Critical illness Archives - Critical Care Science (CCS)

Abstract
Critical Care Science. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-en
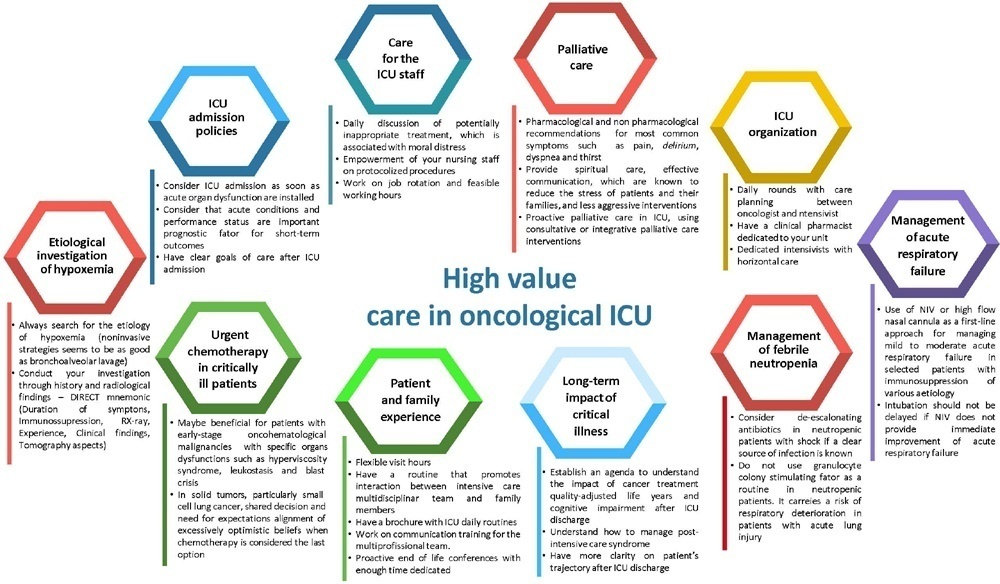
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Critical Care Science. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-en
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
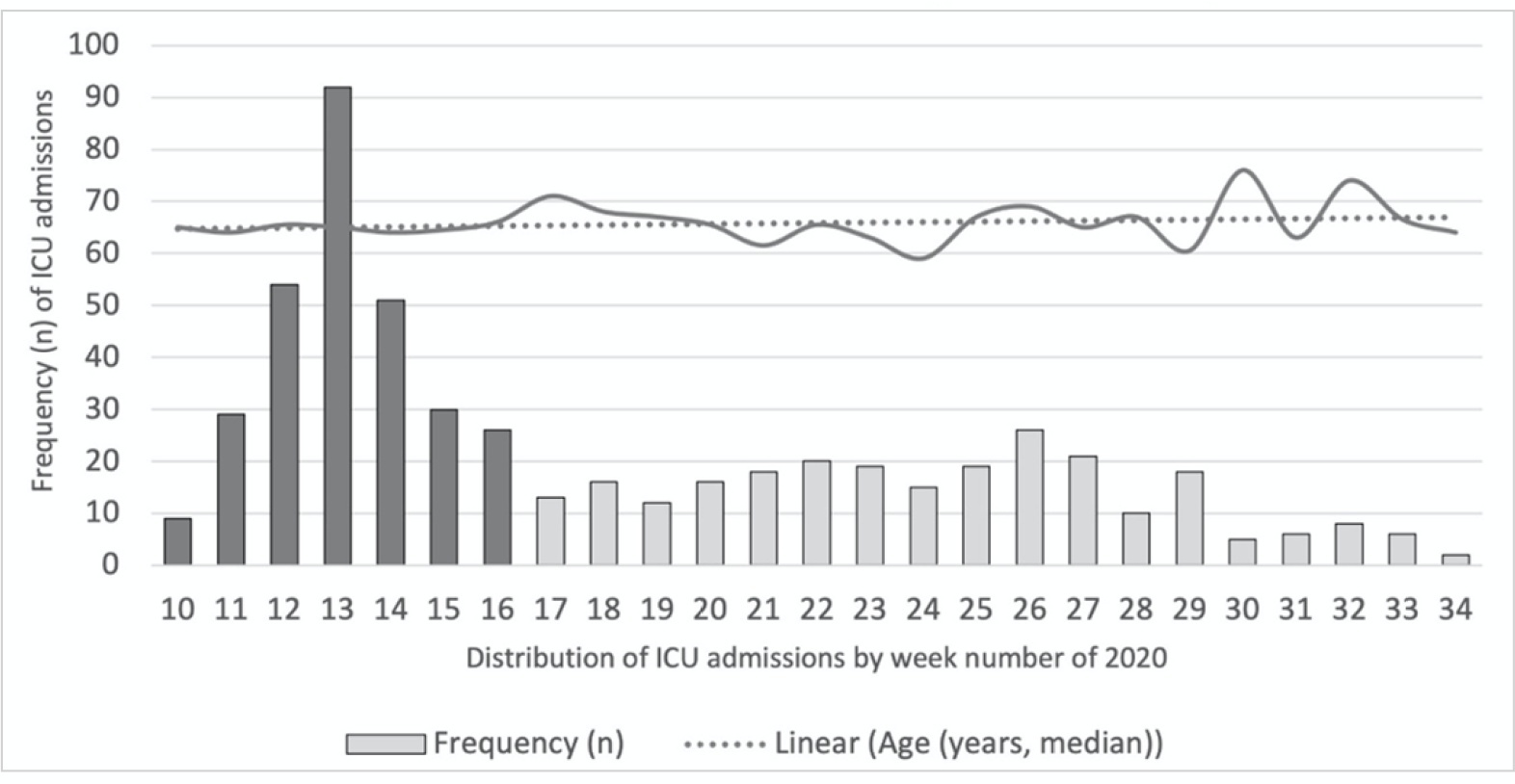
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 - 16 and 17 - 34, were defined.
Five hundred forty-one adult patients with a median age of 65 [57 - 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 - 3] versus 2 [0 - 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(4):433-442
DOI 10.5935/0103-507X.20210037-en
To analyze and compare COVID-19 patient characteristics, clinical management and outcomes between the peak and plateau periods of the first pandemic wave in Portugal.
This was a multicentric ambispective cohort study including consecutive severe COVID-19 patients between March and August 2020 from 16 Portuguese intensive care units. The peak and plateau periods, respectively, weeks 10 - 16 and 17 - 34, were defined.
