Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
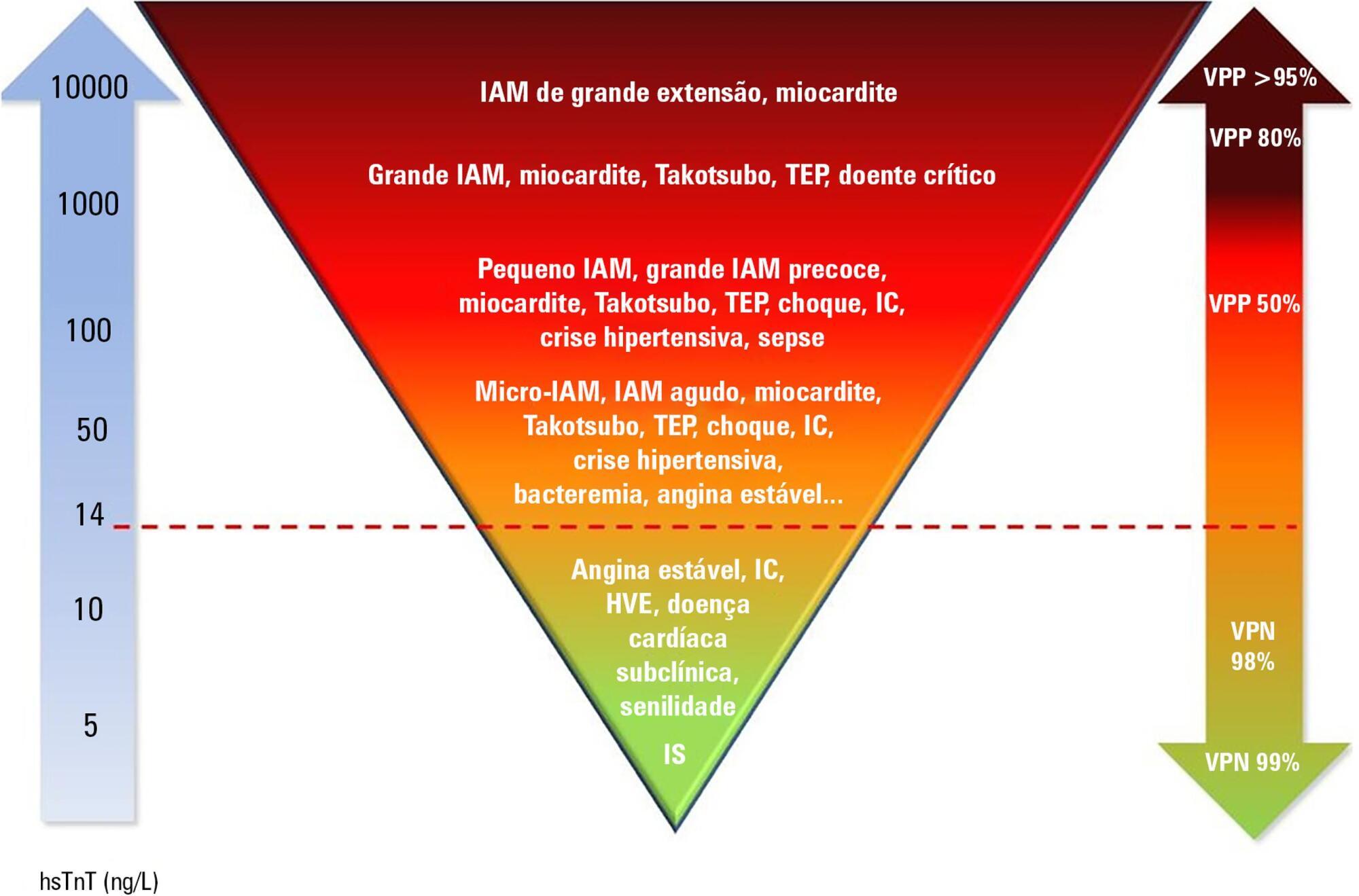
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):93-105
DOI 10.5935/0103-507X.20190001
Cardiac troponins T and I are considered highly sensitive and specific markers for the diagnosis of acute myocardial infarction. Currently, a series of nonprimary cardiac abnormalities may manifest as an elevation in high-sensitive assays. The reduction in their detection limits has allowed earlier diagnosis and the use of evidence-based therapeutic measures; however, this characteristic has increased the spectrum of detectable noncoronary heart diseases, which poses challenges for characterizing acute coronary syndromes and creates a new role for these tests in known disorders in intensive care units, especially sepsis. Management of patients through a greater understanding of how these markers behave should be re-evaluated to ensure their correct interpretation.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):5-14
DOI 10.5935/0103-507X.20190002
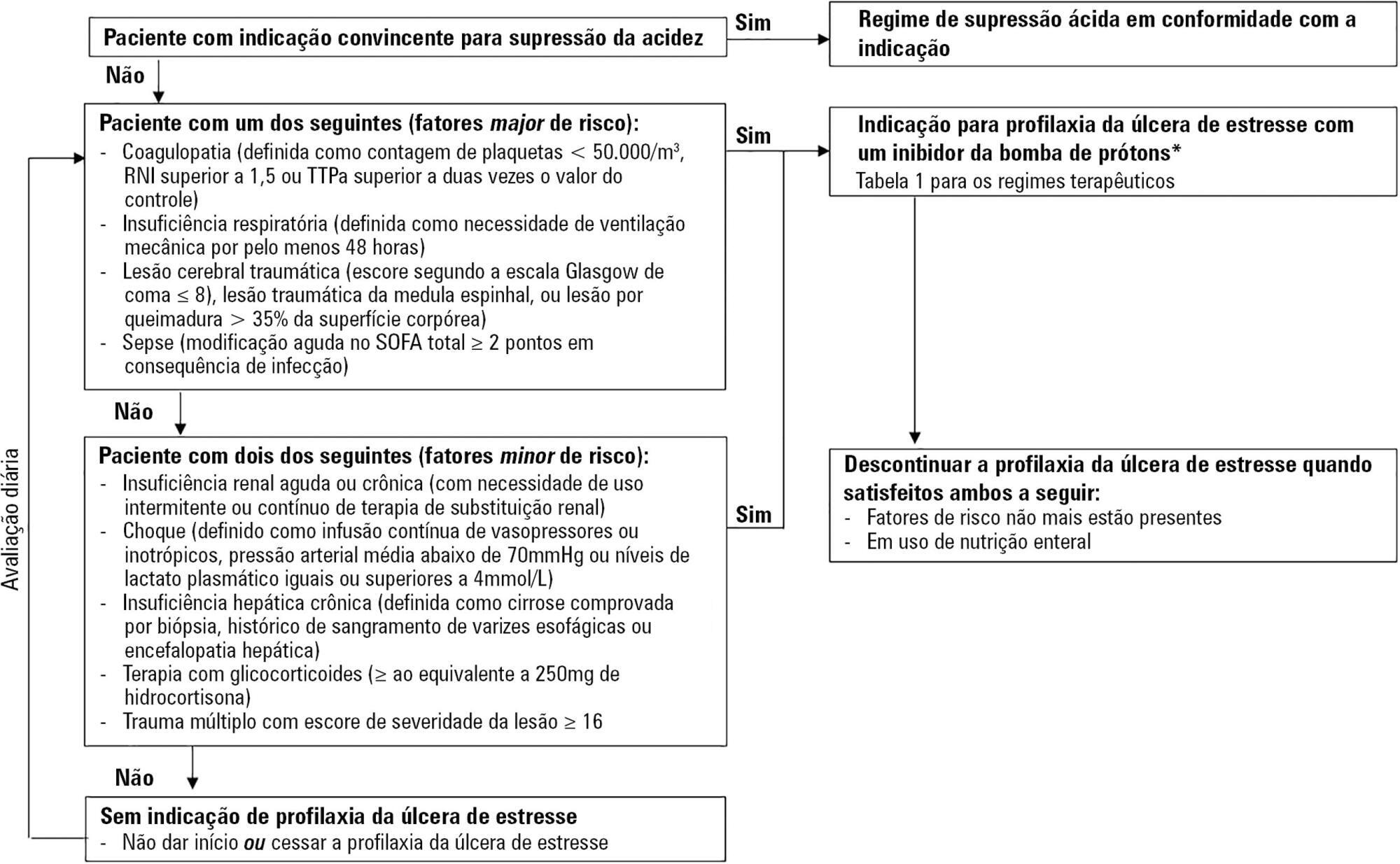
Critically ill patients are at risk of developing stress ulcers in the upper digestive tract. Agents that suppress gastric acid are commonly prescribed to reduce the incidence of clinically important stress ulcer-related gastrointestinal bleeding. However, the indiscriminate use of stress ulcer prophylaxis in all patients admitted to the intensive care unit is not warranted and can have potential adverse clinical effects and cost implications. The present guidelines from the Sociedade Portuguesa de Cuidados Intensivos summarizes the current evidence and gives six clinical statements and an algorithm aiming to provide a standardized prescribing policy for the use of stress ulcer prophylaxis in the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):5-14
DOI 10.5935/0103-507X.20190002
Critically ill patients are at risk of developing stress ulcers in the upper digestive tract. Agents that suppress gastric acid are commonly prescribed to reduce the incidence of clinically important stress ulcer-related gastrointestinal bleeding. However, the indiscriminate use of stress ulcer prophylaxis in all patients admitted to the intensive care unit is not warranted and can have potential adverse clinical effects and cost implications. The present guidelines from the Sociedade Portuguesa de Cuidados Intensivos summarizes the current evidence and gives six clinical statements and an algorithm aiming to provide a standardized prescribing policy for the use of stress ulcer prophylaxis in the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):327-332
DOI 10.5935/0103-507X.20180044
To evaluate the practice of dentistry in intensive care units.
An observational survey study was conducted in which questionnaires were sent via the online platform for collaboration in intensive care research in Brazil (AMIBnet). The study was carried out from June to October 2017. The questionnaires, which contained 26 closed questions about hospitals and dentistry practices in the intensive care units, were sent to 4,569 professionals from different specialties practicing in the units.
