Original Article Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):263-268
DOI 10.5935/0103-507X.20140037
In clinical intensive care practice, weaning from mechanical ventilation is accompanied by concurrent early patient mobilization. The aim of this study was to compare the success of extubation performed with patients seated in an armchair compared to extubation with patients in a supine position.
A retrospective study, observational and non-randomized was conducted in a mixed-gender, 23-bed intensive care unit. The primary study outcome was success of extubation, which was defined as the patient tolerating the removal of the endotracheal tube for at least 48 hours. The differences between the study groups were assessed using Student's t-test and chi-squared analysis.
Ninety-one patients were included from December 2010 and June 2011. The study population had a mean age of 71 years ± 12 months, a mean APACHE II score of 21±7.6, and a mean length of mechanical ventilation of 2.6±2 days. Extubation was performed in 33 patients who were seated in an armchair (36%) and in 58 patients in a supine position (64%). There were no significant differences in age, mean APACHE II score or length of mechanical ventilation between the two groups, and a similar extubation success rate was observed (82%, seated group versus 85%, supine group, p>0.05). Furthermore, no significant differences were found between the two groups in terms of post-extubation distress, need for tracheostomy, duration of mechanical ventilation weaning, or intensive care unit stay.
Our results suggest that the clinical outcomes of patients extubated in a seated position are similar to those of patients extubated in a supine position. This new practice of seated extubation was not associated with adverse events and allowed extubation to occur simultaneously with early mobilization.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):269-276
DOI 10.5935/0103-507X.20140038
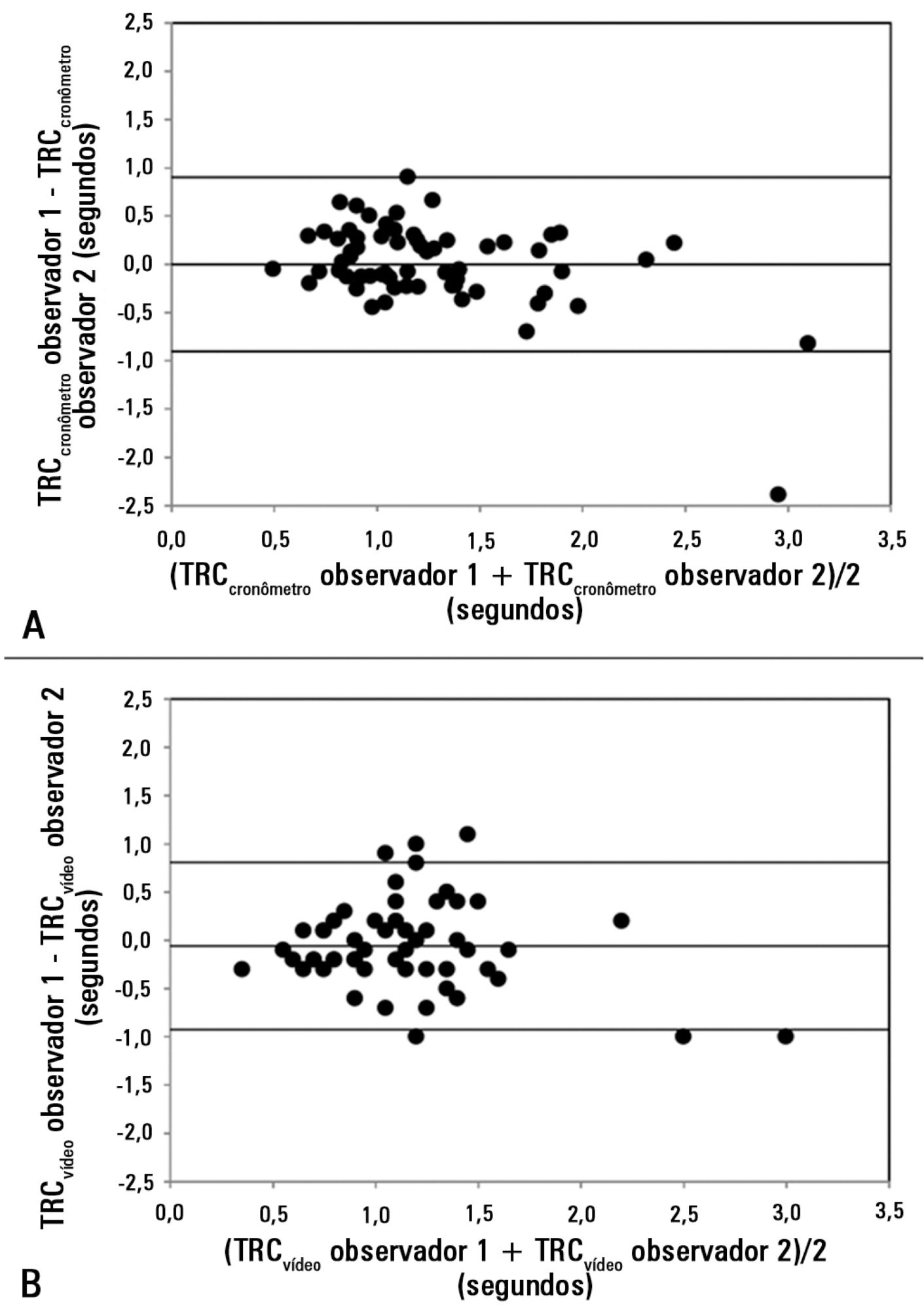
Peripheral perfusion abnormalities are relevant manifestations of shock. Capillary refill time is commonly used for their evaluation. However, the reproducibility of capillary refill time measurements and their correlation with other variables of peripheral perfusion, have not been comprehensively evaluated. Our goal was to determine, in healthy volunteers, the agreement between different methods of capillary refill time quantification and different observers, as well as their correlation with other markers of peripheral perfusion.
