Echocardiography Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e' ratio, were compared between survivors and non-survivors.
A total of 99 echocardiograms (53 at admission and 46 between days 7 - 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e' ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 - 1.76], p = 0.02).
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):333-339
DOI 10.5935/0103-507X.20150057
To evaluate the prevalence of myocardial dysfunction and its prognostic value in patients with severe sepsis and septic shock.
Adult septic patients admitted to an intensive care unit were prospectively studied using transthoracic echocardiography within the first 48 hours after admission and thereafter on the 7th-10th days. Echocardiographic variables of biventricular function, including the E/e' ratio, were compared between survivors and non-survivors.
A total of 99 echocardiograms (53 at admission and 46 between days 7 - 10) were performed on 53 patients with a mean age of 74 (SD 13) years. Systolic and diastolic dysfunction was present in 14 (26%) and 42 (83%) patients, respectively, and both types of dysfunction were present in 12 (23%) patients. The E/e' ratio, an index of diastolic dysfunction, was the best predictor of hospital mortality according to the area under the ROC curve (0.71) and was an independent predictor of outcome, as determined by multivariate analysis (OR = 1.36 [1.05 - 1.76], p = 0.02).
In septic patients admitted to an intensive care unit, echocardiographic systolic dysfunction is not associated with increased mortality. In contrast, diastolic dysfunction is an independent predictor of outcome.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):321-326
DOI 10.5935/0103-507X.20140046
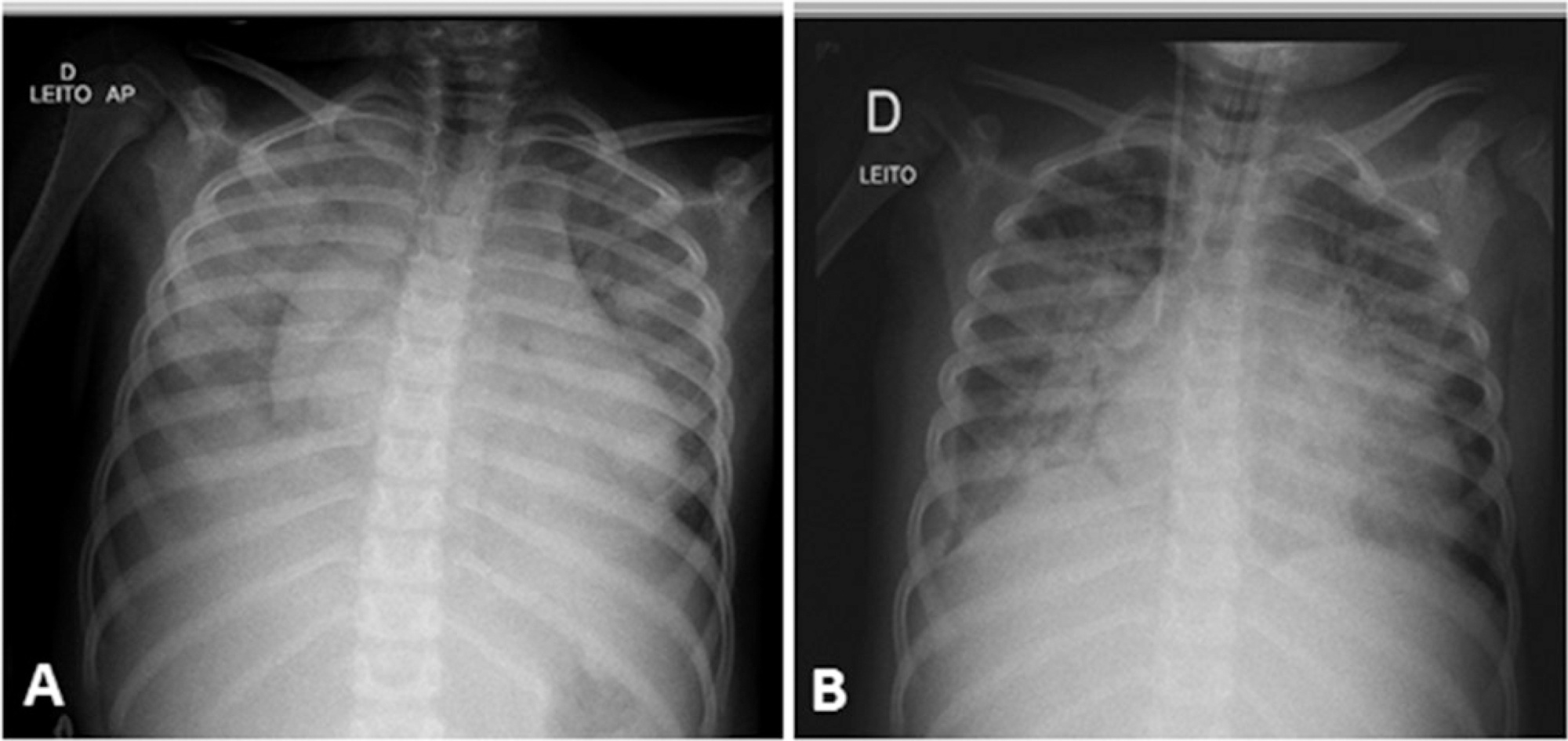
A case of fulminant myocarditis associated with the H1N1 influenza virus. This case report describes the patient's clinical course and emphasizes the importance of bedside echocardiography as an aid in the early diagnosis and management of children with severe myocardial dysfunction. It also discusses aspects relevant to the treatment and prognosis of fulminant myocarditis. The patient was a female, 4 years and 8 months old, previously healthy and with a history of flu symptoms in the past two weeks. The patient was admitted to the emergency room with signs of hemodynamic instability, requiring ventilatory support and vasoactive drugs. The laboratory tests, chest X-ray and echocardiogram suggested the presence of myocarditis. The test for H1N1 in nasopharyngeal secretions was positive. The patient evolved to refractory cardiogenic shock despite the clinical measures applied and died 48 hours after admission to the intensive care unit. The H1N1 influenza virus is an etiological agent associated with acute myocarditis, but there are few reported cases of fulminant myocarditis caused by the H1N1 virus. The identification of signs and symptoms suggestive