Respiration, artificial Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.

Abstract
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
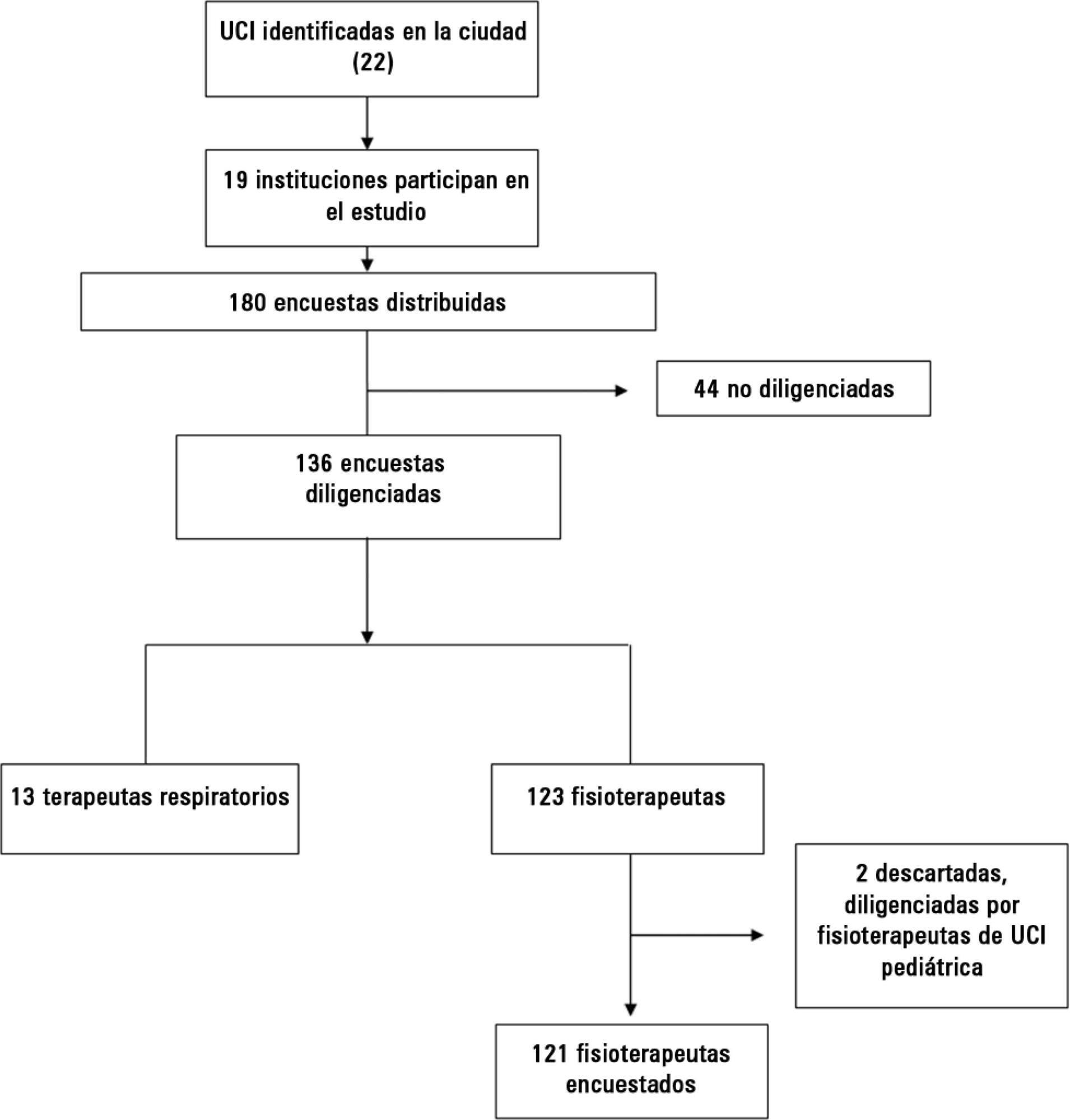
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
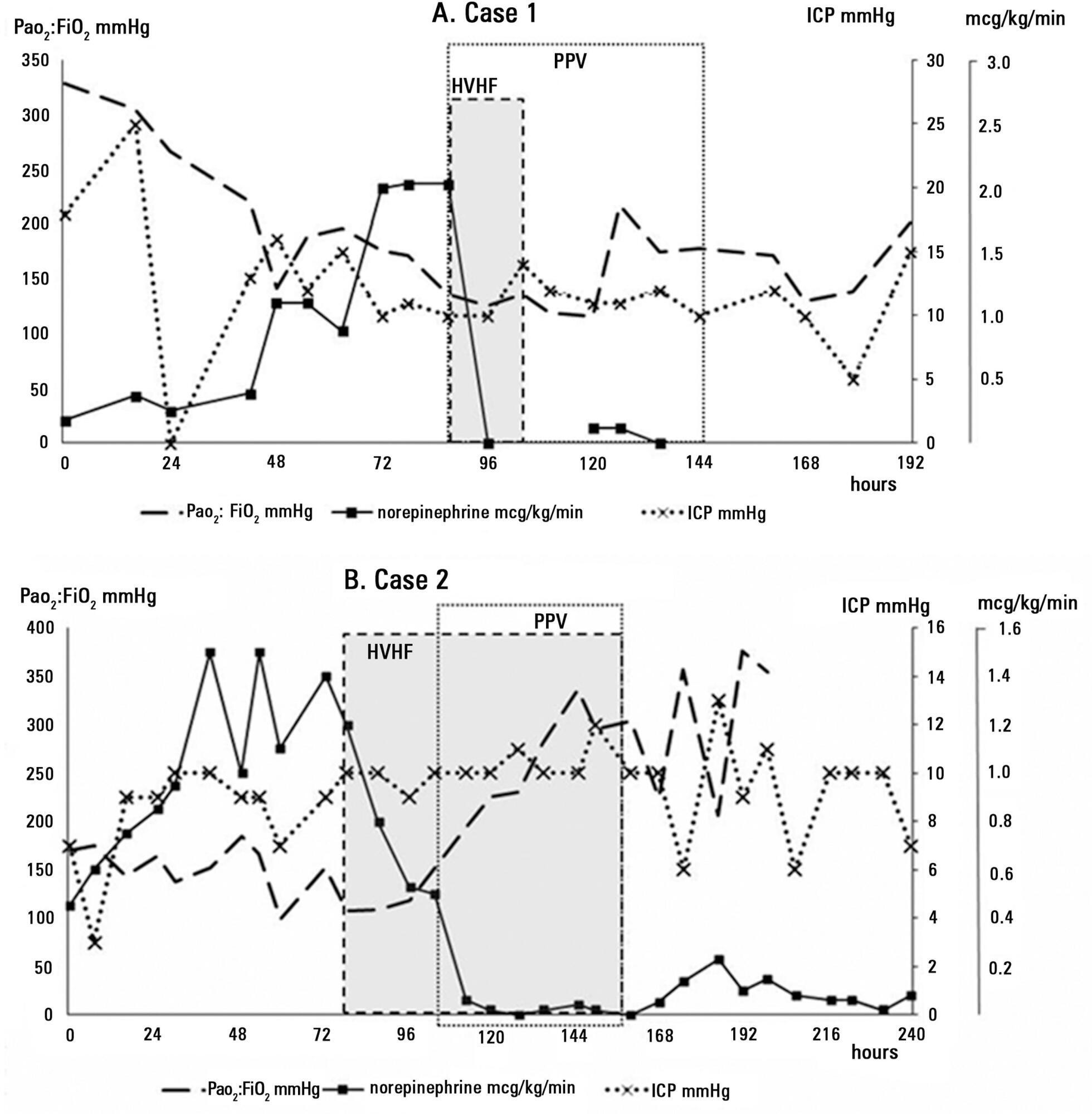
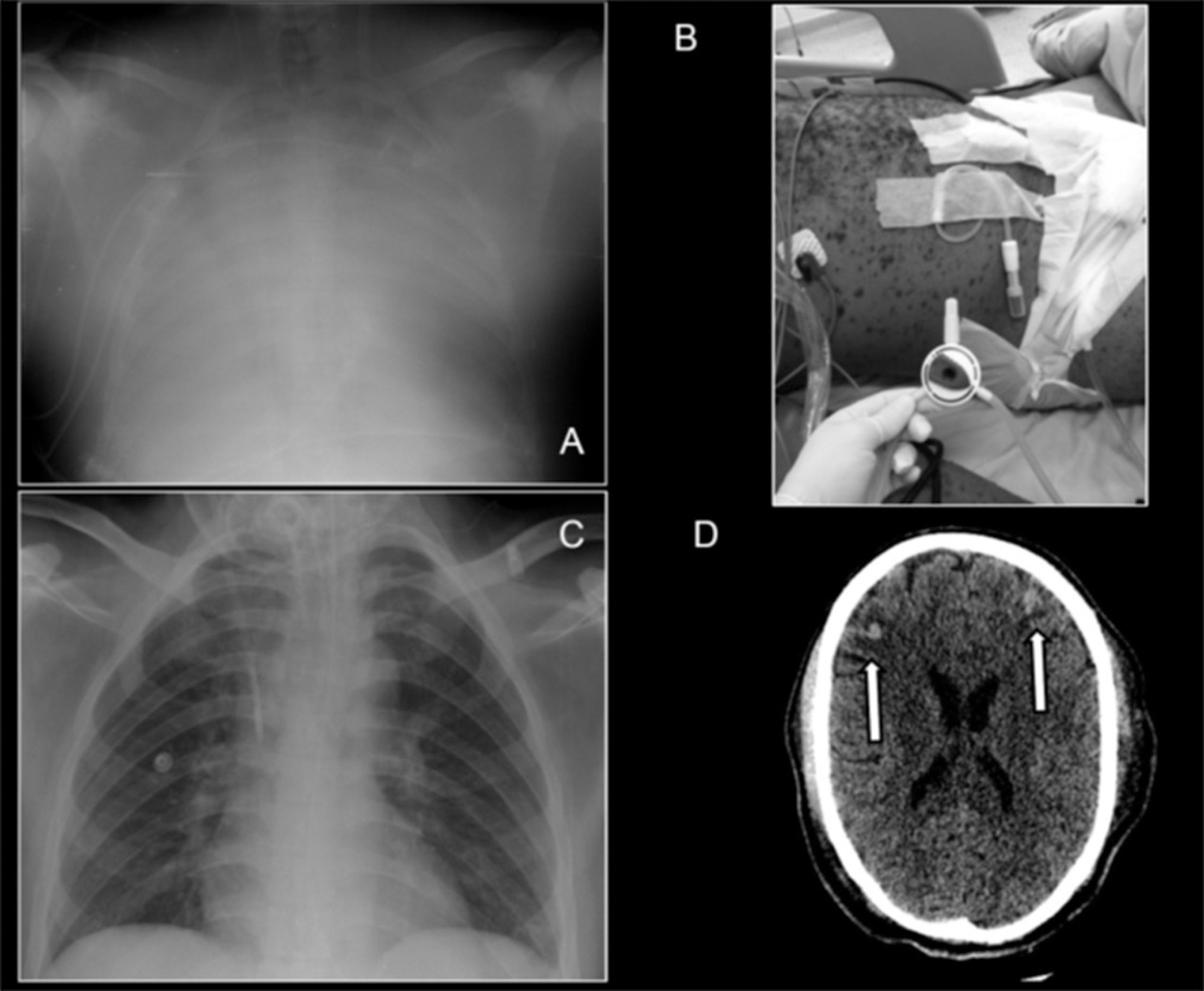
We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):51-56
DOI 10.5935/0103-507X.20140008
To identify risk factors for extubation failure and reintubation in newborn infants subjected to mechanical ventilation and to establish whether ventilation parameters and blood gas analysis behave as predictors of those outcomes.
Prospective study conducted at a neonatal intensive care unit from May to November 2011. A total of 176 infants of both genders subjected to mechanical ventilation were assessed after extubation. Extubation failure was defined as the need to resume mechanical ventilation within less than 72 hours. Reintubation was defined as the need to reintubate the infants any time after the first 72 hours.