We studied 63 healthy volunteers. Two observers measured capillary refill time by means of two methods, direct view (CRTchronometer) and video analysis (CRTvideo). We also measured perfusion index (PI) derived from pulse plethysmography and finger pad temperature (Tºperipheral). The agreement between observers and methods was assessed using the Bland and Altman method. Correlations were calculated using Pearson's correlation. A p-value<0.05 was considered significant.
The 95% limits of agreement between the two observers were 1.9 sec for CRTchronometer and 1.7 sec for CRTvideo. The 95% limits of agreement between CRTchronometer and CRTvideo were 1.7 sec for observer 1 and 2.3 sec for observer 2. Measurements of CRTchronometer performed by the two observers were correlated with Tºperipheral. Measurements of CRTvideo performed by the two observers were correlated with Tºperipheral and perfusion index.
In healthy volunteers, measurements of capillary refill time performed by either different observers or different methods showed poor agreement. Nevertheless, capillary refill time still reflected peripheral perfusion as shown by its correlation with objective variables of peripheral perfusion.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):269-276
DOI 10.5935/0103-507X.20140038
Peripheral perfusion abnormalities are relevant manifestations of shock. Capillary refill time is commonly used for their evaluation. However, the reproducibility of capillary refill time measurements and their correlation with other variables of peripheral perfusion, have not been comprehensively evaluated. Our goal was to determine, in healthy volunteers, the agreement between different methods of capillary refill time quantification and different observers, as well as their correlation with other markers of peripheral perfusion.
We studied 63 healthy volunteers. Two observers measured capillary refill time by means of two methods, direct view (CRTchronometer) and video analysis (CRTvideo). We also measured perfusion index (PI) derived from pulse plethysmography and finger pad temperature (Tºperipheral). The agreement between observers and methods was assessed using the Bland and Altman method. Correlations were calculated using Pearson's correlation. A p-value<0.05 was considered significant.
The 95% limits of agreement between the two observers were 1.9 sec for CRTchronometer and 1.7 sec for CRTvideo. The 95% limits of agreement between CRTchronometer and CRTvideo were 1.7 sec for observer 1 and 2.3 sec for observer 2. Measurements of CRTchronometer performed by the two observers were correlated with Tºperipheral. Measurements of CRTvideo performed by the two observers were correlated with Tºperipheral and perfusion index.
