Original Article Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):315-321
DOI 10.5935/0103-507X.20150055
To assess the impact of intracranial pressure monitoring on the short-term outcomes of traumatic brain injury patients.
Retrospective observational study including 299 consecutive patients admitted due to traumatic brain injury from January 2011 through July 2012 at a Level 1 trauma center in São Paulo, Brazil. Patients were categorized in two groups according to the measurement of intracranial pressure (measured intracranial pressure and non-measured intracranial pressure groups). We applied a propensity-matched analysis to adjust for possible confounders (variables contained in the Crash Score prognostic algorithm).
Global mortality at 14 days (16%) was equal to that observed in high-income countries in the CRASH Study and was better than expected based on the CRASH calculator score (20.6%), with a standardized mortality ratio of 0.77. A total of 28 patients received intracranial pressure monitoring (measured intracranial pressure group), of whom 26 were paired in a 1:1 fashion with patients from the non-measured intracranial pressure group. There was no improvement in the measured intracranial pressure group compared to the non-measured intracranial pressure group regarding hospital mortality, 14-day mortality, or combined hospital and chronic care facility mortality. Survival up to 14 days was also similar between groups.
Patients receiving intracranial pressure monitoring tend to have more severe traumatic brain injuries. However, after adjusting for multiple confounders using propensity scoring, no benefits in terms of survival were observed among intracranial pressure-monitored patients and those managed with a systematic clinical protocol.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):322-332
DOI 10.5935/0103-507X.20150056
The determination of coma patient prognosis after cardiac arrest has clinical, ethical and social implications. Neurological examination, imaging and biochemical markers are helpful tools accepted as reliable in predicting recovery. With the advent of therapeutic hypothermia, these data need to be reconfirmed. In this study, we attempted to determine the validity of different markers, which can be used in the detection of patients with poor prognosis under hypothermia.
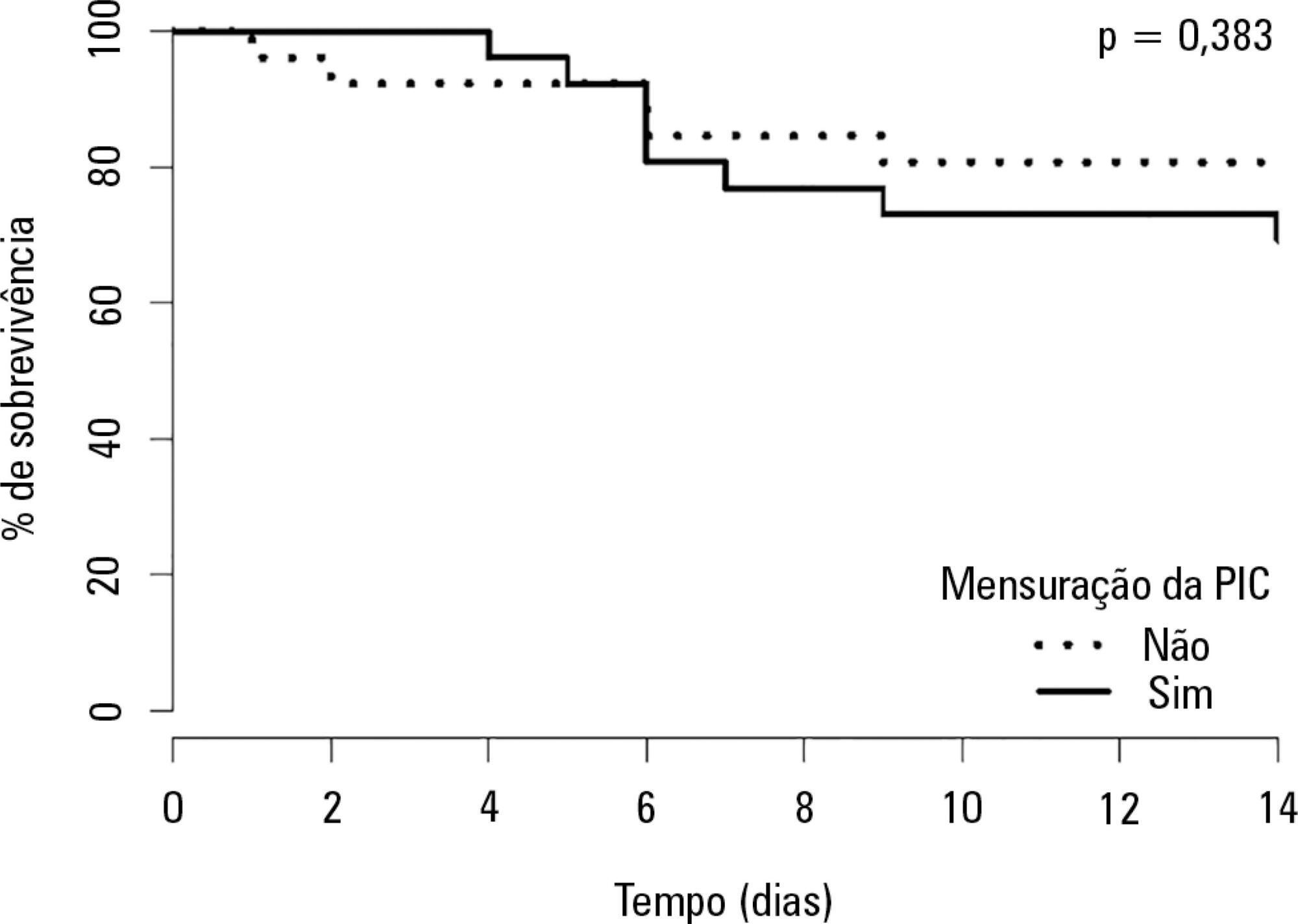
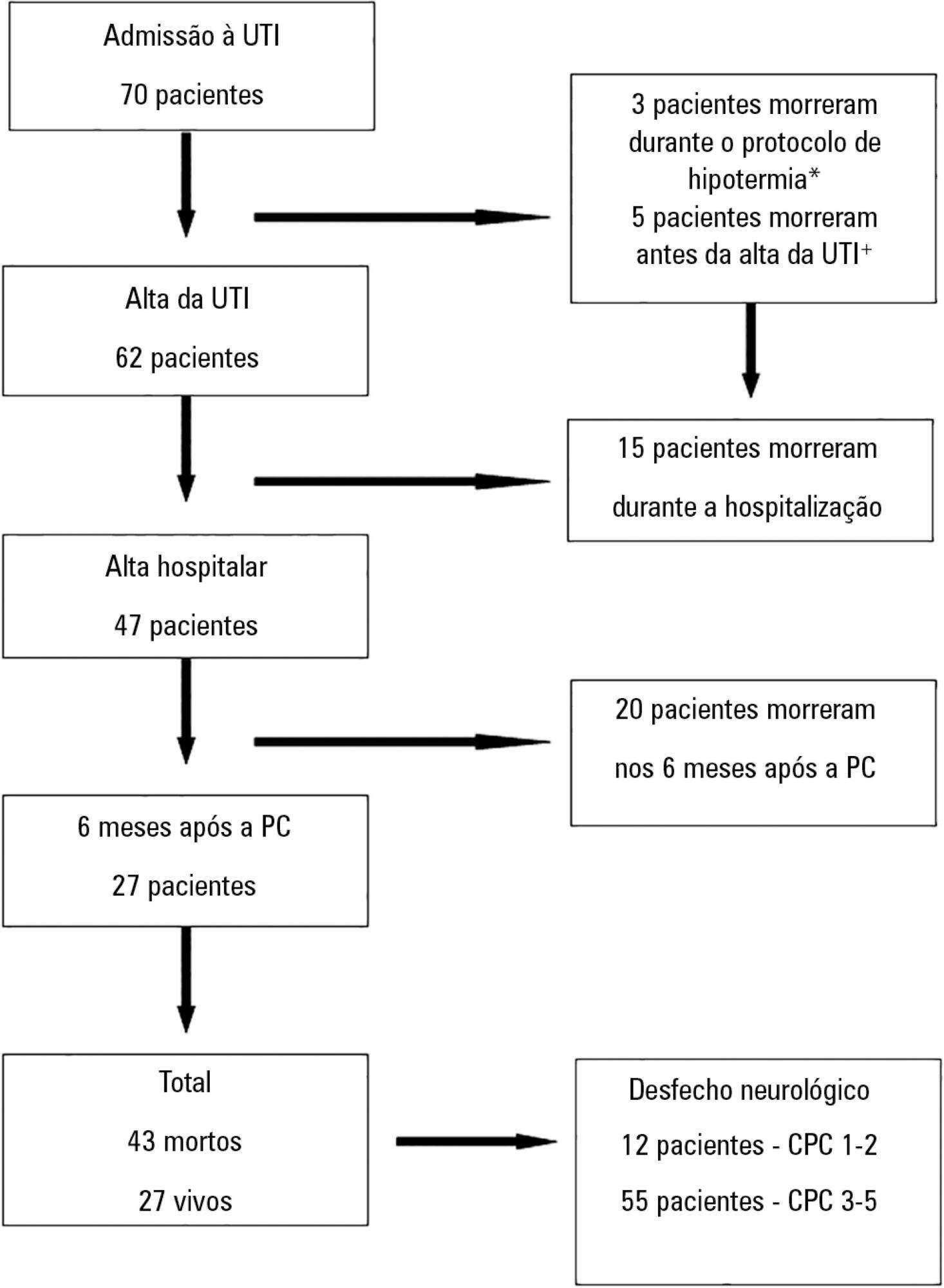
Data from adult patients admitted to our intensive care unit for a hypothermia protocol after cardiac arrest were recorded prospectively to generate a descriptive and analytical study analyzing the relationship between clinical, neurophysiological, imaging and biochemical parameters with 6-month outcomes defined according to the Cerebral Performance Categories scale (good 1-2, poor 3-5). Neuron-specific enolase was collected at 72 hours. Imaging and neurophysiologic exams were carried out in the 24 hours after the rewarming period.
