Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
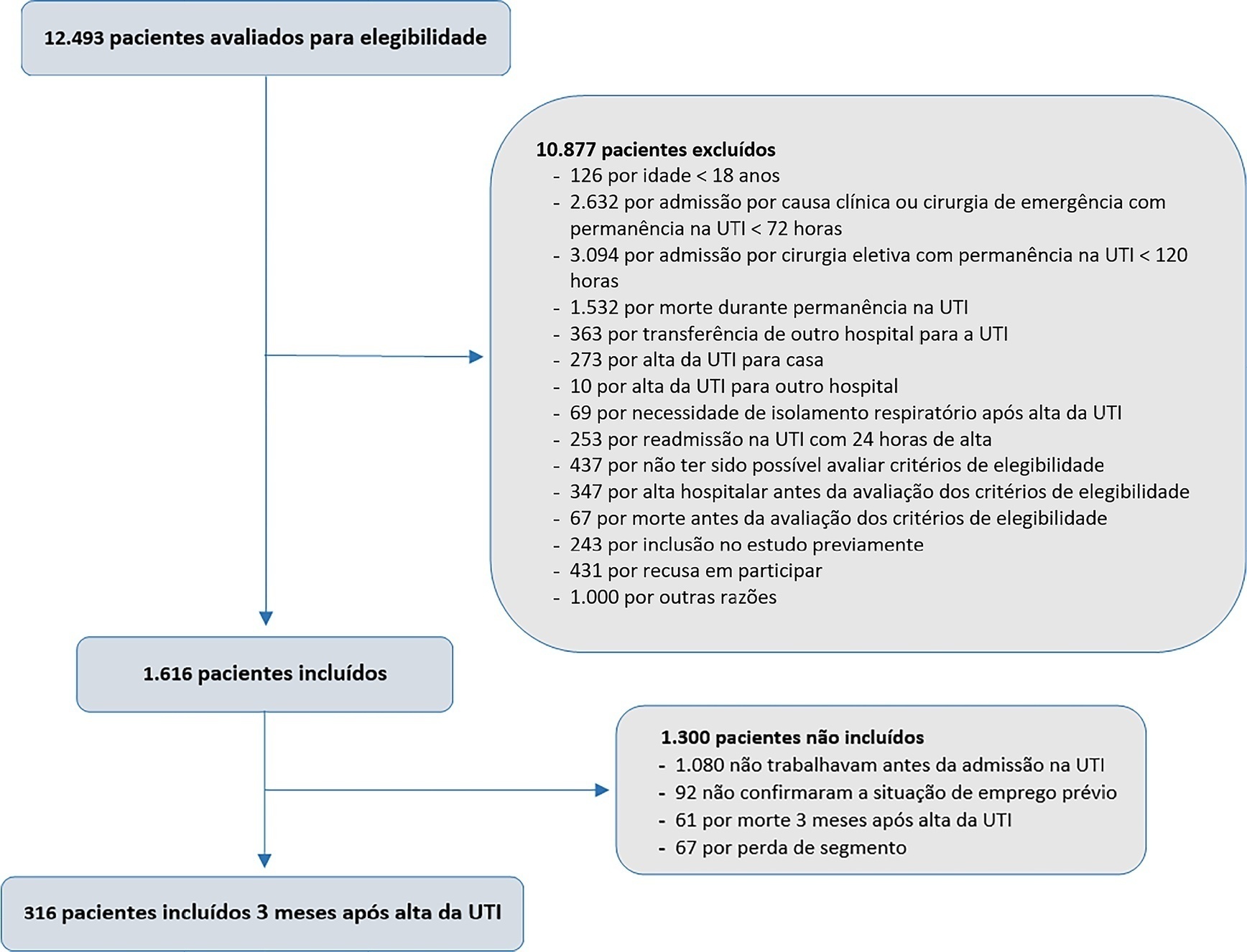
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 - 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 - 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 - 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 - 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):492-498
DOI 10.5935/0103-507X.20220169-en
To describe the rate and factors related to nonreturn to work in the third month after discharge from the intensive care unit and the impact of unemployment, loss of income and health care expenses for survivors.
This was a prospective multicenter cohort study that included survivors of severe acute illness who were hospitalized between 2015 and 2018, previously employed, and who stayed more than 72 hours in the intensive care unit. Outcomes were assessed by telephone interview in the third month after discharge.