In healthy volunteers, measurements of capillary refill time performed by either different observers or different methods showed poor agreement. Nevertheless, capillary refill time still reflected peripheral perfusion as shown by its correlation with objective variables of peripheral perfusion.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):277-286
DOI 10.5935/0103-507X.20140039
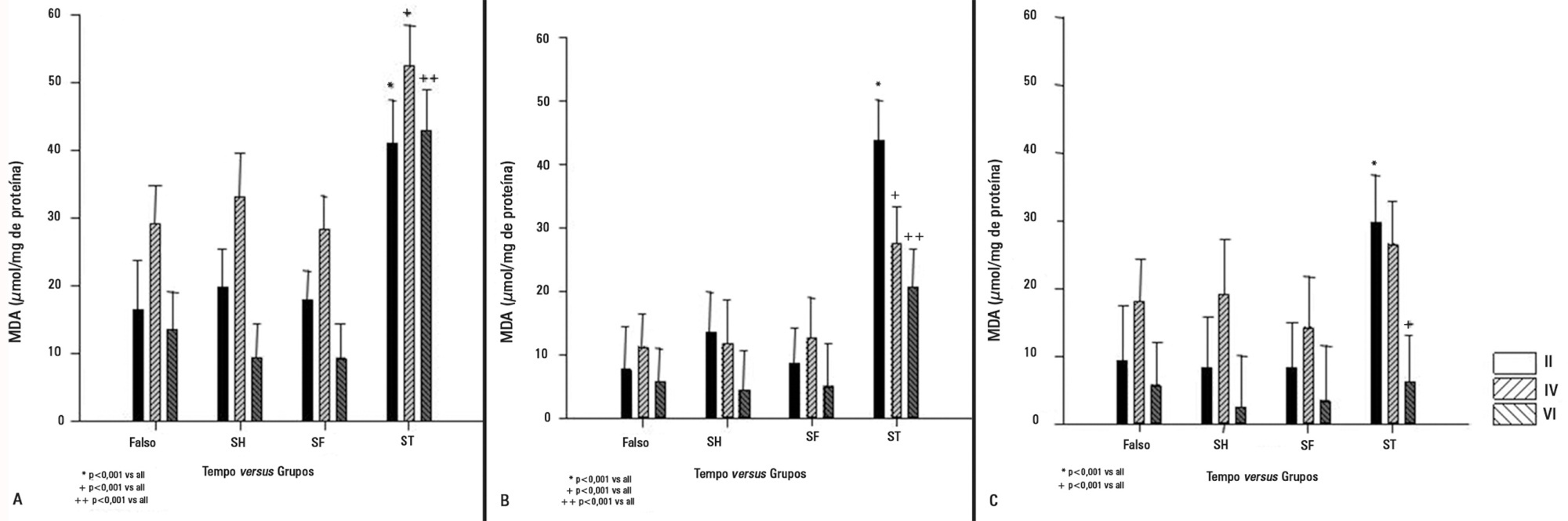
We investigated the effect of two different saline solutions on the mechanisms of injury after intestinal ischemia: oxidative stress and inflammatory responses.
Wistar rats underwent transient superior mesenteric artery occlusion and were studied for 6 hours after reperfusion. After randomization, the animals were divided into four groups: Sham; Hypertonic Saline, in which they received infusion of 4mL/kg body weight of 7.5% hypertonic saline; Saline, in which they received infusion of 33mL/kg body weight of 0.9% saline; and Non Treatment. The infusion was performed immediately prior to the reperfusion. The plasma concentrations of interleukin 6 and interleukin 10 were measured. Tissue samples (lung, liver, and intestine) were collected for malondialdehyde, myeloperoxidase, and interleukin measurements.
The animals that received infusions (Hypertonic Saline and Saline) showed lower levels of tissue malondialdehyde, myeloperoxidase, interleukin 6, and interleukin 10 compared with the Non Treatment group. The plasma concentrations of interleukin 6 and interleukin 10 were higher in the animals treated with 7.5% hypertonic saline compared with Saline and Non Treatment groups.
In this model of transient intestinal ischemia, the adequate maintenance of intravascular volume decreased oxidative stress and the synthesis of inflammatory markers. Both 7.5% Hypertonic Saline and Saline attenuated the deleterious effects observed after intestinal ischemia.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):277-286
DOI 10.5935/0103-507X.20140039
We investigated the effect of two different saline solutions on the mechanisms of injury after intestinal ischemia: oxidative stress and inflammatory responses.