of fulminant progression should be immediate, and bedside echocardiography is a useful tool for the early detection of myocardial dysfunction and for therapeutic guidance. The use of immunosuppressive therapy and antiviral therapy in acute myocarditis of viral etiology is controversial; hence, the treatment is based on hemodynamic and ventilatory support. The use of hemodynamic support by extracorporeal membrane oxygenation emerges as a promising treatment.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):321-326
DOI 10.5935/0103-507X.20140046
A case of fulminant myocarditis associated with the H1N1 influenza virus. This case report describes the patient's clinical course and emphasizes the importance of bedside echocardiography as an aid in the early diagnosis and management of children with severe myocardial dysfunction. It also discusses aspects relevant to the treatment and prognosis of fulminant myocarditis. The patient was a female, 4 years and 8 months old, previously healthy and with a history of flu symptoms in the past two weeks. The patient was admitted to the emergency room with signs of hemodynamic instability, requiring ventilatory support and vasoactive drugs. The laboratory tests, chest X-ray and echocardiogram suggested the presence of myocarditis. The test for H1N1 in nasopharyngeal secretions was positive. The patient evolved to refractory cardiogenic shock despite the clinical measures applied and died 48 hours after admission to the intensive care unit. The H1N1 influenza virus is an etiological agent associated with acute myocarditis, but there are few reported cases of fulminant myocarditis caused by the H1N1 virus. The identification of signs and symptoms suggestive of fulminant progression should be immediate, and bedside echocardiography is a useful tool for the early detection of myocardial dysfunction and for therapeutic guidance. The use of immunosuppressive therapy and antiviral therapy in acute myocarditis of viral etiology is controversial; hence, the treatment is based on hemodynamic and ventilatory support. The use of hemodynamic support by extracorporeal membrane oxygenation emerges as a promising treatment.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):360-366
DOI 10.5935/0103-507X.20140055
In Brazil, there are no data on the preferences of intensivists regarding hemodynamic monitoring methods. The present study aimed to identify the methods used by national intensivists, the hemodynamic variables they consider important, the regional differences, the reasons for choosing a particular method, and the use of protocols and continued training.
National intensivists were invited to answer an electronic questionnaire during three intensive care events and later, through the Associação de Medicina Intensiva Brasileira portal, between March and October 2009. Demographic data and aspects related to the respondent preferences regarding hemodynamic monitoring were researched.
