Original Articles Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
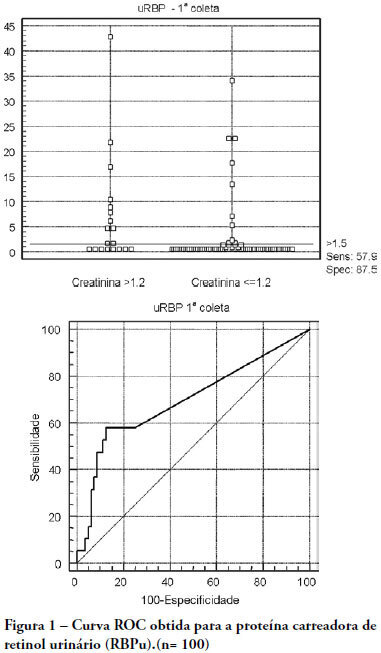
OBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test - it is a practical and non-invasive method.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):385-393
DOI 10.1590/S0103-507X2008000400011
OBJECTIVES: The early assessment of renal dysfunction using common markers does not provide either a sensitive or specific indication of renal dysfunction in critically ill patients. More specific and sensitive markers are desirable for the early detection of an initial renal pathophysiological process. Urinary retinol-binding protein could be an alternative method to early evaluation of renal function in these patients. METHODS: This study followed-up 100 critical care patients and assessed their clinical and laboratory variables, including plasma creatinine and urinary retinol-binding ratio, and demographic variables. RESULTS: The sample was characterized by geriatric (63.4±15.6 years), male (68%), being 53% surgical patients. Statistical analysis showed association between plasma creatinine and the following variables: gender (p-0.026), age (p-0.038), use of vasoactive drugs (p-0.003), proteinuria (p-0.025), Acute Physiological Chronic Health Evaluation (APACHE) II score (p-0.000), urea (p-0.000), potassium (p-0.003) and estimated creatinine clearance (p-0.000). Urinary retinol-binding protein was correlated with more variables: weight, use of invasive ventilation (p-0.000), use of nonsteroidal antiinflammatory drugs (p-0.018), use of vasoactive drugs (p-0.021), high temperature (>37.5ºC) (p-0.005), proteinuria (p-0.000), bilirubinuria (p-0.004), urinary flow (p-0.019), minimal diastolic pressure (p-0.032), minimal systolic pressure (p-0.029), APACHE II (p-0.000), creatinine (p-0.001), urea (p-0.001), estimated creatinine clearance (p-0.000). Urinary retinol-binding protein also tended to associate with previous renal disease, vasculopathy and neoplasm. Sodium excretion fraction correlated with plasma creatinine and urinary retinol-binding protein in univariate analysis. CONCLUSIONS: Urinary retinol-binding protein might be considered in clinical practice as a better marker regarding diagnostic performance in patients at risk of developing acute kidney injury, when compared with other markers routinely used. Moreover, urinary retinol-binding protein has other features of a good diagnostic test - it is a practical and non-invasive method.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):394-397
DOI 10.1590/S0103-507X2008000400012
OBJECTIVES: To evaluate risks for persistent pulmonary hypertension in the newborn, confirmed by echocardiography, associated with cesarean deliveries and other factors. METHODS: Cohort of all deliveries >36 weeks within a period of 23 months. A nested case-control study was performed in a subset of the cohort, involving newborns admitted into neonatal intensive care unit with diagnosis of persistent pulmonary hypertension matched with normal controls, with application of questionnaires to mothers to identify risks. Logistic regression was used to calculate odds ratios. RESULTS: From 9452 newborns, 8388 (88.7%) were delivered by cesarean and 1064 (11.3%) by vaginal delivery. Questionnaires were applied to 173 mothers. Infants from cesareans had a fivefold increased risk of persistent pulmonary hypertension of the newborn: 42 (0.5%) versus 1 case (0.09%) in the vaginal group (OR 5.32, p=0.027). No interactions were found between smoking, parity, arterial hypertension and labor before cesarean section and persistent pulmonary hypertension of the newborn. First minute Apgar score <7 and maternal diabetes were related to increased risk. CONCLUSION: Reducing cesarean deliveries could prevent many cases of serious persistent pulmonary hypertension of the newborn.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):394-397