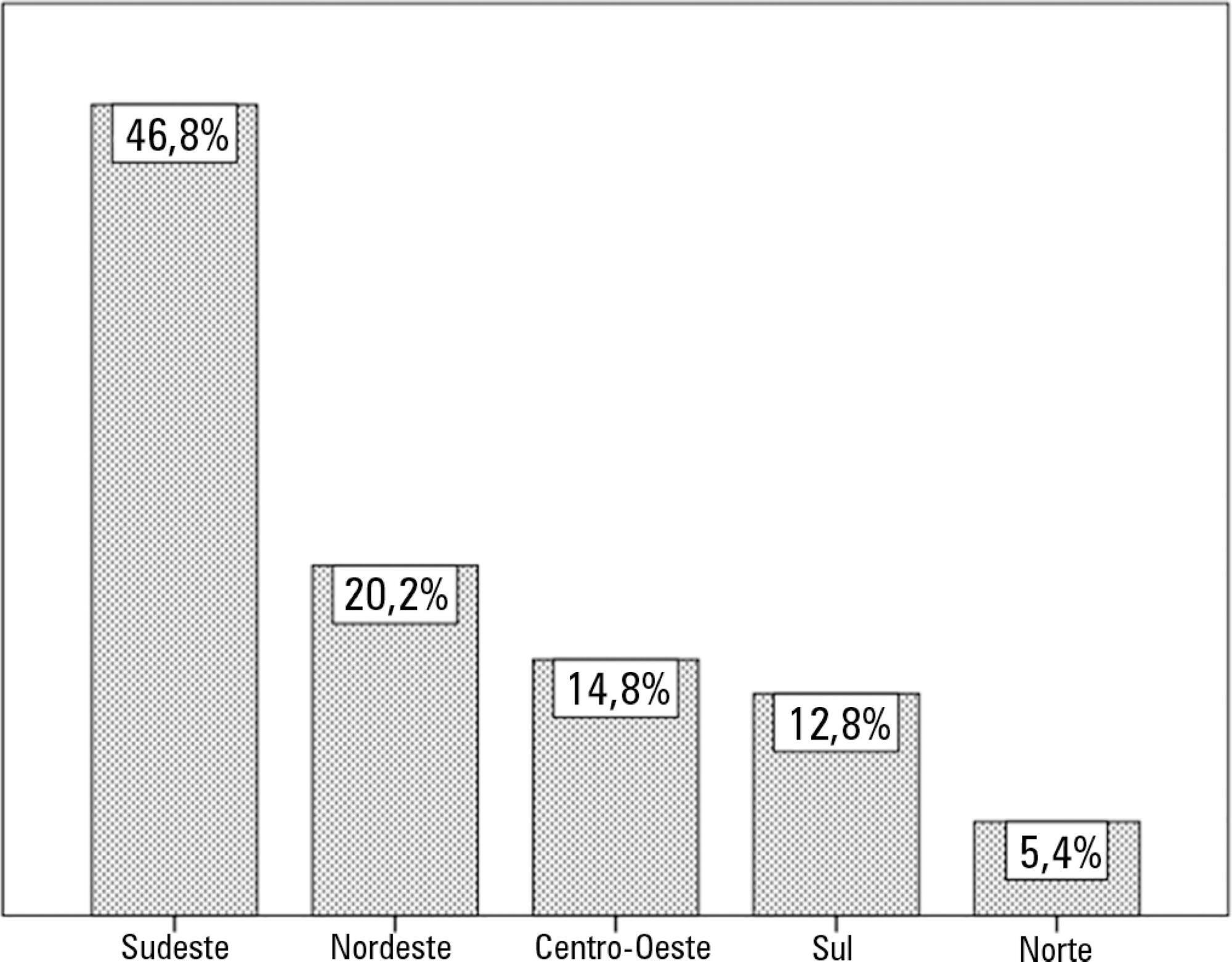
In total, 203 questionnaires were returned, resulting in a response rate of 4.44%. Most of the responses were from intensive care units in the Southeast region of the country (46.8%). Public hospitals (37.9%) and private hospitals (36.4%) had similar participation rates. Of the respondents, 55% indicated that a bedside dentistry service was present, and they were provided in different ways.
The presence of dentistry services and oral health service delivery training and protocols were correlated. The oral care methods varied greatly among the intensive care units surveyed.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):327-332
DOI 10.5935/0103-507X.20180044
To evaluate the practice of dentistry in intensive care units.
An observational survey study was conducted in which questionnaires were sent via the online platform for collaboration in intensive care research in Brazil (AMIBnet). The study was carried out from June to October 2017. The questionnaires, which contained 26 closed questions about hospitals and dentistry practices in the intensive care units, were sent to 4,569 professionals from different specialties practicing in the units.
In total, 203 questionnaires were returned, resulting in a response rate of 4.44%. Most of the responses were from intensive care units in the Southeast region of the country (46.8%). Public hospitals (37.9%) and private hospitals (36.4%) had similar participation rates. Of the respondents, 55% indicated that a bedside dentistry service was present, and they were provided in different ways.
