Original Articles Archives - Page 3 of 25 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology - Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology - Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):270-278
DOI 10.5935/0103-507X.20130047
The current definition of severe sepsis and septic shock includes a heterogeneous profile of patients. Although the prognostic value of hyperlactatemia is well established, hyperlactatemia is observed in patients with and without shock. The present study aimed to compare the prognosis of septic patients by stratifying them according to two factors: hyperlactatemia and persistent hypotension.
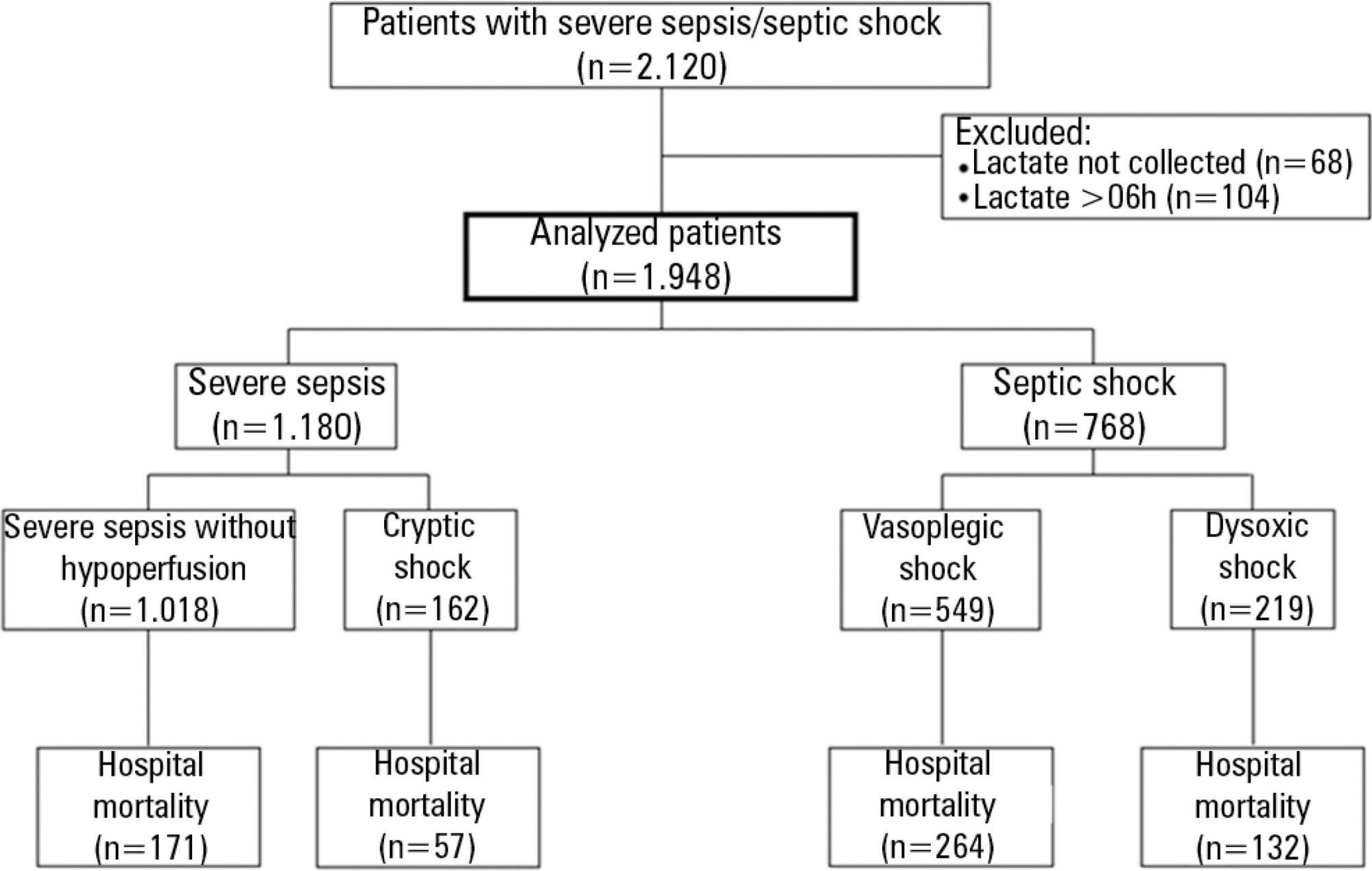
The present study is a secondary analysis of an observational study conducted in ten hospitals in Brazil (Rede Amil - SP). Septic patients with initial lactate measurements in the first 6 hours of diagnosis were included and divided into 4 groups according to hyperlactatemia (lactate >4mmol/L) and persistent hypotension: (1) severe sepsis (without both criteria); (2) cryptic shock (hyperlactatemia without persistent hypotension); (3) vasoplegic shock (persistent hypotension without hyperlactatemia); and (4) dysoxic shock (both criteria).
