Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(4):490-496
DOI 10.5935/0103-507X.20190086
To evaluate the concordance between the modified NUTRIC and NUTRIC with C-reactive protein instruments in identifying nutritional risk patients and predicting mortality in critically ill patients. The risk of death in patient groups was also investigated according to nutritional risk and malnutrition detected by subjective global assessment.
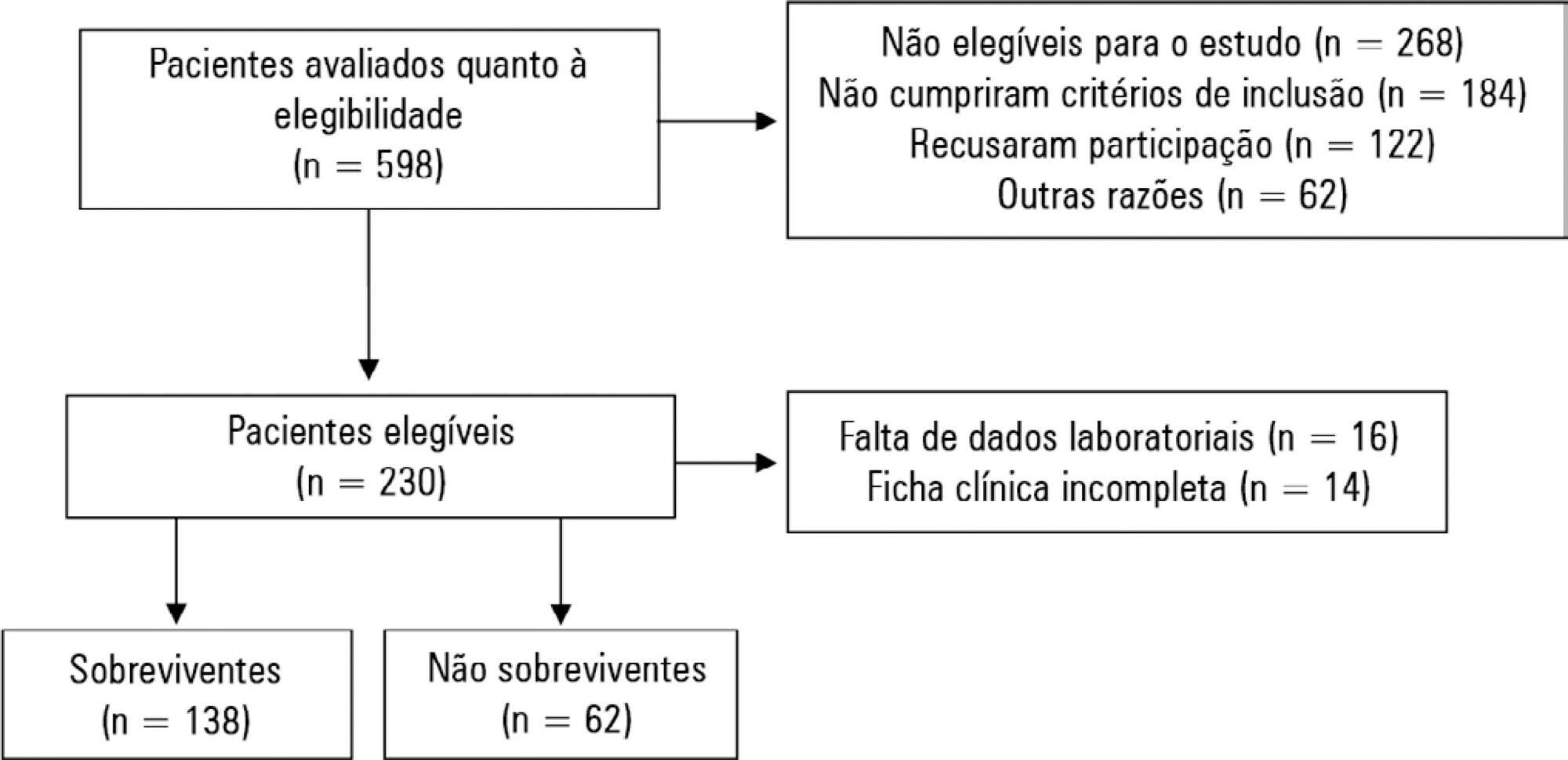
A cohort study of patients admitted to an intensive care unit. Nutritional risk was assessed by modified NUTRIC and a version of NUTRIC with C-reactive protein. Subjective global assessment was applied to diagnose malnutrition. Kappa statistics were calculated, and an ROC curve was constructed considering modified NUTRIC as a reference. The predictive validity was assessed considering mortality in 28 days (whether in the intensive care unit or after discharge) as the outcome.