Five hundred forty-one adult patients with a median age of 65 [57 - 74] years, mostly male (71.2%), were included. There were no significant differences in median age (p = 0.3), Simplified Acute Physiology Score II (40 versus 39; p = 0.8), partial arterial oxygen pressure/fraction of inspired oxygen ratio (139 versus 136; p = 0.6), antibiotic therapy (57% versus 64%; p = 0.2) at admission, or 28-day mortality (24.4% versus 22.8%; p = 0.7) between the peak and plateau periods. During the peak period, patients had fewer comorbidities (1 [0 - 3] versus 2 [0 - 5]; p = 0.002) and presented a higher use of vasopressors (47% versus 36%; p < 0.001) and invasive mechanical ventilation (58.1 versus 49.2%; p < 0.001) at admission, prone positioning (45% versus 36%; p = 0.04), and hydroxychloroquine (59% versus 10%; p < 0.001) and lopinavir/ritonavir (41% versus 10%; p < 0.001) prescriptions. However, a greater use of high-flow nasal cannulas (5% versus 16%, p < 0.001) on admission, remdesivir (0.3% versus 15%; p < 0.001) and corticosteroid (29% versus 52%, p < 0.001) therapy, and a shorter ICU length of stay (12 days versus 8, p < 0.001) were observed during the plateau.