The presence of dentistry services and oral health service delivery training and protocols were correlated. The oral care methods varied greatly among the intensive care units surveyed.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
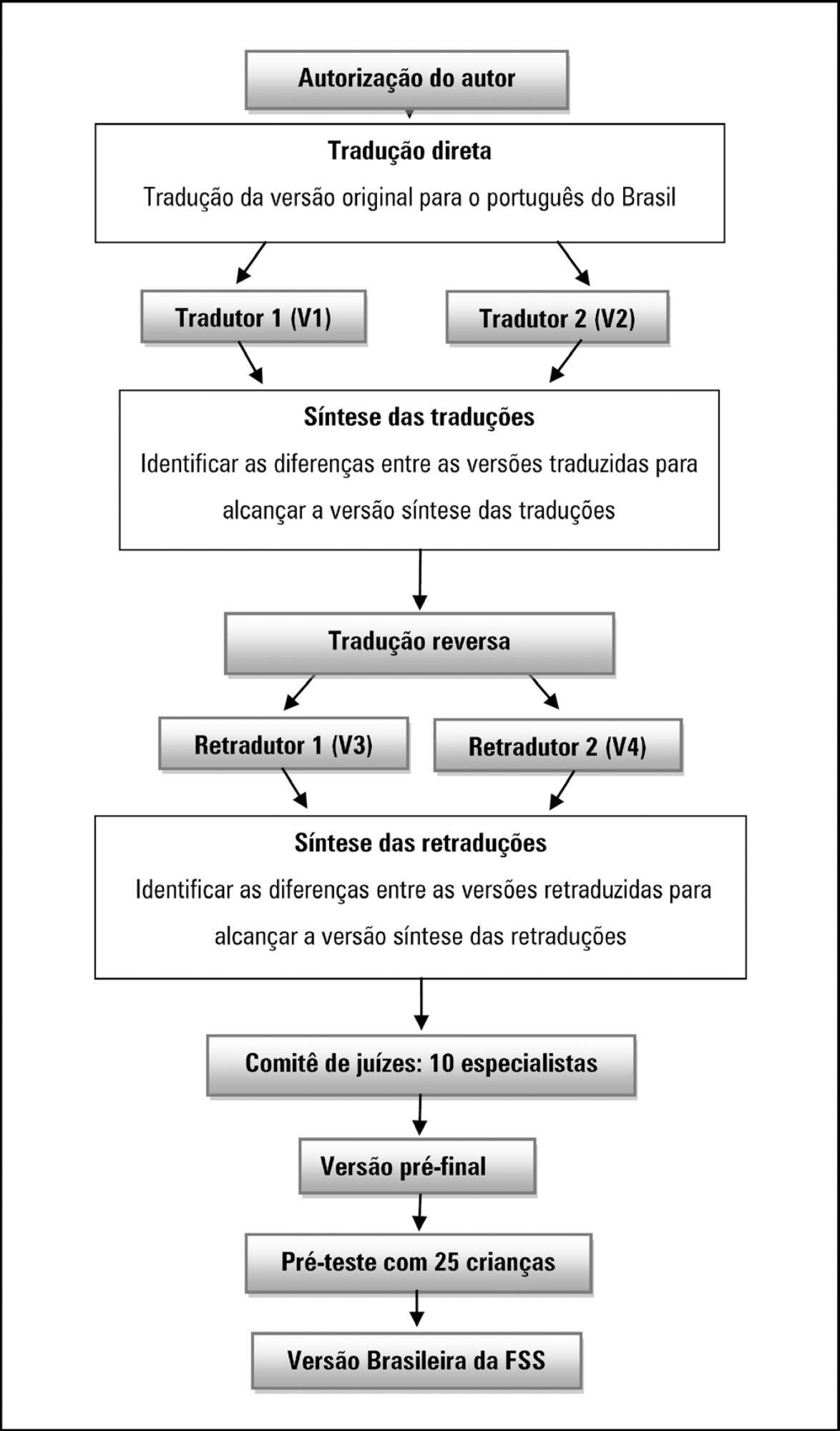
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 - 0.95).
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):301-307
DOI 10.5935/0103-507X.20180043
To translate and cross-culturally adapt the Functional Status Scale for hospitalized children into Brazilian Portuguese.
A methodological study of the translation and cross-cultural adaptation of the Functional Status Scale was conducted, according to the stages of translation, synthesis of translations, back-translation, synthesis of back-translations, expert committee analysis and pre-test with a sample of the target population. During the evaluation by the committee of experts, semantic, content and item analyses were performed.
The semantic, idiomatic, cultural and conceptual equivalences between the translated version and the original version were obtained, resulting in the Brazilian version of the Functional Status Scale. After the analysis by the expert committee, there were no problems regarding the cultural or conceptual equivalences because the items were pertinent to the Brazilian culture and few terms were modified. In the pre-test stage, the scale was applied by two evaluators to a sample of 25 children. Clarity and ease in answering the scale items were observed. Good inter-observer reliability was obtained, with an intraclass correlation coefficient of 0.85 (0.59 - 0.95).