In total, 1,948 patients were analyzed, and the sepsis group represented 52% of the patients, followed by 28% with vasoplegic shock, 12% with dysoxic shock and 8% with cryptic shock. Survival at 28 days differed among the groups (p<0.001). Survival was highest among the severe sepsis group (69%, p<0.001 versus others), similar in the cryptic and vasoplegic shock groups (53%, p=0.39), and lowest in the dysoxic shock group (38%, p<0.001 versus others). In the adjusted analysis, the survival at 28 days remained different among the groups (p<0.001) and the dysoxic shock group exhibited the highest hazard ratio (HR=2.99, 95%CI 2.21-4.05).
The definition of sepsis includes four different profiles if we consider the presence of hyperlactatemia. Further studies are needed to better characterize septic patients, to understand the etiology and to design adequate targeted treatments.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):270-278
DOI 10.5935/0103-507X.20130047
The current definition of severe sepsis and septic shock includes a heterogeneous profile of patients. Although the prognostic value of hyperlactatemia is well established, hyperlactatemia is observed in patients with and without shock. The present study aimed to compare the prognosis of septic patients by stratifying them according to two factors: hyperlactatemia and persistent hypotension.
The present study is a secondary analysis of an observational study conducted in ten hospitals in Brazil (Rede Amil - SP). Septic patients with initial lactate measurements in the first 6 hours of diagnosis were included and divided into 4 groups according to hyperlactatemia (lactate >4mmol/L) and persistent hypotension: (1) severe sepsis (without both criteria); (2) cryptic shock (hyperlactatemia without persistent hypotension); (3) vasoplegic shock (persistent hypotension without hyperlactatemia); and (4) dysoxic shock (both criteria).
In total, 1,948 patients were analyzed, and the sepsis group represented 52% of the patients, followed by 28% with vasoplegic shock, 12% with dysoxic shock and 8% with cryptic shock. Survival at 28 days differed among the groups (p<0.001). Survival was highest among the severe sepsis group (69%, p<0.001 versus others), similar in the cryptic and vasoplegic shock groups (53%, p=0.39), and lowest in the dysoxic shock group (38%, p<0.001 versus others). In the adjusted analysis, the survival at 28 days remained different among the groups (p<0.001) and the dysoxic shock group exhibited the highest hazard ratio (HR=2.99, 95%CI 2.21-4.05).
The definition of sepsis includes four different profiles if we consider the presence of hyperlactatemia. Further studies are needed to better characterize septic patients, to understand the etiology and to design adequate targeted treatments.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):279-283
DOI 10.5935/0103-507X.20130048
To evaluate the level of knowledge of medical students about transplantation and brain death.
An anonymous self-administered questionnaire answered by medical students from the first through the sixth year that was based on information from the Associação Brasileira de Transplante de Órgãos e Tecidos, the Registro Brasileiro de Transplantes and the resolution that defines the criteria for brain death.
