Você pesquisou por y - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
To contribute to updating the recommendations for brain-dead potential organ donor management.
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):1-11
DOI 10.5935/0103-507X.20210001
To contribute to updating the recommendations for brain-dead potential organ donor management.
A group of 27 experts, including intensivists, transplant coordinators, transplant surgeons, and epidemiologists, answered questions related to the following topics were divided into mechanical ventilation, hemodynamics, endocrine-metabolic management, infection, body temperature, blood transfusion, and checklists use. The outcomes considered were cardiac arrests, number of organs removed or transplanted as well as function / survival of transplanted organs. The quality of evidence of the recommendations was assessed using the Grading of Recommendations Assessment, Development, and Evaluation system to classify the recommendations.
A total of 19 recommendations were drawn from the expert panel. Of these, 7 were classified as strong, 11 as weak and 1 was considered a good clinical practice.
Despite the agreement among panel members on most recommendations, the grade of recommendation was mostly weak.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):102-110
DOI 10.5935/0103-507X.20210011
To perform a cross-cultural adaptation of the Richmond Agitation-Sedation Scale (RASS) to Brazilian Portuguese for the evaluation of sedation in pediatric intensive care.
Cross-cultural adaptation process including the conceptual, item, semantic and operational equivalence stages according to current recommendations.
Pretests, divided into two stages, included 30 professionals from the pediatric intensive care unit of a university hospital, who administered the translated RASS to patients aged 29 days to 18 years. The pretests showed a content validity index above 0.90 for all items: 0.97 in the first stage of pretests and 0.99 in the second.
The cross-cultural adaptation of RASS to Brazilian Portuguese resulted in a version with excellent comprehensibility and acceptability in a pediatric intensive care setting. Reliability and validity studies should be performed to evaluate the psychometric properties of the Brazilian Portuguese version of the RASS.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):111-118
DOI 10.5935/0103-507X.20210012
To evaluate the incidence of hypothermia in patients undergoing continuous renal replacement therapy in the intensive care unit. As secondary objectives, we determined associated factors and compared the occurrence of hypothermia between two modalities of continuous renal replacement therapy.
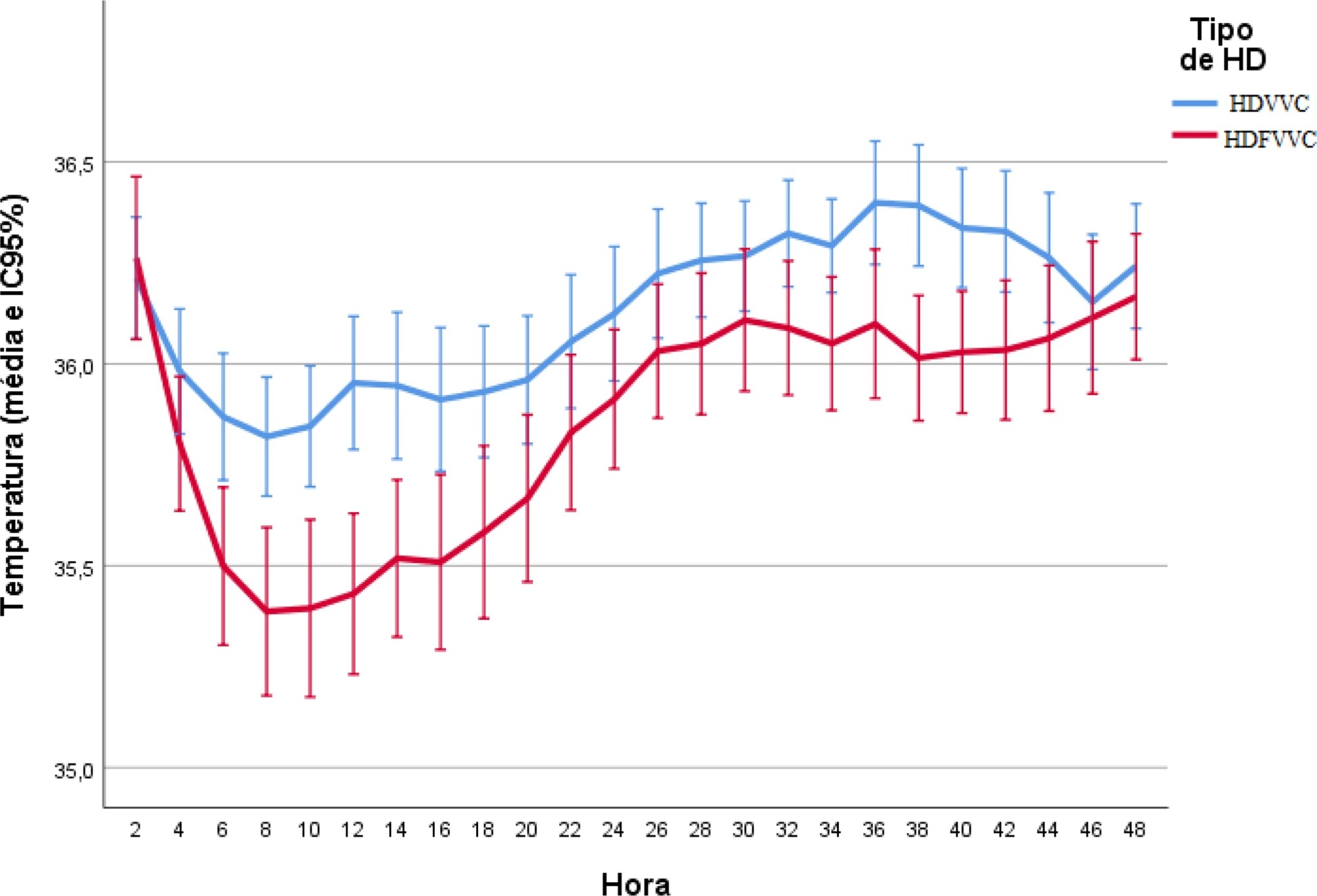
A prospective cohort study was conducted with adult patients who were admitted to a clinical-surgical intensive care unit and underwent continuous renal replacement therapy in a high-complexity public university hospital in southern Brazil from April 2017 to July 2018. Hypothermia was defined as a body temperature ≤ 35ºC. The patients included in the study were followed for the first 48 hours of continuous renal replacement therapy. The researchers collected data from medical records and continuous renal replacement therapy records.