There were significant changes in patient comorbidities, intensive care unit therapies and length of stay between the peak and plateau periods of the first COVID-19 wave.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
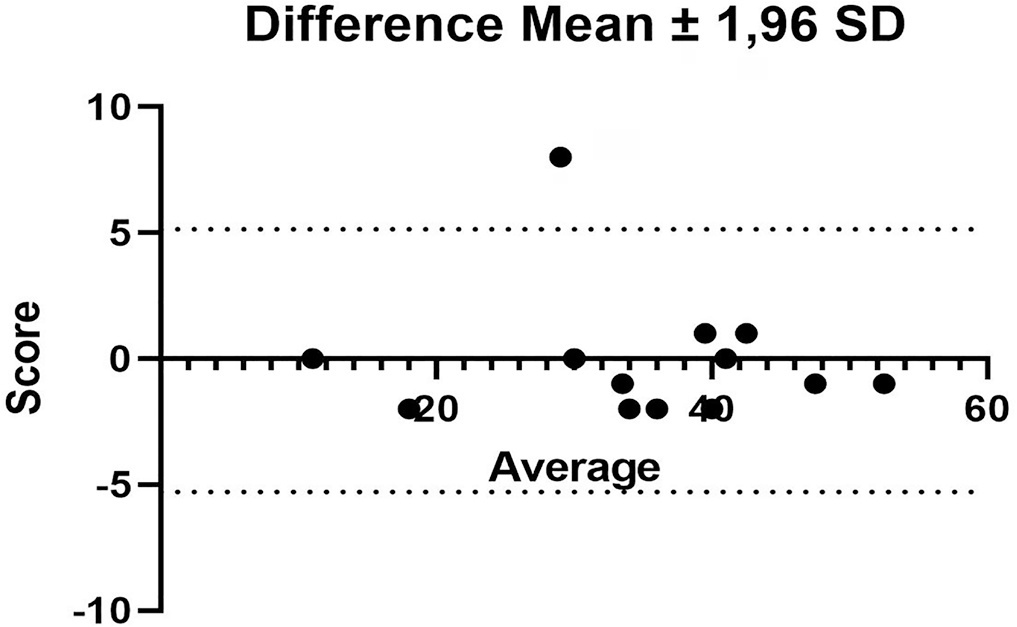
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):272-278
DOI 10.5935/0103-507X.20220025-en
To translate, crossculturally adapt and evaluate the clinimetric properties of the Critical Care Functional Rehabilitation Outcome Measure for evaluating the functionality of patients admitted to intensive care units in Brazil.
The process of translation and cross-cultural adaptation involved the following steps: initial translation, synthesis, back-translation, expert committee review and pretesting. The intra- and interrater reliability and agreement were analyzed between two physical therapists who evaluated the same group of patients (n = 35). The evaluations were performed by each therapist independently and blinded to the score assigned by the other professional. The qualitative analysis was performed by the review committee, and the experts adapted and synthesized the Portuguese translation of the Critical Care Functional Rehabilitation Outcome Measure.
There was agreement between the initial Brazilian translations of the Critical Care Functional Rehabilitation Outcome Measure scale. The conceptual, idiomatic, semantic and experimental equivalences between the original and translated versions were assessed, resulting in the final Brazilian version of the scale, called the Medida de Resultado da Reabilitação Funcional em Cuidados Intensivos. The evaluation of the clinimetric properties showed evidence of a high degree of agreement and reliability, as all had an intraclass correlation coefficient above 0.75. The overall intraclass correlation coefficient was 0.89.