Of the 677 medical students asked, 310 (45.8%) agreed to answer the questionnaire. In total, 22 (7.0%) subjects were excluded. Of the students who participated, 41.3% reported having already attended a class on organ transplantation and 33% on brain death; 9.7% felt able to diagnose brain death (p<0.01); only 66.8% indicated the kidney as the most transplanted solid organ in Brazil.
The level of knowledge of medical students at this institution regarding brain death and transplantation is limited, which may be the result of an inadequate approach during medical school.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):279-283
DOI 10.5935/0103-507X.20130048
To evaluate the level of knowledge of medical students about transplantation and brain death.
An anonymous self-administered questionnaire answered by medical students from the first through the sixth year that was based on information from the Associação Brasileira de Transplante de Órgãos e Tecidos, the Registro Brasileiro de Transplantes and the resolution that defines the criteria for brain death.
Of the 677 medical students asked, 310 (45.8%) agreed to answer the questionnaire. In total, 22 (7.0%) subjects were excluded. Of the students who participated, 41.3% reported having already attended a class on organ transplantation and 33% on brain death; 9.7% felt able to diagnose brain death (p<0.01); only 66.8% indicated the kidney as the most transplanted solid organ in Brazil.
The level of knowledge of medical students at this institution regarding brain death and transplantation is limited, which may be the result of an inadequate approach during medical school.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):284-289
DOI 10.5935/0103-507X.20130049
The HLA haplotype has been associated with many autoimmune diseases, but no associations have been described in sepsis. This study aims to investigate the HLA system as a possible marker of genetic sepsis susceptibility.
This is a prospective cohort study including patients admitted to an intensive care unit and healthy controls from a list of renal transplant donors. Patients with less 18 years of age; pregnant or HIV positive patients; those with metastatic malignancies or receiving chemotherapy; or with advanced liver disease; or with end-of-life conditions were excluded. The DNA was extracted from the whole blood and HLA haplotypes determined using MiliPlex® technology.
From October 2010 to October 2012, 1,121 patients were included (1,078 kidney donors, 20 patients admitted with severe sepsis and 23 with septic shock). HLA-A*31 positive subjects had increased risk of developing sepsis (OR 2.36, 95%CI 1.26-5.35). Considering a p value <0.01, no other significant association was identified.
HLA-A*31 expression is associated to risk of developing sepsis.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):284-289
DOI 10.5935/0103-507X.20130049
The HLA haplotype has been associated with many autoimmune diseases, but no associations have been described in sepsis. This study aims to investigate the HLA system as a possible marker of genetic sepsis susceptibility.
This is a prospective cohort study including patients admitted to an intensive care unit and healthy controls from a list of renal transplant donors. Patients with less 18 years of age; pregnant or HIV positive patients; those with metastatic malignancies or receiving chemotherapy; or with advanced liver disease; or with end-of-life conditions were excluded. The DNA was extracted from the whole blood and HLA haplotypes determined using MiliPlex® technology.
From October 2010 to October 2012, 1,121 patients were included (1,078 kidney donors, 20 patients admitted with severe sepsis and 23 with septic shock). HLA-A*31 positive subjects had increased risk of developing sepsis (OR 2.36, 95%CI 1.26-5.35). Considering a p value <0.01, no other significant association was identified.
