Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Jorge Ibrain Figueira Salluh"
We found (31) results for your search.Abstract
Rev Bras Ter Intensiva. 2010;22(1):53-63
DOI 10.1590/S0103-507X2010000100010
OBJECTIVE: Nutritional therapy is an important element in critical ill patient care. Although recognized as specialty, multidisciplinary teams in nutrition support are scarce in our country. Possibly, nutrition support therapy is applied by intensive care physicians and this may vary. The aim of the study is describe these specialists perceptions about theirs attitudes in enteral nutrition support. METHODS: A questionnaire was elaborated in an on-line platform. After pre-validation, it was sent by electronic mail to intensivists. In 30 days answers were collected, considering only the full-filled questionnaires. RESULTS: One hundred an fourteen forms were returned, 112 were analyzed. The responders were localized at majority in southeastern region. About beggining of nutritional support, the majority of answers reflect perceptions in accord to specialists societies recommendations. The responders' perception the frequent utilization of assistentials protocols in nutrition care. After support beginning, the responders perceptions about theirs participation in changes in therapeutic plan seems to be lower. The self-knowledge about the theme among the responders was 6.0 (arithmetic media) in a 1 to 10 scale. CONCLUSIONS: More studies are necessary to evaluate nutritional support practices among intensive care physicians. Alternatives to on-line platform should be considered. Possibly, intensive care physicians do better in the initial phases of enteral support than in continuity of care. Intensive care physicians knowledge about the issue is suboptimal.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):53-63
DOI 10.1590/S0103-507X2010000100010
OBJECTIVE: Nutritional therapy is an important element in critical ill patient care. Although recognized as specialty, multidisciplinary teams in nutrition support are scarce in our country. Possibly, nutrition support therapy is applied by intensive care physicians and this may vary. The aim of the study is describe these specialists perceptions about theirs attitudes in enteral nutrition