Based on the univariate analysis, the variables gestational age <28 weeks, birth weight <1,000g and low Apgar scores were associated with extubation failure and reintubation. Based on the multivariate analysis, the variables length of mechanical ventilation (days), potential of hydrogen (pH) and partial pressure of oxygen (pO2) remained associated with extubation failure, and the five-minute Apgar score and age at extubation were associated with reintubation.
Low five-minute Apgar scores, age at extubation, length of mechanical ventilation, acid-base disorders and hyperoxia exhibited associations with the investigated outcomes of extubation failure and reintubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):51-56
DOI 10.5935/0103-507X.20140008
To identify risk factors for extubation failure and reintubation in newborn infants subjected to mechanical ventilation and to establish whether ventilation parameters and blood gas analysis behave as predictors of those outcomes.
Prospective study conducted at a neonatal intensive care unit from May to November 2011. A total of 176 infants of both genders subjected to mechanical ventilation were assessed after extubation. Extubation failure was defined as the need to resume mechanical ventilation within less than 72 hours. Reintubation was defined as the need to reintubate the infants any time after the first 72 hours.
Based on the univariate analysis, the variables gestational age <28 weeks, birth weight <1,000g and low Apgar scores were associated with extubation failure and reintubation. Based on the multivariate analysis, the variables length of mechanical ventilation (days), potential of hydrogen (pH) and partial pressure of oxygen (pO2) remained associated with extubation failure, and the five-minute Apgar score and age at extubation were associated with reintubation.