Of the 316 patients included in the study who had previously worked, 193 (61.1%) did not return to work within 3 months after discharge from the intensive care unit. The following factors were associated with nonreturn to work: low educational level (prevalence ratio 1.39; 95%CI 1.10 - 1.74; p = 0.006), previous employment relationship (prevalence ratio 1.32; 95%CI 1 10 - 1.58; p = 0.003), need for mechanical ventilation (prevalence ratio 1.20; 95%CI 1.01 - 1.42; p = 0.04) and physical dependence in the third month after discharge (prevalence ratio 1.27; 95%CI 1.08 - 1.48; p = 0.003). Survivors who were unable to return to work more often had reduced family income (49.7% versus 33.3%; p = 0.008) and increased health expenditures (66.9% versus 48.3%; p = 0.002). compared to those who returned to work in the third month after discharge from the intensive care unit.
Intensive care unit survivors often do not return to work until the third month after discharge from the intensive care unit. Low educational level, formal job, need for ventilatory support and physical dependence in the third month after discharge were related to nonreturn to work. Failure to return to work was also associated with reduced family income and increased health care costs after discharge.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
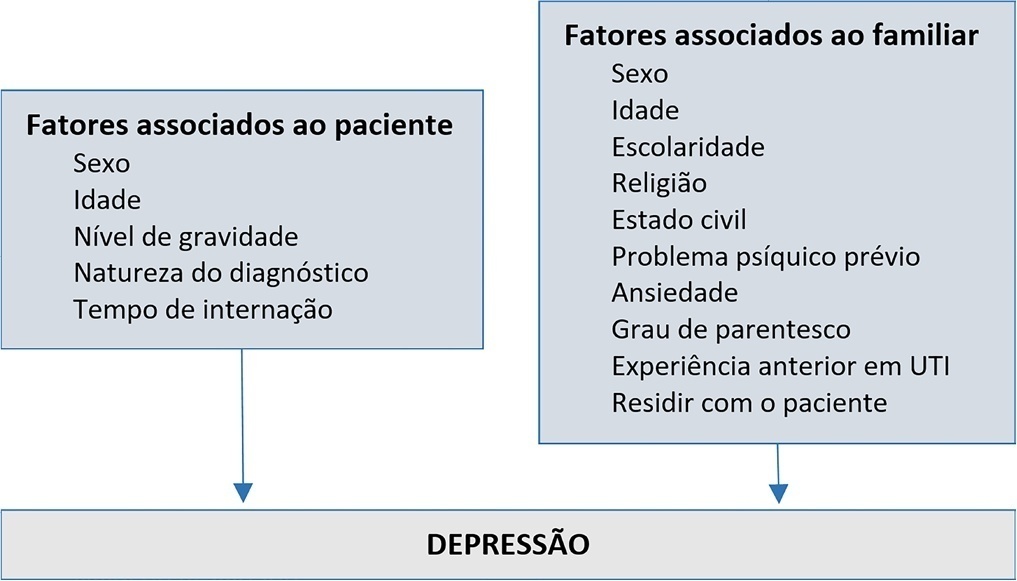
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):499-506
DOI 10.5935/0103-507X.20220080-en
To evaluate the prevalence and factors associated with depression in family members of people hospitalized in intensive care units.
A cross-sectional study was conducted with 980 family members of patients admitted to the intensive care units of a large public hospital in the interior of Bahia. Depression was measured using the Patient Health Questionnaire-8. The multivariate model consisted of the following variables: sex and age of the patient, sex and age of the family member, education level, religion, living with the family member, previous mental illness and anxiety.
Depression had a prevalence of 43.5%. In the multivariate analysis, the model with the best representativeness indicated that factors associated with a higher prevalence of depression were being female (39%), age younger than 40 years (26%) and previous mental illness (38%). A higher education level was associated with a 19% lower prevalence of depression in family members.