A total of 130 patients were studied (63.05 ± 16.46 years, 53.8% males). According to NUTRIC with C-reactive protein, 34.4% were classified as having a high score, while 28.5% of patients had this classification with modified NUTRIC. According to SGA 48.1% of patients were malnourished. There was excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein (Kappa = 0.88, p < 0.001). The area under the ROC curve was equal to 0.942 (0.881 - 1.000) for NUTRIC with C-reactive protein. The risk of death within 28 days was increased in patients with high modified NUTRIC (HR = 1.827; 95%CI 1.029 - 3.244; p = 0.040) and NUTRIC with C-reactive protein (HR = 2.685; 95%CI 1.423 - 5.064; p = 0.002) scores. A high risk of death was observed in patients with high nutritional risk and malnutrition, independent of the version of the NUTRIC score applied.
An excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein was observed. In addition, combining NUTRIC and subjective global assessment may increase the accuracy of predicting mortality in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):490-496
DOI 10.5935/0103-507X.20190086
To evaluate the concordance between the modified NUTRIC and NUTRIC with C-reactive protein instruments in identifying nutritional risk patients and predicting mortality in critically ill patients. The risk of death in patient groups was also investigated according to nutritional risk and malnutrition detected by subjective global assessment.
A cohort study of patients admitted to an intensive care unit. Nutritional risk was assessed by modified NUTRIC and a version of NUTRIC with C-reactive protein. Subjective global assessment was applied to diagnose malnutrition. Kappa statistics were calculated, and an ROC curve was constructed considering modified NUTRIC as a reference. The predictive validity was assessed considering mortality in 28 days (whether in the intensive care unit or after discharge) as the outcome.
