization in the intensive care unit.
Methods:
This work was a prospective longitudinal study conducted in a critical care unit of a public hospital in the city of Salvador (BA) from September to November 2010. The main variable evaluated was the passive joint range of motion. A goniometer was used to measure the elbows, knees and ankles at the time of admission and at discharge. All patients admitted in the period were included other than patients with length of stay <72 hours and patients with reduced joint range of motion on admission.
Results:
The sample consisted of 22 subjects with a mean age of 53.5±17.6 years, duration of stay in the intensive care unit of 13.0±6.0 days and time on mechanical ventilation of 12.0±6.3 days. The APACHE II score was 28.5±7.3, and the majority of patients had functional independence at admission with a prior Barthel index of 88.8±19. The losses of joint range of motion were 11.1±2.1°, 11.0±2.2°, 8.4±1.7°, 9.2±1.6°, 5.8±0.9° and 5.1±1.0°, for the right and left elbows, knees and ankles, respectively (p<0.001).
Conclusion:
There was a tendency towards decreased range of motion of large joints such as the ankle, knee and elbow during hospitalization in the intensive care unit.
-
Review Article
Assessment and treatment of hyperglycemia in critically ill patients
Rev Bras Ter Intensiva. 2014;26(1):71-76
Abstract
Review ArticleAssessment and treatment of hyperglycemia in critically ill patients
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
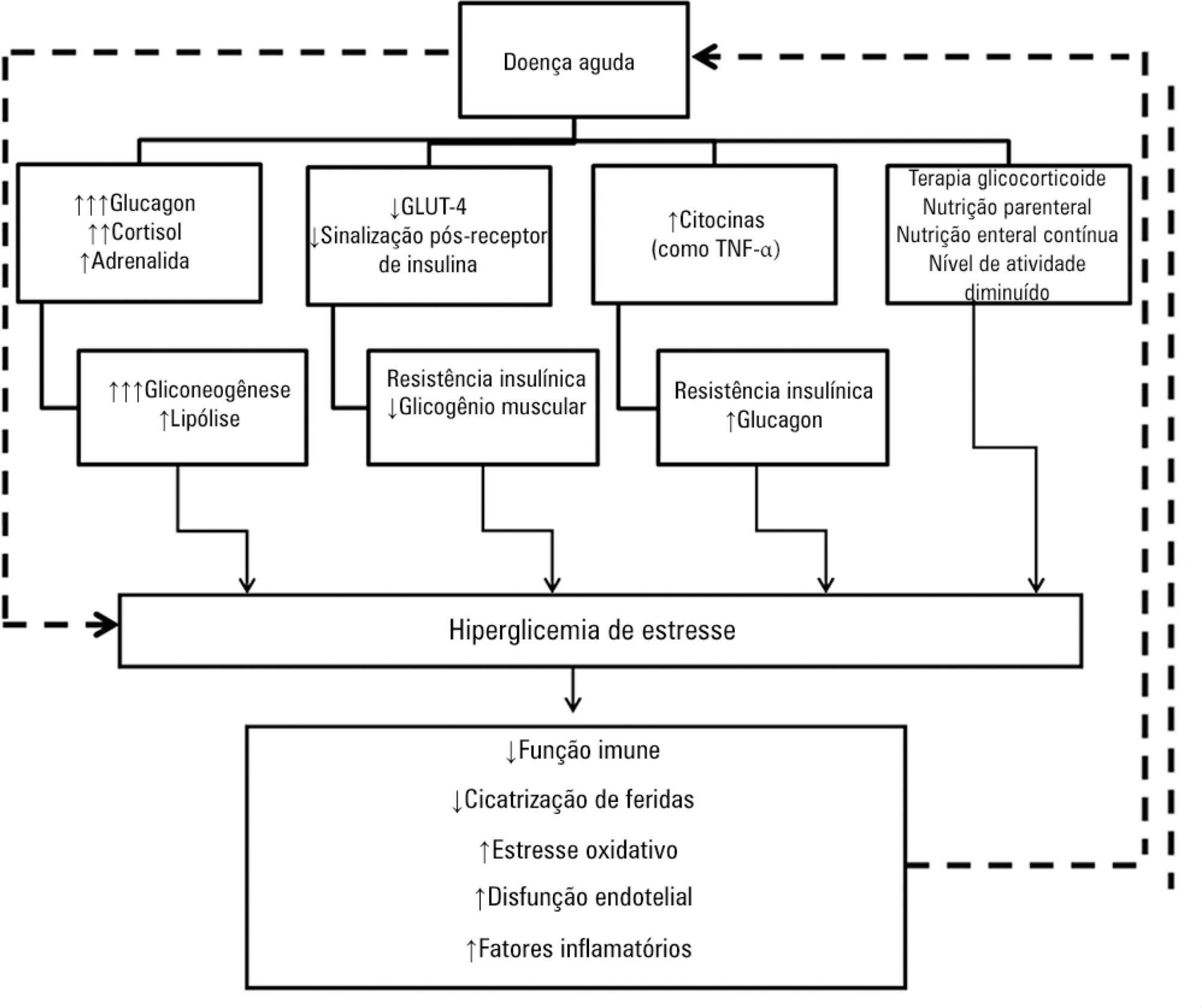
Views0See moreHyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients’ care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Views0Abstract
Review ArticleAssessment and treatment of hyperglycemia in critically ill patients
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
Views0See moreHyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients’ care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Volume Articles - Critical Care Science (CCS)