The increase in the prevalence of depression was associated with female sex, age younger than 40 years and previous psychological problems. Such elements should be valued in actions aimed at family members of people hospitalized in intensive care.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
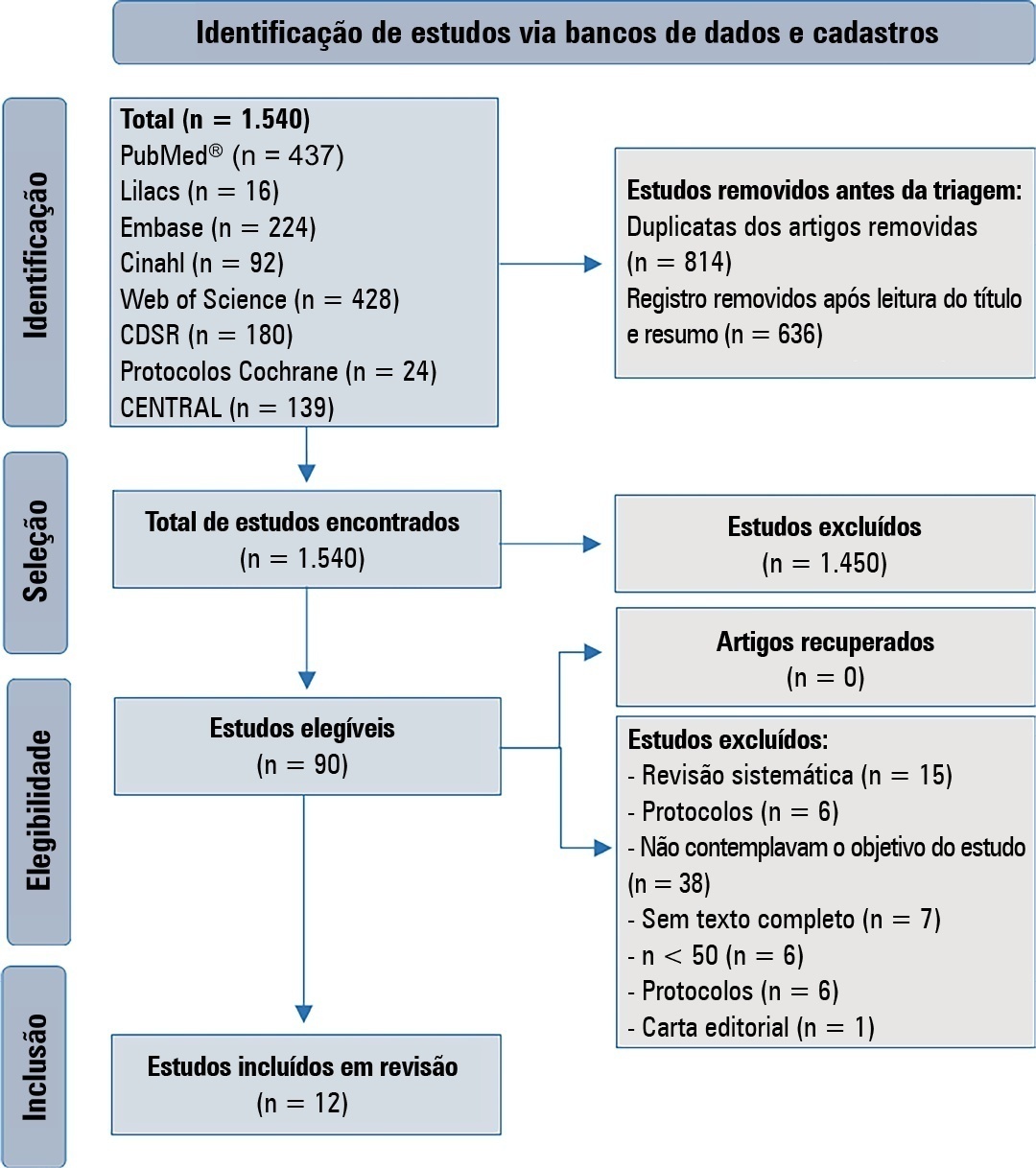
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2022;34(4):507-518
DOI 10.5935/0103-507X.20220145-en
To verify strategies for the prevention and treatment of abstinence syndrome in a pediatric intensive care unit.
This is a systematic review in the PubMed database®, Lilacs, Embase, Web of Science, Cochrane, Cinahl, Cochrane Database Systematic Review and CENTRAL. A three-step search strategy was used for this review, and the protocol was approved in PROSPERO (CRD42021274670).
Twelve articles were included in the analysis. There was great heterogeneity among the studies included, especially regarding the therapeutic regimens used for sedation and analgesia. Midazolam doses ranged from 0.05mg/kg/hour to 0.3mg/kg/hour. Morphine also varied considerably, from 10mcg/kg/hour to 30mcg/kg/hour, between studies. Among the 12 selected studies, the most commonly used scale for the identification of withdrawal symptoms was the Sophia Observational Withdrawal Symptoms Scale. In three studies, there was a statistically significant difference in the prevention and management of the withdrawal syndrome due to the implementation of different protocols (p < 0.01 and p < 0.001).
