Critical care Archives - Page 2 of 12 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
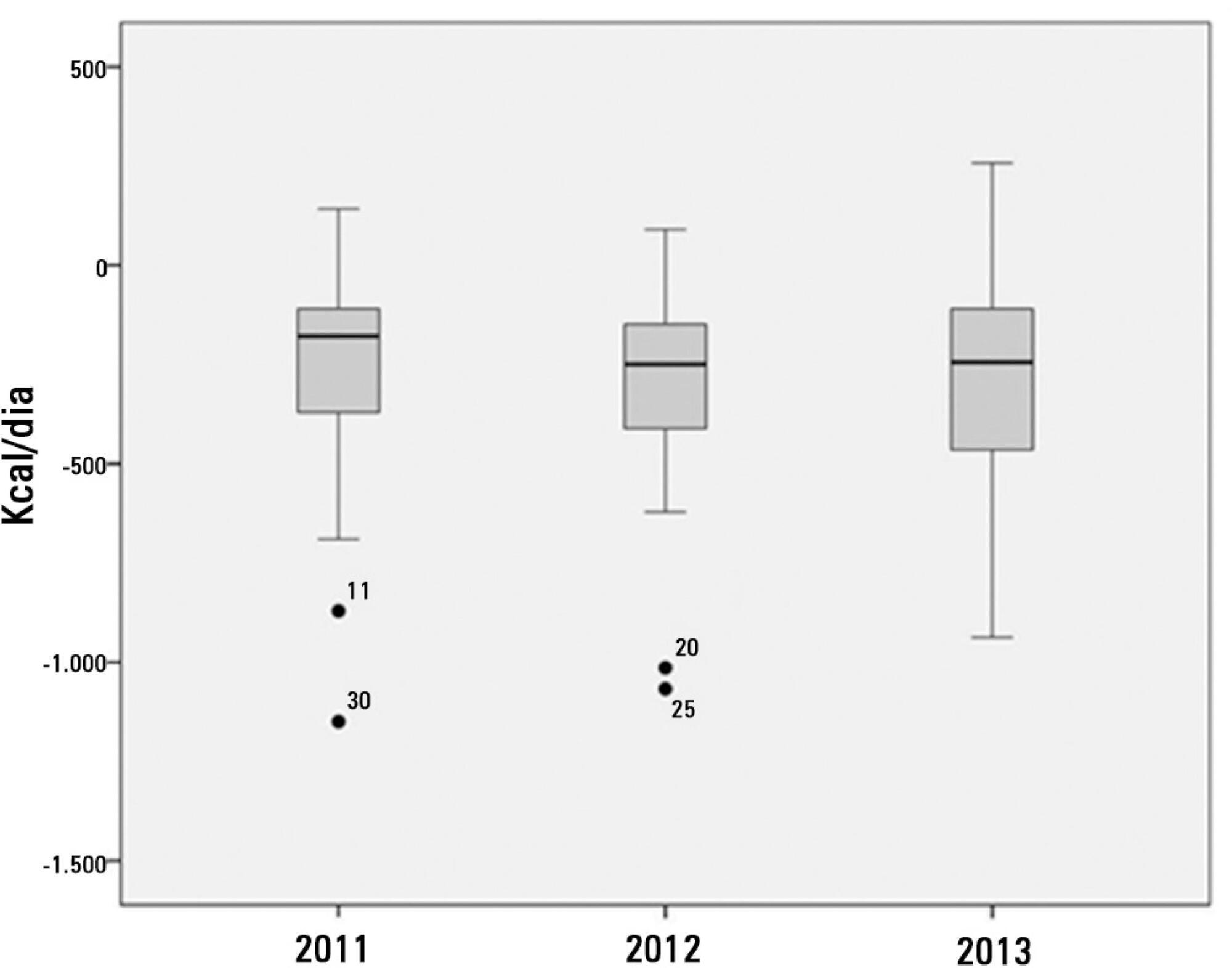
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):155-162
DOI 10.5935/0103-507X.20140023
To determine the factors that influence the adequacy of enteral nutritional therapy in an intensive care unit.
This prospective observational study was conducted in an intensive care unit between 2010 and 2012. Patients >18 years of age underwent exclusive enteral nutritional therapy for ≥72 hours. The energy and protein requirements were calculated according to the ICU protocols. The data regarding enteral nutrition, the causes of non-compliance, and the biochemical test results were collected daily.