In total, 211 professionals answered the questionnaire. Private hospitals showed higher availability of resources for hemodynamic monitoring than did public institutions. The pulmonary artery catheter was considered the most trusted by 56.9% of the respondents, followed by echocardiograms, at 22.3%. Cardiac output was considered the most important variable. Other variables also considered relevant were mixed/central venous oxygen saturation, pulmonary artery occlusion pressure, and right ventricular end-diastolic volume. Echocardiography was the most used method (64.5%), followed by pulmonary artery catheter (49.3%). Only half of respondents used treatment protocols, and 25% worked in continuing education programs in hemodynamic monitoring.
Hemodynamic monitoring has a greater availability in intensive care units of private institutions in Brazil. Echocardiography was the most used monitoring method, but the pulmonary artery catheter remains the most reliable. The implementation of treatment protocols and continuing education programs in hemodynamic monitoring in Brazil is still insufficient.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):360-366
DOI 10.5935/0103-507X.20140055
In Brazil, there are no data on the preferences of intensivists regarding hemodynamic monitoring methods. The present study aimed to identify the methods used by national intensivists, the hemodynamic variables they consider important, the regional differences, the reasons for choosing a particular method, and the use of protocols and continued training.
National intensivists were invited to answer an electronic questionnaire during three intensive care events and later, through the Associação de Medicina Intensiva Brasileira portal, between March and October 2009. Demographic data and aspects related to the respondent preferences regarding hemodynamic monitoring were researched.
In total, 211 professionals answered the questionnaire. Private hospitals showed higher availability of resources for hemodynamic monitoring than did public institutions. The pulmonary artery catheter was considered the most trusted by 56.9% of the respondents, followed by echocardiograms, at 22.3%. Cardiac output was considered the most important variable. Other variables also considered relevant were mixed/central venous oxygen saturation, pulmonary artery occlusion pressure, and right ventricular end-diastolic volume. Echocardiography was the most used method (64.5%), followed by pulmonary artery catheter (49.3%). Only half of respondents used treatment protocols, and 25% worked in continuing education programs in hemodynamic monitoring.
Hemodynamic monitoring has a greater availability in intensive care units of private institutions in Brazil. Echocardiography was the most used monitoring method, but the pulmonary artery catheter remains the most reliable. The implementation of treatment protocols and continuing education programs in hemodynamic monitoring in Brazil is still insufficient.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):345-347
DOI 10.5935/0103-507X.20130057
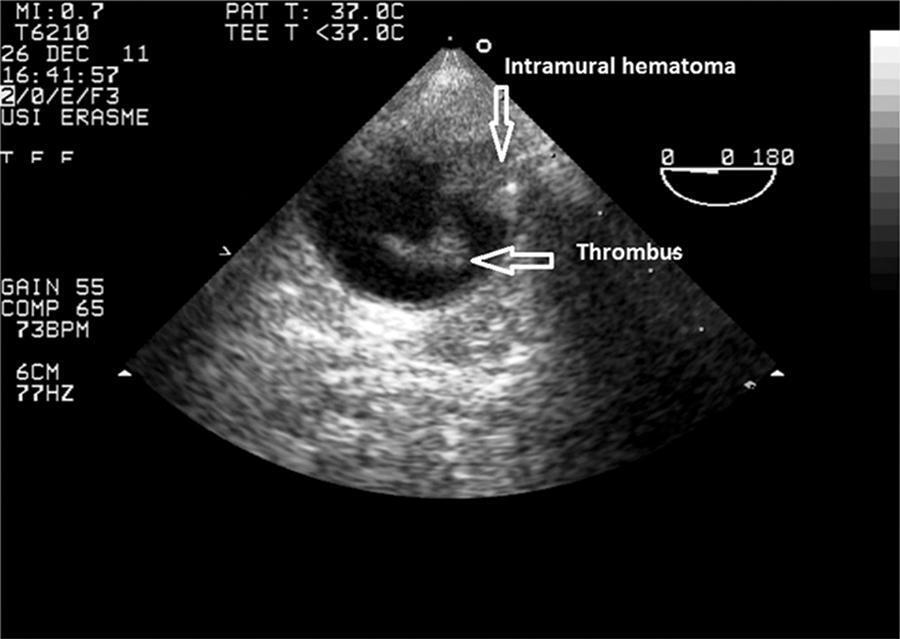