Sixty-seven patients were included in the study, of which 12 had good neurological outcomes. Ventricular fibrillation and electroencephalographic theta activity were associated with increased likelihood of survival and improved neurological outcomes. Patients who had more rapid cooling (mean time of 163 versus 312 minutes), hypoxic-ischemic brain injury on magnetic resonance imaging or neuron-specific enolase > 58ng/mL had poor neurological outcomes (p < 0.05).
Hypoxic-ischemic brain injury on magnetic resonance imaging and neuron-specific enolase were strong predictors of poor neurological outcomes. Although there is the belief that early achievement of target temperature improves neurological prognoses, in our study, there were increased mortality and worse neurological outcomes with earlier target-temperature achievement.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):322-332
DOI 10.5935/0103-507X.20150056
The determination of coma patient prognosis after cardiac arrest has clinical, ethical and social implications. Neurological examination, imaging and biochemical markers are helpful tools accepted as reliable in predicting recovery. With the advent of therapeutic hypothermia, these data need to be reconfirmed. In this study, we attempted to determine the validity of different markers, which can be used in the detection of patients with poor prognosis under hypothermia.
Data from adult patients admitted to our intensive care unit for a hypothermia protocol after cardiac arrest were recorded prospectively to generate a descriptive and analytical study analyzing the relationship between clinical, neurophysiological, imaging and biochemical parameters with 6-month outcomes defined according to the Cerebral Performance Categories scale (good 1-2, poor 3-5). Neuron-specific enolase was collected at 72 hours. Imaging and neurophysiologic exams were carried out in the 24 hours after the rewarming period.
Sixty-seven patients were included in the study, of which 12 had good neurological outcomes. Ventricular fibrillation and electroencephalographic theta activity were associated with increased likelihood of survival and improved neurological outcomes. Patients who had more rapid cooling (mean time of 163 versus 312 minutes), hypoxic-ischemic brain injury on magnetic resonance imaging or neuron-specific enolase > 58ng/mL had poor neurological outcomes (p < 0.05).
Hypoxic-ischemic brain injury on magnetic resonance imaging and neuron-specific enolase were strong predictors of poor neurological outcomes. Although there is the belief that early achievement of target temperature improves neurological prognoses, in our study, there were increased mortality and worse neurological outcomes with earlier target-temperature achievement.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e' ratio, were compared between survivors and non-survivors.
A total of 99 echocardiograms (53 at admission and 46 between days 7 - 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e' ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 - 1.76], p = 0.02).
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e' ratio, were compared between survivors and non-survivors.
A total of 99 echocardiograms (53 at admission and 46 between days 7 - 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e' ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 - 1.76], p = 0.02).