Ninety-three patients admitted to the intensive care unit were evaluated. Among these patients, 82% underwent early enteral nutritional therapy, and 80% reached the nutritional goal in <36 hours. In addition, 81.6%±15.4% of the enteral nutrition volume was infused, with an adequacy of 82.2%±16.0% for calories, 82.2%±15.9% for proteins, and a mean energy balance of -289.9±277.1kcal/day. A negative correlation of C-reactive protein with the volume infused and the energy and protein balance was observed. In contrast, a positive correlation was found between C-reactive protein and the time required to reach nutritional goals. Extubation was the main cause for interrupting the enteral nutritional therapy (29.9% of the interruption hours), and the patients >60 years of age exhibited a lower percentage of recovery of the oral route compared with the younger patients (p=0.014).
Early enteral nutritional therapy and the adequacy for both energy and protein of the nutritional volume infused were in accordance with the established guidelines. Possible inadequacies of energy and protein balance appeared to be associated with an acute inflammatory response, which was characterized by elevated C-reactive protein levels. The main cause of interruption of the enteral nutritional therapy was the time spent in extubation.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
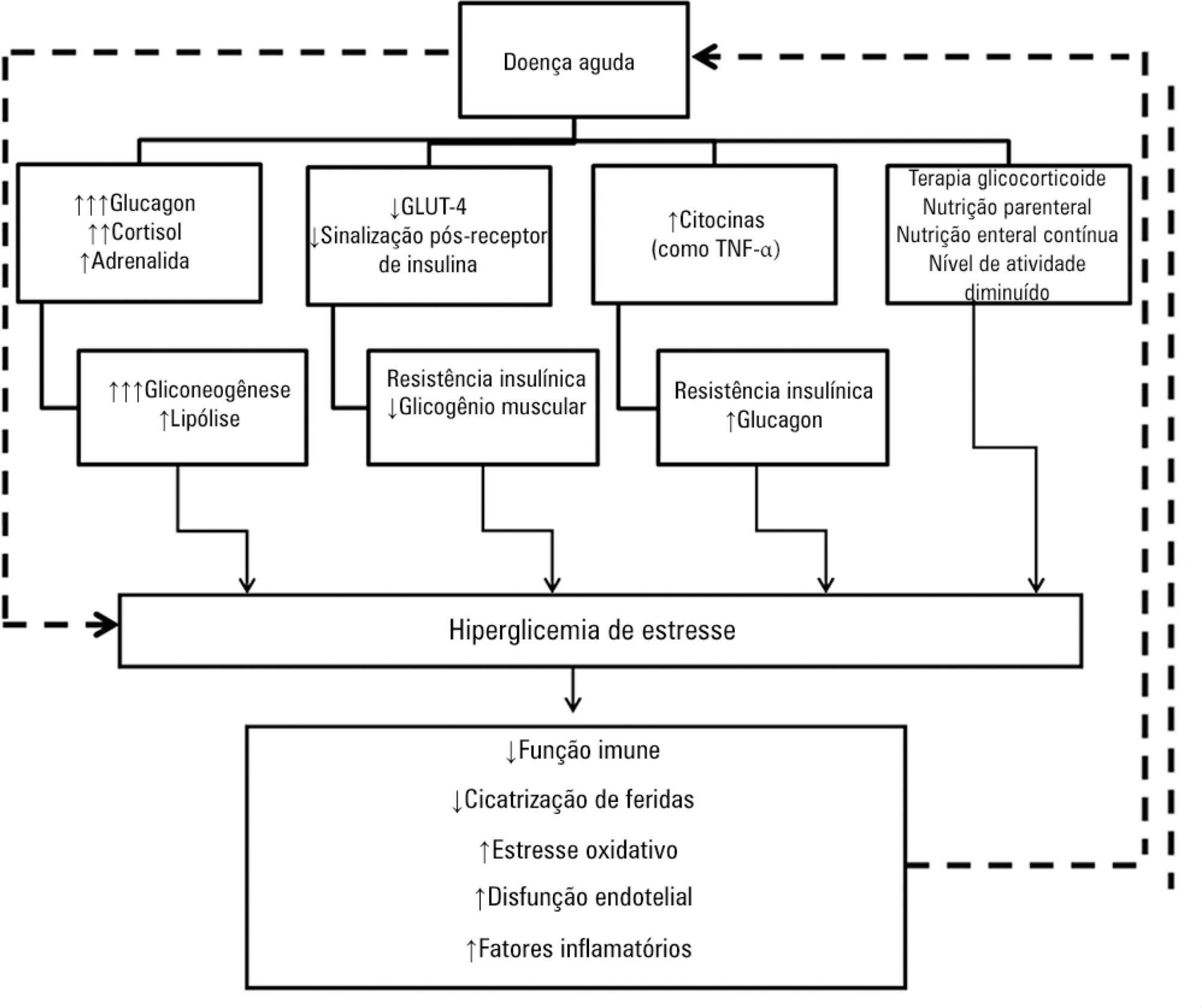
Hyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients' care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Abstract
Rev Bras Ter Intensiva. 2014;26(1):71-76
DOI 10.5935/0103-507X.20140011
Hyperglycemia is a commonly encountered issue in critically ill patients in the intensive care setting. The presence of hyperglycemia is associated with increased morbidity and mortality, regardless of the reason for admission (e.g., acute myocardial infarction, status post-cardiovascular surgery, stroke, sepsis). However, the pathophysiology and, in particular, the treatment of hyperglycemia in the critically ill patient remain controversial. In