support. METHODS: A questionnaire was elaborated in an on-line platform. After pre-validation, it was sent by electronic mail to intensivists. In 30 days answers were collected, considering only the full-filled questionnaires. RESULTS: One hundred an fourteen forms were returned, 112 were analyzed. The responders were localized at majority in southeastern region. About beggining of nutritional support, the majority of answers reflect perceptions in accord to specialists societies recommendations. The responders' perception the frequent utilization of assistentials protocols in nutrition care. After support beginning, the responders perceptions about theirs participation in changes in therapeutic plan seems to be lower. The self-knowledge about the theme among the responders was 6.0 (arithmetic media) in a 1 to 10 scale. CONCLUSIONS: More studies are necessary to evaluate nutritional support practices among intensive care physicians. Alternatives to on-line platform should be considered. Possibly, intensive care physicians do better in the initial phases of enteral support than in continuity of care. Intensive care physicians knowledge about the issue is suboptimal.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):541-547
DOI 10.5935/0103-507X.20190079
Ventilator-associated lower respiratory tract infection is one of the most frequent complications in mechanically ventilated patients. Ventilator-associated tracheobronchitis has been considered a disease that does not warrant antibiotic treatment by the medical community for many years. In the last decade, several studies have shown that tracheobronchitis could be considered an intermediate process that leads to ventilator-associated pneumonia. Furthermore, ventilator-associated tracheobronchitis has a limited impact on overall mortality but shows a significant association with increased patient costs, length of stay, antibiotic use, and duration of mechanical ventilation. Although we still need clear evidence, especially concerning treatment modalities, the present study on ventilator-associated tracheobronchitis highlights that there are important impacts of including this condition in clinical management and epidemiological and infection surveillance.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