The Functional Status Scale for pediatric use was translated and culturally adapted into Portuguese spoken in Brazil. The translated items were pertinent to the Brazilian culture and evaluated the dimensions proposed by the original instrument. Validation studies of this instrument are suggested to make it feasible for use in different regions of Brazil.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):308-316
DOI 10.5935/0103-507X.20180042
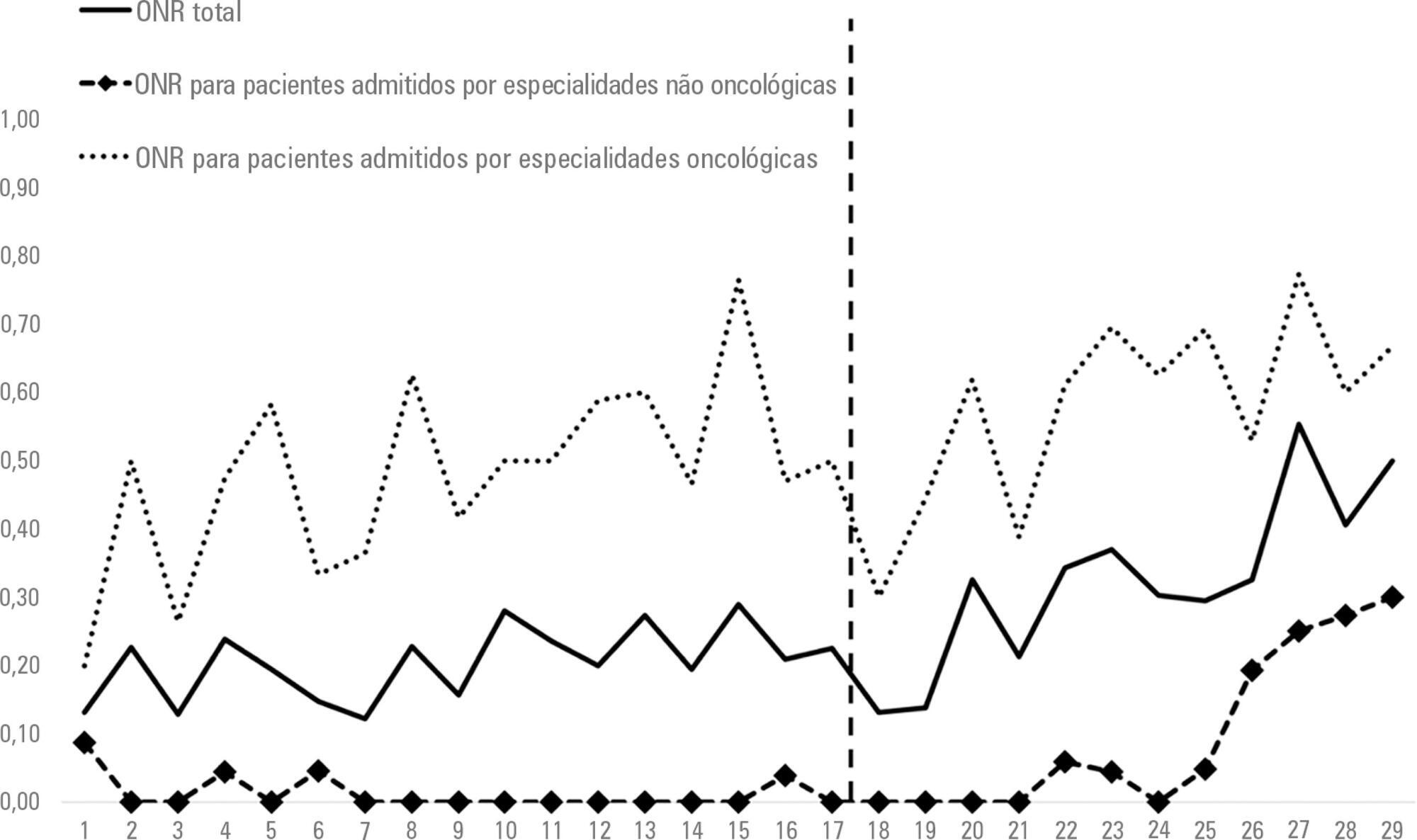
To assess the effect of the implementation of a palliative care program on do-not-resuscitate orders and intensive care unit utilization during terminal hospitalizations.
Data were retrospectively collected for all patients who died in a tertiary hospital in Brazil from May 2014 to September 2016. We analyzed the frequency of do-not-resuscitate orders and intensive care unit admissions among in-hospital deaths. Interrupted time series analyses were used to evaluate differences in trends of do-not-resuscitate orders and intensive care unit admissions before (17 months) and after (12 months) the implementation of a palliative care program.
We analyzed 48,372 hospital admissions and 1,071 in-hospital deaths. Deaths were preceded by do-not-resuscitate orders in 276 (25.8%) cases and admissions to the intensive care unit occurred in 814 (76%) cases. Do-not-resuscitate orders increased from 125 (20.4%) to 151 (33%) cases in the pre-implementation and post-implementation periods, respectively (p < 0.001). Intensive care unit admissions occurred in 469 (76.5%) and 345 (75.3%) cases in the pre-implementation and post-implementation periods, respectively (p = 0.654). Interrupted time series analyses confirmed a trend of increased do-not-resuscitate order registrations, from an increase of 0.5% per month pre-implementation to an increase of 2.9% per month post-implementation (p < 0.001), and demonstrated a trend of decreased intensive care unit utilization, from an increase of 0.6% per month pre-implementation to a decrease of -0.9% per month in the post-implementation period (p = 0.001).