HLA-A*31 expression is associated to risk of developing sepsis.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
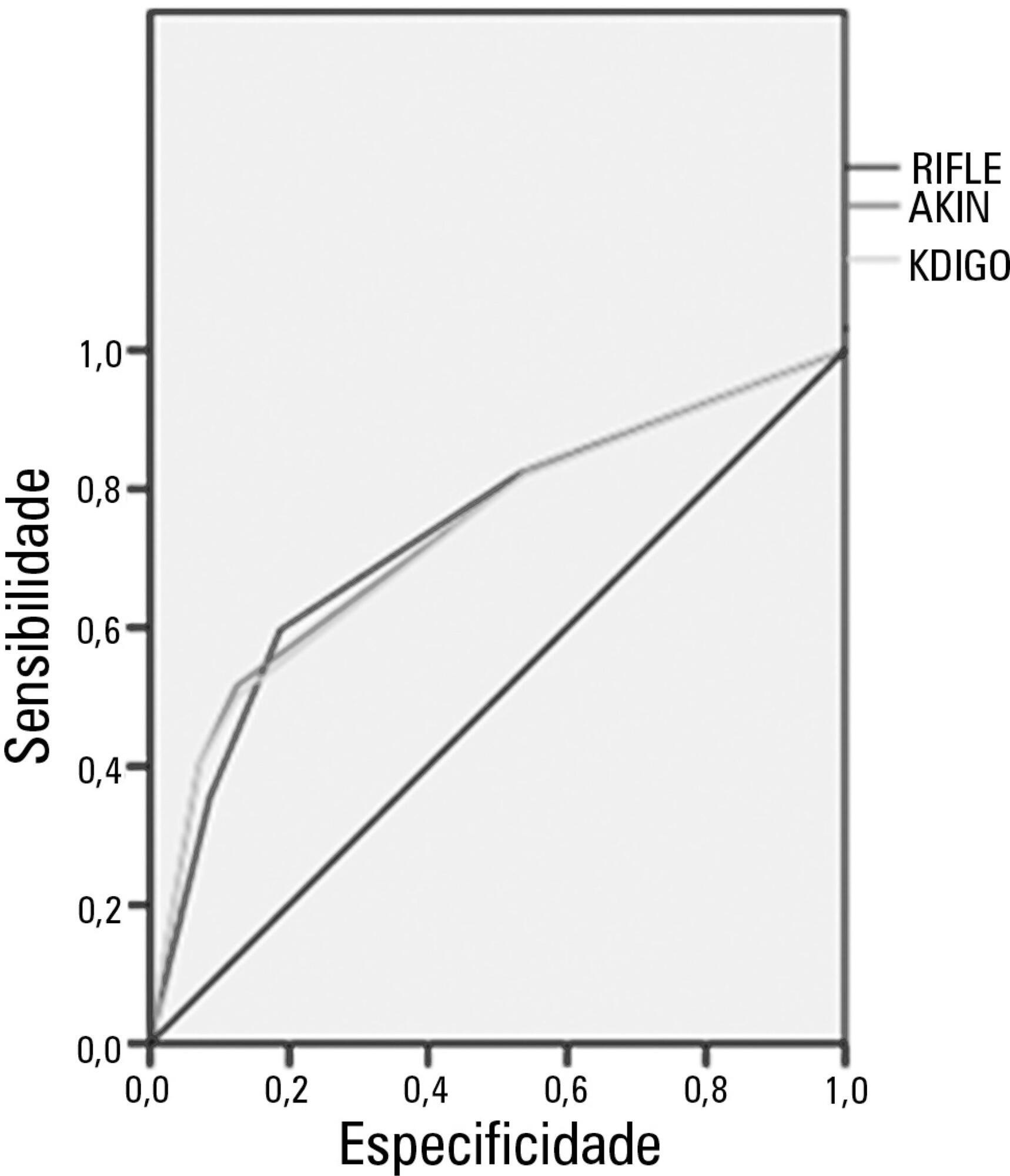
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study's aim was to compare these criteria as predictors of mortality in critically ill patients.
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student's t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):290-296
DOI 10.5935/0103-507X.20130050
Acute kidney injury is a common complication in critically ill patients, and the RIFLE, AKIN and KDIGO criteria are used to classify these patients. The present study's aim was to compare these criteria as predictors of mortality in critically ill patients.
Prospective cohort study using medical records as the source of data. All patients admitted to the intensive care unit were included. The exclusion criteria were hospitalization for less than 24 hours and death. Patients were followed until discharge or death. Student's t test, chi-squared analysis, a multivariate logistic regression and ROC curves were used for the data analysis.