There was great variation in the sedoanalgesia regimen used by the studies and the method of weaning and evaluation of withdrawal syndrome. More studies are needed to provide more robust evidence about the most appropriate treatment for the prevention and reduction of withdrawal signs and symptoms in critically ill children.
CRD 42021274670
Abstract
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
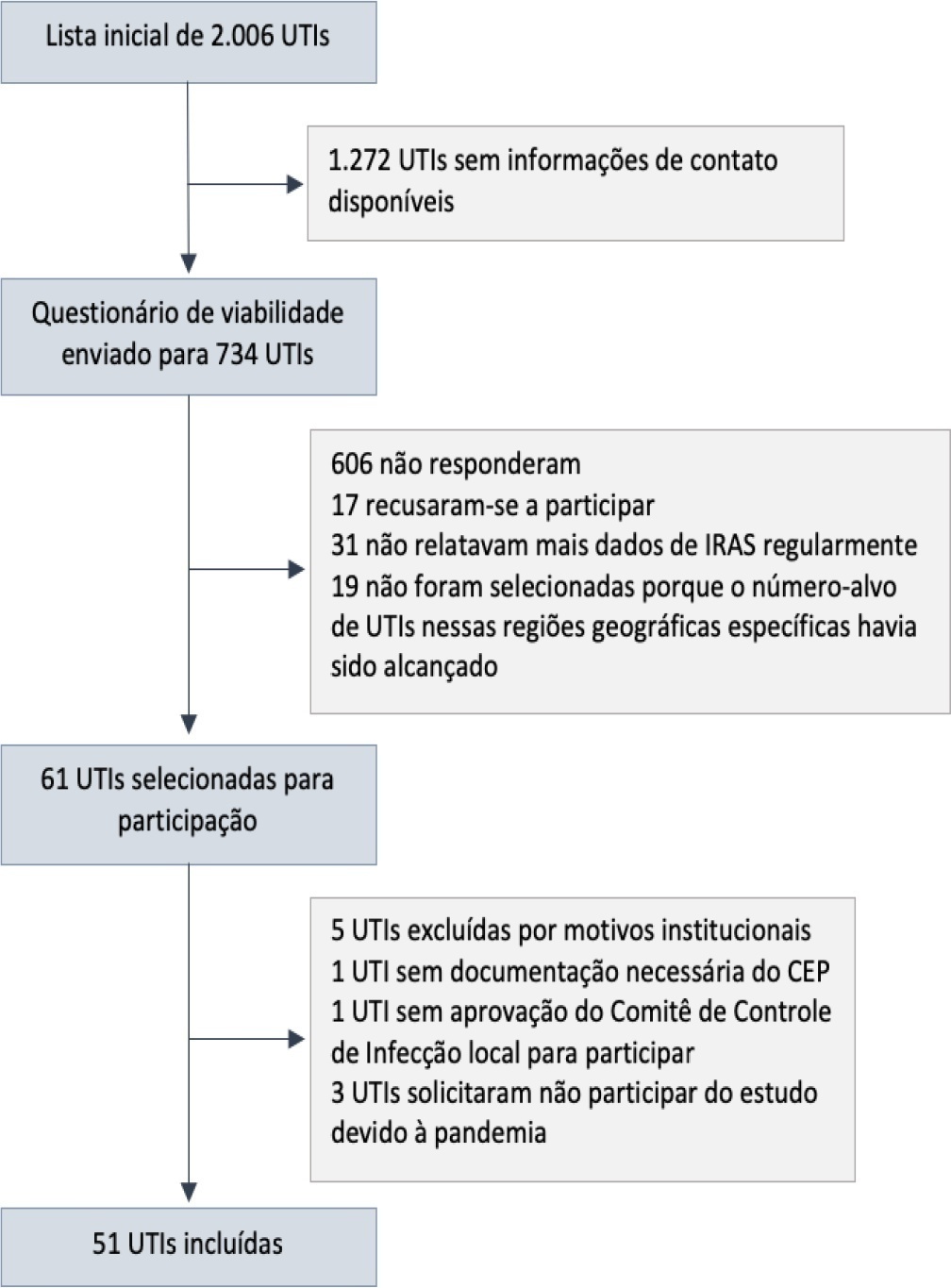
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):418-425
DOI 10.5935/0103-507X.20220209-en
To describe the IMPACTO-MR, a Brazilian nationwide intensive care unit platform study focused on the impact of health care-associated infections due to multidrug-resistant bacteria.