A total of 186 patients were equally distributed between two types of continuous renal replacement therapy: hemodialysis and hemodiafiltration. The incidence of hypothermia was 52.7% and was higher in patients admitted for shock (relative risk of 2.11; 95%CI 1.21 - 3.69; p = 0.009) and in those who underwent hemodiafiltration with heating in the return line (relative risk of 1.50; 95%CI 1.13 - 1.99; p = 0.005).
Hypothermia in critically ill patients with continuous renal replacement therapy is frequent, and the intensive care team should be attentive, especially when there are associated risk factors.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):111-118
DOI 10.5935/0103-507X.20210012
To evaluate the incidence of hypothermia in patients undergoing continuous renal replacement therapy in the intensive care unit. As secondary objectives, we determined associated factors and compared the occurrence of hypothermia between two modalities of continuous renal replacement therapy.
A prospective cohort study was conducted with adult patients who were admitted to a clinical-surgical intensive care unit and underwent continuous renal replacement therapy in a high-complexity public university hospital in southern Brazil from April 2017 to July 2018. Hypothermia was defined as a body temperature ≤ 35ºC. The patients included in the study were followed for the first 48 hours of continuous renal replacement therapy. The researchers collected data from medical records and continuous renal replacement therapy records.
A total of 186 patients were equally distributed between two types of continuous renal replacement therapy: hemodialysis and hemodiafiltration. The incidence of hypothermia was 52.7% and was higher in patients admitted for shock (relative risk of 2.11; 95%CI 1.21 - 3.69; p = 0.009) and in those who underwent hemodiafiltration with heating in the return line (relative risk of 1.50; 95%CI 1.13 - 1.99; p = 0.005).
Hypothermia in critically ill patients with continuous renal replacement therapy is frequent, and the intensive care team should be attentive, especially when there are associated risk factors.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):119-124
DOI 10.5935/0103-507X.20210013
To assess the performance of Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 2 scores in the pediatric intensive care unit.
A retrospective cohort study. Data were retrospectively collected from medical records of all patients admitted to the pediatric intensive care unit of a cancer hospital from January 2017 to June 2018.