clinical practice, several aspects must be taken into account in the management of these patients, including blood glucose targets, history of diabetes mellitus, the route of nutrition (enteral or parenteral), and available monitoring equipment, which substantially increases the workload of providers involved in the patients' care. This review describes the epidemiology, pathophysiology, management, and monitoring of hyperglycemia in the critically ill adult patient.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):305-312
DOI 10.5935/0103-507X.20140043
The number of studies investigating circulating nucleic acids as potential biomarkers has increased in recent years. The detection of such biomarkers is a minimally invasive alternative for the diagnosis and prognosis of various clinical conditions. The value of circulating DNA levels as a predictive biomarker has been demonstrated in patients suffering from numerous acute pathologies that have a high risk of intensive care needs and in-hospital deaths. The mechanism by which circulating DNA levels increase in patients with these conditions remains unclear. In this review, we focused on the potential use of this biomarker for prognosis prediction in critically ill and trauma patients. The literature review was performed by searching MedLine using PubMed in the English language.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):305-312
DOI 10.5935/0103-507X.20140043
The number of studies investigating circulating nucleic acids as potential biomarkers has increased in recent years. The detection of such biomarkers is a minimally invasive alternative for the diagnosis and prognosis of various clinical conditions. The value of circulating DNA levels as a predictive biomarker has been demonstrated in patients suffering from numerous acute pathologies that have a high risk of intensive care needs and in-hospital deaths. The mechanism by which circulating DNA levels increase in patients with these conditions remains unclear. In this review, we focused on the potential use of this biomarker for prognosis prediction in critically ill and trauma patients. The literature review was performed by searching MedLine using PubMed in the English language.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