The implementation of a palliative care program was associated with a trend of increased registration of do-not-resuscitate orders and a trend of decreased intensive care unit utilization during terminal hospitalizations.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):308-316
DOI 10.5935/0103-507X.20180042
To assess the effect of the implementation of a palliative care program on do-not-resuscitate orders and intensive care unit utilization during terminal hospitalizations.
Data were retrospectively collected for all patients who died in a tertiary hospital in Brazil from May 2014 to September 2016. We analyzed the frequency of do-not-resuscitate orders and intensive care unit admissions among in-hospital deaths. Interrupted time series analyses were used to evaluate differences in trends of do-not-resuscitate orders and intensive care unit admissions before (17 months) and after (12 months) the implementation of a palliative care program.
We analyzed 48,372 hospital admissions and 1,071 in-hospital deaths. Deaths were preceded by do-not-resuscitate orders in 276 (25.8%) cases and admissions to the intensive care unit occurred in 814 (76%) cases. Do-not-resuscitate orders increased from 125 (20.4%) to 151 (33%) cases in the pre-implementation and post-implementation periods, respectively (p < 0.001). Intensive care unit admissions occurred in 469 (76.5%) and 345 (75.3%) cases in the pre-implementation and post-implementation periods, respectively (p = 0.654). Interrupted time series analyses confirmed a trend of increased do-not-resuscitate order registrations, from an increase of 0.5% per month pre-implementation to an increase of 2.9% per month post-implementation (p < 0.001), and demonstrated a trend of decreased intensive care unit utilization, from an increase of 0.6% per month pre-implementation to a decrease of -0.9% per month in the post-implementation period (p = 0.001).
The implementation of a palliative care program was associated with a trend of increased registration of do-not-resuscitate orders and a trend of decreased intensive care unit utilization during terminal hospitalizations.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
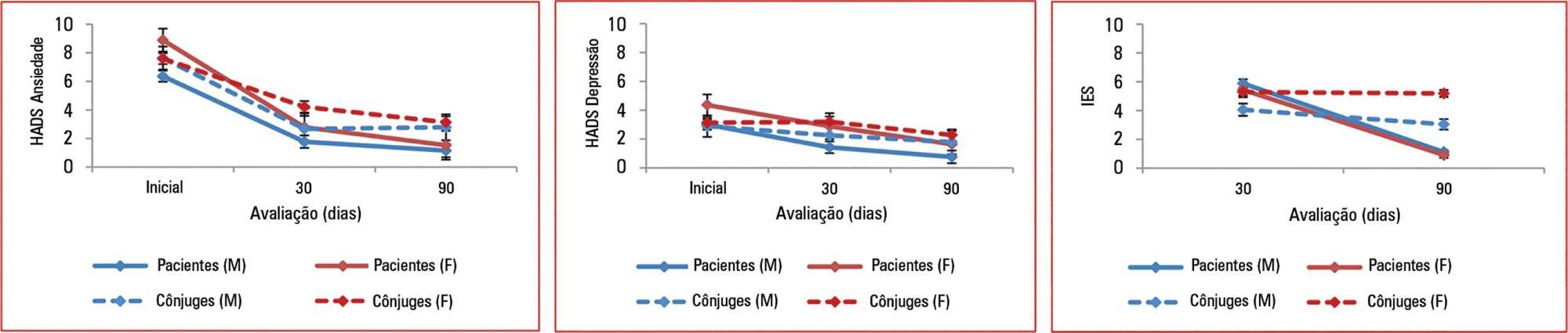
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale - subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):35-41
DOI 10.5935/0103-507X.20180004
To assess the effect of sex and spouse condition on symptoms of anxiety, depression and posttraumatic stress symptoms in patients and their spouses.
A prospective study conducted in a 22-bed adult mixed intensive care unit in a tertiary hospital in São Paulo, Brazil. Patients and their spouses were enrolled 2 days after intensive care unit admission. They were interviewed while in the intensive care unit using the Hospital Anxiety and Depression Scale. At 30 and 90 days after intensive care unit discharge, they completed the Impact of Event Scale and Hospital Anxiety and Depression Scale by phone.
From March 2011 to March 2013, we analyzed 118 patients and their spouses. We observed that female sex was associated with higher scores than male sex was in terms of the anxiety Hospital Anxiety and Depression Scale - subscale (p = 0.032) and depression (p = 0.034). There was no association between sex and posttraumatic stress disorder symptoms. However, spouses had higher Impact of Event Scale points compared with patients (p = 0.001).