We describe the case of a patient with an intramural hematoma and floating thrombus after cardiopulmonary resuscitation. The 92-year old man had a cardiac arrest due to ventricular fibrillation and witnesses immediately initiated manual cardiopulmonary resuscitation. Transesophageal echocardiography was performed immediately on hospital admission because the patient was in cardiogenic shock. In addition to an akinetic anterior wall, examination of the descending thoracic aorta demonstrated an intramural hematoma and a floating intra-aortic thrombus at a distance of 40cm from the dental arch. There was no aortic dissection. The thrombus was attributed to aortic compression during cardiopulmonary resuscitation. Although the aortic thrombus and intramural hematoma were not associated with any complications in this patient, insertion of an intra-aortic balloon may have led to aortic rupture or embolic events. Transesophageal echocardiography should be performed, when available, prior to insertion of an intra-aortic balloon for counterpulsation in patients who have undergone cardiopulmonary resuscitation.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):345-347
DOI 10.5935/0103-507X.20130057
We describe the case of a patient with an intramural hematoma and floating thrombus after cardiopulmonary resuscitation. The 92-year old man had a cardiac arrest due to ventricular fibrillation and witnesses immediately initiated manual cardiopulmonary resuscitation. Transesophageal echocardiography was performed immediately on hospital admission because the patient was in cardiogenic shock. In addition to an akinetic anterior wall, examination of the descending thoracic aorta demonstrated an intramural hematoma and a floating intra-aortic thrombus at a distance of 40cm from the dental arch. There was no aortic dissection. The thrombus was attributed to aortic compression during cardiopulmonary resuscitation. Although the aortic thrombus and intramural hematoma were not associated with any complications in this patient, insertion of an intra-aortic balloon may have led to aortic rupture or embolic events. Transesophageal echocardiography should be performed, when available, prior to insertion of an intra-aortic balloon for counterpulsation in patients who have undergone cardiopulmonary resuscitation.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
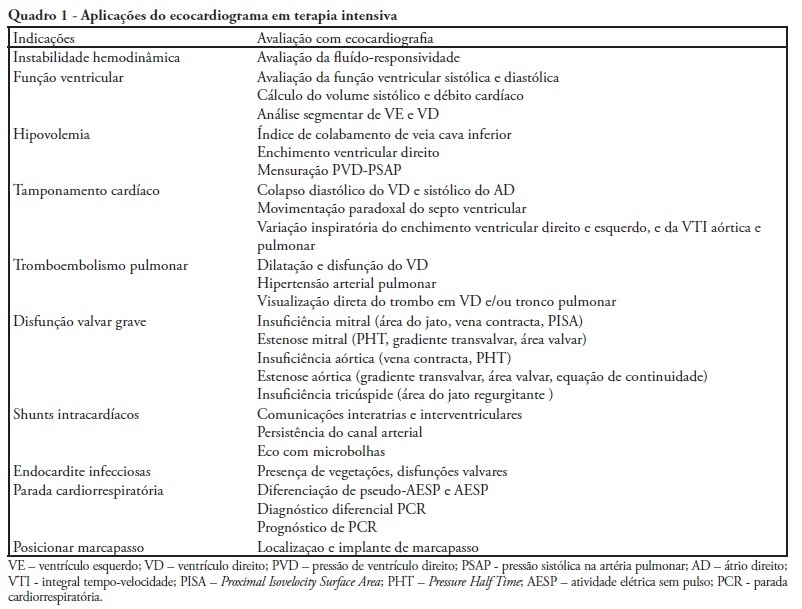
During the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
During the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
Use of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients' safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):190-196
DOI 10.1590/S0103-507X2009000200012
Use of ultrasound introduced as part of intensive care therapy makes viable bedside invasive procedures and diagnosis. Due to portability, combined with team training, its use guarantees less complications related to insertion, as well as patients' safety. It also reduces severe conditions related to the catheter, such as pneumothorax among others. Probably, in a near future, as purchase of ultrasound equipment becomes easier and team training more adequate, this tool will become essential in daily clinical practice.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
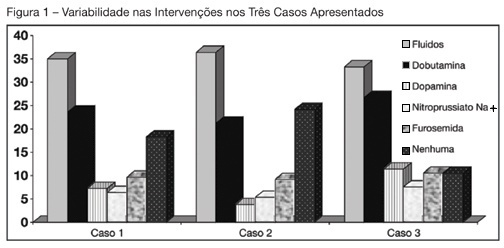
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
Abstract
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
BACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.