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
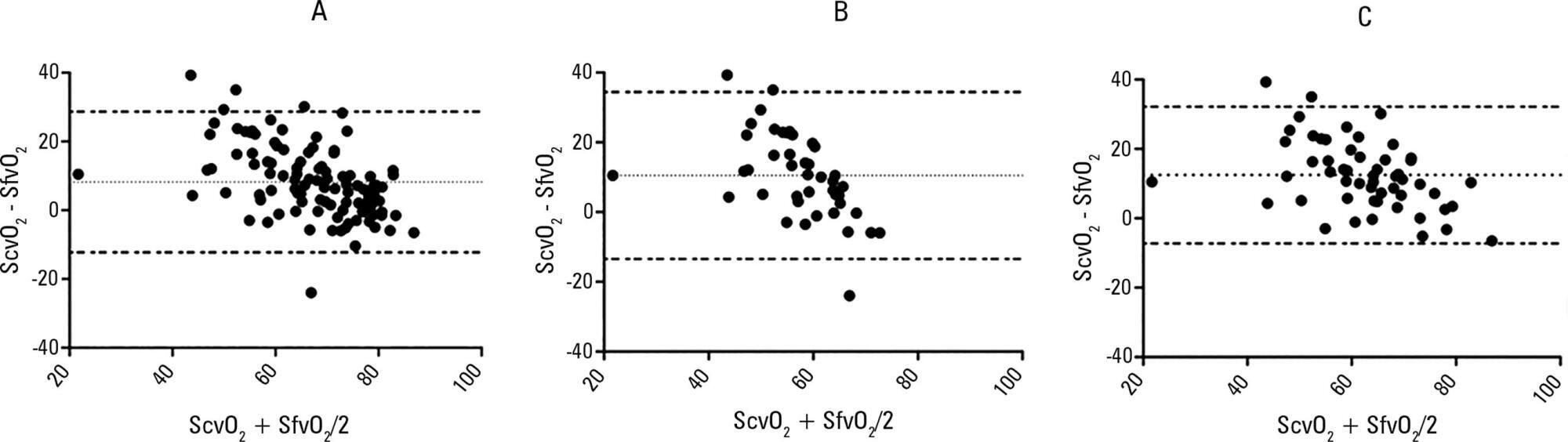
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):340-346
DOI 10.5935/0103-507X.20150058
The purpose of this study was to test if venous blood drawn from femoral access can be used to estimate the central venous oxygen saturation and arterial lactate levels in critically ill patients.
Bland-Altman analysis and Spearman correlations were used to compare the femoral venous oxygen saturation and central venous oxygen saturation as well as arterial lactate levels and femoral lactate. A pre-specified subgroup analysis was conducted in patients with signs of hypoperfusion. In addition, the clinical agreement was also investigated.
Blood samples were obtained in 26 patients. In 107 paired samples, there was a moderate correlation (r = 0.686, p < 0.0001) between the central venous oxygen saturation and femoral venous oxygen saturation with a bias of 8.24 ± 10.44 (95% limits of agreement: -12.23 to 28.70). In 102 paired samples, there was a strong correlation between the arterial lactate levels and femoral lactate levels (r = 0.972, p < 0.001) with a bias of -2.71 ± 9.86 (95% limits of agreement: -22.03 to 16.61). The presence of hypoperfusion did not significantly change these results. The clinical agreement for venous saturation was inadequate, with different therapeutic decisions in 22.4% of the situation; for lactate, this was the case only in 5.2% of the situations.
Femoral venous oxygen saturation should not be used as a surrogate of central venous oxygen saturation. However, femoral lactate levels can be used in clinical practice, albeit with caution.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
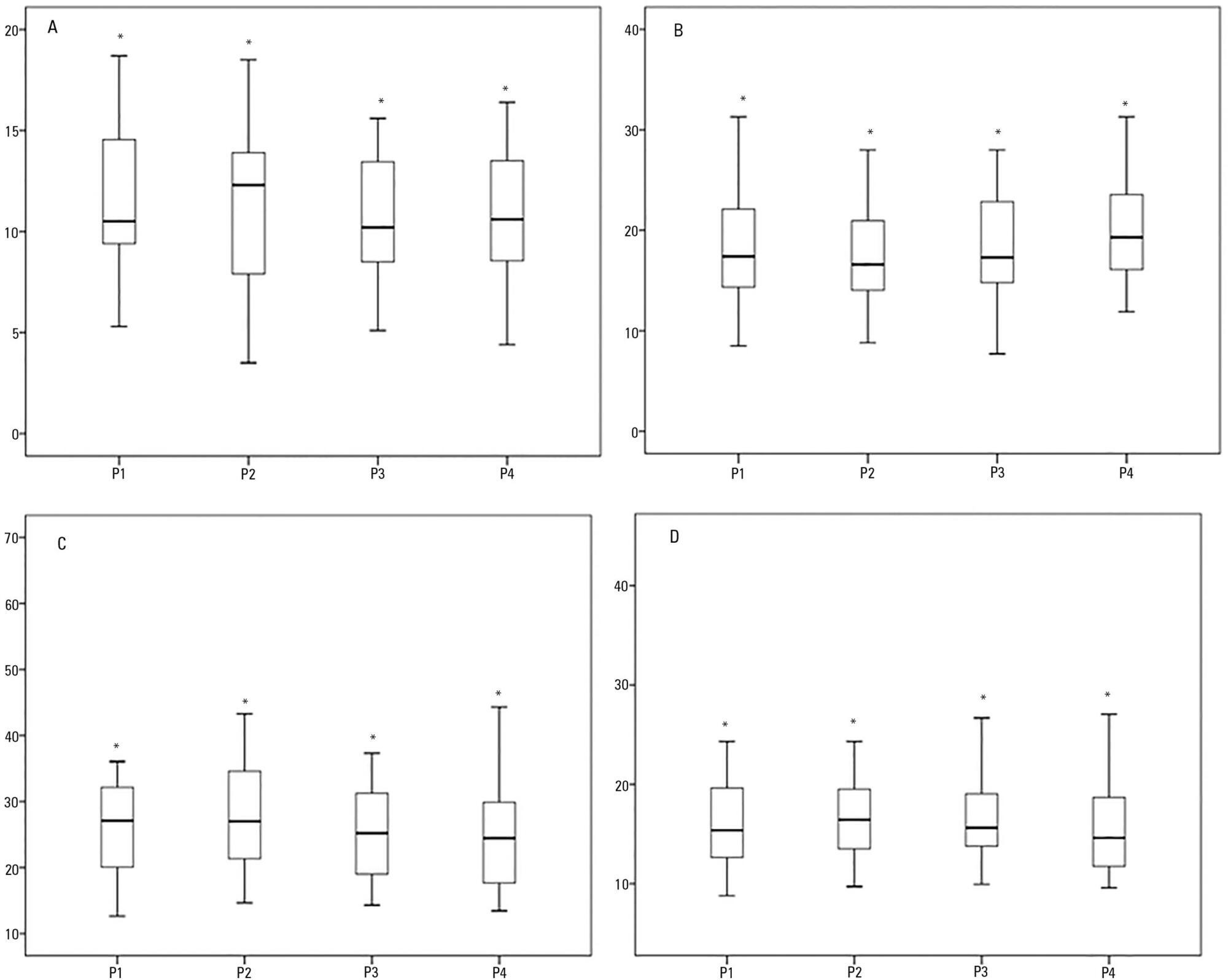
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):347-352
DOI 10.5935/0103-507X.20150059
The positioning of a patient in bed may directly affect their respiratory mechanics. The objective of this study was to evaluate the respiratory mechanics of mechanically ventilated patients positioned with different head angles hospitalized in an intensive care unit.