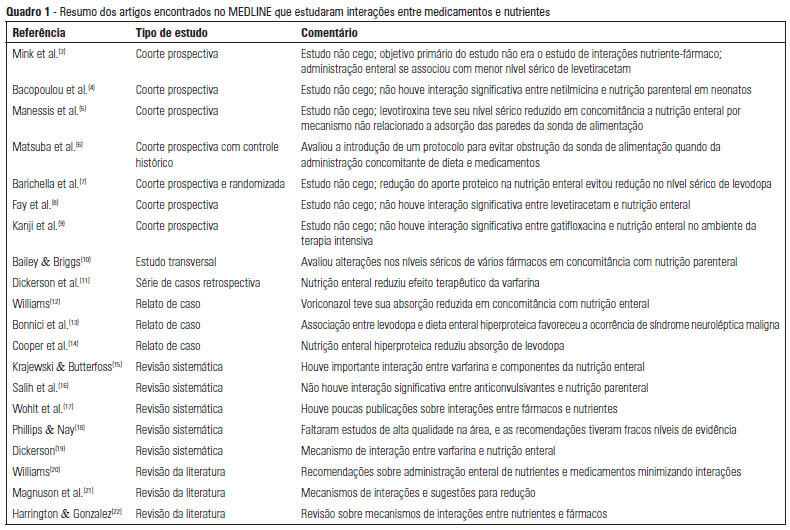
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):407-414
DOI 10.1590/S0103-507X2012000400019
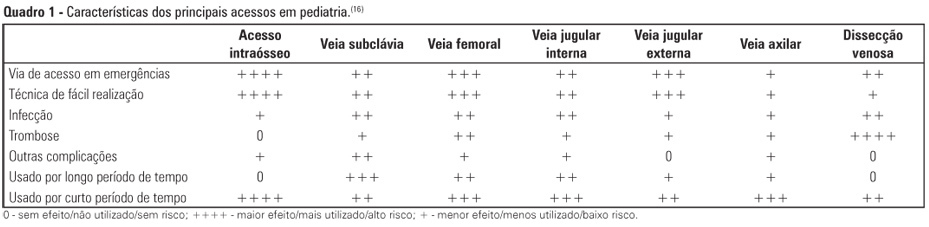
Obtaining venous access in critically ill children is an essential procedure to restore blood volume and administer drugs during pediatric emergencies. The first option for vascular access is through a peripheral vein puncture. If this route cannot be used or if a prolonged period of access is necessary, then the intraosseous route is an effective option for rapid and safe venous access. The present work is a descriptive and exploratory literature review. The study's aim was to describe the techniques, professional responsibilities, and care related to obtaining venous access via the intraosseous route in pediatric emergencies. We selected 22 articles (published between 2000 and 2011) that were available in the Latin American and Caribbean Health Sciences (LILACS) and MEDLINE databases and the SciELO electronic library, in addition to the current protocol of cardiopulmonary resuscitation from the American Heart Association (2010). After the literature search, data were pooled and grouped into the following categories of analysis: historical aspects and physiological principles; indications, benefits, and contraindications; professional assignments; technical principles; care during the access; and possible complications. The results of the present study revealed that the intraosseous route is considered the main secondary option for vascular access during the emergency response because the technique is quick and easily executed, presents several non-collapsible puncture sites, and enables the rapid and effective administration of drugs and fluid replacement.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):407-414
DOI 10.1590/S0103-507X2012000400019