Wistar rats underwent transient superior mesenteric artery occlusion and were studied for 6 hours after reperfusion. After randomization, the animals were divided into four groups: Sham; Hypertonic Saline, in which they received infusion of 4mL/kg body weight of 7.5% hypertonic saline; Saline, in which they received infusion of 33mL/kg body weight of 0.9% saline; and Non Treatment. The infusion was performed immediately prior to the reperfusion. The plasma concentrations of interleukin 6 and interleukin 10 were measured. Tissue samples (lung, liver, and intestine) were collected for malondialdehyde, myeloperoxidase, and interleukin measurements.
The animals that received infusions (Hypertonic Saline and Saline) showed lower levels of tissue malondialdehyde, myeloperoxidase, interleukin 6, and interleukin 10 compared with the Non Treatment group. The plasma concentrations of interleukin 6 and interleukin 10 were higher in the animals treated with 7.5% hypertonic saline compared with Saline and Non Treatment groups.
In this model of transient intestinal ischemia, the adequate maintenance of intravascular volume decreased oxidative stress and the synthesis of inflammatory markers. Both 7.5% Hypertonic Saline and Saline attenuated the deleterious effects observed after intestinal ischemia.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):287-291
DOI 10.5935/0103-507X.20140040
To develop experimental models of erythrocyte transfusion, the first step is to ensure the viability of the red blood cells transfused. In this pilot study, we assessed the viability of transfused red blood cells with validation in vitro and in vivo of homologous swine erythrocytes stored for 14 days.
Blood collected from one Agroceres® swine was stored in two red blood cell units. In vivo validation was performed by labeling the red blood cells with Na2 51CrO4 and recovering the viable erythrocytes after 24 hours of infusion in one autologous and four homologous animals. In vitro validation was performed at baseline and after 14 days in sixteen red blood cell units by measuring hemoglobin, hematocrit, hemolysis index and free hemoglobin. A post-mortem splenectomy was performed to evaluate the splenic sequestration of erythrocytes, and the radioactivity of the supernatant samples was counted to evaluate intravascular hemolysis.
After 14 days of storage, the red blood cell units had lower volumes and equivalent total concentrations of hemoglobin and hematocrit compared to human standards. The free hemoglobin concentration increased from 31.0±9.3 to 112.4±31.4mg/dL (p<0.001), and the hemolysis index increased from 0.1±0.1 to 0.5±0.1% (p<0.001). However, these tests were within the acceptable range for human standards. The percentage of radioactivity in supernatant samples was similar at baseline and after 24 hours, thus excluding significant hemolysis. No evidence of splenic sequestration of radioactive erythrocytes was found.
Swine red blood cells stored for 14 days are viable and can be used in experimental studies of transfusion. These validation experiments are important to aid investigators in establishing experimental models of transfusion.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):287-291
DOI 10.5935/0103-507X.20140040
To develop experimental models of erythrocyte transfusion, the first step is to ensure the viability of the red blood cells transfused. In this pilot study, we assessed the viability of transfused red blood cells with validation in vitro and in vivo of homologous swine erythrocytes stored for 14 days.
Blood collected from one Agroceres® swine was stored in two red blood cell units. In vivo validation was performed by labeling the red blood cells with Na2 51CrO4 and recovering the viable erythrocytes after 24 hours of infusion in one autologous and four homologous animals. In vitro validation was performed at baseline and after 14 days in sixteen red blood cell units by measuring hemoglobin, hematocrit, hemolysis index and free hemoglobin. A post-mortem splenectomy was performed to evaluate the splenic sequestration of erythrocytes, and the radioactivity of the supernatant samples was counted to evaluate intravascular hemolysis.
After 14 days of storage, the red blood cell units had lower volumes and equivalent total concentrations of hemoglobin and hematocrit compared to human standards. The free hemoglobin concentration increased from 31.0±9.3 to 112.4±31.4mg/dL (p<0.001), and the hemolysis index increased from 0.1±0.1 to 0.5±0.1% (p<0.001). However, these tests were within the acceptable range for human standards. The percentage of radioactivity in supernatant samples was similar at baseline and after 24 hours, thus excluding significant hemolysis. No evidence of splenic sequestration of radioactive erythrocytes was found.