We described the IMPACTO-MR platform, its development, criteria for intensive care unit selection, characterization of core data collection, objectives, and future research projects to be held within the platform.
The core data were collected using the Epimed Monitor System® and consisted of demographic data, comorbidity data, functional status, clinical scores, admission diagnosis and secondary diagnoses, laboratory, clinical, and microbiological data, and organ support during intensive care unit stay, among others. From October 2019 to December 2020, 33,983 patients from 51 intensive care units were included in the core database.
The IMPACTO-MR platform is a nationwide Brazilian intensive care unit clinical database focused on researching the impact of health care-associated infections due to multidrug-resistant bacteria. This platform provides data for individual intensive care unit development and research and multicenter observational and prospective trials.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
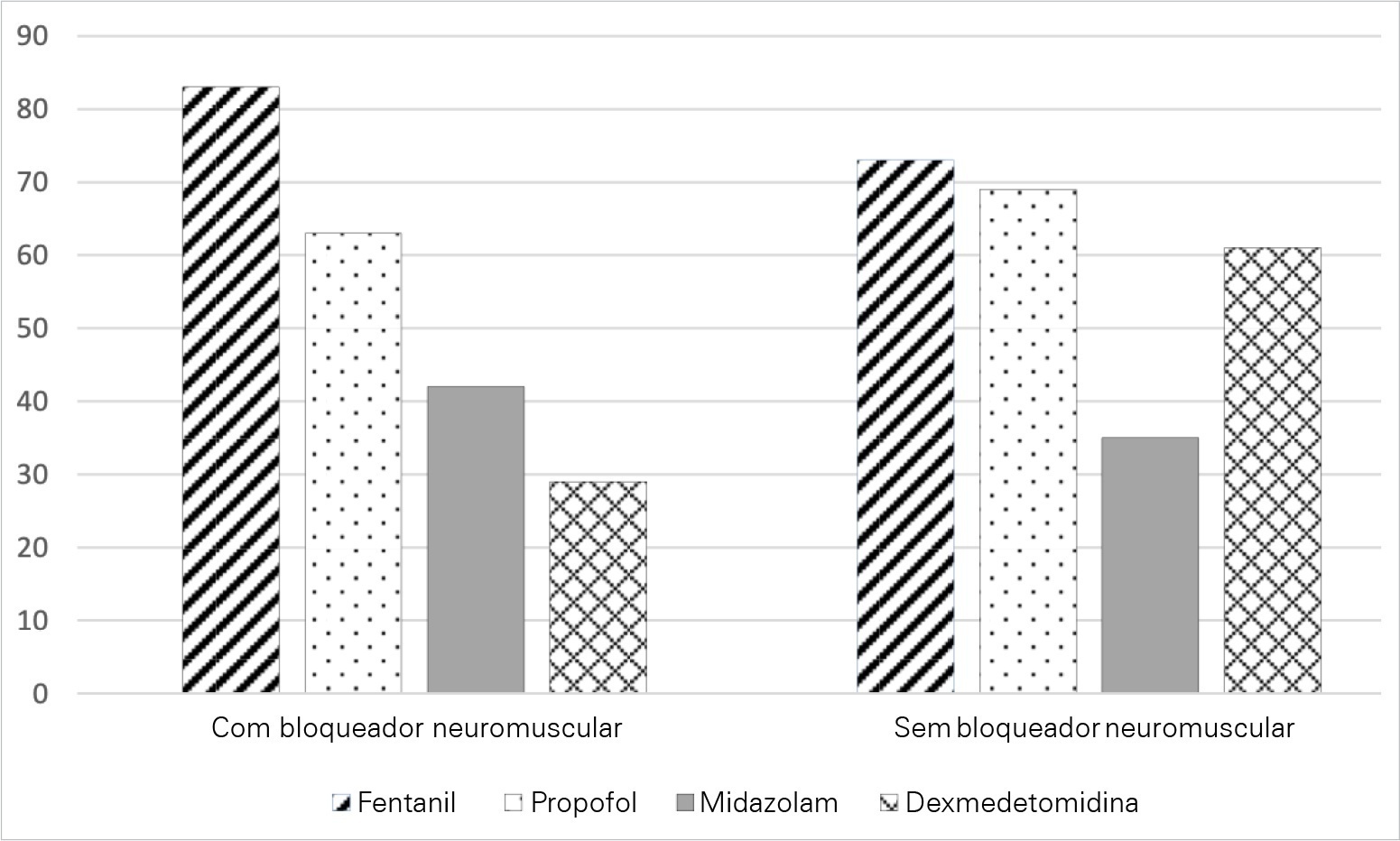
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2022;34(4):426-432
DOI 10.5935/0103-507X.20220278-en
To characterize the knowledge and perceived attitudes toward pharmacologic interventions for light sedation in mechanically ventilated patients and to understand the current gaps comparing current practice with the recommendations of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the Intensive Care Unit.