Obtaining venous access in critically ill children is an essential procedure to restore blood volume and administer drugs during pediatric emergencies. The first option for vascular access is through a peripheral vein puncture. If this route cannot be used or if a prolonged period of access is necessary, then the intraosseous route is an effective option for rapid and safe venous access. The present work is a descriptive and exploratory literature review. The study's aim was to describe the techniques, professional responsibilities, and care related to obtaining venous access via the intraosseous route in pediatric emergencies. We selected 22 articles (published between 2000 and 2011) that were available in the Latin American and Caribbean Health Sciences (LILACS) and MEDLINE databases and the SciELO electronic library, in addition to the current protocol of cardiopulmonary resuscitation from the American Heart Association (2010). After the literature search, data were pooled and grouped into the following categories of analysis: historical aspects and physiological principles; indications, benefits, and contraindications; professional assignments; technical principles; care during the access; and possible complications. The results of the present study revealed that the intraosseous route is considered the main secondary option for vascular access during the emergency response because the technique is quick and easily executed, presents several non-collapsible puncture sites, and enables the rapid and effective administration of drugs and fluid replacement.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
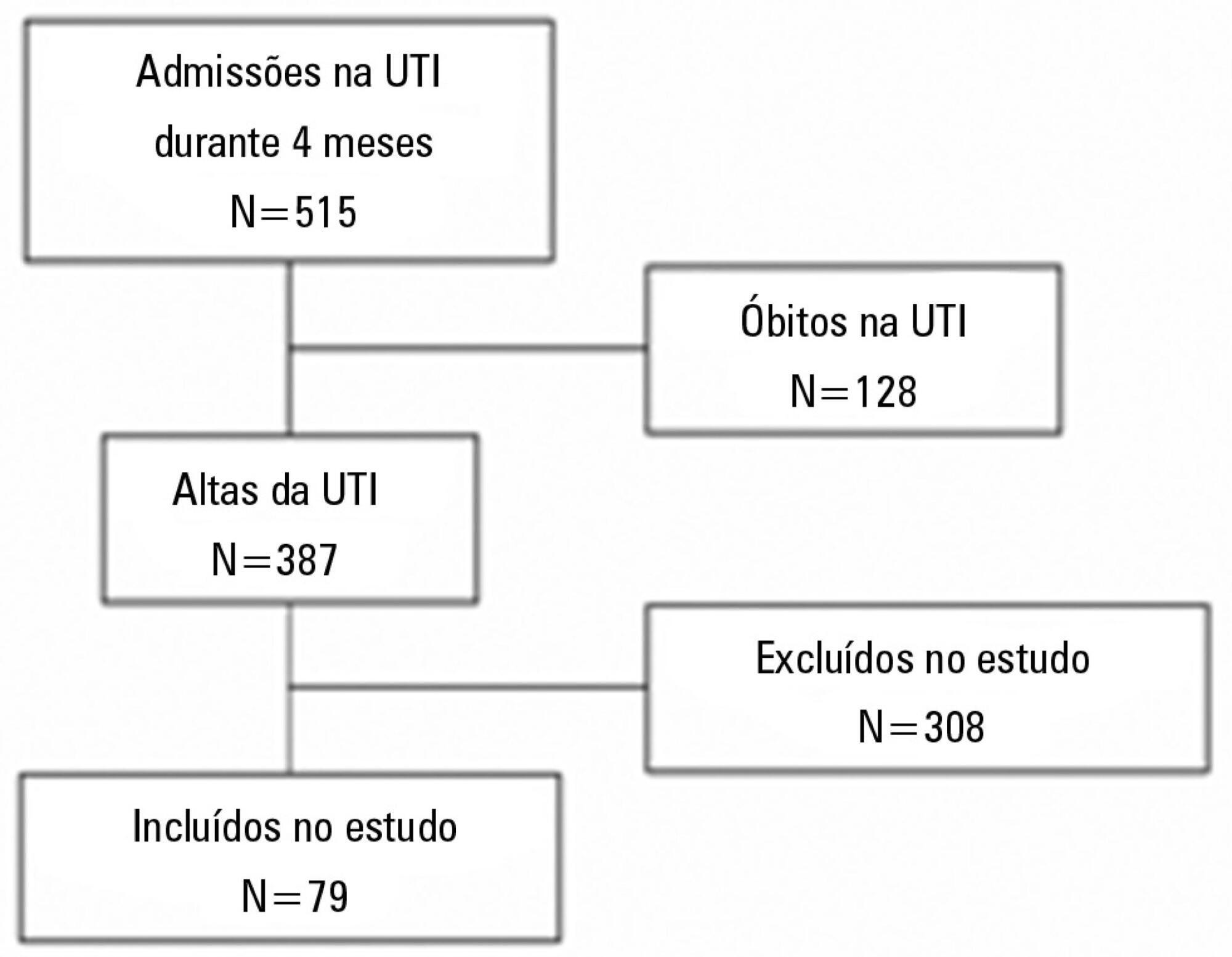
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
Abstract
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):327-333
DOI 10.5935/0103-507X.20130055
To analyze the outcomes of increased or decreased intracranial pressure and/or the decrease in cerebral perfusion pressure resulting from respiratory physiotherapy on critically ill patients admitted to the intensive care unit.