The translated version of the Critical Care Functional Rehabilitation Outcome Measure scale for assessing the functionality of patients admitted to an intensive care unit can be used reliably in Brazil following translation and cross-cultural adaptation to Brazilian Portuguese and presents evidence of excellent interrater reliability.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
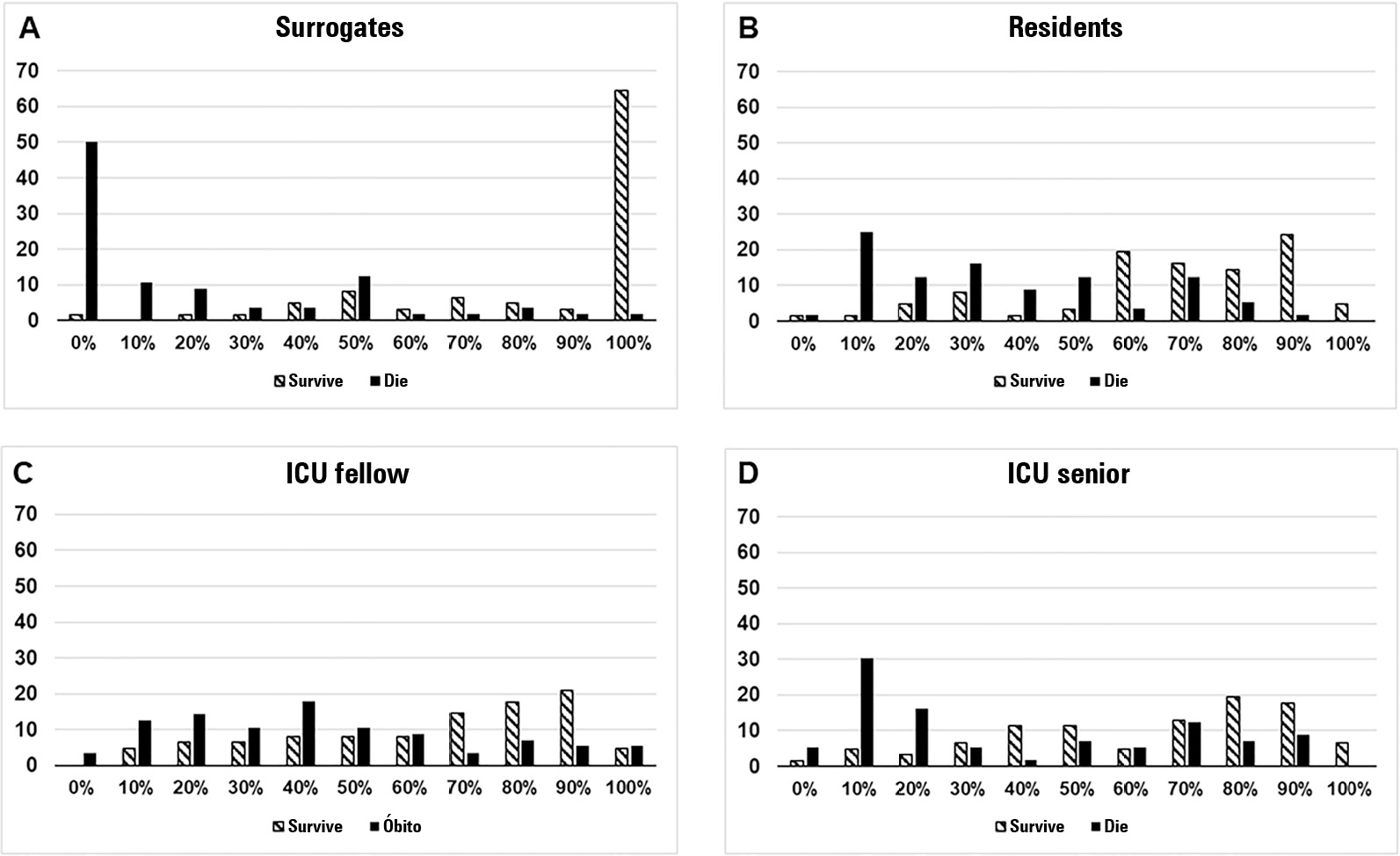
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(2):220-226
DOI 10.5935/0103-507X.20220019-en
To compare the predictive performance of residents, senior intensive care unit physicians and surrogates early during intensive care unit stays and to evaluate whether different presentations of prognostic data (probability of survival versus probability of death) influenced their performance.
We questioned surrogates and physicians in charge of critically ill patients during the first 48 hours of intensive care unit admission on the patient’s probability of hospital outcome. The question framing (i.e., probability of survival versus probability of death during hospitalization) was randomized. To evaluate the predictive performance, we compared the areas under the ROC curves (AUCs) for hospital outcome between surrogates and physicians’ categories. We also stratified the results according to randomized question framing.
We interviewed surrogates and physicians on the hospital outcomes of 118 patients. The predictive performance of surrogate decisionmakers was significantly lower than that of physicians (AUC of 0.63 for surrogates, 0.82 for residents, 0.80 for intensive care unit fellows and 0.81 for intensive care unit senior physicians). There was no increase in predictive performance related to physicians’ experience (i.e., senior physicians did not predict outcomes better than junior physicians). Surrogate decisionmakers worsened their prediction performance when they were asked about probability of death instead of probability of survival, but there was no difference for physicians.