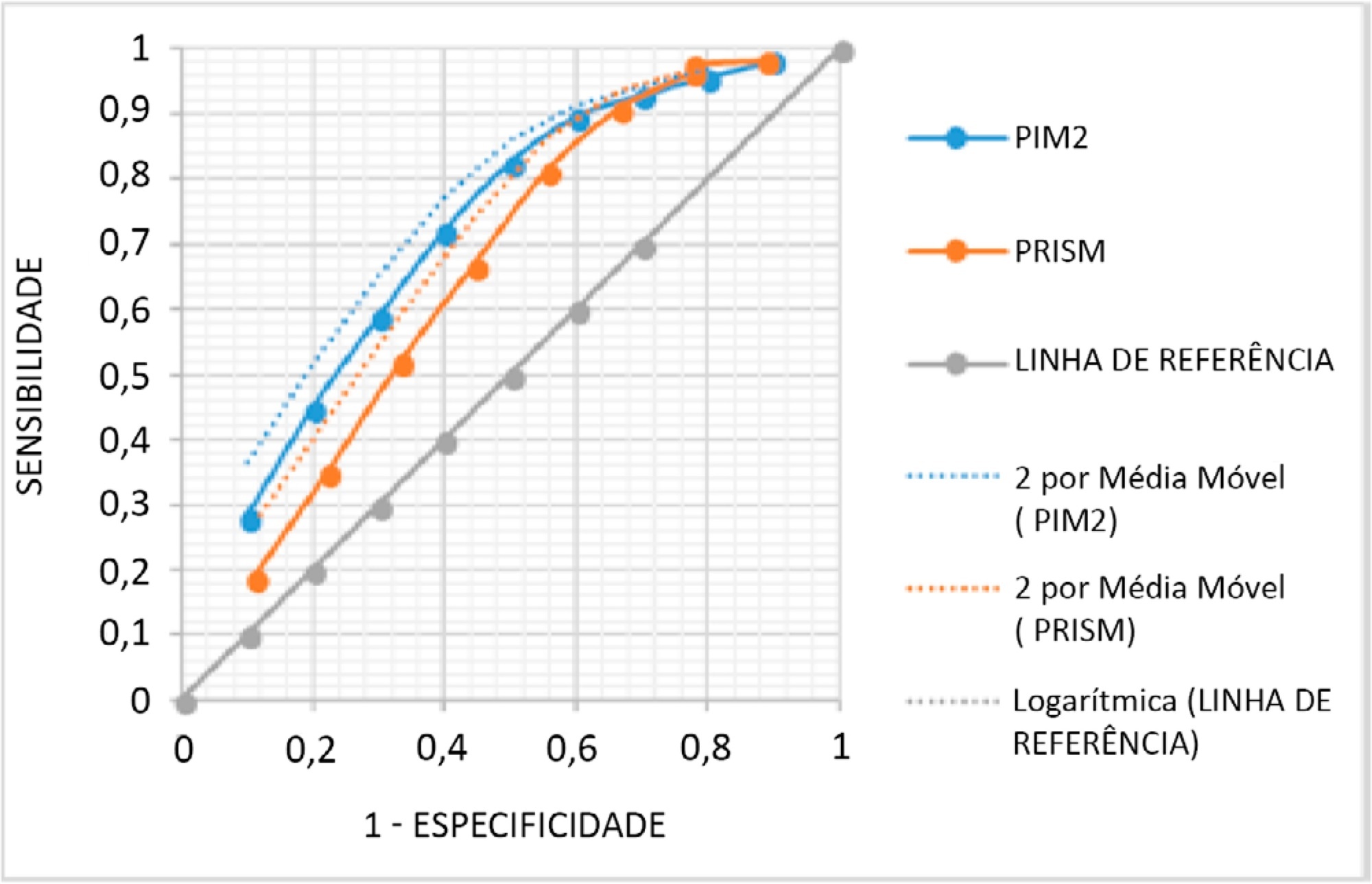
The mean PRISM III score was 15, and PIM 2, 24%. From the 338 studied patients, 62 (18.34%) died. The PRISM III estimated mortality was 79.52 patients (23.52%) and for PIM 2 80.19 patients (23.72%), corresponding to a standardized mortality ratio (95% confidence interval: 0.78 for PRISM II and 0.77 for PIM 2). The Hosmer-Lemeshow chi-square test was 11.56, 8df, 0.975 for PRISM II and 0.48, 8df, p = 0.999 for PIM 2. The area under the Receiver Operating Characteristic curve was 0.71 for PRISM III and 0.76 for PIM 2.
Both scores overestimated mortality and have shown a regular ability to discriminate between survivors and non-survivors. Models should be developed to quantify the severity of cancer pediatric patients in Pediatric Intensive Care Units and to predict the mortality risk accounting for their peculiarities.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):119-124
DOI 10.5935/0103-507X.20210013
To assess the performance of Pediatric Risk of Mortality (PRISM) III and Pediatric Index of Mortality (PIM) 2 scores in the pediatric intensive care unit.
A retrospective cohort study. Data were retrospectively collected from medical records of all patients admitted to the pediatric intensive care unit of a cancer hospital from January 2017 to June 2018.
The mean PRISM III score was 15, and PIM 2, 24%. From the 338 studied patients, 62 (18.34%) died. The PRISM III estimated mortality was 79.52 patients (23.52%) and for PIM 2 80.19 patients (23.72%), corresponding to a standardized mortality ratio (95% confidence interval: 0.78 for PRISM II and 0.77 for PIM 2). The Hosmer-Lemeshow chi-square test was 11.56, 8df, 0.975 for PRISM II and 0.48, 8df, p = 0.999 for PIM 2. The area under the Receiver Operating Characteristic curve was 0.71 for PRISM III and 0.76 for PIM 2.