A total of 130 patients were studied (63.05 ± 16.46 years, 53.8% males). According to NUTRIC with C-reactive protein, 34.4% were classified as having a high score, while 28.5% of patients had this classification with modified NUTRIC. According to SGA 48.1% of patients were malnourished. There was excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein (Kappa = 0.88, p < 0.001). The area under the ROC curve was equal to 0.942 (0.881 - 1.000) for NUTRIC with C-reactive protein. The risk of death within 28 days was increased in patients with high modified NUTRIC (HR = 1.827; 95%CI 1.029 - 3.244; p = 0.040) and NUTRIC with C-reactive protein (HR = 2.685; 95%CI 1.423 - 5.064; p = 0.002) scores. A high risk of death was observed in patients with high nutritional risk and malnutrition, independent of the version of the NUTRIC score applied.
An excellent agreement between modified NUTRIC and NUTRIC with C-reactive protein was observed. In addition, combining NUTRIC and subjective global assessment may increase the accuracy of predicting mortality in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):434-443
DOI 10.5935/0103-507X.20190084
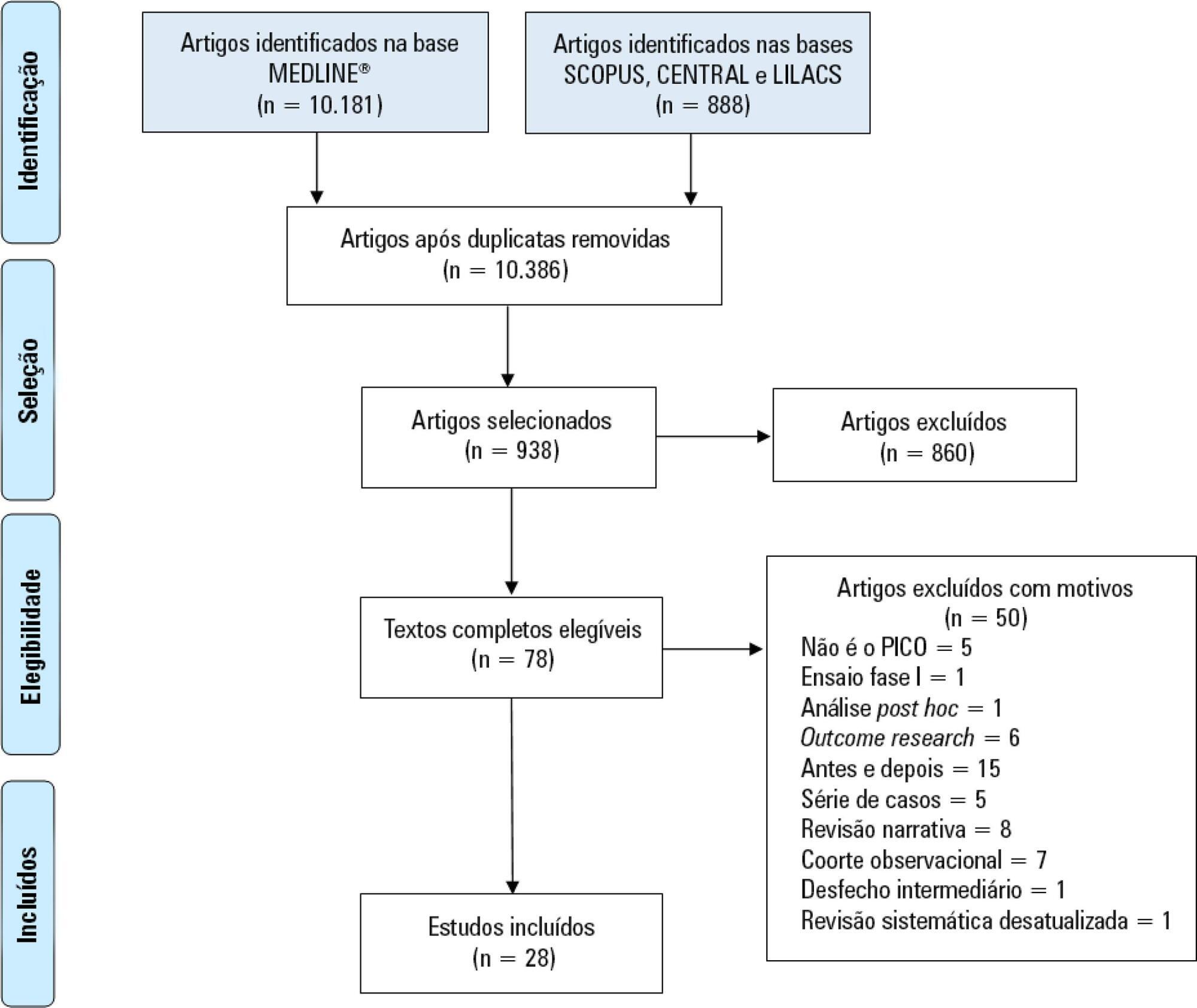
Immobility can cause several complications, including skeletal muscle atrophy and weakness, that influence the recovery of critically ill patients. This effect can be mitigated by early mobilization. Six key questions guided this research: Is early mobilization safe? Which patients are candidates for early mobilization? What are the contraindications? What is the appropriate dose, and how should it be defined? What results are obtained? What are the prognostic indicators for the use of early mobilization? The objective of this guideline was to produce a document that would provide evidence-based recommendations and suggestions regarding the early mobilization of critically ill adult patients, with the aim of improving understanding of the topic and making a positive impact on patient care. This guideline was based on a systematic review of articles conducted using the PICO search strategy, as recommended by the Guidelines Project of the Associação Médica Brasileira. Randomized clinical trials, prognostic cohort studies, and systematic reviews with or without meta-analysis were selected, and the evidence was classified according to the Oxford Center for Evidence-based Medicine Levels of Evidence. For all the questions addressed, enough evidence was found to support safe and well-defined early mobilization, with prognostic indicators that support and recommend the technique. Early mobilization is associated with better functional outcomes and should be performed whenever indicated. Early mobilization is safe and should be the goal of the entire multidisciplinary team.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):434-443