DOI 10.1590/S0103-507X2008000400012
OBJECTIVES: To evaluate risks for persistent pulmonary hypertension in the newborn, confirmed by echocardiography, associated with cesarean deliveries and other factors. METHODS: Cohort of all deliveries >36 weeks within a period of 23 months. A nested case-control study was performed in a subset of the cohort, involving newborns admitted into neonatal intensive care unit with diagnosis of persistent pulmonary hypertension matched with normal controls, with application of questionnaires to mothers to identify risks. Logistic regression was used to calculate odds ratios. RESULTS: From 9452 newborns, 8388 (88.7%) were delivered by cesarean and 1064 (11.3%) by vaginal delivery. Questionnaires were applied to 173 mothers. Infants from cesareans had a fivefold increased risk of persistent pulmonary hypertension of the newborn: 42 (0.5%) versus 1 case (0.09%) in the vaginal group (OR 5.32, p=0.027). No interactions were found between smoking, parity, arterial hypertension and labor before cesarean section and persistent pulmonary hypertension of the newborn. First minute Apgar score <7 and maternal diabetes were related to increased risk. CONCLUSION: Reducing cesarean deliveries could prevent many cases of serious persistent pulmonary hypertension of the newborn.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
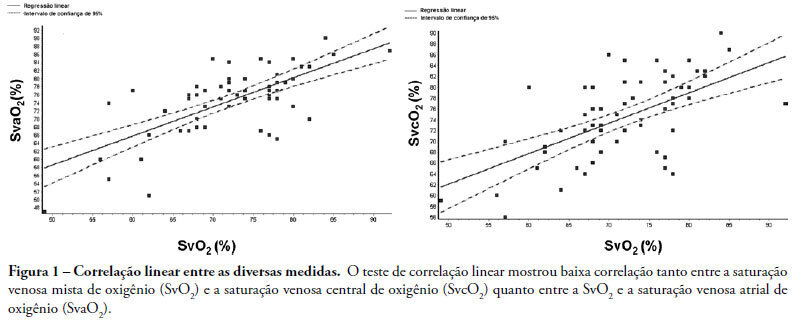
INTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
INTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):325-330
DOI 10.1590/S0103-507X2008000400002
OBJECTIVES: Sedation scores are important tools for use in pediatric intensive care units. The Comfort-Behavior scale is a valid method for the assessment of children although it is considered an extensive scale. The motor activity assessment scale is validated for an adult population. We considered it simpler then the one above and suitable for application in children. None of these scores had been translated into Portuguese. Our objective was to apply both scales in Portuguese to a pediatric population under mechanical ventilation. Secondary objectives were to evaluate the sedation level of children on mechanical ventilation in tertiary pediatric intensive care units and to compare the Comfort- Behavior and motor activity assessment scales in this population. METHODS: After translating the scales into Portuguese, both were simultaneously applied to 26 patients by 2 pediatricians. Each scale was applied 116 times in total. RESULTS: The intraclass correlation coefficient was 0.90 (0.85 - 0.93 CI 95%) for the Comfort-Behavior and 0.94 (0.92 - 0.96 CI 95%) for the motor activity assessment scale. When applying the Comfort-Behavior scale, the Crombach's alpha was 0.81 for observer A and 0.92 for observer B. The Spearman coefficient was 0.86 for observer A and 0.91 for observer B. These patients were found to be deeply sedated, showing low values in both scales. CONCLUSIONS: The scales were successfully translated into Portuguese and both were adequate to assess pain and sedation in the pediatric population under mechanical ventilation. Sedation level was high in this sample of applications.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):325-330