This was a cross-sectional cohort study based on the application of an electronic questionnaire focused on sedation practices.
A total of 303 critical care physicians provided responses to the survey. Most respondents reported routine use of a structured sedation scale (281; 92.6%). Almost half of the respondents reported performing daily interruptions of sedation (147; 48.4%), and the same percentage of participants (48.0%) agreed that patients are often over sedated. During the COVID-19 pandemic, participants reported that patients had a higher chance of receiving midazolam compared to before the pandemic (178; 58.8% versus 106; 34.0%; p = 0.05), and heavy sedation was more common during the COVID-19 pandemic (241; 79.4% versus 148; 49.0%; p = 0.01).
This survey provides valuable data on the perceived attitudes of Brazilian intensive care physicians regarding sedation. Although daily interruption of sedation was a well-known concept and sedation scales were often used by the respondents, insufficient effort was put into frequent monitoring, use of protocols and systematic implementation of sedation strategies. Despite the perception of the benefits linked with light sedation, there is a need to identify improvement targets to propose educational strategies to improve current practices.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):386-392
DOI 10.5935/0103-507X.20220446-en
To analyze the association of patient safety culture perceived by nursing professionals with incidents recorded during nursing shifts in intensive care units.
This was a cross-sectional study that investigated patient safety culture measured by the Hospital Survey on Patient Safety Culture instrument. Descriptive statistics, chi-square tests, Student’s t-test and multiple linear regression models were analyzed considering a significance level of 5%.
The study reported a mean of 3.1 (standard deviation of 0.4) for the culture of patient safety in the perception of nursing professionals and 480 incidents with and without damage recorded during the nursing shifts. The variables patient safety culture with a difference between means of 0.543 (95%CI 0.022 - 1.065; p < 0.05) and nursing assistants with a difference between means of -0.133 (95%CI -0.192 - -0.074; p < 0.05) were associated with the incidents recorded during the nursing shifts. Further, nursing assistants had a lower tendency to record incidents than did the nurses.
The strengthening of the patient safety culture and the aspects tangential to the nursing professionals represent a possible target for interventions to encourage the recording of incidents during the nursing shift shifts and improve patient safety.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):386-392
DOI 10.5935/0103-507X.20220446-en
To analyze the association of patient safety culture perceived by nursing professionals with incidents recorded during nursing shifts in intensive care units.
This was a cross-sectional study that investigated patient safety culture measured by the Hospital Survey on Patient Safety Culture instrument. Descriptive statistics, chi-square tests, Student’s t-test and multiple linear regression models were analyzed considering a significance level of 5%.
The study reported a mean of 3.1 (standard deviation of 0.4) for the culture of patient safety in the perception of nursing professionals and 480 incidents with and without damage recorded during the nursing shifts. The variables patient safety culture with a difference between means of 0.543 (95%CI 0.022 - 1.065; p < 0.05) and nursing assistants with a difference between means of -0.133 (95%CI -0.192 - -0.074; p < 0.05) were associated with the incidents recorded during the nursing shifts. Further, nursing assistants had a lower tendency to record incidents than did the nurses.