Low five-minute Apgar scores, age at extubation, length of mechanical ventilation, acid-base disorders and hyperoxia exhibited associations with the investigated outcomes of extubation failure and reintubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
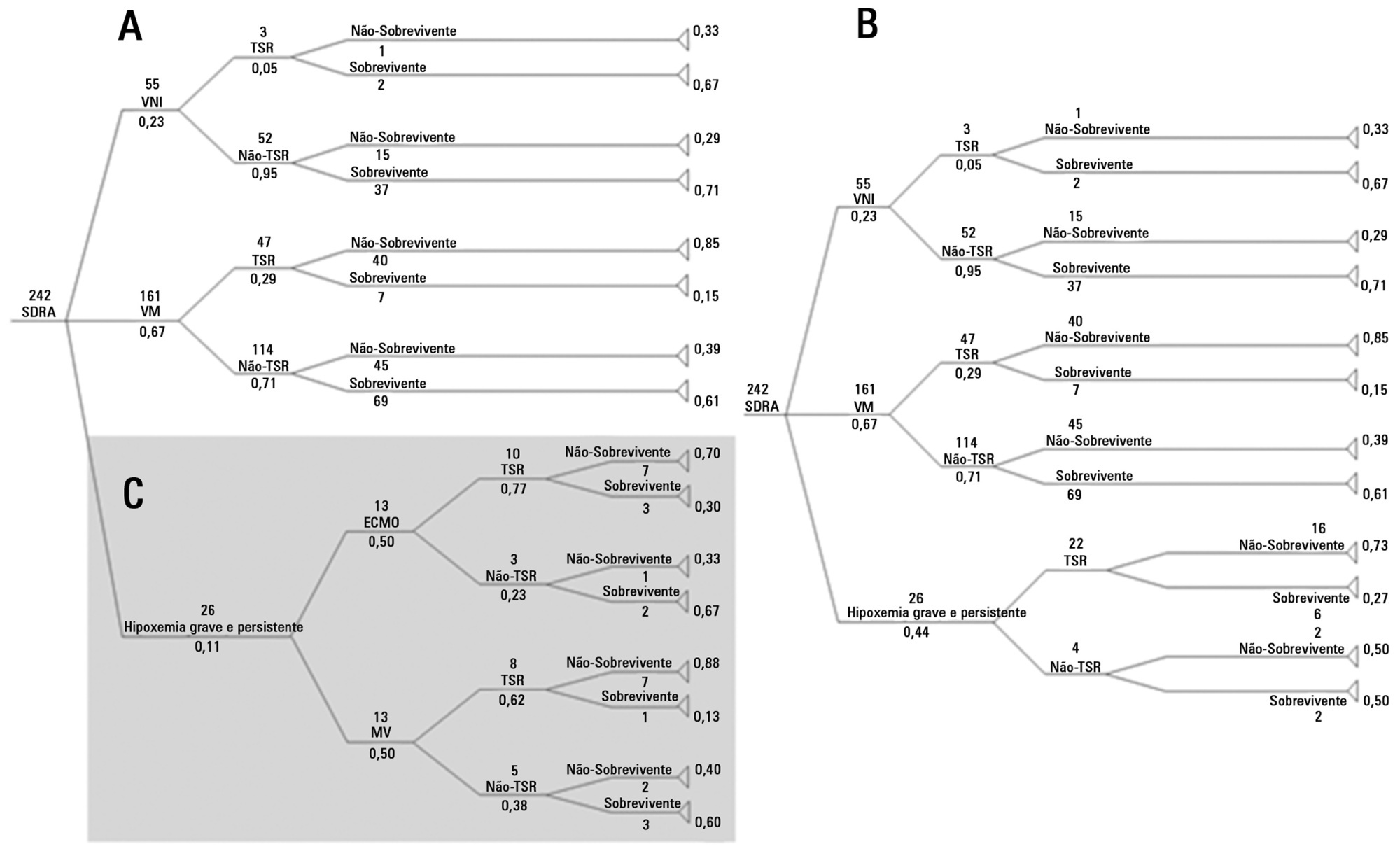
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):367-372
DOI 10.5935/0103-507X.20140056
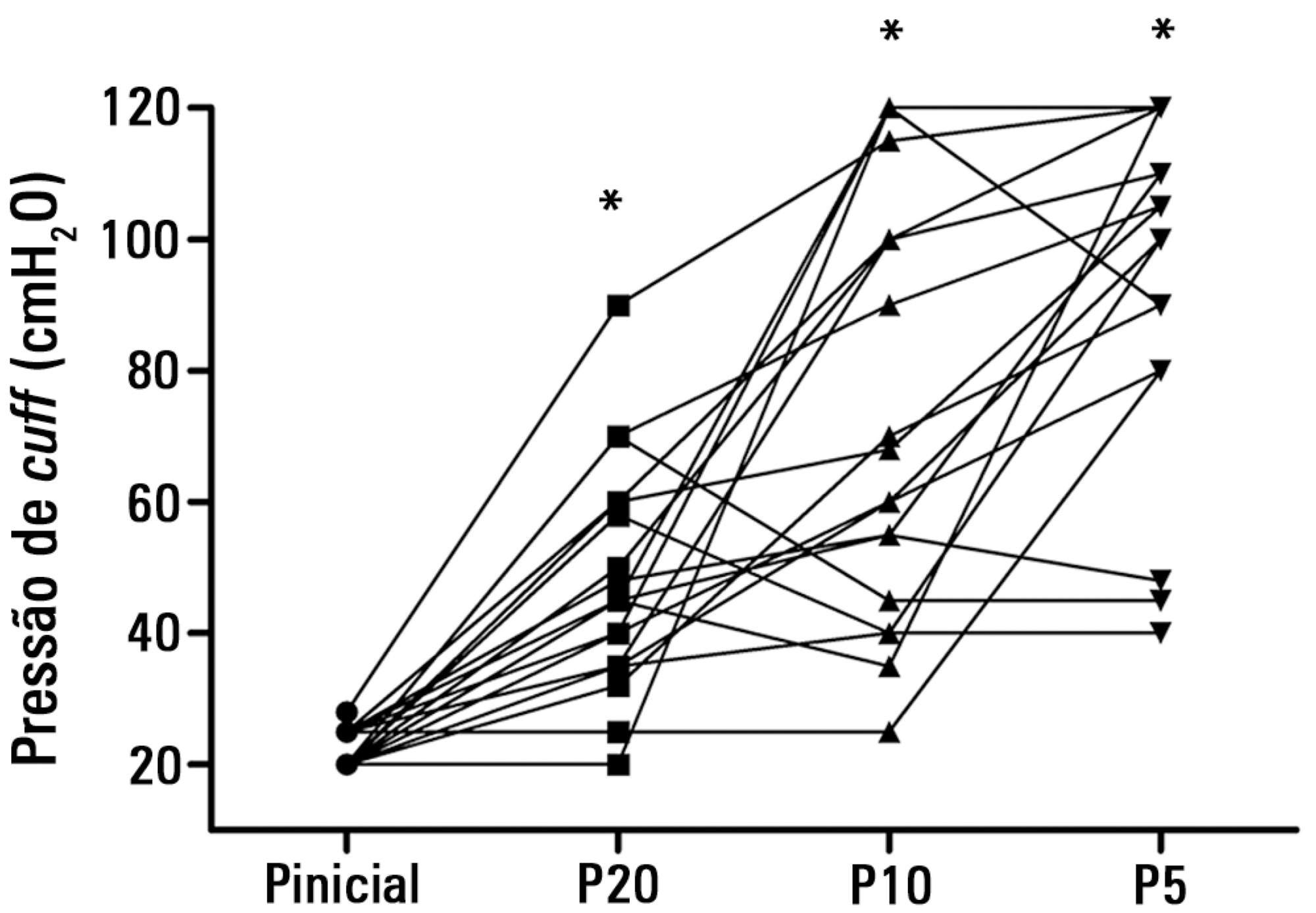
To test the effectiveness of using a cuff pressure relief valve technique to maintain cuff pressure levels within the normal in vitro range (Phase 1) in patients admitted to the intensive care unit (Phase 2) and to test the reproducibility of the technique using different syringes.
In Phase 1, a tracheal tube was inserted into a trachea model. Ten- and 20mL syringes were used to inflate the cuff through the tracheal tube. The cuff was slowly and steadily inflated until the syringe plunger would move in the opposite direction of the application. After the plunger stopped, the cuff pressures were recorded. In Phase 2, the same maneuvers for inflating the cuff were performed on 20 patients using 5, 10, and 20mL syringes and were compared with manometer measurements. The intraclass correlation coefficient and Bland-Altman analysis were employed to determine the reproducibility and agreement between syringes. Data were expressed as medians (interquartile range).
There was no reproducibility between syringes with an intraclass correlation coefficient ranging between -0.33 and 0.8 (p>0.05). The pressures generated with the syringes were higher than the pressures generated using a standard manometer: the 5mL syringe pressure was 105cmH2O (82.5-120cmH2O), the 10mL syringe pressure was 69cmH2O (47.5-111.3cmH2O), and the 20mL syringe pressure was 45cmH2O (35-59.5cmH2O). The Bland-Altman analysis confirmed the large bias and variability between the syringes used, compared with the manometer.