Female sex was associated with anxiety and depression, and spouses were more vulnerable to post-traumatic stress symptoms than the patients were. Increasing age and a later time of assessment were also associated with lower scores on the Impact of Event Scale.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
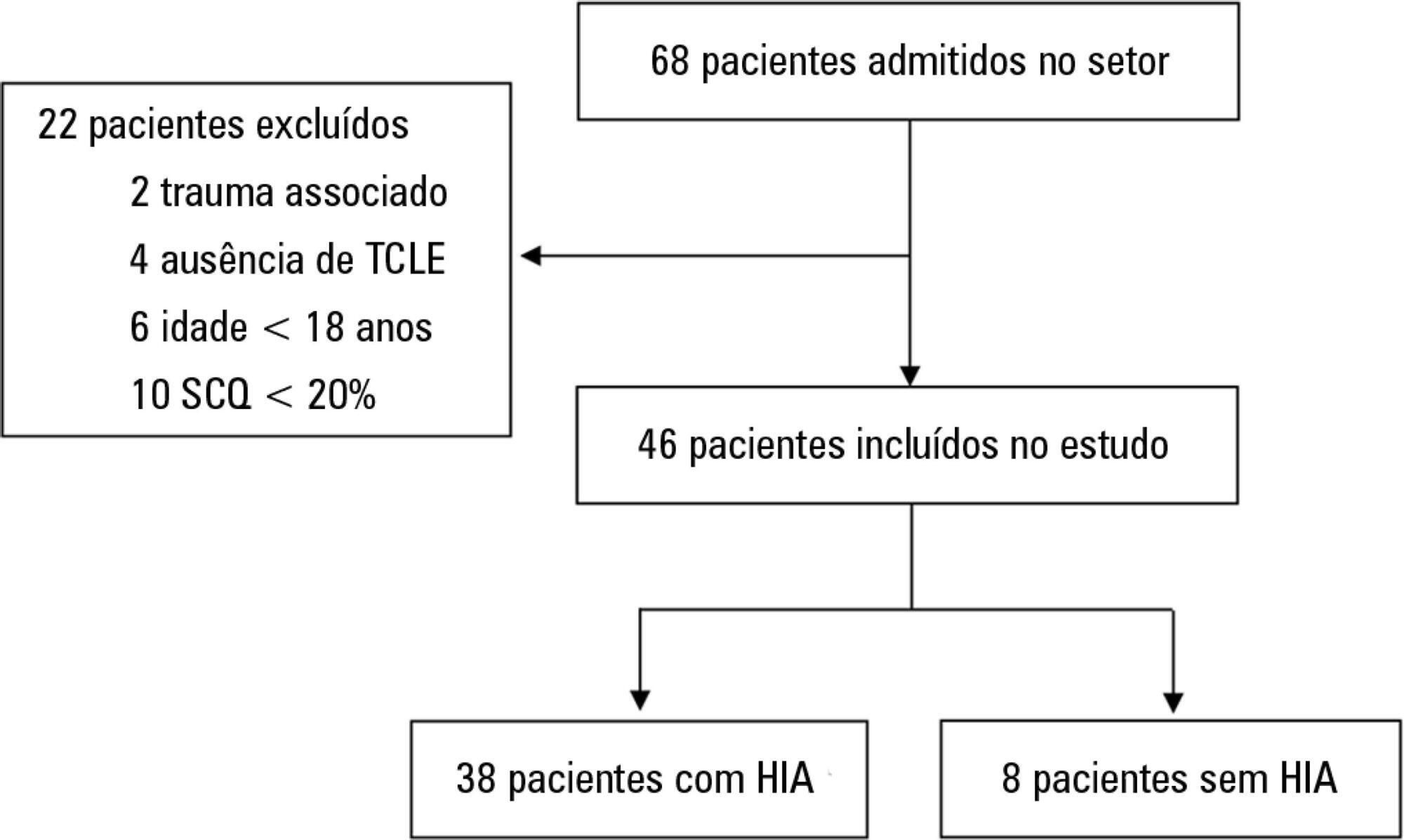
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):15-20
DOI 10.5935/0103-507X.20180001
To evaluate the frequency of intra-abdominal hypertension in major burn patients and its association with the occurrence of acute kidney injury.
This was a prospective cohort study of a population of burn patients hospitalized in a specialized intensive care unit. A convenience sample was taken of adult patients hospitalized in the period from 1 August 2015 to 31 October 2016. Clinical and burn data were collected, and serial intra-abdominal pressure measurements taken. The significance level used was 5%.
A total of 46 patients were analyzed. Of these, 38 patients developed intra-abdominal hypertension (82.6%). The median increase in intra-abdominal pressure was 15.0mmHg (interquartile range: 12.0 to 19.0). Thirty-two patients (69.9%) developed acute kidney injury. The median time to development of acute kidney injury was 3 days (interquartile range: 1 - 7). The individual analysis of risk factors for acute kidney injury indicated an association with intra-abdominal hypertension (p = 0.041), use of glycopeptides (p = 0.001), use of vasopressors (p = 0.001) and use of mechanical ventilation (p = 0.006). Acute kidney injury was demonstrated to have an association with increased 30-day mortality (log-rank, p = 0.009).