The strengthening of the patient safety culture and the aspects tangential to the nursing professionals represent a possible target for interventions to encourage the recording of incidents during the nursing shift shifts and improve patient safety.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
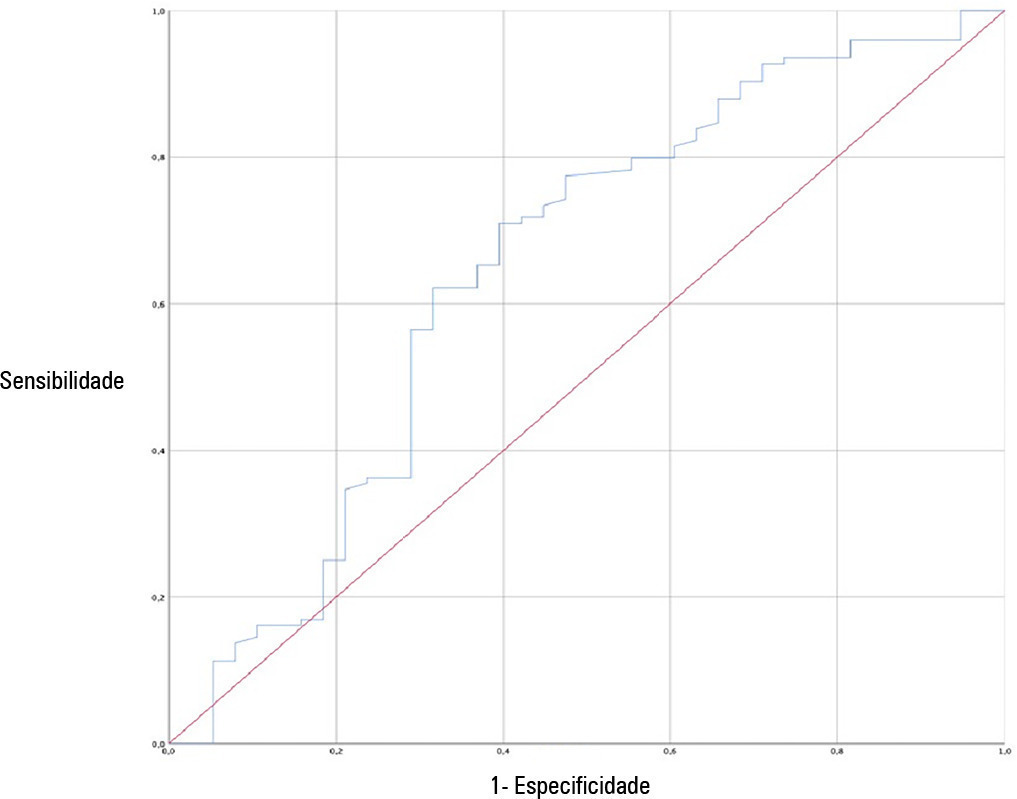
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):360-366
DOI 10.5935/0103-507X.20220477-en
To investigate the applicability of the Respiratory Rate-Oxygenation Index to identify the risk of high-flow nasal cannula failure in post-extubation pneumonia patients.
This was a 2-year retrospective observational study conducted in a reference hospital in Bogotá, Colombia. All patients in whom post-extubation high-flow nasal cannula therapy was used as a bridge to extubation were included in the study. The Respiratory Rate-Oxygenation Index was calculated to assess the risk of post-extubation high-flow nasal cannula failure.
A total of 162 patients were included in the study. Of these, 23.5% developed high-flow nasal cannula failure. The Respiratory Rate-Oxygenation Index was significantly lower in patients who had high-flow nasal cannula failure [median (IQR): 10.0 (7.7 - 14.4) versus 12.6 (10.1 - 15.6); p = 0.006]. Respiratory Rate-Oxygenation Index > 4.88 showed a crude OR of 0.23 (95%CI 0.17 - 0.30) and an adjusted OR of 0.89 (95%CI 0.81 - 0.98) stratified by severity and comorbidity. After logistic regression analysis, the Respiratory Rate-Oxygenation Index had an adjusted OR of 0.90 (95%CI 0.82 - 0.98; p = 0.026). The area under the Receiver Operating Characteristic curve for extubation failure was 0.64 (95%CI 0.53 - 0.75; p = 0.06). The Respiratory Rate-Oxygenation Index did not show differences between patients who survived and those who died during the intensive care unit stay.