This was a prospective physiological study in which static and dynamic compliance, resistive airway pressure, and peripheral oxygen saturation were measured with the head at four different positions (0° = P1, 30° = P2, 45° = P3, and 60° = P4). Repeated-measures analysis of variance (ANOVA) with a Bonferroni post-test and Friedman analysis were used to compare the values obtained at the different positions.
A comparison of the 35 evaluated patients revealed that the resistive airway pressure values in the 0° position were higher than those obtained when patients were positioned at greater angles. The elastic pressure analysis revealed that the 60° position produced the highest value relative to the other positions. Regarding static compliance, a reduction in values was observed from the 0° position to the 60° position. The dynamic compliance analysis revealed that the 30° angle produced the greatest value compared to the other positions. The peripheral oxygen saturation showed little variation, with the highest value obtained at the 0° position.
The highest dynamic compliance value was observed at the 30° position, and the highest oxygenation value was observed at the 0° position.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):353-359
DOI 10.5935/0103-507X.20150060
To evaluate the incidence of potential drug-drug interactions in an intensive care unit of a hospital, focusing on antimicrobial drugs.
This cross-sectional study analyzed electronic prescriptions of patients admitted to the intensive care unit of a teaching hospital between January 1 and March 31, 2014 and assessed potential drug-drug interactions associated with antimicrobial drugs. Antimicrobial drug consumption levels were expressed in daily doses per 100 patient-days. The search and classification of the interactions were based on the Micromedex® system.
The daily prescriptions of 82 patients were analyzed, totaling 656 prescriptions. Antimicrobial drugs represented 25% of all prescription drugs, with meropenem, vancomycin and ceftriaxone being the most prescribed medications. According to the approach of daily dose per 100 patient-days, the most commonly used antimicrobial drugs were cefepime, meropenem, sulfamethoxazole + trimethoprim and ciprofloxacin. The mean number of interactions per patient was 2.6. Among the interactions, 51% were classified as contraindicated or significantly severe. Highly significant interactions (clinical value 1 and 2) were observed with a prevalence of 98%.