DOI 10.5935/0103-507X.20190084
Immobility can cause several complications, including skeletal muscle atrophy and weakness, that influence the recovery of critically ill patients. This effect can be mitigated by early mobilization. Six key questions guided this research: Is early mobilization safe? Which patients are candidates for early mobilization? What are the contraindications? What is the appropriate dose, and how should it be defined? What results are obtained? What are the prognostic indicators for the use of early mobilization? The objective of this guideline was to produce a document that would provide evidence-based recommendations and suggestions regarding the early mobilization of critically ill adult patients, with the aim of improving understanding of the topic and making a positive impact on patient care. This guideline was based on a systematic review of articles conducted using the PICO search strategy, as recommended by the Guidelines Project of the Associação Médica Brasileira. Randomized clinical trials, prognostic cohort studies, and systematic reviews with or without meta-analysis were selected, and the evidence was classified according to the Oxford Center for Evidence-based Medicine Levels of Evidence. For all the questions addressed, enough evidence was found to support safe and well-defined early mobilization, with prognostic indicators that support and recommend the technique. Early mobilization is associated with better functional outcomes and should be performed whenever indicated. Early mobilization is safe and should be the goal of the entire multidisciplinary team.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):521-528
DOI 10.5935/0103-507X.20190065
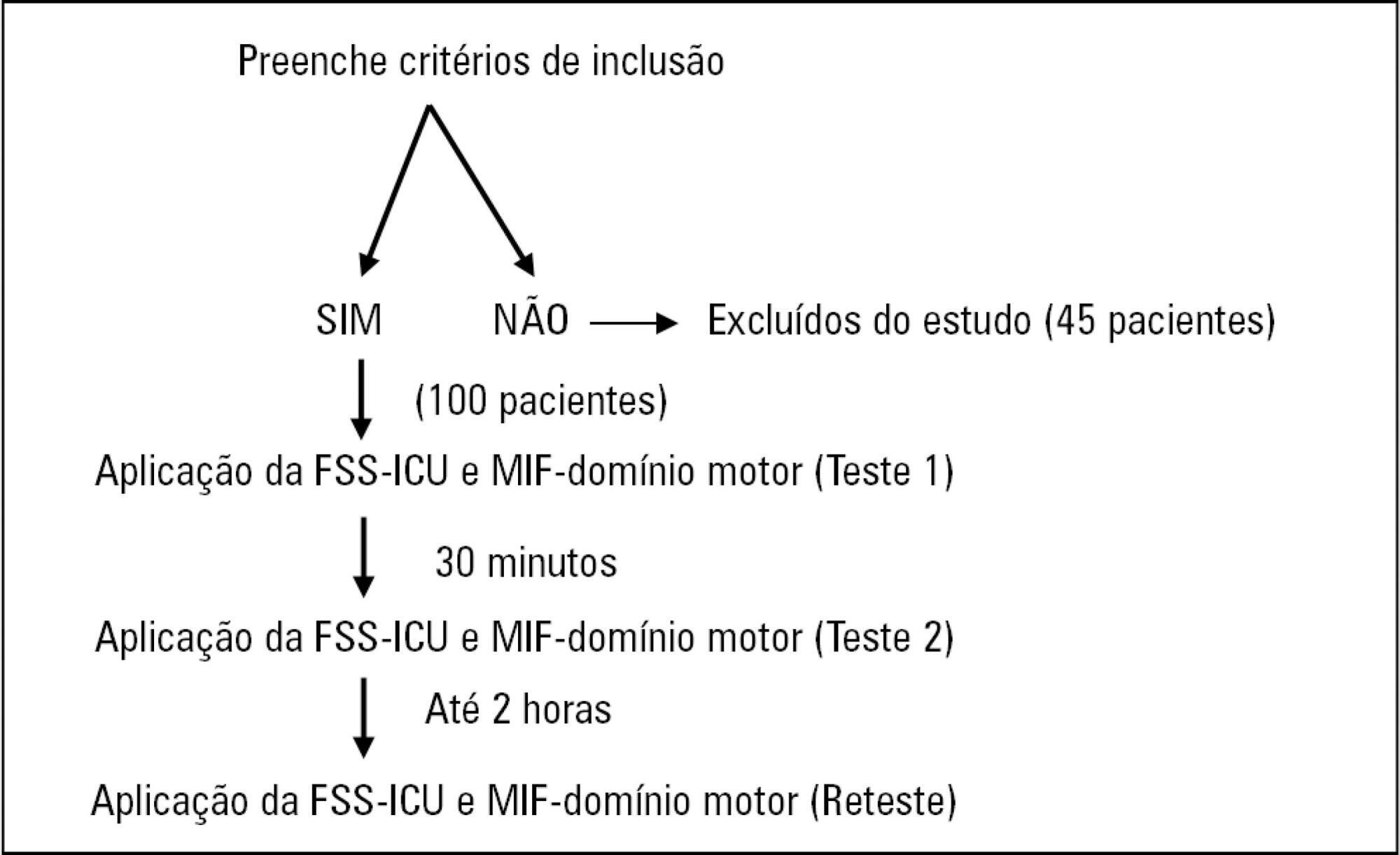
To compare the measurement properties (internal consistency, intra and interrater reliability, construct validity, and ceiling and floor effects) of the Functional Status Score for the ICU (FSS-ICU) and the Functional Independence Measure (FIM-motor domain).