Swine red blood cells stored for 14 days are viable and can be used in experimental studies of transfusion. These validation experiments are important to aid investigators in establishing experimental models of transfusion.

Abstract
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients' condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients' condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):299-304
DOI 10.5935/0103-507X.20140042
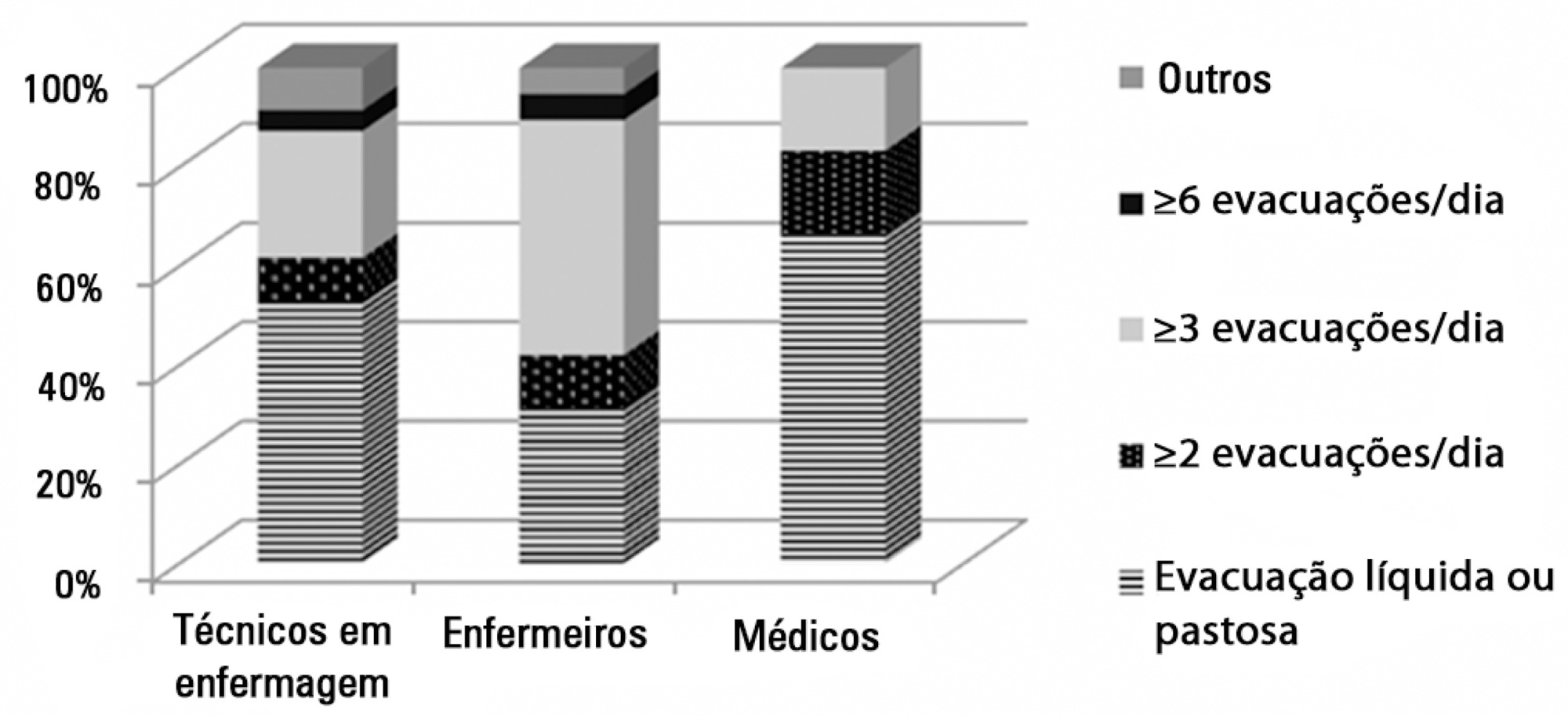
To assess the opinions and practices of intensive care professionals with regard to diarrhea in critically ill patients.
A multicenter cross-sectional study was conducted among health care professionals working at three adult intensive care units. Participants responded individually to a self-administered questionnaire about their length of work experience in intensive care; the definition, characterization, and causes of diarrhea; types of records in the patient's medical record; and training received.