Both scores overestimated mortality and have shown a regular ability to discriminate between survivors and non-survivors. Models should be developed to quantify the severity of cancer pediatric patients in Pediatric Intensive Care Units and to predict the mortality risk accounting for their peculiarities.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):12-30
DOI 10.5935/0103-507X.20210002
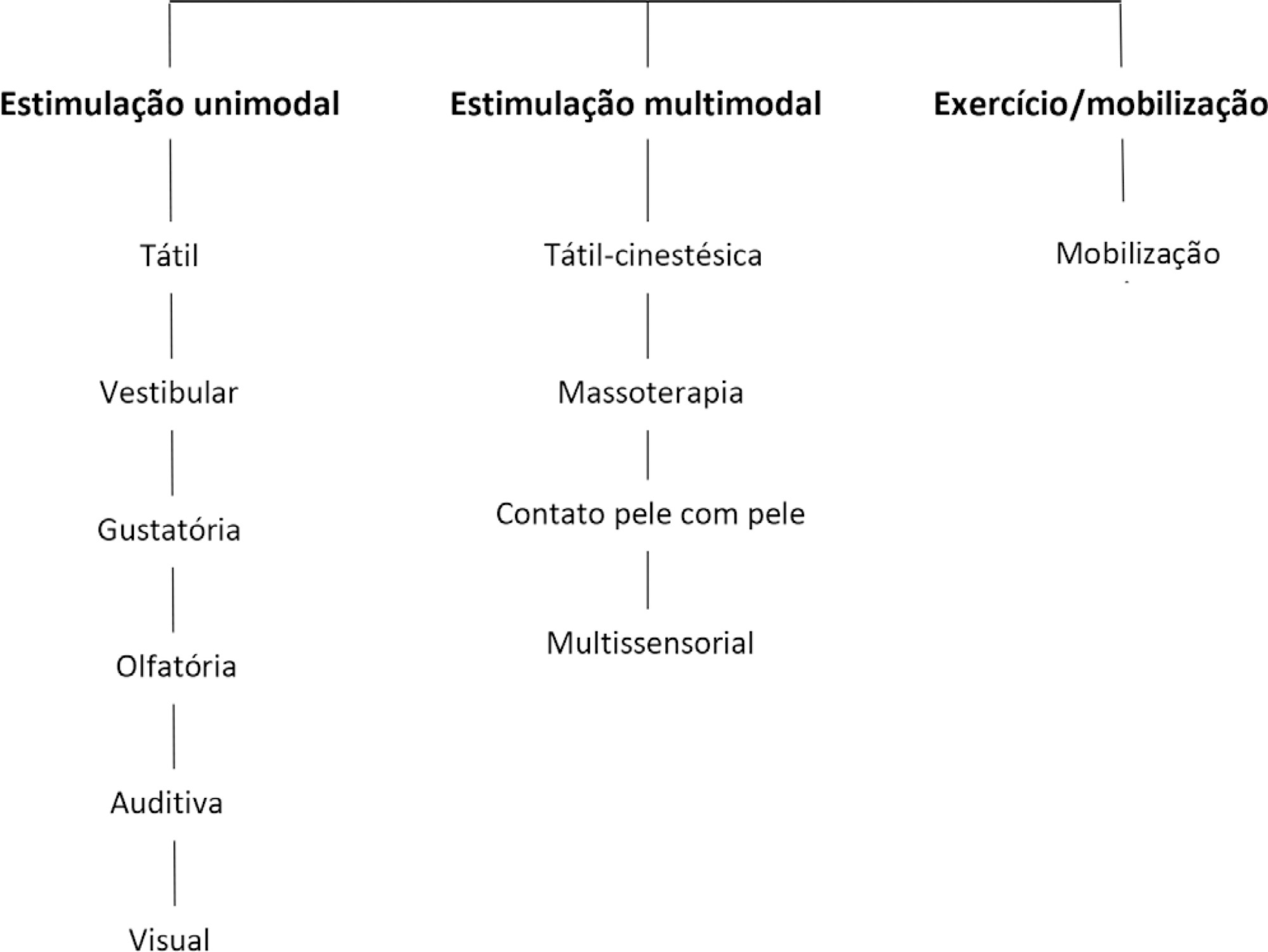
To present guidelines on sensory motor stimulation for newborns and infants in the intensive care unit.
We employed a mixed methods design with a systematic review of the literature and recommendations based on scientific evidence and the opinions of physiotherapists with neonatal expertise. The research included studies published between 2010 and 2018 in the MEDLINE® and Cochrane databases that included newborns (preterm and term) and infants (between 28 days and 6 months of age) hospitalized in the intensive care unit and submitted to sensory motor stimulation methods. The studies found were classified according to the GRADE score by five physiotherapists in different regions of Brazil and presented at eight Scientific Congresses held to discuss the clinical practice guidelines.
We included 89 articles to construct the clinical practice guidelines. Auditory, gustatory and skin-to-skin stimulation stand out for enhancing vital signs, and tactile-kinesthetic massage and multisensory stimulation stand out for improving weight or sucking.
Although all modalities have good ratings for pain or stress control, it is recommended that sensory motor stimulation procedures be tailored to the infant’s specific needs and that interventions and be carried out by expert professionals.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):12-30
DOI 10.5935/0103-507X.20210002
To present guidelines on sensory motor stimulation for newborns and infants in the intensive care unit.