The mean patient age was 64 years old, and the majority of patients were women of African descent. According to RIFLE, the mortality rates were 17.74%, 22.58%, 24.19% and 35.48% for patients without acute kidney injury (AKI) in stages of Risk, Injury and Failure, respectively. For AKIN, the mortality rates were 17.74%, 29.03%, 12.90% and 40.32% for patients without AKI and at stage I, stage II and stage III, respectively. For KDIGO 2012, the mortality rates were 17.74%, 29.03%, 11.29% and 41.94% for patients without AKI and at stage I, stage II and stage III, respectively. All three classification systems showed similar ROC curves for mortality.
The RIFLE, AKIN and KDIGO criteria were good tools for predicting mortality in critically ill patients with no significant difference between them.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
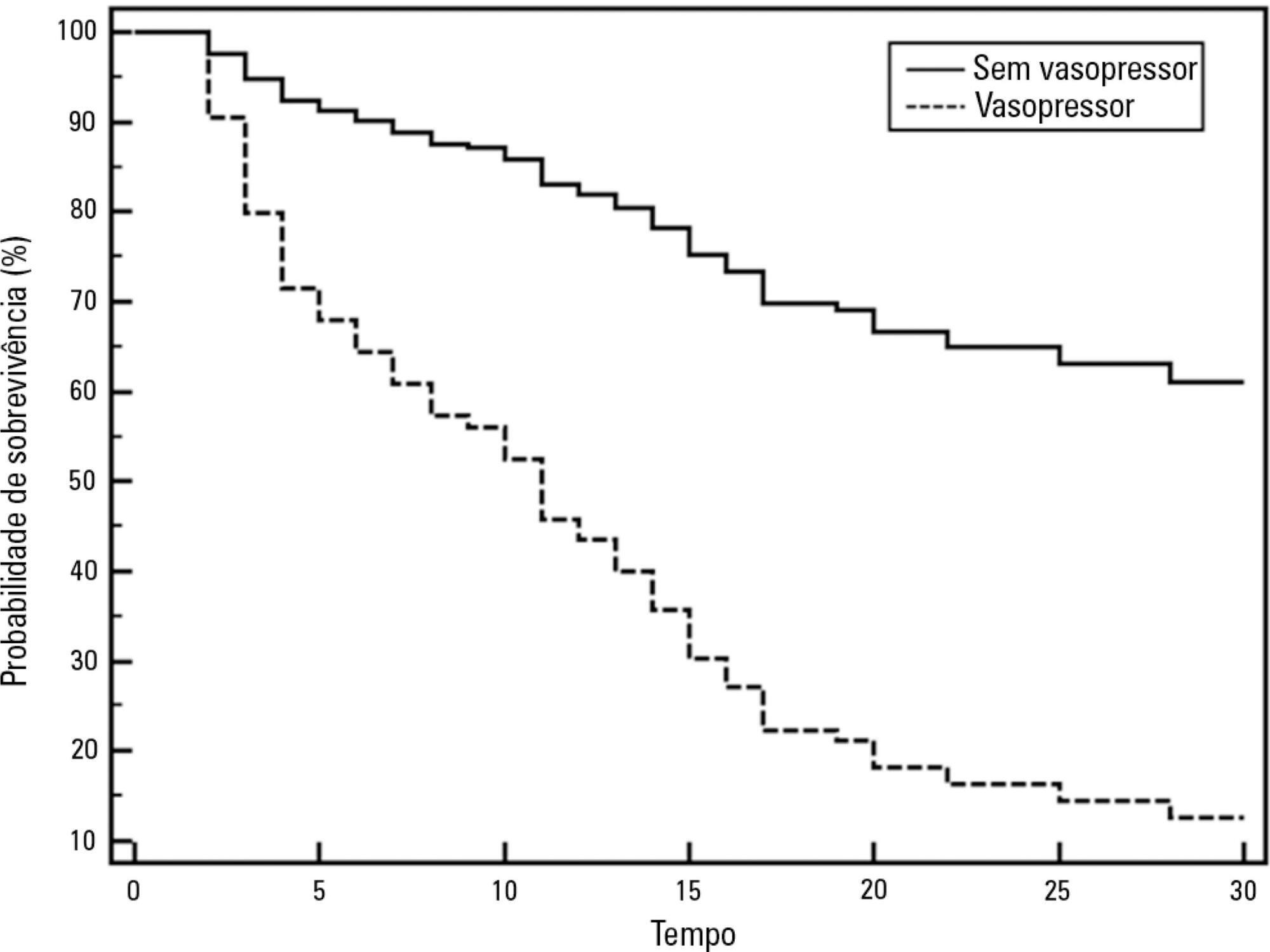
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):297-305
DOI 10.5935/0103-507X.20130051
To describe a single center experience involving the administration of colistin to treat nosocomial infections caused by multidrug-resistant Gram-negative bacteria and identify factors associated with acute kidney injury and mortality.