Different predictive performance was observed when comparing surrogate decision-makers and physicians, with no effect of experience on health care professionals’ prediction. Question framing affected the predictive performance of surrogates but not of physicians.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
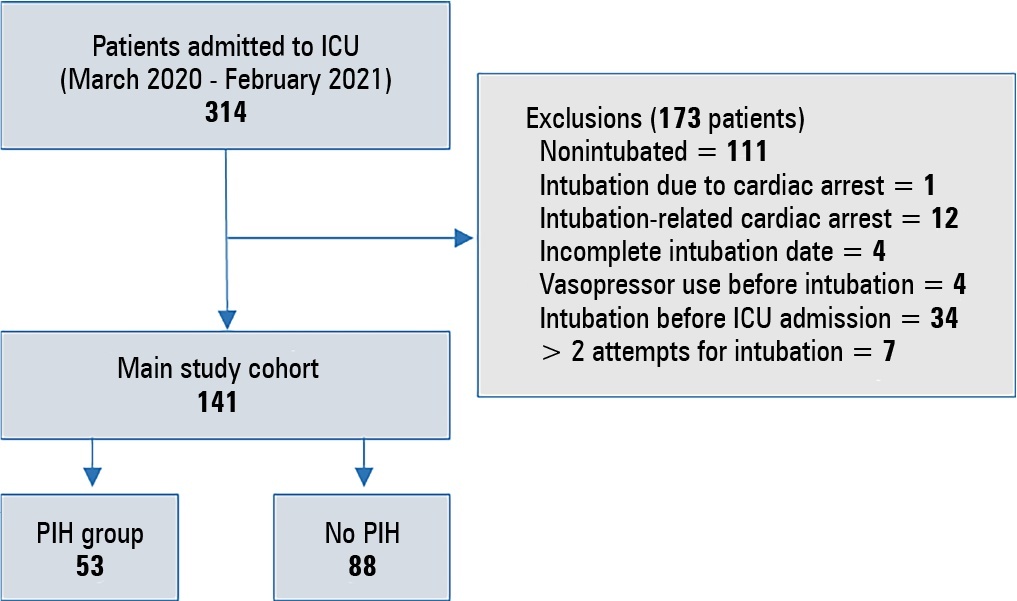
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 - 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 - 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):131-140
DOI 10.5935/0103-507X.20220007-en
To evaluate the incidence of risk factors for postintubation hypotension in critically ill patients with COVID-19.
We conducted a retrospective study of 141 patients with COVID-19 who were intubated in the intensive care unit. Postintubation hypotension was defined as the need for any vasopressor dose at any time within the 60 minutes following intubation. Patients with intubation-related cardiac arrest and hypotension before intubation were excluded from the study.
Of the 141 included patients, 53 patients (37.5%) had postintubation hypotension, and 43.6% of the patients (n = 17) were female. The median age of the postintubation hypotension group was 75.0 (interquartile range: 67.0 - 84.0). In the multivariate analysis, shock index ≥ 0.90 (OR = 7.76; 95%CI 3.14 - 19.21; p < 0.001), albumin levels < 2.92g/dL (OR = 3.65; 95%CI 1.49 - 8.96; p = 0.005), and procalcitonin levels (OR = 1.07, 95%CI 1.01 - 1.15; p = 0.045) were independent risk factors for postintubation hypotension. Hospital mortality was similar in patients with postintubation hypotension and patients without postintubation hypotension (92.5% versus 85.2%; p = 0.29).