The Respiratory Rate-Oxygenation Index is an accessible tool to identify patients at risk of failing high-flow nasal cannula post-extubation treatment. Prospective studies are needed to broaden the utility in this scenario.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
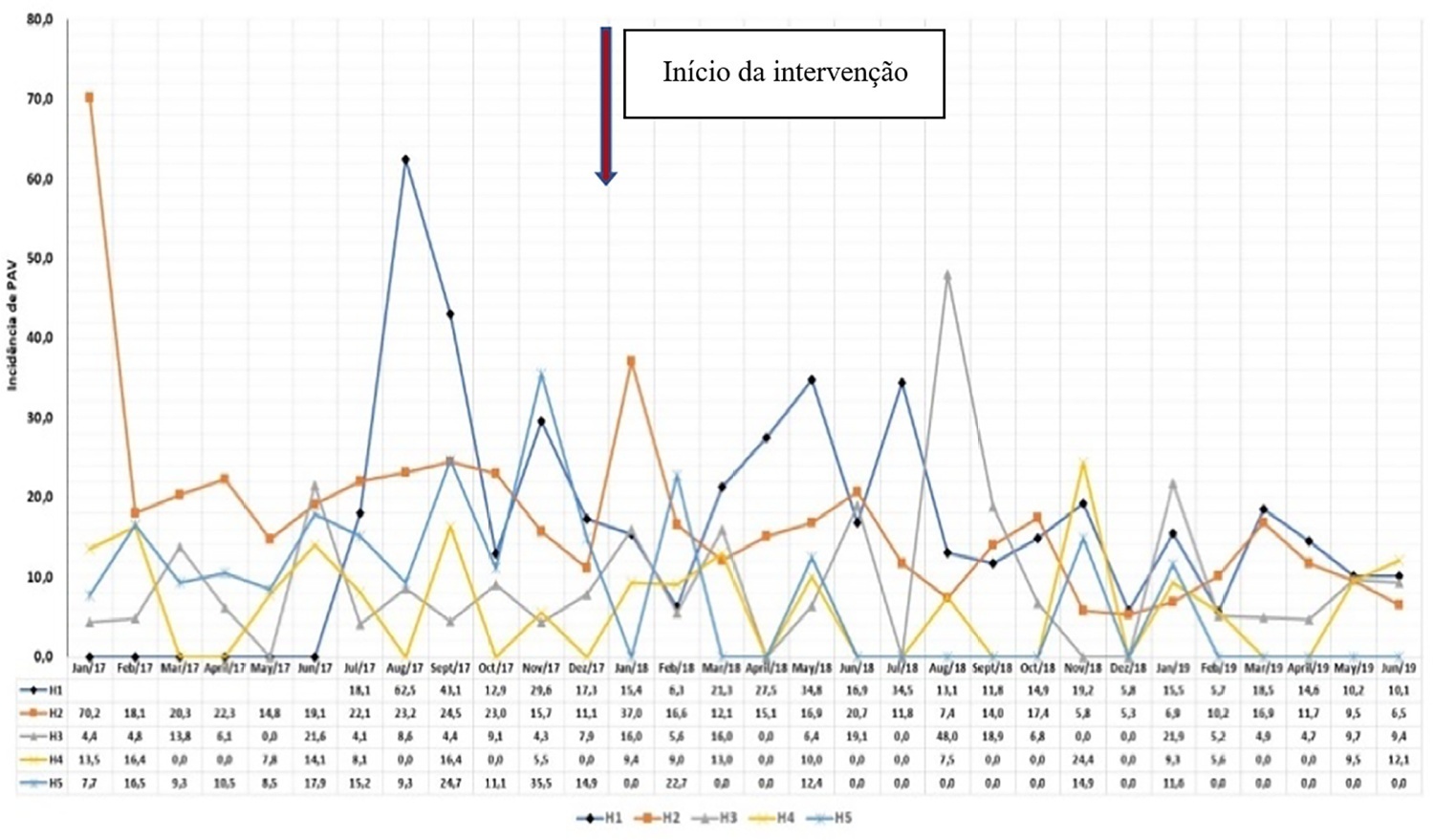
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):327-334
DOI 10.5935/0103-507X.20220070-en
To describe the implementation and results of the collaborative PROADI-SUS project by the Brazilian Ministry of Health to reduce healthcare-associated infections: ventilator-associated pneumonia, primary central line-associated bloodstream infection and catheter-associated urinary tract infections.
This was a prospective observational study that investigated the implementation stages and outcomes during 18 months in five intensive care units in the city of Recife. Reductions in healthcare-associated infections in each unit were calculated using previous medians compared to those of the study period.
The goal of reducing the three healthcare-associated infections, i.e., 30% in 18 months, was achieved in at least one of the healthcare-associated infections and was also achieved for two healthcare-associated infections in two hospitals and three healthcare-associated infections in just one hospital; the latter reached the target of 36 months. Implementing the bundles and monitoring the results by the professionals were considered essential actions by the local management teams. In addition, the acquisition of supplies and their availability alongside the beds, signage, checklists, staff awareness, adaptation, team building, training and celebration of achievements were assessed as being relevant for reducing healthcare-associated infections.
The collaborative approach reduced healthcare-associated infections, despite partial adherence to the bundles. The hypothesis is that success is related to the project methodology and motivated multidisciplinary teams, especially nursing teams.