Intra-abdominal hypertension occurred in most patients, predominantly in grades I and II. The identified risk factors for the occurrence of acute kidney injury were intra-abdominal hypertension and use of glycopeptides, vasopressors and mechanical ventilation. Acute kidney injury was associated with increased 30-day mortality.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
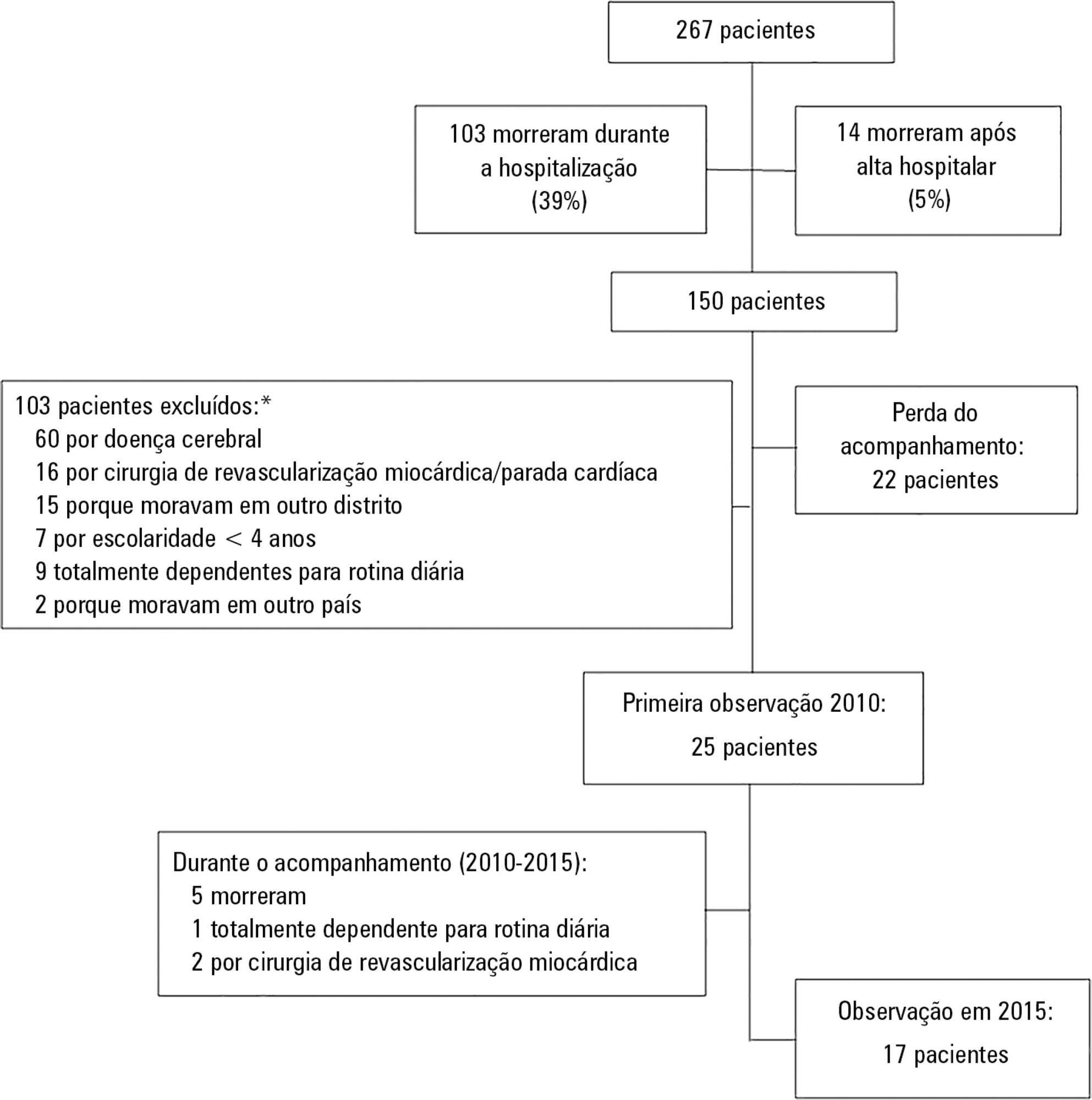
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):28-34
DOI 10.5935/0103-507X.20180008
To investigate the longterm psychological outcome in survivors of critical illness after intensive care unit discharge.
A prospective cohort of survivors admitted to a mixed intensive care unit between January and September 2010 was evaluated six months and five years after hospital discharge. The Dementia Rating Scale-2, the Hospital Anxiety and Depression Scale, the Posttraumatic stress syndrome 14-questions inventory, the Euro Quality of Life 5 Dimensions (EQ-5-D), and the Visual Analogue Scale (EQ VAS) were assessed at both follow-up periods.
Of 267 patients, 25 patients were evaluated at 6 months after discharge (62 ± 16 years); 12 (48%) presented cognitive impairment, 6 (24%) anxiety, 4 (16%) depression, and 4 (16%) post-traumatic stress disorder. Among those re-evaluated five years after discharge (n = 17; 65 ± 15 years), the frequency of cognitive impairment dropped from 8 (47%) to 3 (18%) (p = 0.063), due to improvement in these patients over time, and other patients did not acquire any dysfunction after discharge. At five years after discharge, only two patients (12%) reported anxiety, and none had depression or post-traumatic stress disorder. No differences were found between the six-month and five-year follow-ups regarding EQ-5-D and EQ VAS.
Survivors do not show a progressive decline in cognitive function or quality of life within five years after intensive care unit discharge. Psychopathological symptoms tend to decrease with time.