A total of 78 professionals participated in this study, of whom 59.0% were nurse technicians, 25.7% were nurses, and 15.3% were physicians; 77.0% of them had worked in intensive care for over 1 year. Only 37.2% had received training on this topic. Half of the interviewees defined diarrhea as "liquid and/or pasty stools" regardless of frequency, while the other 50.0% defined diarrhea based on the increased number of daily bowel movements. The majority of them mentioned diet as the main cause of diarrhea, followed by "use of medications" (p<0.001). Distinct nutritional practices were observed among the analyzed professionals regarding episodes of diarrhea, such as discontinuing, maintaining, or reducing the volume of enteral nutrition; physicians reported that they do not routinely communicate the problem to other professionals (for example, to a nutritionist) and do not routinely record and quantify diarrhea events in patients' medical records.
Different opinions and practices were observed in intensive care professionals with regard to diarrhea.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):299-304
DOI 10.5935/0103-507X.20140042
To assess the opinions and practices of intensive care professionals with regard to diarrhea in critically ill patients.
A multicenter cross-sectional study was conducted among health care professionals working at three adult intensive care units. Participants responded individually to a self-administered questionnaire about their length of work experience in intensive care; the definition, characterization, and causes of diarrhea; types of records in the patient's medical record; and training received.
A total of 78 professionals participated in this study, of whom 59.0% were nurse technicians, 25.7% were nurses, and 15.3% were physicians; 77.0% of them had worked in intensive care for over 1 year. Only 37.2% had received training on this topic. Half of the interviewees defined diarrhea as "liquid and/or pasty stools" regardless of frequency, while the other 50.0% defined diarrhea based on the increased number of daily bowel movements. The