In this study of measurement properties, the FSS-ICU and FIM were applied to 100 patients (72.1 ± 15.9 years; 53% male; Sequential Organ Failure Assessment = 11.0 ± 3.5 points, Simplified Acute Physiology Score 3 = 50.2 ± 16.8 points) in an intensive care unit at baseline and after 2 hours by physiotherapist 1 (test and retest) and 30 minutes after baseline by physiotherapist 2. The measurement properties evaluated were internal consistency (Cronbach's alpha), intra- and interrater reliability (intraclass correlation coefficient), agreement (standard error of measurement) and minimum detectable change at a 90% confidence level, ceiling and floor effects (frequency of maximum and minimum scores) and construct validity (Pearson's correlation).
The FSS-ICU and FIM presented adequate internal consistency (Cronbach's alpha, FSS-ICU = 0.95 and FIM = 0.86), intra-and interrater reliability for overall FSS-ICU and FIM score (ICC > 0.75), agreement (minimum detectable change at a 90% confidence level: FSS-ICU and FIM = 1.0 point; standard error of measurement: FSS-ICU = 2% and FIM = 1%) and construct validity (r = 0.94; p < 0.001). However, the FSS-ICU and FIM presented ceiling effects (maximum score for 16% of patients for the FSS-ICU and 18% for the FIM).
The FSS-ICU and FIM present adequate measurement properties to assess functionality in critically ill patients, although they present ceiling effects.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):521-528
DOI 10.5935/0103-507X.20190065
To compare the measurement properties (internal consistency, intra and interrater reliability, construct validity, and ceiling and floor effects) of the Functional Status Score for the ICU (FSS-ICU) and the Functional Independence Measure (FIM-motor domain).
In this study of measurement properties, the FSS-ICU and FIM were applied to 100 patients (72.1 ± 15.9 years; 53% male; Sequential Organ Failure Assessment = 11.0 ± 3.5 points, Simplified Acute Physiology Score 3 = 50.2 ± 16.8 points) in an intensive care unit at baseline and after 2 hours by physiotherapist 1 (test and retest) and 30 minutes after baseline by physiotherapist 2. The measurement properties evaluated were internal consistency (Cronbach's alpha), intra- and interrater reliability (intraclass correlation coefficient), agreement (standard error of measurement) and minimum detectable change at a 90% confidence level, ceiling and floor effects (frequency of maximum and minimum scores) and construct validity (Pearson's correlation).
The FSS-ICU and FIM presented adequate internal consistency (Cronbach's alpha, FSS-ICU = 0.95 and FIM = 0.86), intra-and interrater reliability for overall FSS-ICU and FIM score (ICC > 0.75), agreement (minimum detectable change at a 90% confidence level: FSS-ICU and FIM = 1.0 point; standard error of measurement: FSS-ICU = 2% and FIM = 1%) and construct validity (r = 0.94; p < 0.001). However, the FSS-ICU and FIM presented ceiling effects (maximum score for 16% of patients for the FSS-ICU and 18% for the FIM).