The current study demonstrated that antimicrobial drugs are frequently prescribed in intensive care units and present a very high number of potential drug-drug interactions, with most of them being considered highly significant.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):360-368
DOI 10.5935/0103-507X.20150061
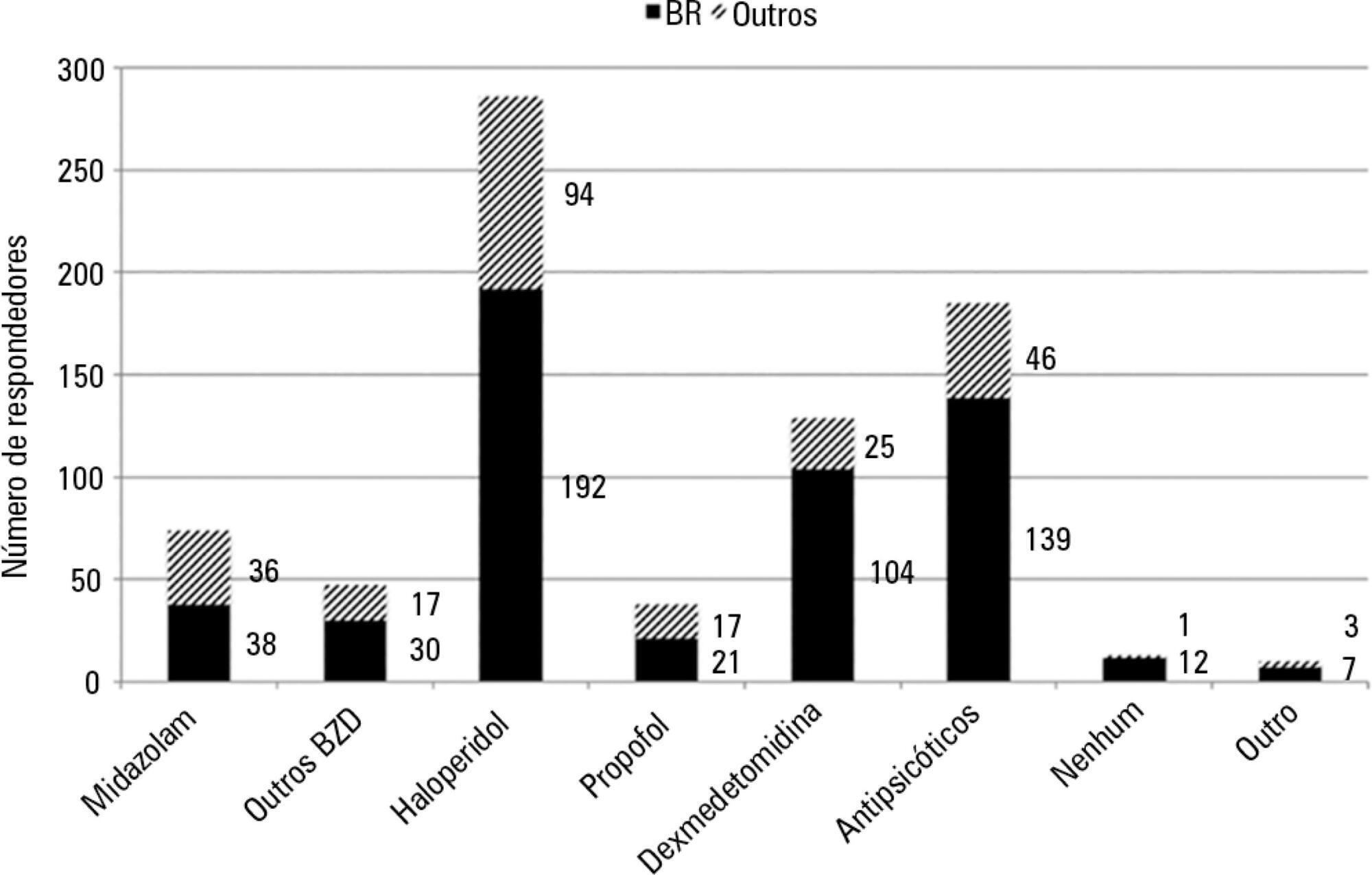
To conduct a multinational survey of intensive care unit professionals to determine the practices on delirium assessment and management, in addition to their perceptions and attitudes toward the evaluation and impact of delirium in patients requiring noninvasive ventilation.
An electronic questionnaire was created to evaluate the profiles of the respondents and their related intensive care units, the systematic delirium assessment and management and the respondents' perceptions and attitudes regarding delirium in patients requiring noninvasive ventilation. The questionnaire was distributed to the cooperative network for research of the Associação de Medicina Intensiva Brasileira (AMIB-Net) mailing list and to researchers in different centers in Latin America and Europe.