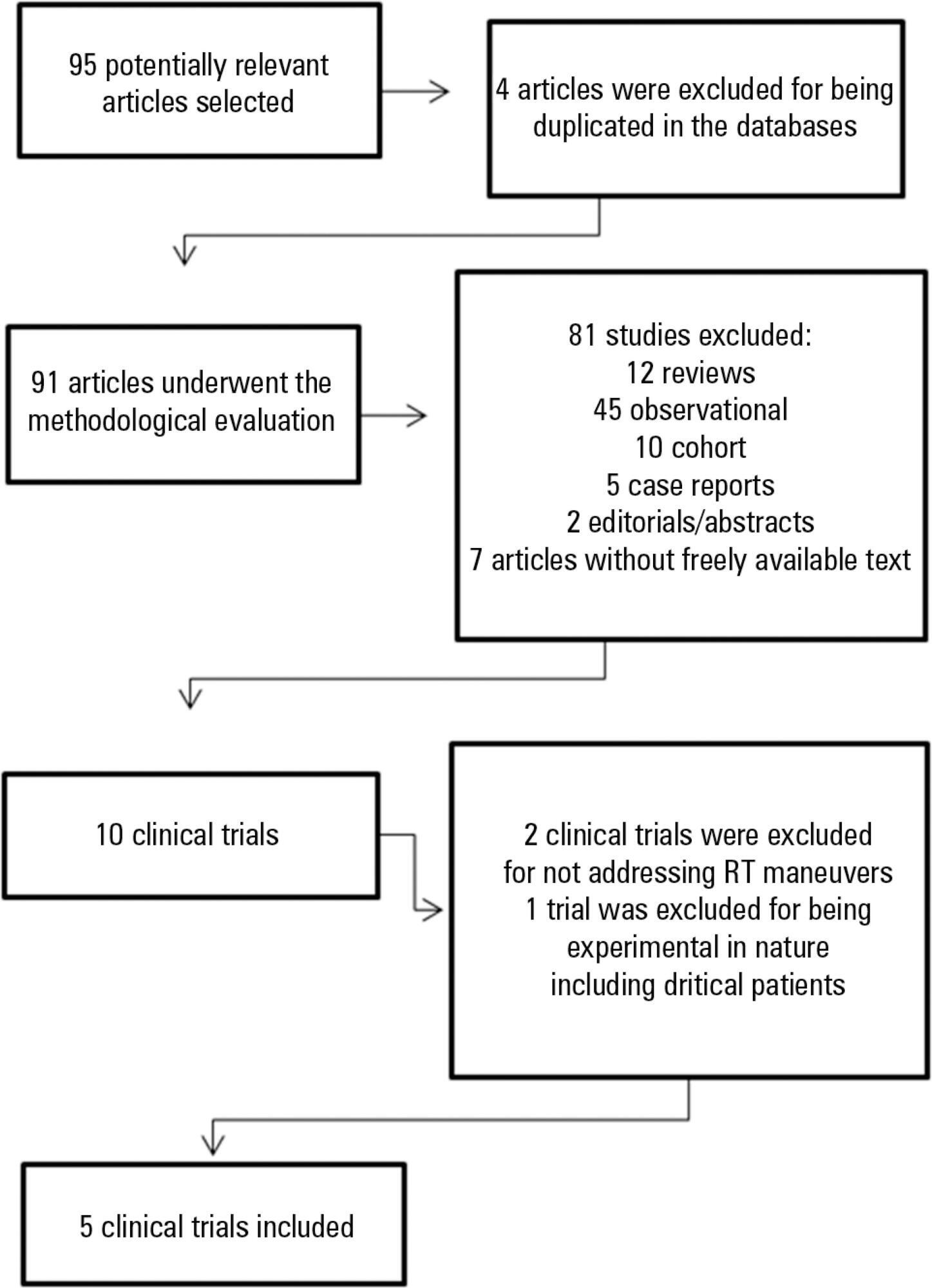
Through a systematic review of the literature, clinical trials published between 2002 and 2012 were selected. The search involved the LILACS, SciELO, MedLine and PEDro databases using the keywords "physical therapy", "physiotherapy", "respiratory therapy" and "randomized controlled trials" combined with the keyword "intracranial pressure".
In total, five studies, including a total of 164 patients between 25 and 65 years of age, reporting that respiratory physiotherapy maneuvers significantly increased intracranial pressure without changing the cerebral perfusion pressure were included. The articles addressed several techniques including vibration, vibrocompression, tapping, postural drainage, and the endotracheal aspiration maneuver. All patients required invasive mechanical ventilation.
Respiratory physiotherapy leads to increased intracranial pressure. Studies suggest that there are no short-term hemodynamic or respiratory repercussions or changes in the cerebral perfusion pressure. However, none of the studies evaluated the clinical outcomes or ensured the safety of the maneuvers.
Abstract
Rev Bras Ter Intensiva. 2013;25(4):327-333
DOI 10.5935/0103-507X.20130055
To analyze the outcomes of increased or decreased intracranial pressure and/or the decrease in cerebral perfusion pressure resulting from respiratory physiotherapy on critically ill patients admitted to the intensive care unit.
Through a systematic review of the literature, clinical trials published between 2002 and 2012 were selected. The search involved the LILACS, SciELO, MedLine and PEDro databases using the keywords "physical therapy", "physiotherapy", "respiratory therapy" and "randomized controlled trials" combined with the keyword "intracranial pressure".