majority of them mentioned diet as the main cause of diarrhea, followed by "use of medications" (p<0.001). Distinct nutritional practices were observed among the analyzed professionals regarding episodes of diarrhea, such as discontinuing, maintaining, or reducing the volume of enteral nutrition; physicians reported that they do not routinely communicate the problem to other professionals (for example, to a nutritionist) and do not routinely record and quantify diarrhea events in patients' medical records.
Different opinions and practices were observed in intensive care professionals with regard to diarrhea.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
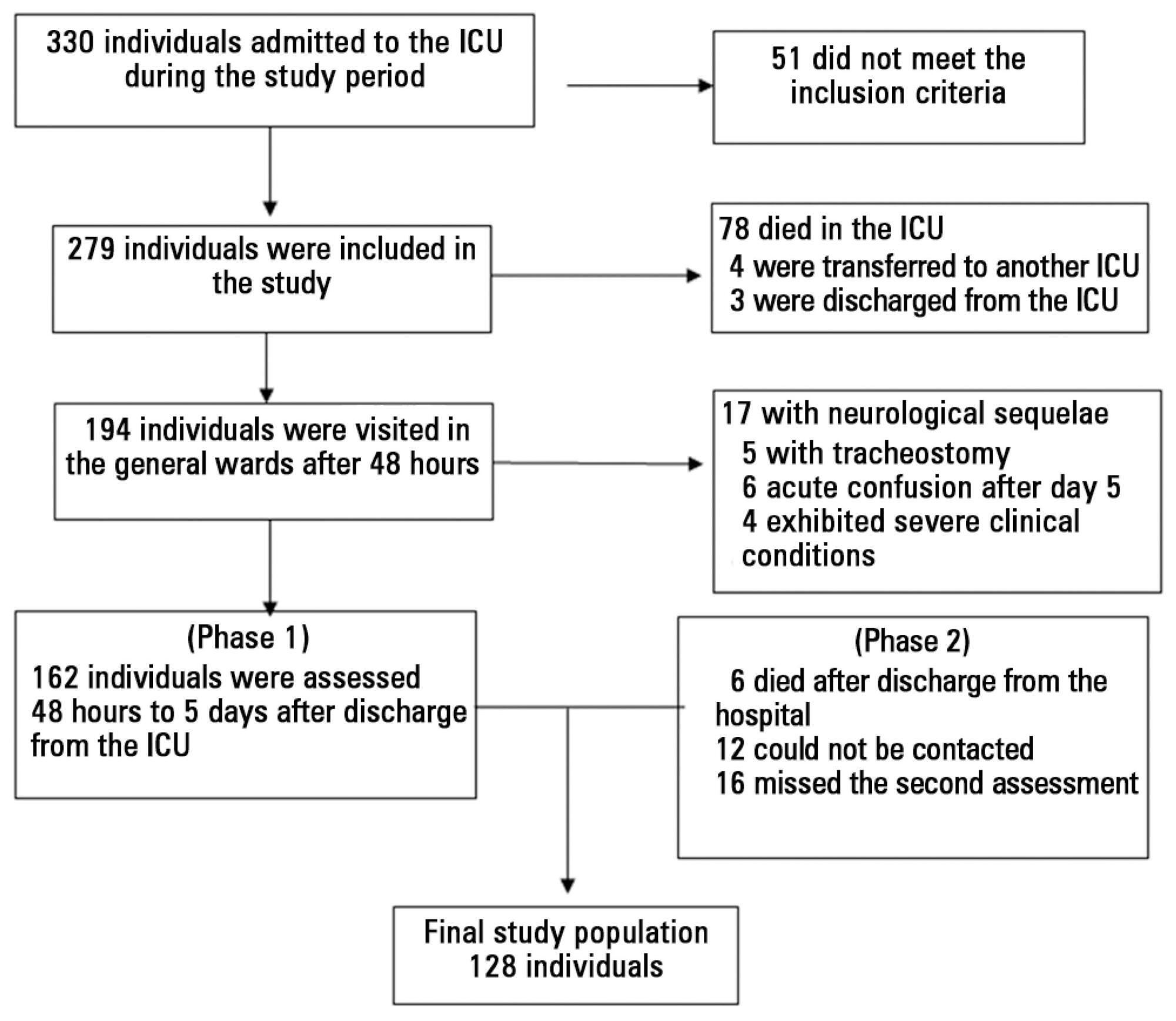
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants' clinical records; the data relative to the participants' memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):122-129
DOI 10.5935/0103-507X.20140018
To investigate the relationship between sedation and the memories reported by patients subjected to mechanical ventilation following discharge from the intensive care unit.
This prospective, observational, cohort study was conducted with individuals subjected to mechanical ventilation who remained in the intensive care unit for more than 24 hours. Clinical statistics and sedation records were extracted from the participants' clinical records; the data relative to the participants' memories were collected using a specific validated instrument. Assessment was performed three months after discharge from the intensive care unit.
A total of 128 individuals were assessed, most of whom (84.4%) reported recollections from their stay in the intensive care unit as predominantly a combination of real and illusory events. The participants subjected to sedation (67.2%) at deep levels (Richmond Agitation-Sedation Scale [RASS] -4 and -5) for more than two days and those with psychomotor agitation (33.6%) exhibited greater susceptibility to occurrence of illusory memories (p>0.001).