The incidence of postintubation hypotension was 37.5% in critically ill COVID-19 patients. A shock index ≥ 0.90 and albumin levels < 2.92g/dL were independently associated with postintubation hypotension. Furthermore, a shock index ≥ 0.90 may be a practical tool to predict the increased risk of postintubation hypotension in bedside scenarios before endotracheal intubation. In this study, postintubation hypotension was not associated with increased hospital mortality in COVID-19 patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):583-591
DOI 10.5935/0103-507X.20210085
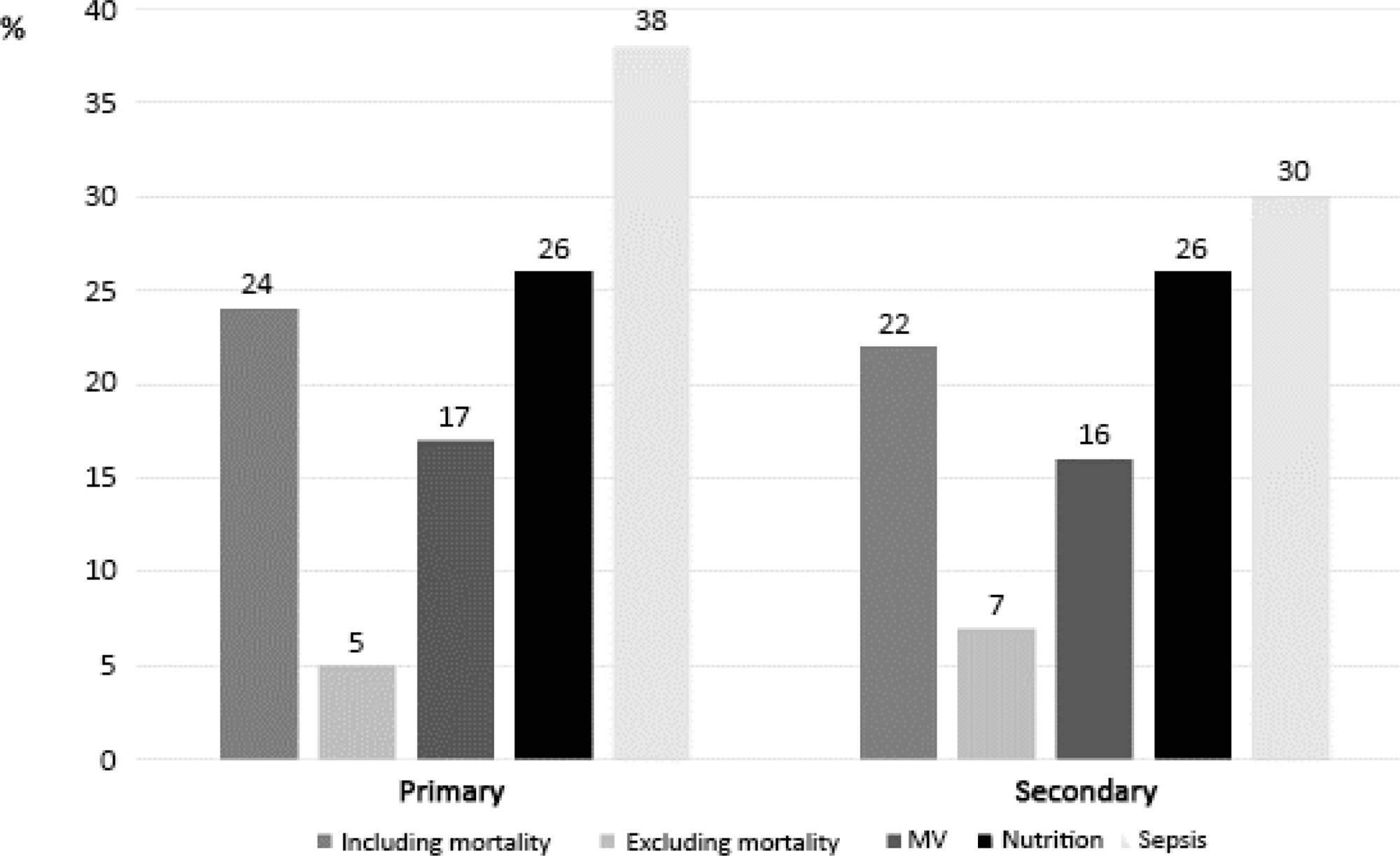
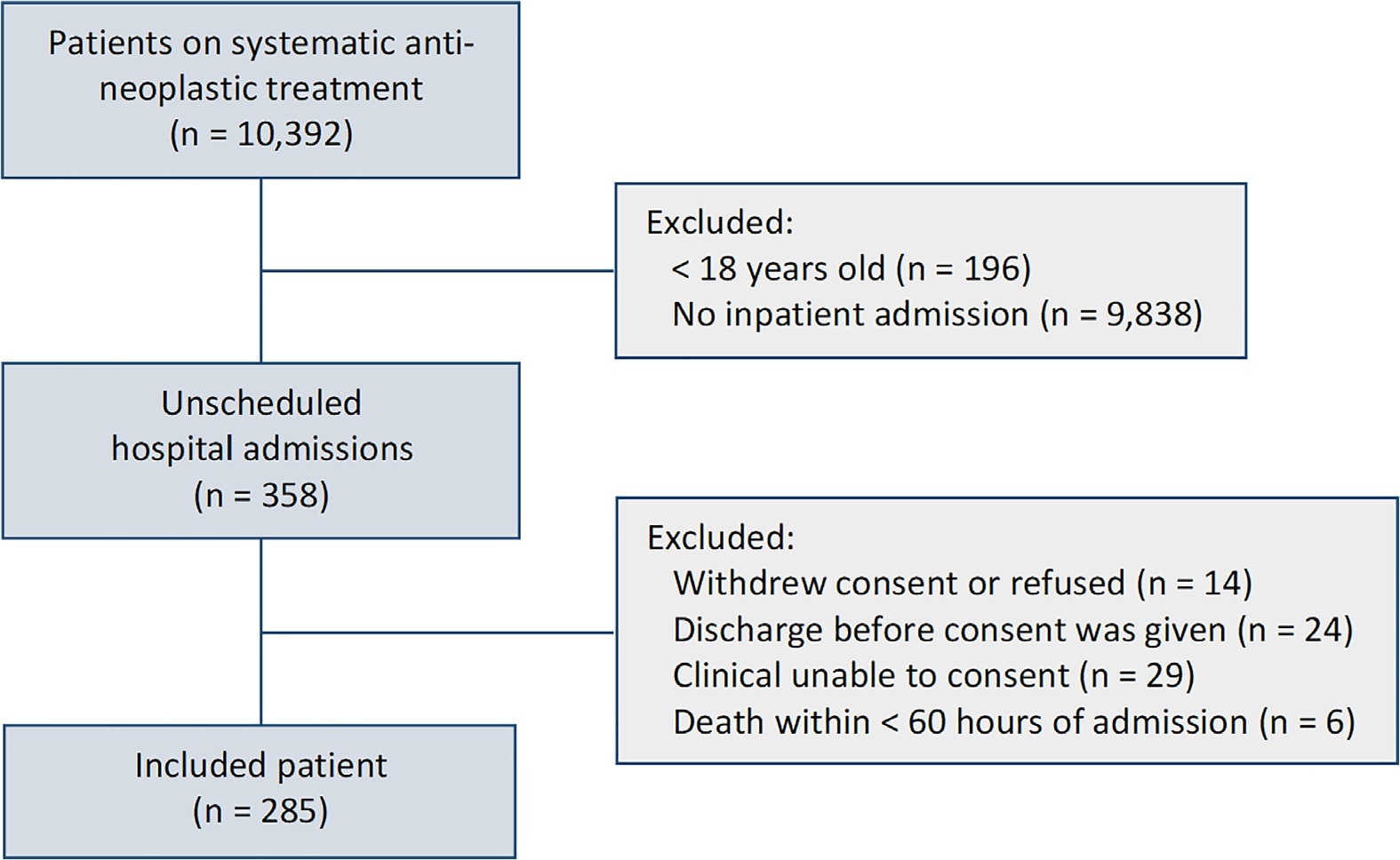
To ascertain the cumulative incidence of acute organ failure and intensive care unit admission in cancer patients.
This was a single-center prospective cohort study of adult cancer patients admitted for unscheduled inpatient care while on systemic cancer treatment.
Between August 2018 and February 2019, 10,392 patients were on systemic treatment, 358 had unscheduled inpatient care and were eligible for inclusion, and 285 were included. The mean age was 60.9 years, 50.9% were male, and 17.9% of patients had hematologic cancers. The cumulative risk of acute organ failure was 39.6% (95%CI: 35 - 44), and that of intensive care unit admission among patients with acute organ failure was 15.0% (95%CI: 12 - 18). On admission, 62.1% of patients were considered not eligible for artificial organ replacement therapy. The median follow-up time was 9.5 months. Inpatient mortality was 17.5%, with an intensive care unit mortality rate of 58.8% and a median cohort survival of 134 days (95%CI: 106 - 162). In multivariate analysis, acute organ failure was associated with 6-month postdischarge mortality (HR 1.6; 95%CI: 1.2 - 2.2).