The FSS-ICU and FIM present adequate measurement properties to assess functionality in critically ill patients, although they present ceiling effects.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):529-535
DOI 10.5935/0103-507X.20190066
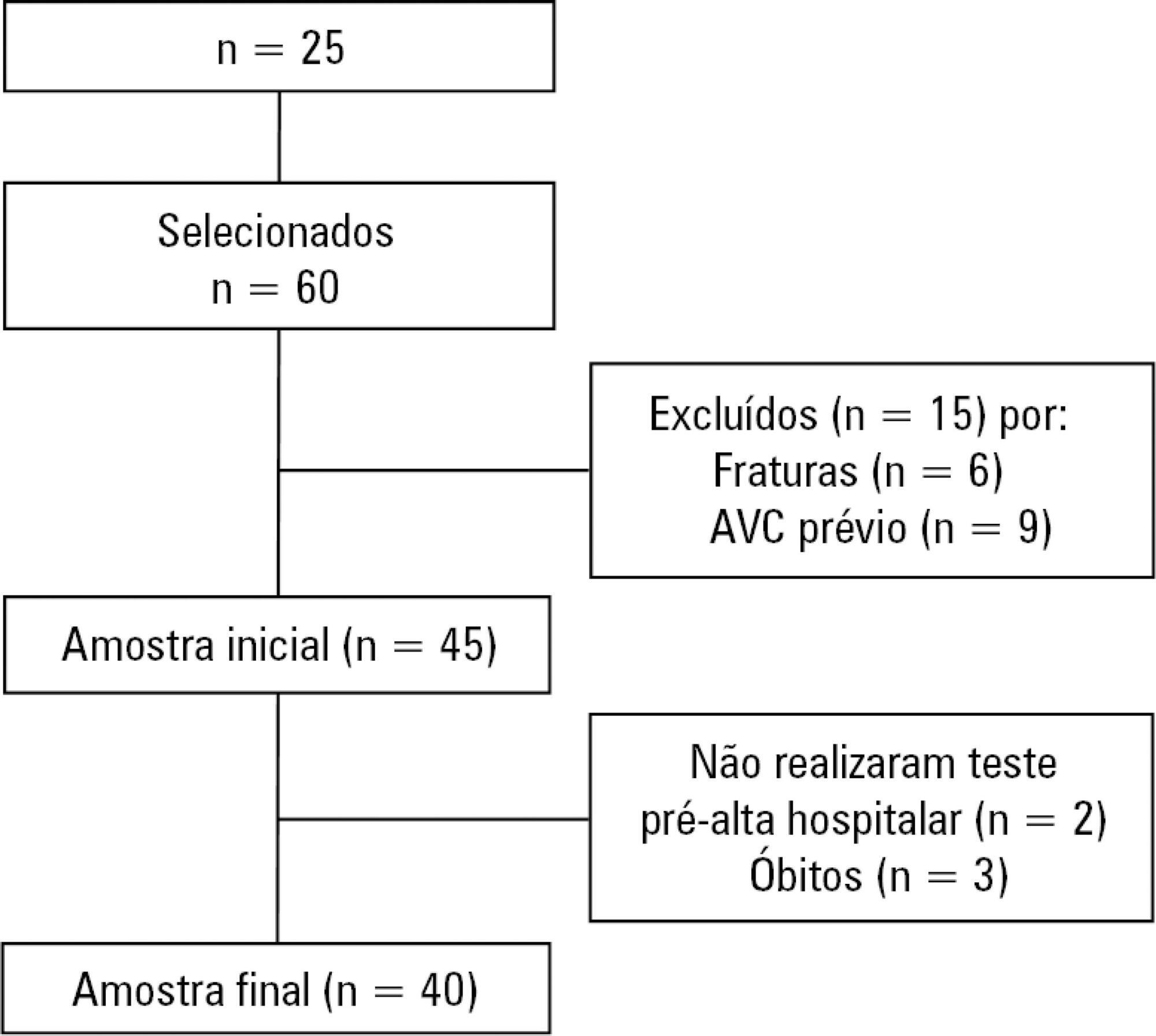
To measure and compare the functionality of patients after discharge from the intensive care unit and at the time of hospital discharge.
Quantitative study of a prospective cohort performed between August of 2016 and December of 2017 at a university hospital. A 10-meter walk test was performed at 2 timepoints: after discharge from the intensive care unit and prior to hospital discharge. The data were analyzed using Student's t-test and Pearson or Spearman correlation. Statistical Package for Social Science (SPSS) version 21.0 was used for the analysis, and p ≤ 0.05 was adopted as the level of significance.
Forty patients, with a mean age of 57.1 ± 12.2 years and with a predominance of males (60%), were evaluated. For the post-intensive care unit test, a mean speed of 0.48m/s was observed, and for the pre-hospital discharge test, there was an increase to 0.71m/s, evidencing functional evolution during the hospital stay (p < 0.001).