DOI 10.1590/S0103-507X2008000400002
OBJECTIVES: Sedation scores are important tools for use in pediatric intensive care units. The Comfort-Behavior scale is a valid method for the assessment of children although it is considered an extensive scale. The motor activity assessment scale is validated for an adult population. We considered it simpler then the one above and suitable for application in children. None of these scores had been translated into Portuguese. Our objective was to apply both scales in Portuguese to a pediatric population under mechanical ventilation. Secondary objectives were to evaluate the sedation level of children on mechanical ventilation in tertiary pediatric intensive care units and to compare the Comfort- Behavior and motor activity assessment scales in this population. METHODS: After translating the scales into Portuguese, both were simultaneously applied to 26 patients by 2 pediatricians. Each scale was applied 116 times in total. RESULTS: The intraclass correlation coefficient was 0.90 (0.85 - 0.93 CI 95%) for the Comfort-Behavior and 0.94 (0.92 - 0.96 CI 95%) for the motor activity assessment scale. When applying the Comfort-Behavior scale, the Crombach's alpha was 0.81 for observer A and 0.92 for observer B. The Spearman coefficient was 0.86 for observer A and 0.91 for observer B. These patients were found to be deeply sedated, showing low values in both scales. CONCLUSIONS: The scales were successfully translated into Portuguese and both were adequate to assess pain and sedation in the pediatric population under mechanical ventilation. Sedation level was high in this sample of applications.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
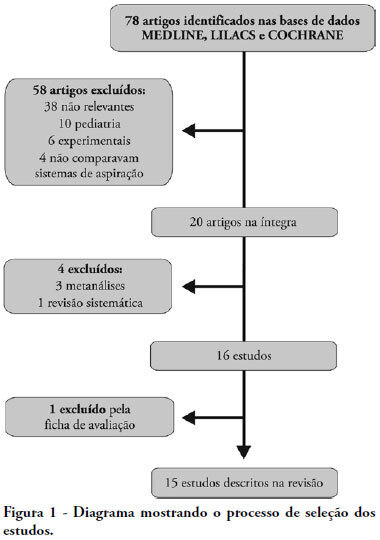
OBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):331-338
DOI 10.1590/S0103-507X2008000400003
OBJECTIVES: This study attempted to identify which is the more effective suction system. The objective was to compare open versus closed suction systems according to a systematic review. METHODS: A search of scientific literature was conducted in MedLine, LILACS and Cochrane between 1997 and August 2007 using the key words: endotracheal suction and closed suction. Included were articles that compared the open and closed suction systems used in adult humans and that were randomized and controlled trials. RESULTS: From the 78 articles identified, only 15 were accepted and described in this review. Nine compared incidence of ventilator-associated pneumonia, six compared oxygen saturation, four compared blood pressure and heart rate, three compared pulmonary volumes, two compared secretion removal and four compared costs. No difference was found in these variables compared: incidence of ventilator associated pneumonia, mortality, intensive care unit length of stay, duration of mechanical ventilation, PaCO2, PaO2, mean blood pressure, heart rate and secretion removal. However, there were always SpO2 and pulmonary volume decreases when using the open suction system; and costs were lower in most of the studies that used the closed suction system. CONCLUSIONS: Closed suction system seems to increase the risk of colonization, but has the advantage of not reducing the pulmonary volumes and not entailing a drop of saturation, especially in patients with severe respiratory failure and in the use of higher levels of positive end expiratory pressure.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
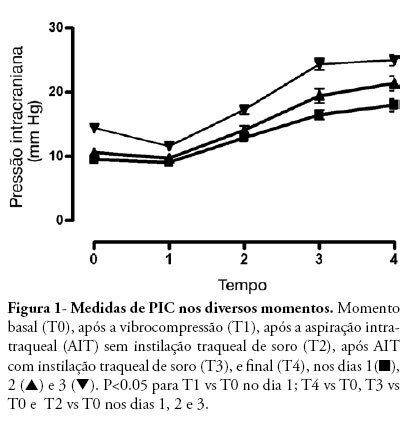
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):339-343
DOI 10.1590/S0103-507X2008000400004