The risk of acute organ failure in cancer patients admitted for unscheduled inpatient care while on systemic treatment was 39.6%, and the risk of intensive care unit admission was 15.0%. Acute organ failure in cancer patients was an independent poor prognostic factor for inpatient hospital mortality and 6-month survival.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):583-591
DOI 10.5935/0103-507X.20210085
To ascertain the cumulative incidence of acute organ failure and intensive care unit admission in cancer patients.
This was a single-center prospective cohort study of adult cancer patients admitted for unscheduled inpatient care while on systemic cancer treatment.
Between August 2018 and February 2019, 10,392 patients were on systemic treatment, 358 had unscheduled inpatient care and were eligible for inclusion, and 285 were included. The mean age was 60.9 years, 50.9% were male, and 17.9% of patients had hematologic cancers. The cumulative risk of acute organ failure was 39.6% (95%CI: 35 - 44), and that of intensive care unit admission among patients with acute organ failure was 15.0% (95%CI: 12 - 18). On admission, 62.1% of patients were considered not eligible for artificial organ replacement therapy. The median follow-up time was 9.5 months. Inpatient mortality was 17.5%, with an intensive care unit mortality rate of 58.8% and a median cohort survival of 134 days (95%CI: 106 - 162). In multivariate analysis, acute organ failure was associated with 6-month postdischarge mortality (HR 1.6; 95%CI: 1.2 - 2.2).