The use of syringes is not an effective technique for determining the cuff pressure in patients admitted to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):367-372
DOI 10.5935/0103-507X.20140056
To test the effectiveness of using a cuff pressure relief valve technique to maintain cuff pressure levels within the normal in vitro range (Phase 1) in patients admitted to the intensive care unit (Phase 2) and to test the reproducibility of the technique using different syringes.
In Phase 1, a tracheal tube was inserted into a trachea model. Ten- and 20mL syringes were used to inflate the cuff through the tracheal tube. The cuff was slowly and steadily inflated until the syringe plunger would move in the opposite direction of the application. After the plunger stopped, the cuff pressures were recorded. In Phase 2, the same maneuvers for inflating the cuff were performed on 20 patients using 5, 10, and 20mL syringes and were compared with manometer measurements. The intraclass correlation coefficient and Bland-Altman analysis were employed to determine the reproducibility and agreement between syringes. Data were expressed as medians (interquartile range).
There was no reproducibility between syringes with an intraclass correlation coefficient ranging between -0.33 and 0.8 (p>0.05). The pressures generated with the syringes were higher than the pressures generated using a standard manometer: the 5mL syringe pressure was 105cmH2O (82.5-120cmH2O), the 10mL syringe pressure was 69cmH2O (47.5-111.3cmH2O), and the 20mL syringe pressure was 45cmH2O (35-59.5cmH2O). The Bland-Altman analysis confirmed the large bias and variability between the syringes used, compared with the manometer.
The use of syringes is not an effective technique for determining the cuff pressure in patients admitted to the intensive care unit.