OBJECTIVE: After brain injury intracranial hypertension is the major cause of mortality, in addition to the possibility of functional, behavioral and cognitive sequels. Scarcity of studies on the effects of respiratory physiotherapy on these patients may lead to contradictory performances. This study aimed to assess the effects of customary respiratory physiotherapy maneuvers on intracranial and cerebral perfusion pressures in patients with severe brain injury. METHODS: Clinical, prospective trial with patients with severe traumatic brain injury, mechanically ventilated and with a continued measurement of intracranial pressure. The effects of manual vibrocompression maneuvers and intratracheal aspiration with or without saline infusion on the measurements of intracranial and cerebral perfusion pressures, between the first and third day after cerebral injury were evaluated. RESULTS: Data were collected from 11 patients, 41 years of age (median) and APACHE II of 19.5 ± 5. The manual vibrocompression maneuver did not cause an increase of intracranial pressure on any of the days assessed. Intracranial pressure significantly increased after intratracheal aspiration maneuvers in relation to the basal measurement (day1, 9.5 ± 0.9 mm Hg vs 18.0 ± 3.2 mm Hg; day 2, 10.6 ± 1.7 mm Hg vs 21.4 ± 3.8 mm Hg; day 3, 14.4 ± 1.0 vs 24.9 ± 2.7 mm Hg; p<0.05 for all). However, these elevations were transient (about 27 seconds) and accompanied by compensatory increases of the cerebral perfusion pressure. CONCLUSION: The manual vibrocompression maneuver did not increase intracranial pressure or cerebral perfusion pressure in patients with severe brain injury. Intratracheal aspiration induced a significant and transient increase of the intracranial and cerebral perfusion pressures.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
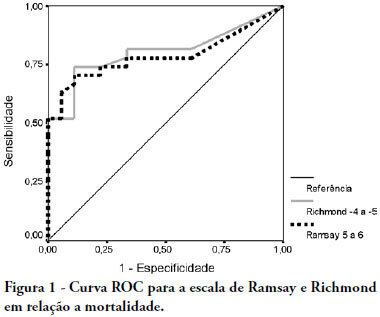
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):344-348
DOI 10.1590/S0103-507X2008000400005
OBJECTIVE: The main purpose of this study was to compare performance of the Ramsay and Richmond sedation scores on mechanically ventilated critically ill patients, in a university-affiliated hospital. METHODS: This was a 4-month prospective study, which included a total of 45 patients mechanically ventilated, with at least 48 hours stay in the intensive care unit. Each patient was assessed daily for sedation mode, sedative and analgesic doses and sedation level using the Ramsay and Richmond scores. Statistical analysis was made using Student's t-test, Pearson's and Spearman's correlation, and constructing ROC-curves. RESULTS: A high general mortality of 60% was observed. The length of sedation and daily dose of medication did not correlate with mortality. Deep sedation (Ramsay > 4 or Richmond < -3) was positively correlated with probability of death with an AUC > 0.78. An adequate level of sedation (Ramsay 2 to 4 or Richmond 0 to -3) was sensitively correlated with probability of survival with an AUC > 0.80. A low level of sedation was observed in 63 days evaluated (8.64%), and no correlation was found between occurrence of agitation and unfavorable outcomes. Correlation between Ramsay and Richmond scores (Pearson's > 0.810 - p<0.0001) was good. CONCLUSION: In this study, Ramsay and Richmond sedation scores were similar for the assessment of deep, insufficient and adequate sedation. Both have good correlation with mortality in over sedated patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
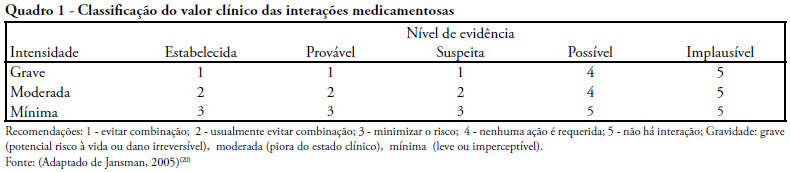
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.