Four hundred thirty-six questionnaires were available for analysis; the majority of the questionnaires were from Brazil (61.9%), followed by Turkey (8.7%) and Italy (4.8%). Approximately 61% of the respondents reported no delirium assessment in the intensive care unit, and 31% evaluated delirium in patients under noninvasive ventilation. The Confusion Assessment Method for the intensive care unit was the most reported validated diagnostic tool (66.9%). Concerning the indication of noninvasive ventilation in patients already presenting with delirium, 16.3% of respondents never allow the use of noninvasive ventilation in this clinical context.
This survey provides data that strongly reemphasizes poor efforts toward delirium assessment and management in the intensive care unit setting, especially regarding patients requiring noninvasive ventilation.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):360-368
DOI 10.5935/0103-507X.20150061
To conduct a multinational survey of intensive care unit professionals to determine the practices on delirium assessment and management, in addition to their perceptions and attitudes toward the evaluation and impact of delirium in patients requiring noninvasive ventilation.
An electronic questionnaire was created to evaluate the profiles of the respondents and their related intensive care units, the systematic delirium assessment and management and the respondents' perceptions and attitudes regarding delirium in patients requiring noninvasive ventilation. The questionnaire was distributed to the cooperative network for research of the Associação de Medicina Intensiva Brasileira (AMIB-Net) mailing list and to researchers in different centers in Latin America and Europe.
Four hundred thirty-six questionnaires were available for analysis; the majority of the questionnaires were from Brazil (61.9%), followed by Turkey (8.7%) and Italy (4.8%). Approximately 61% of the respondents reported no delirium assessment in the intensive care unit, and 31% evaluated delirium in patients under noninvasive ventilation. The Confusion Assessment Method for the intensive care unit was the most reported validated diagnostic tool (66.9%). Concerning the indication of noninvasive ventilation in patients already presenting with delirium, 16.3% of respondents never allow the use of noninvasive ventilation in this clinical context.
This survey provides data that strongly reemphasizes poor efforts toward delirium assessment and management in the intensive care unit setting, especially regarding patients requiring noninvasive ventilation.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):369-375
DOI 10.5935/0103-507X.20150062
To verify the relationship between the adductor pollicis muscle thickness test and the subjective global assessment and to correlate it with other anthropometric methods.
This observational cross-sectional study was conducted in the intensive care unit of a cardiology hospital in the state of Rio Grande do Sul, Brazil. The hospitalized patients underwent subjective global assessment and adductor pollicis muscle thickness tests on both hands, along with measurement of the right calf circumference. Laboratory parameters, length of stay, vital signs and electronic medical record data and tests were all collected.