In total, five studies, including a total of 164 patients between 25 and 65 years of age, reporting that respiratory physiotherapy maneuvers significantly increased intracranial pressure without changing the cerebral perfusion pressure were included. The articles addressed several techniques including vibration, vibrocompression, tapping, postural drainage, and the endotracheal aspiration maneuver. All patients required invasive mechanical ventilation.
Respiratory physiotherapy leads to increased intracranial pressure. Studies suggest that there are no short-term hemodynamic or respiratory repercussions or changes in the cerebral perfusion pressure. However, none of the studies evaluated the clinical outcomes or ensured the safety of the maneuvers.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):236-245
DOI 10.1590/S0103-507X2012000300006
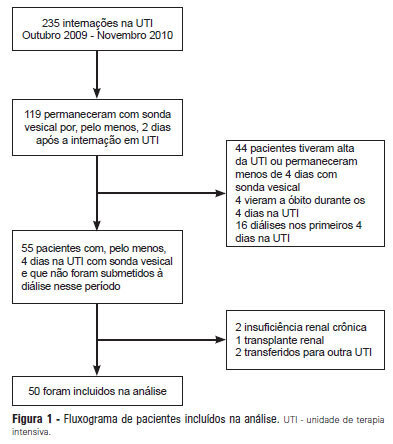
OBJECTIVE: Intensive care unit survivors and non-survivors have distinct acid-base profiles. The kidney's regulation of urinary electrolytes and the urinary strong ion difference plays a major role in acid-base homeostasis. The aim of this study was to evaluate the potential utility of daily spot urinary electrolyte measurement in acid-base and renal function monitoring. METHODS: We prospectively recorded daily plasma acid-base parameters and traditional markers of renal function in parallel with spot urinary electrolyte measurements in patients with urinary catheters admitted to our intensive care unit. Patients who remained in the intensive care unit for at least 4 days with a urinary catheter were included in the study. RESULTS: Of the 50 patients included in the study, 22% died during their intensive care unit stay. The incidence of acute kidney injury was significantly higher in non-survivors during the 4-day observation period (64% vs. 18% in survivors). Urinary chloride and sodium were lower and urinary strong ion difference was higher on day 1 in patients who developed acute kidney injury among both survivors and non-survivors. Both groups had similar urine output, although non-survivors had persistently higher urinary strong ion difference on all days. Survivors had a progressive improvement in metabolic acid-base profile due to increases in the plasma strong ion difference and decreases in weak acids. These changes were concomitant with decreases in urinary strong ion difference. In non-survivors, acid-base parameters did not significantly change during follow-up. CONCLUSIONS: Daily assessment of spot urinary electrolytes and strong ion difference are useful components of acid-base and renal function evaluations in critically ill patients, having distinct profiles between intensive care unit survivors and non-survivors.
Abstract
Rev Bras Ter Intensiva. 2012;24(3):236-245
DOI 10.1590/S0103-507X2012000300006
OBJECTIVE: Intensive care unit survivors and non-survivors have distinct acid-base profiles. The kidney's regulation of urinary electrolytes and the urinary strong ion difference plays a major role in acid-base homeostasis. The aim of this study was to evaluate the potential utility of daily spot urinary electrolyte measurement in acid-base and renal function monitoring. METHODS: We prospectively recorded daily plasma acid-base parameters and traditional markers of renal function in parallel with spot urinary electrolyte measurements in patients with urinary catheters admitted to our intensive care unit. Patients who remained in the intensive care unit for at least 4 days with a urinary catheter were included in the study. RESULTS: Of the 50 patients included in the study, 22% died during their intensive care unit stay. The incidence of acute kidney injury was significantly higher in non-survivors during the 4-day observation period (64% vs. 18% in survivors). Urinary chloride and sodium were lower and urinary strong ion difference was higher on day 1 in patients who developed acute kidney injury among both survivors and non-survivors. Both groups had similar urine output, although non-survivors had persistently higher urinary strong ion difference on all days. Survivors had a progressive improvement in metabolic acid-base profile due to increases in the plasma strong ion difference and decreases in weak acids. These changes were concomitant with decreases in urinary strong ion difference. In non-survivors, acid-base parameters did not significantly change during follow-up. CONCLUSIONS: Daily assessment of spot urinary electrolytes and strong ion difference are useful components of acid-base and renal function evaluations in critically ill patients, having distinct profiles between intensive care unit survivors and non-survivors.