We employed a mixed methods design with a systematic review of the literature and recommendations based on scientific evidence and the opinions of physiotherapists with neonatal expertise. The research included studies published between 2010 and 2018 in the MEDLINE® and Cochrane databases that included newborns (preterm and term) and infants (between 28 days and 6 months of age) hospitalized in the intensive care unit and submitted to sensory motor stimulation methods. The studies found were classified according to the GRADE score by five physiotherapists in different regions of Brazil and presented at eight Scientific Congresses held to discuss the clinical practice guidelines.
We included 89 articles to construct the clinical practice guidelines. Auditory, gustatory and skin-to-skin stimulation stand out for enhancing vital signs, and tactile-kinesthetic massage and multisensory stimulation stand out for improving weight or sucking.
Although all modalities have good ratings for pain or stress control, it is recommended that sensory motor stimulation procedures be tailored to the infant’s specific needs and that interventions and be carried out by expert professionals.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):125-137
DOI 10.5935/0103-507X.20210014
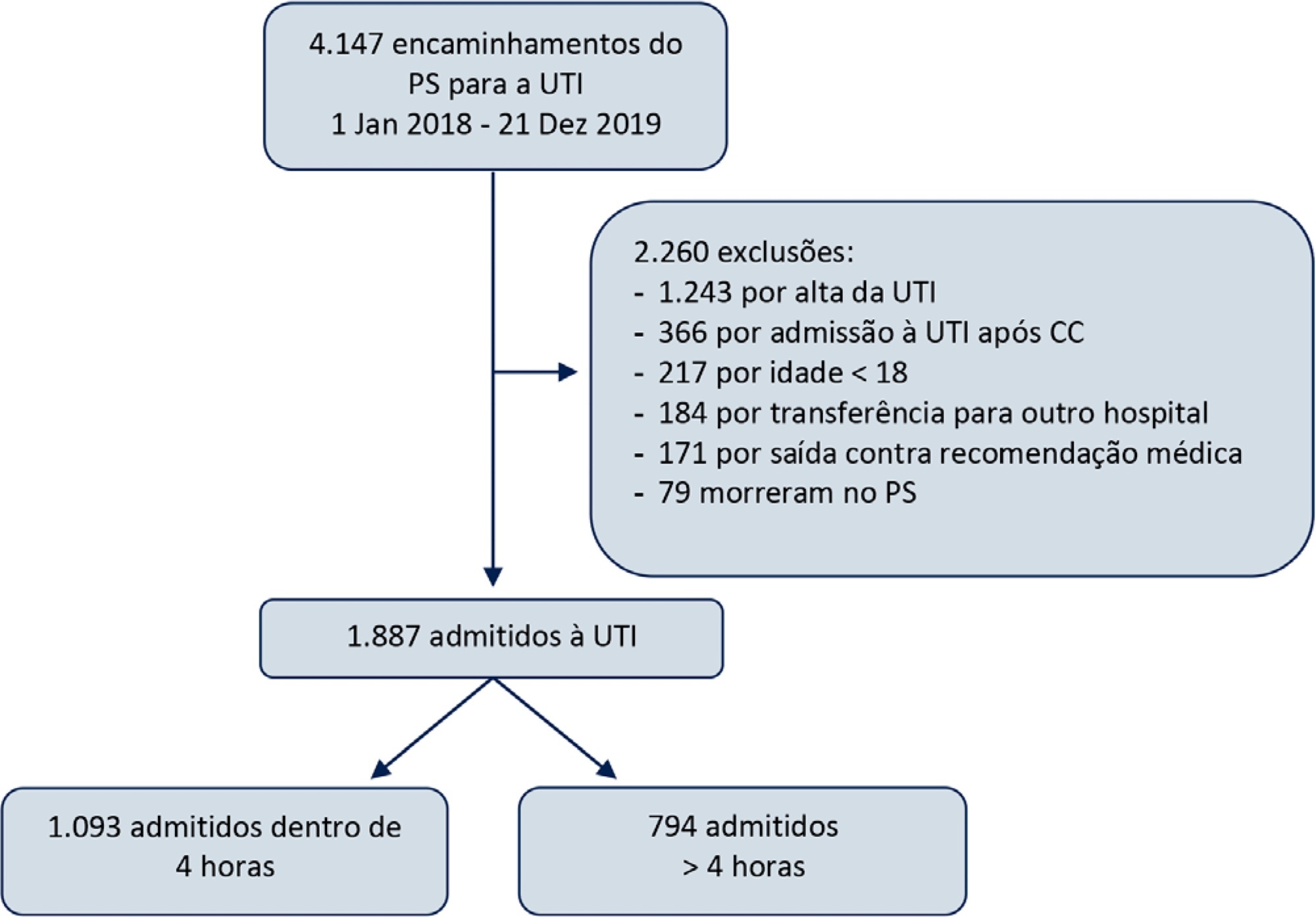
To study the impact of delayed admission by more than 4 hours on the outcomes of critically ill patients.