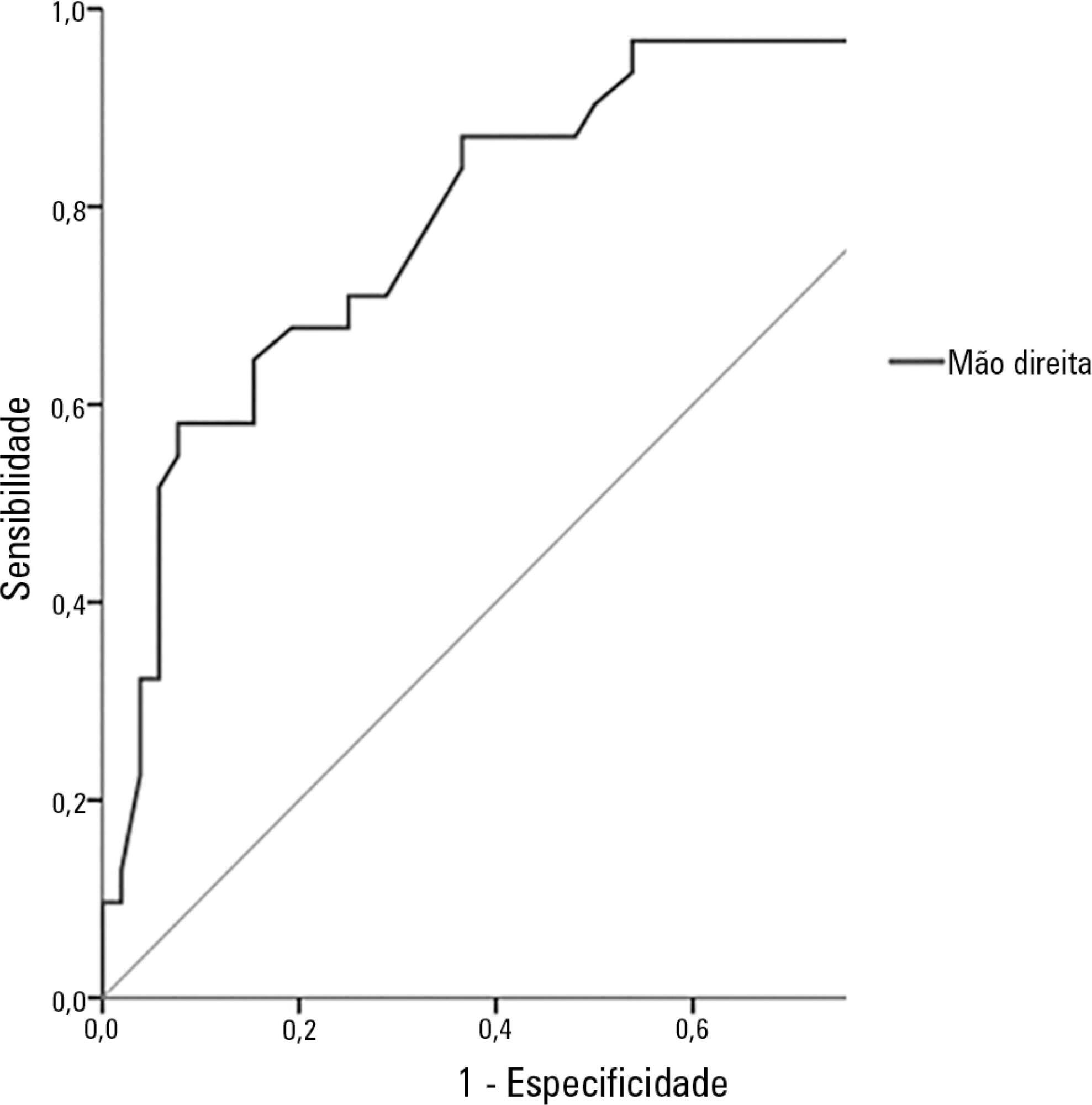
The study population included 83 patients, of whom 62% were men. The average age was 68.6 ± 12.5 years. The most common reason for hospitalization was acute myocardial infarction (34.9%), and the most common pathology was systolic blood pressure (63.9%), followed by diabetes mellitus (28.9%). According to subjective global assessment classifications, 62.7% of patients presented no nutritional risk, 20.5% were moderately malnourished and 16.9% were severely malnourished. Women had a higher nutritional risk, according to both the subjective global assessment and the adductor pollicis muscle thickness test, the cutoff for which was < 6.5mm (54.8%; p = 0.001). The pathology presenting the greatest nutritional risk was congestive heart failure (p = 0.001). Evaluation of the receiver operating characteristic (ROC) curve between adductor pollicis muscle thickness and subjective global assessment showed the accuracy of the former, with an area of 0.822.
Adductor pollicis muscle thickness proved to be a good method for evaluating nutritional risk.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):369-375
DOI 10.5935/0103-507X.20150062
To verify the relationship between the adductor pollicis muscle thickness test and the subjective global assessment and to correlate it with other anthropometric methods.
This observational cross-sectional study was conducted in the intensive care unit of a cardiology hospital in the state of Rio Grande do Sul, Brazil. The hospitalized patients underwent subjective global assessment and adductor pollicis muscle thickness tests on both hands, along with measurement of the right calf circumference. Laboratory parameters, length of stay, vital signs and electronic medical record data and tests were all collected.
The study population included 83 patients, of whom 62% were men. The average age was 68.6 ± 12.5 years. The most common reason for hospitalization was acute myocardial infarction (34.9%), and the most common pathology was systolic blood pressure (63.9%), followed by diabetes mellitus (28.9%). According to subjective global assessment classifications, 62.7% of patients presented no nutritional risk, 20.5% were moderately malnourished and 16.9% were severely malnourished. Women had a higher nutritional risk, according to both the subjective global assessment and the adductor pollicis muscle thickness test, the cutoff for which was < 6.5mm (54.8%; p = 0.001). The pathology presenting the greatest nutritional risk was congestive heart failure (p = 0.001). Evaluation of the receiver operating characteristic (ROC) curve between adductor pollicis muscle thickness and subjective global assessment showed the accuracy of the former, with an area of 0.822.
Adductor pollicis muscle thickness proved to be a good method for evaluating nutritional risk.