The risk of acute organ failure in cancer patients admitted for unscheduled inpatient care while on systemic treatment was 39.6%, and the risk of intensive care unit admission was 15.0%. Acute organ failure in cancer patients was an independent poor prognostic factor for inpatient hospital mortality and 6-month survival.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(3):428-433
DOI 10.5935/0103-507X.20210068
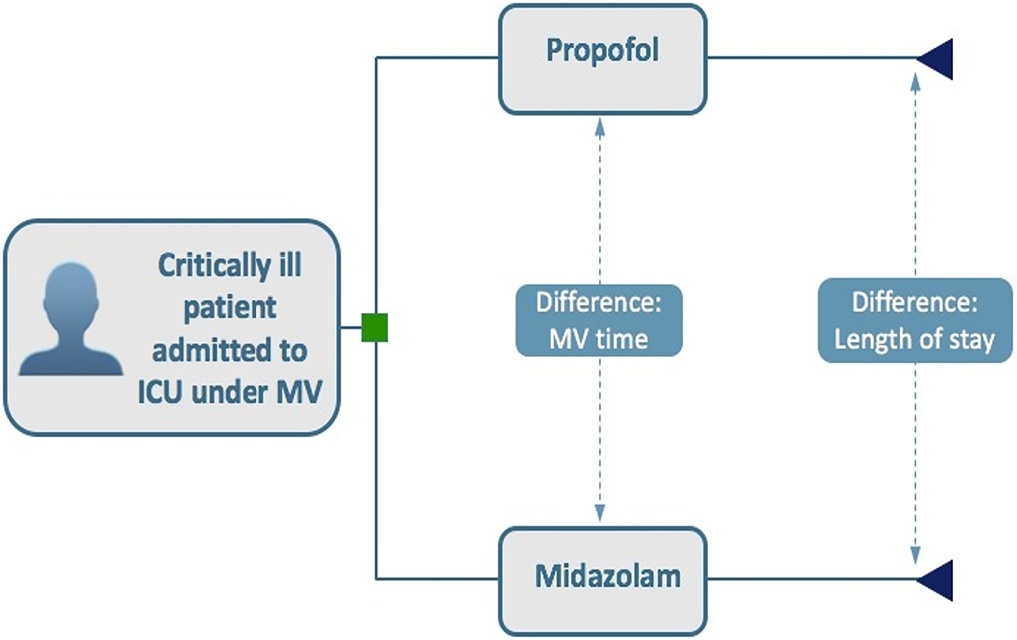
To build a cost-effectiveness model to compare the use of propofol versus midazolam in critically ill adult patients under mechanical ventilation.
We built a decision tree model for critically ill patients submitted to mechanical ventilation and analyzed it from the Brazilian private health care system perspective. The time horizon was that of intensive care unit hospitalization. The outcomes were cost-effectiveness per hour of intensive care unit stay avoided and cost-effectiveness per hour of mechanical ventilation avoided. We retrieved data for the model from a previous meta-analysis. We assumed that the cost of medication was embedded in the intensive care unit cost. We conducted univariate and probabilistic sensitivity analyses.
Mechanically ventilated patients using propofol had their intensive care unit stay and the duration of mechanical ventilation decreased by 47.97 hours and 21.65 hours, respectively. There was an average cost reduction of US$ 2,998.971 for propofol when compared to midazolam. The cost-effectiveness per hour of intensive care unit stay and mechanical ventilation avoided were dominant 94.40% and 80.8% of the time, respectively.
There was a significant reduction in costs associated with propofol use related to intensive care unit stay and duration of mechanical ventilation for critically ill adult patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(3):428-433
DOI 10.5935/0103-507X.20210068
To build a cost-effectiveness model to compare the use of propofol versus midazolam in critically ill adult patients under mechanical ventilation.
We built a decision tree model for critically ill patients submitted to mechanical ventilation and analyzed it from the Brazilian private health care system perspective. The time horizon was that of intensive care unit hospitalization. The outcomes were cost-effectiveness per hour of intensive care unit stay avoided and cost-effectiveness per hour of mechanical ventilation avoided. We retrieved data for the model from a previous meta-analysis. We assumed that the cost of medication was embedded in the intensive care unit cost. We conducted univariate and probabilistic sensitivity analyses.
Mechanically ventilated patients using propofol had their intensive care unit stay and the duration of mechanical ventilation decreased by 47.97 hours and 21.65 hours, respectively. There was an average cost reduction of US$ 2,998.971 for propofol when compared to midazolam. The cost-effectiveness per hour of intensive care unit stay and mechanical ventilation avoided were dominant 94.40% and 80.8% of the time, respectively.
There was a significant reduction in costs associated with propofol use related to intensive care unit stay and duration of mechanical ventilation for critically ill adult patients.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.