This was a retrospective observational study in which adult patients admitted directly from the emergency department to the intensive care unit were divided into two groups: Timely Admission if they were admitted within 4 hours and Delayed Admission if admission was delayed for more than 4 hours. Intensive care unit length of stay and hospital/intensive care unit mortality were compared between the groups. Propensity score matching was performed to correct for imbalances. Logistic regression analysis was used to explore delayed admission as an independent risk factor for intensive care unit mortality.
During the study period, 1,887 patients were admitted directly from the emergency department to the intensive care unit, with 42% being delayed admissions. Delayed patients had significantly longer intensive care unit lengths of stay and higher intensive care unit and hospital mortality. These results were persistent after propensity score matching of the groups. Delayed admission was an independent risk factor for intensive care unit mortality (OR = 2.6; 95%CI 1.9 - 3.5; p < 0.001). The association of delay and intensive care unit mortality emerged after a delay of 2 hours and was highest after a delay of 4 hours.
Delayed admission to the intensive care unit from the emergency department is an independent risk factor for intensive care unit mortality, with the strongest association being after a delay of 4 hours.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):125-137
DOI 10.5935/0103-507X.20210014
To study the impact of delayed admission by more than 4 hours on the outcomes of critically ill patients.
This was a retrospective observational study in which adult patients admitted directly from the emergency department to the intensive care unit were divided into two groups: Timely Admission if they were admitted within 4 hours and Delayed Admission if admission was delayed for more than 4 hours. Intensive care unit length of stay and hospital/intensive care unit mortality were compared between the groups. Propensity score matching was performed to correct for imbalances. Logistic regression analysis was used to explore delayed admission as an independent risk factor for intensive care unit mortality.
During the study period, 1,887 patients were admitted directly from the emergency department to the intensive care unit, with 42% being delayed admissions. Delayed patients had significantly longer intensive care unit lengths of stay and higher intensive care unit and hospital mortality. These results were persistent after propensity score matching of the groups. Delayed admission was an independent risk factor for intensive care unit mortality (OR = 2.6; 95%CI 1.9 - 3.5; p < 0.001). The association of delay and intensive care unit mortality emerged after a delay of 2 hours and was highest after a delay of 4 hours.
Delayed admission to the intensive care unit from the emergency department is an independent risk factor for intensive care unit mortality, with the strongest association being after a delay of 4 hours.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):138-145
DOI 10.5935/0103-507X.20210015
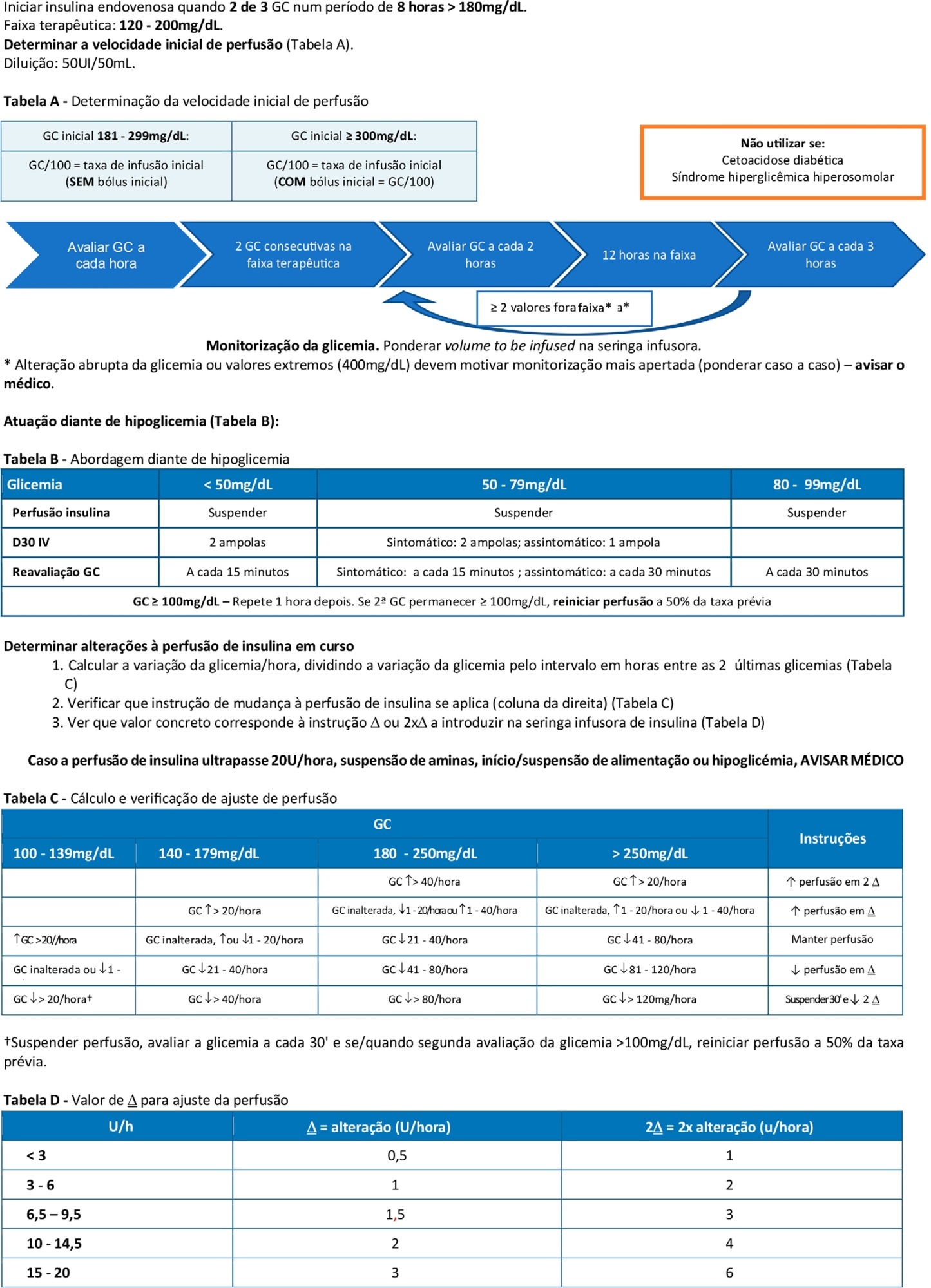