This retrospective longitudinal study evaluates critically ill patients with infections caused by multidrug-resistant Gram-negative bacteria. All adult patients who required treatment with intravenous colistin (colistimethate sodium) from January to December 2008 were considered eligible for the study. Data include demographics, diagnosis, duration of treatment, presence of acute kidney injury and 30-day mortality.
Colistin was used to treat an infection in 109 (13.8%) of the 789 patients admitted to the intensive care unit. The 30-day mortality observed in these patients was 71.6%. Twenty-nine patients (26.6%) presented kidney injury prior to colistin treatment, and six of these patients were able to recover kidney function even during colistin treatment. Twenty-one patients (19.2%) developed acute kidney injury while taking colistin, and 11 of these patients required dialysis. The variable independently associated with the presence of acute kidney injury was the Sequential Organ Failure Assessment at the beginning of colistin treatment (OR 1.46; 95%CI 1.20-1.79; p<0.001). The factors age (OR 1.03; 95%CI 1.00-1.05; p=0.02) and vasopressor use (OR 12.48; 95%CI 4.49-34.70; p<0.001) were associated with death in the logistic-regression model.
Organ dysfunction at the beginning of colistin treatment was associated with acute kidney injury. In a small group of patients, we were able to observe an improvement of kidney function during colistin treatment. Age and vasopressor use were associated with death.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):306-311
DOI 10.5935/0103-507X.20130052
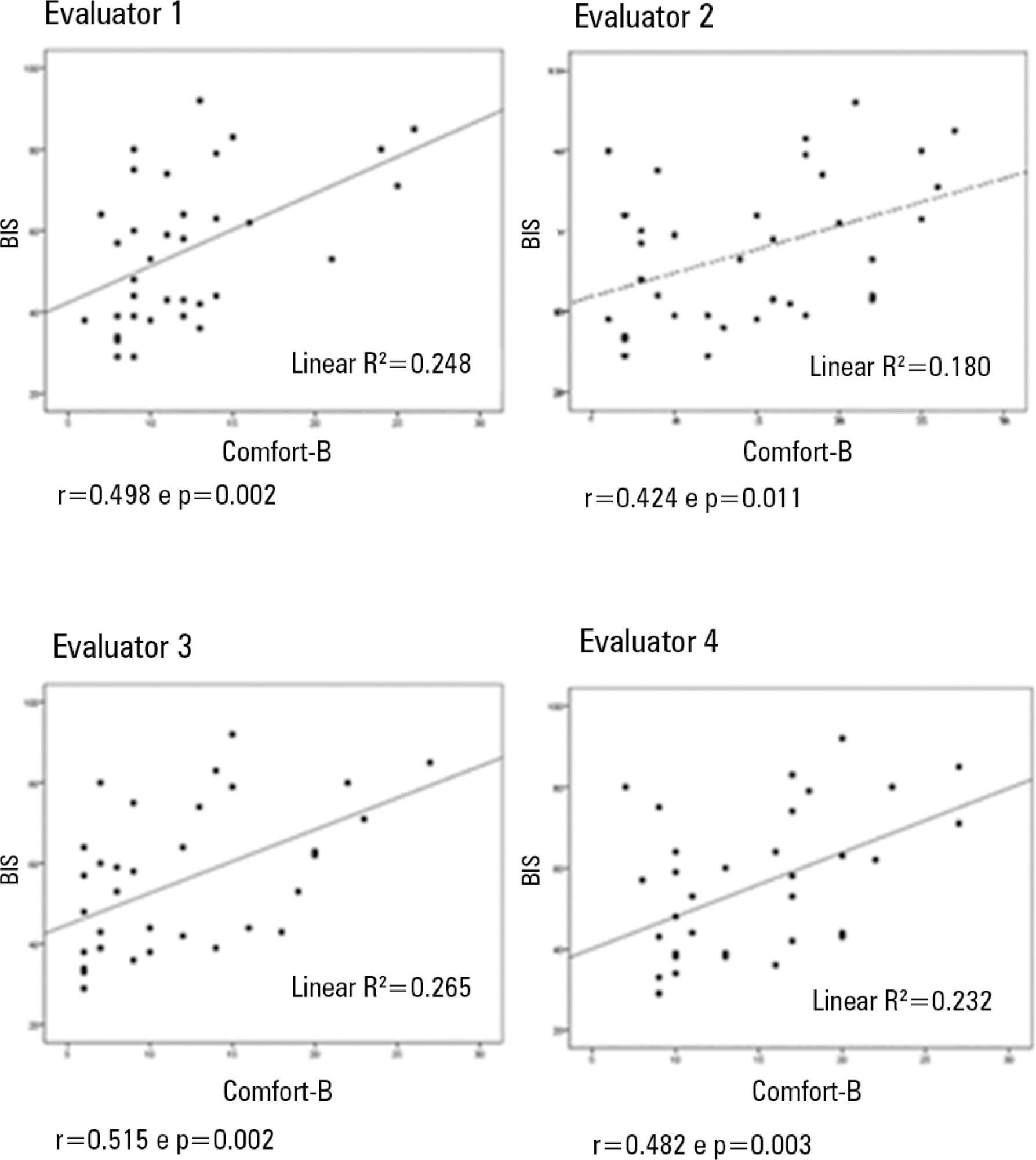
Compare the scores resulting from the Comfort-B scale with the bispectral index in children in an intensive care unit.
Eleven children between the ages of 1 month and 16 years requiring mechanical ventilation and sedation were simultaneously classified based on the bispectral index and the Comfort-B scale. Their behavior was recorded using digital photography, and the record was later evaluated by three independent evaluators. Agreement tests (Bland-Altman and Kappa) were then performed. The correlation between the two methods (Pearson correlation) was tested.