The probability of the occurrence of illusory memories was greater among the participants who were subjected to deep sedation. Sedation seems to be an additional factor that contributed to the occurrence of illusory memories in severely ill individuals subjected to mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
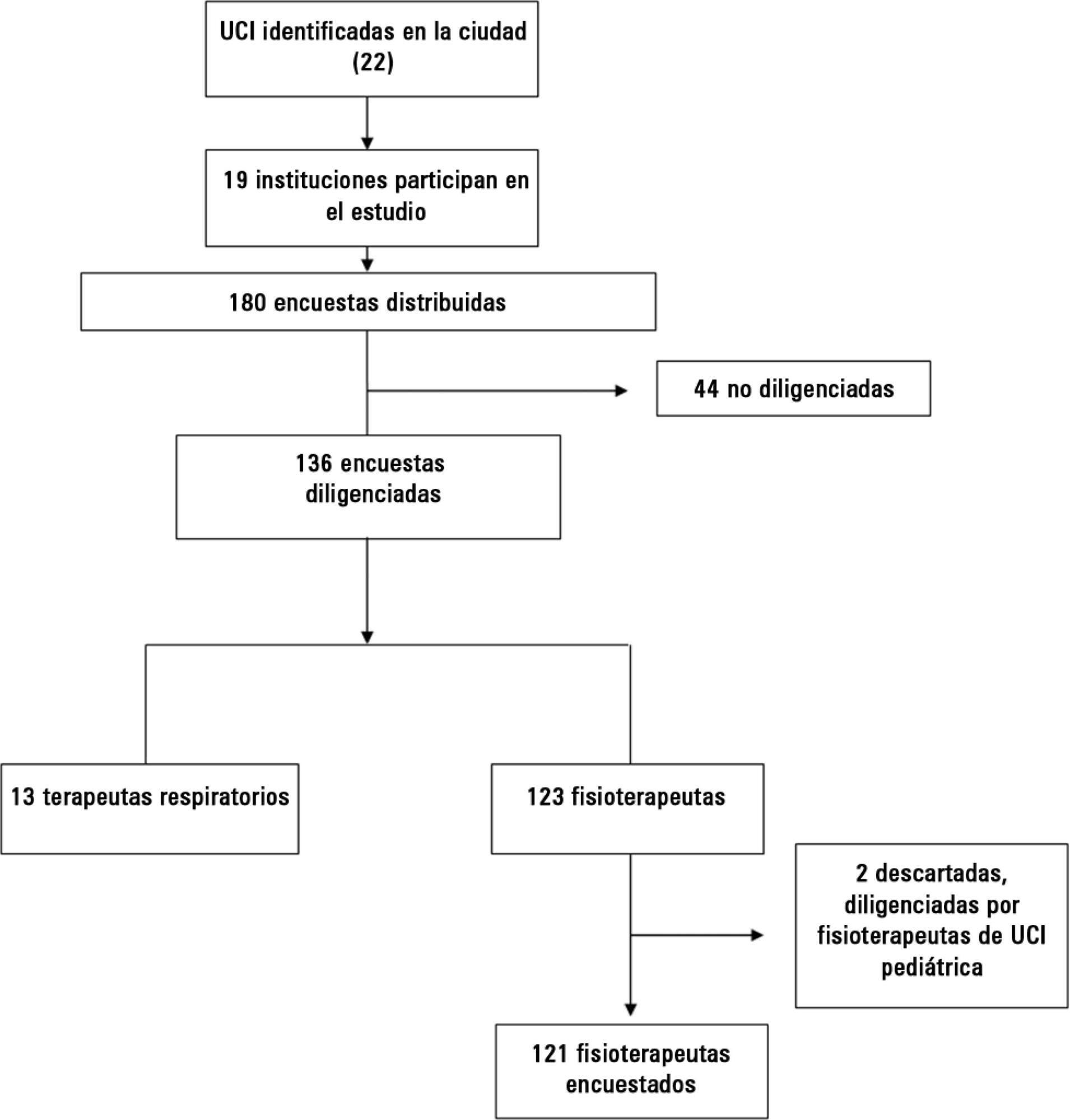
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):137-142
DOI 10.5935/0103-507X.20140020
Early weaning from mechanical ventilation is one of the primary goals in managing critically ill patients. There are various techniques and measurement parameters for such weaning. The objective of this study was to describe the practices of ventilatory weaning in adult intensive care units in the city of Cali.
A survey of 32 questions (some multiple choice) evaluating weaning practices was distributed to physiotherapists and respiratory therapists working in intensive care units, to be answered anonymously.
The most common strategy for the parameter set was the combination of continuous positive airway pressure with pressure support (78%), with a large variability in pressure levels, the most common range being 6 to 8cmH2O. The most common weaning parameters were as follows: tidal volume (92.6%), respiratory rate (93.3%) and oxygen saturation (90.4%). The most common waiting time for registration of the parameters was >15 minutes (40%). The measurements were preferably obtained from the ventilator display.
The methods and measurement parameters of ventilatory weaning vary greatly. The most commonly used method was continuous positive airway pressure with more pressure support and the most commonly used weaning parameters were the measured tidal volume and respiratory rate.
Search
Search in:
Case reports (56) Child (53) Coronavirus infections (34) COVID-19 (46) Critical care (116) Critical illness (54) Extracorporeal membrane oxygenation (26) Infant, newborn (27) Intensive care (72) Intensive care units (256) Intensive care units, pediatric (31) mechanical ventilation (38) Mortality (76) Physical therapy modalities (28) Prognosis (61) Respiration, artificial (119) Respiratory insufficiency (26) risk factors (34) SARS-CoV-2 (28) Sepsis (98)