To double the percentage of time within the 100 - 180mg/dL blood glucose range in the first three months following a phased implementation of a formal education program, and then, of an insulin therapy protocol, without entailing an increased incidence of hypoglycemia.
The pre-intervention glycemic control was assessed retrospectively. Next, were carried out the implementation of a formal education program, distribution of manual algorithms for intravenous insulin therapy - optimized by the users, based on the modified Yale protocol - and informal training of the nursing staff. The use of electronic blood glucose control systems was supported, and the results were recorded prospectively.
The first phase of the program (formal education) lead to improvement of the time within the euglycemic interval (28% to 37%). In the second phase, euglycemia was achieved 66% of the time, and the incidence of hypoglycemia was decreased. The percentage of patients on intravenous insulin infusion at 48 hours from admission increased from 6% to 35%.
The phased implementation of a formal education program, fostering the use of electronic insulin therapy protocols and dynamic manuals, received good adherence and has shown to be safe and effective for blood glucose control in critically ill patients, with a concomitant decrease in hypoglycemia.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):138-145
DOI 10.5935/0103-507X.20210015
To double the percentage of time within the 100 - 180mg/dL blood glucose range in the first three months following a phased implementation of a formal education program, and then, of an insulin therapy protocol, without entailing an increased incidence of hypoglycemia.
The pre-intervention glycemic control was assessed retrospectively. Next, were carried out the implementation of a formal education program, distribution of manual algorithms for intravenous insulin therapy - optimized by the users, based on the modified Yale protocol - and informal training of the nursing staff. The use of electronic blood glucose control systems was supported, and the results were recorded prospectively.
The first phase of the program (formal education) lead to improvement of the time within the euglycemic interval (28% to 37%). In the second phase, euglycemia was achieved 66% of the time, and the incidence of hypoglycemia was decreased. The percentage of patients on intravenous insulin infusion at 48 hours from admission increased from 6% to 35%.
The phased implementation of a formal education program, fostering the use of electronic insulin therapy protocols and dynamic manuals, received good adherence and has shown to be safe and effective for blood glucose control in critically ill patients, with a concomitant decrease in hypoglycemia.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):146-153
DOI 10.5935/0103-507X.20210016
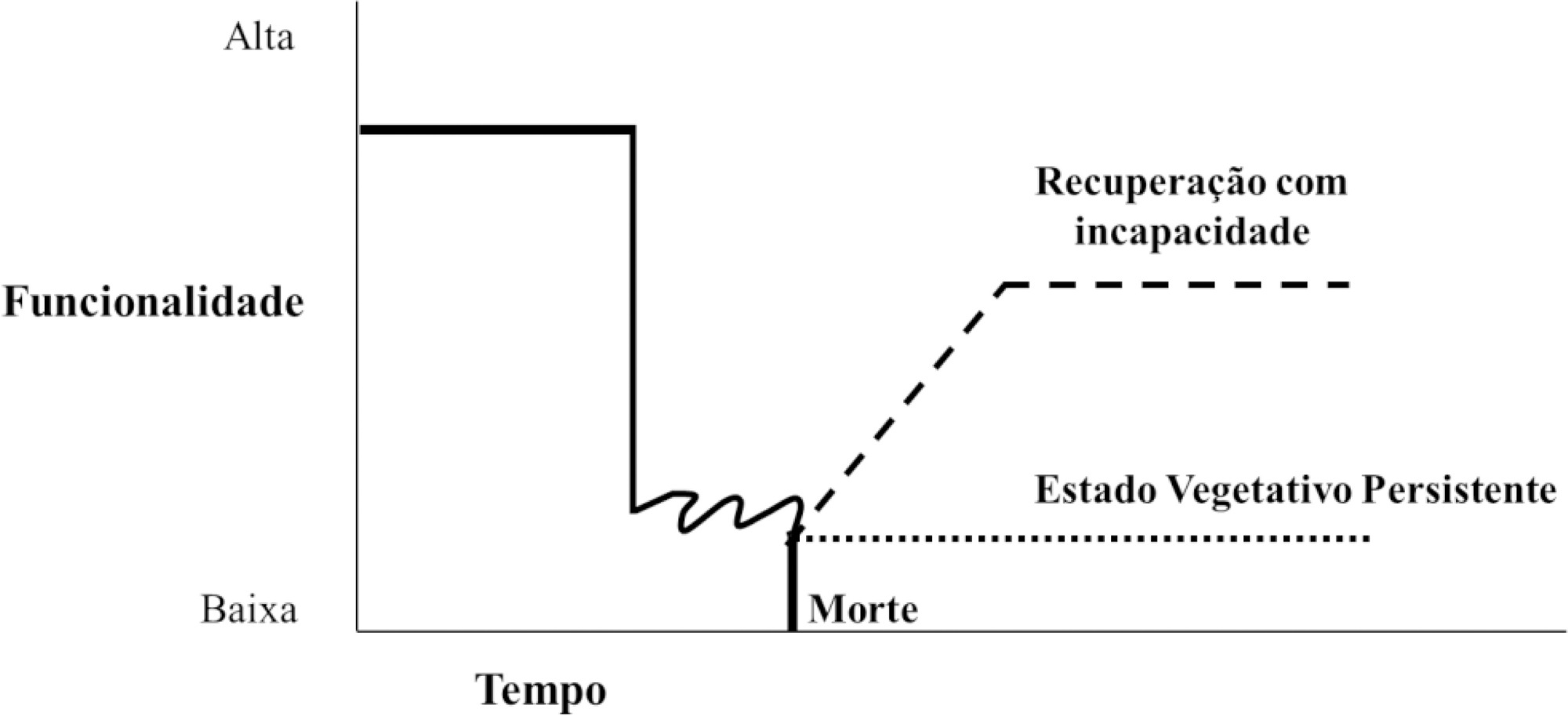