There was significant improvement in walking speed at the time of hospital discharge when compared to the walking speed at the time of intensive care unit discharge.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):529-535
DOI 10.5935/0103-507X.20190066
To measure and compare the functionality of patients after discharge from the intensive care unit and at the time of hospital discharge.
Quantitative study of a prospective cohort performed between August of 2016 and December of 2017 at a university hospital. A 10-meter walk test was performed at 2 timepoints: after discharge from the intensive care unit and prior to hospital discharge. The data were analyzed using Student's t-test and Pearson or Spearman correlation. Statistical Package for Social Science (SPSS) version 21.0 was used for the analysis, and p ≤ 0.05 was adopted as the level of significance.
Forty patients, with a mean age of 57.1 ± 12.2 years and with a predominance of males (60%), were evaluated. For the post-intensive care unit test, a mean speed of 0.48m/s was observed, and for the pre-hospital discharge test, there was an increase to 0.71m/s, evidencing functional evolution during the hospital stay (p < 0.001).
There was significant improvement in walking speed at the time of hospital discharge when compared to the walking speed at the time of intensive care unit discharge.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):282-288
DOI 10.5935/0103-507X.20190053
To describe the epidemiological profile of victims of cardiac arrest assisted using a nontransporting emergency medical service vehicle and to determine whether these patients met the criteria for the use of extracorporeal membrane oxygenation.
This study employed a retrospective, cohort, descriptive, and exploratory design. Data were collected in January 2018 in northern Portugal by consulting the records of nontransporting emergency medical service vehicles that provided assistance between 2012 and 2016. An observation grid was prepared that was supported by the instrument used for collecting data from the national registry of out-ofhospital cardiac arrests.
After applying the inclusion criteria, the sample consisted of 36 victims. Extracorporeal membrane oxygenation could have been applied to 24 victims during the period analyzed, which might have increased the odds for transplantation, survival, or both, for either the victim or other individuals.
Nontransporting emergency medical service vehicles have the potential for inclusion in the extracorporeal membrane oxygenation network of the study area.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):282-288
DOI 10.5935/0103-507X.20190053
To describe the epidemiological profile of victims of cardiac arrest assisted using a nontransporting emergency medical service vehicle and to determine whether these patients met the criteria for the use of extracorporeal membrane oxygenation.
This study employed a retrospective, cohort, descriptive, and exploratory design. Data were collected in January 2018 in northern Portugal by consulting the records of nontransporting emergency medical service vehicles that provided assistance between 2012 and 2016. An observation grid was prepared that was supported by the instrument used for collecting data from the national registry of out-ofhospital cardiac arrests.
After applying the inclusion criteria, the sample consisted of 36 victims. Extracorporeal membrane oxygenation could have been applied to 24 victims during the period analyzed, which might have increased the odds for transplantation, survival, or both, for either the victim or other individuals.
Nontransporting emergency medical service vehicles have the potential for inclusion in the extracorporeal membrane oxygenation network of the study area.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
To validate the "Checklist for Managing Critical Patients' Daily Awakening" instrument.
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):318-325
DOI 10.5935/0103-507X.20190057
To validate the "Checklist for Managing Critical Patients' Daily Awakening" instrument.
This was a descriptive study that used a quantitative approach for content validation using the Delphi method to obtain the consensus of experts who evaluated the instrument using a Likert scale. The validity index of each item of the instrument was calculated, with a minimum consensus parameter above 0.78.
Three Delphi rounds were required, starting with 29 experts and ending with 15 experts who were invited in person and via e-mail to participate in the study. Of the 15 items in the instrument, 13 had a content validity index > 0.78. The instrument maintained its attributes, and six items were reformulated without the need to exclude any of them. The validated items enabled the assessment of and decisions regarding the dimensions related to the level of sedation and agitation, vital signs, ventilatory parameters and pain. The instrument presented psychometric indicators with acceptable content validity.
The instrument proposed in the study exhibited content validity for most of its items and emerges as a practical strategy for the management of the daily interruption of sedation of critical patients.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients' medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 - 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 - 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 - 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 - 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 - 6.44; p < 0.001).
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients' medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 - 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 - 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 - 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 - 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 - 6.44; p < 0.001).
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.