In total, 35 observations were performed on 11 patients. Based on the Kappa coefficient, the agreement among evaluators ranged from 0.56 to 0.75 (p<0.001). There was a positive and consistent association between the bispectral index and the Comfort-B scale [r=0.424 (p=0.011) to r=0.498 (p=0.002)].
Due to the strong correlation between the independent evaluators and the consistent correlation between the two methods, the results suggest that the Comfort-B scale is reproducible and useful in classifying the level of sedation in children requiring mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):306-311
DOI 10.5935/0103-507X.20130052
Compare the scores resulting from the Comfort-B scale with the bispectral index in children in an intensive care unit.
Eleven children between the ages of 1 month and 16 years requiring mechanical ventilation and sedation were simultaneously classified based on the bispectral index and the Comfort-B scale. Their behavior was recorded using digital photography, and the record was later evaluated by three independent evaluators. Agreement tests (Bland-Altman and Kappa) were then performed. The correlation between the two methods (Pearson correlation) was tested.
In total, 35 observations were performed on 11 patients. Based on the Kappa coefficient, the agreement among evaluators ranged from 0.56 to 0.75 (p<0.001). There was a positive and consistent association between the bispectral index and the Comfort-B scale [r=0.424 (p=0.011) to r=0.498 (p=0.002)].
Due to the strong correlation between the independent evaluators and the consistent correlation between the two methods, the results suggest that the Comfort-B scale is reproducible and useful in classifying the level of sedation in children requiring mechanical ventilation.