Neurological diseases are estimated to affect 1 billion people worldwide and are the cause of one in 10 deaths. In Brazil, they are responsible for approximately 14% of clinical admissions to intensive care units, 9% of elective neurosurgeries and 14% of emergency neurosurgeries. Many of these conditions are incurable, result in reduced life expectancy and quality of life and increased dependence, and are associated with symptoms that are likely to cause suffering, which justifies the integration of palliative care into usual care. In addition, factors unique to acute neurological injuries, such as their catastrophic clinical presentation, complex and uncertain prognosis, associated communication difficulties and issues related to quality of life, require a specific approach, which has recently been termed "neuropalliative care". Although the topic is relevant and current, it is still little discussed, and much of what is known about palliative care in this context is extrapolated from approaches used under other conditions. Therefore, the objective of this study was to conduct a narrative literature review to identify the challenges of applying the palliative care approach in the care of neurocritically ill patients, with a focus on three groups: neurocritically ill patients, families and intensive care teams. This review identified that in intensive care, the main demands for palliative care are for prognostic definitions and care planning. Training in primary palliative care and improving communication were also needs identified by intensivists and families, respectively. In contrast with what has been found under other conditions, the management of symptoms was not indicated as a complex issue, although it is still relevant.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):146-153
DOI 10.5935/0103-507X.20210016
Neurological diseases are estimated to affect 1 billion people worldwide and are the cause of one in 10 deaths. In Brazil, they are responsible for approximately 14% of clinical admissions to intensive care units, 9% of elective neurosurgeries and 14% of emergency neurosurgeries. Many of these conditions are incurable, result in reduced life expectancy and quality of life and increased dependence, and are associated with symptoms that are likely to cause suffering, which justifies the integration of palliative care into usual care. In addition, factors unique to acute neurological injuries, such as their catastrophic clinical presentation, complex and uncertain prognosis, associated communication difficulties and issues related to quality of life, require a specific approach, which has recently been termed "neuropalliative care". Although the topic is relevant and current, it is still little discussed, and much of what is known about palliative care in this context is extrapolated from approaches used under other conditions. Therefore, the objective of this study was to conduct a narrative literature review to identify the challenges of applying the palliative care approach in the care of neurocritically ill patients, with a focus on three groups: neurocritically ill patients, families and intensive care teams. This review identified that in intensive care, the main demands for palliative care are for prognostic definitions and care planning. Training in primary palliative care and improving communication were also needs identified by intensivists and families, respectively. In contrast with what has been found under other conditions, the management of symptoms was not indicated as a complex issue, although it is still relevant.