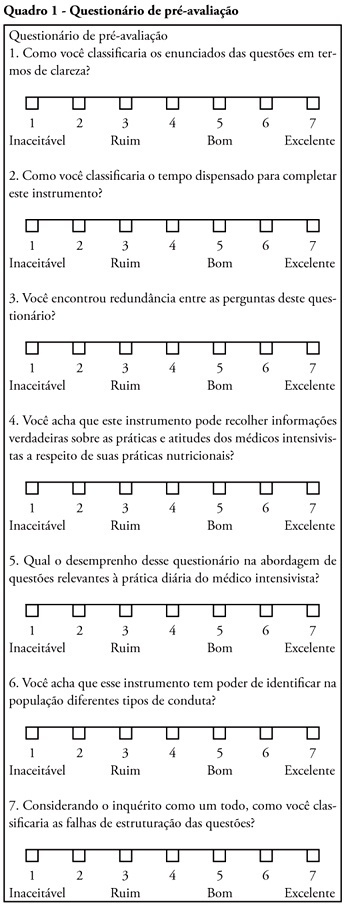
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
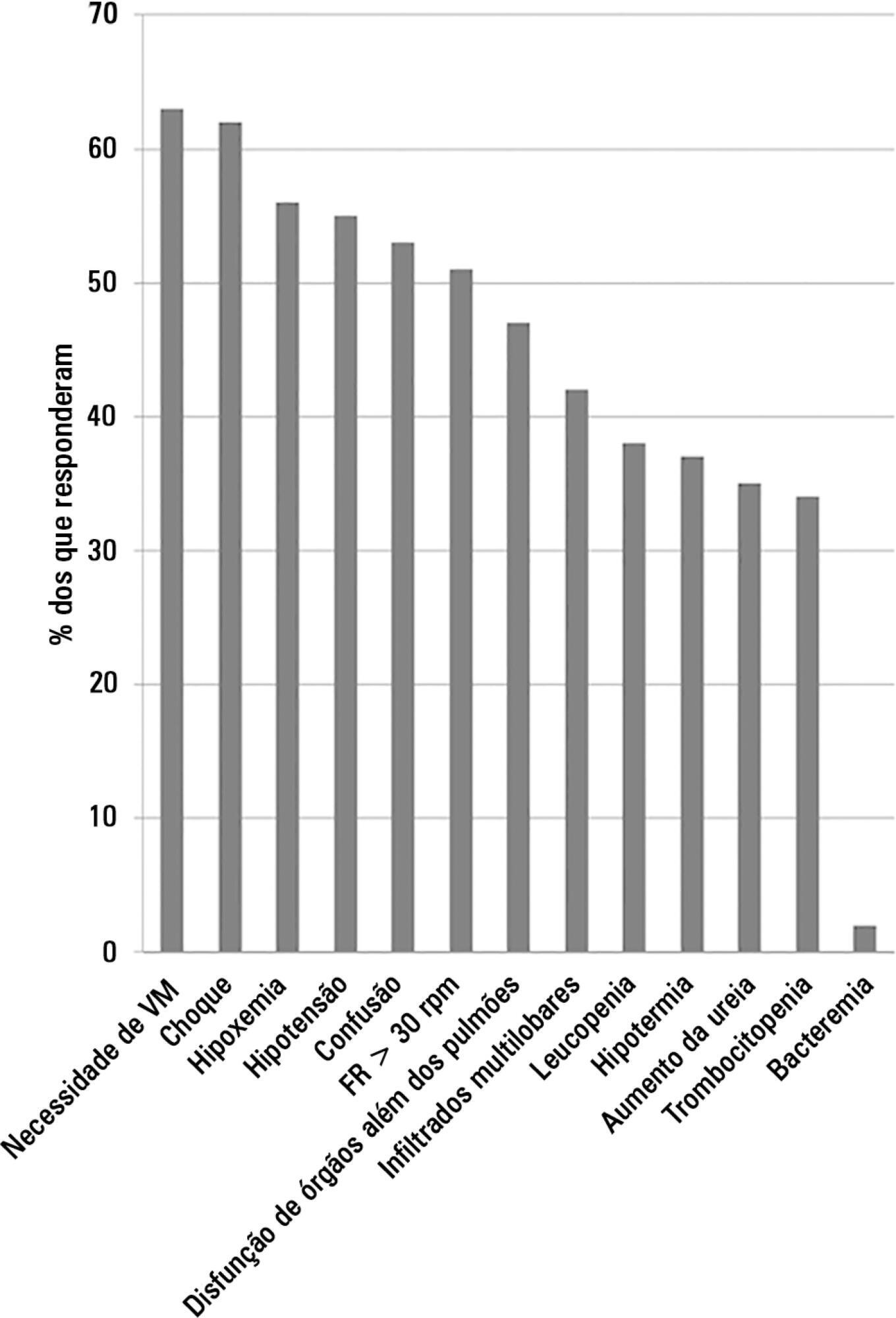
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
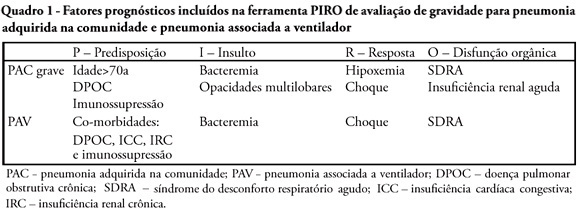
A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Abstract
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Abstract
Rev Bras Ter Intensiva. 2006;18(1):7-8
Abstract
Rev Bras Ter Intensiva. 2006;18(1):7-8
Abstract
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
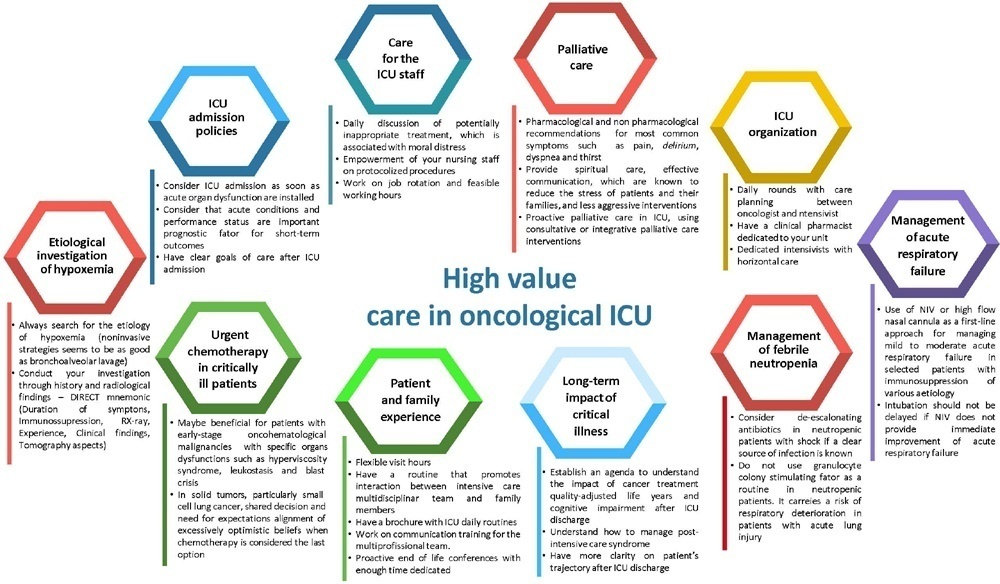
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Crit Care Sci. 2023;35(1):84-96
DOI 10.5935/2965-2774.20230405-pt
The number of patients with cancer requiring intensive care unit admission is increasing around the world. The improvement in the pathophysiological understanding of this group of patients, as well as the increasingly better and more targeted treatment options for their underlying disease, has led to a significant increase in their survival over the past three decades. Within the organizational concepts, it is necessary to know what adds value in the care of critical oncohematological patients. Practices in medicine that do not benefit patients and possibly cause harm are called low-value practices, while high-value practices are defined as high-quality care at relatively low cost. In this article, we discuss ten domains with high-value evidence in the care of cancer patients: (1) intensive care unit admission policies; (2) intensive care unit organization; (3) etiological investigation of hypoxemia; (4) management of acute respiratory failure; (5) management of febrile neutropenia; (6) urgent chemotherapy treatment in critically ill patients; (7) patient and family experience; (8) palliative care; (9) care of intensive care unit staff; and (10) long-term impact of critical disease on the cancer population. The disclosure of such policies is expected to have the potential to change health care standards. We understand that it is a lengthy process, and initiatives such as this paper are one of the first steps in raising awareness and beginning a discussion about high-value care in various health scenarios.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
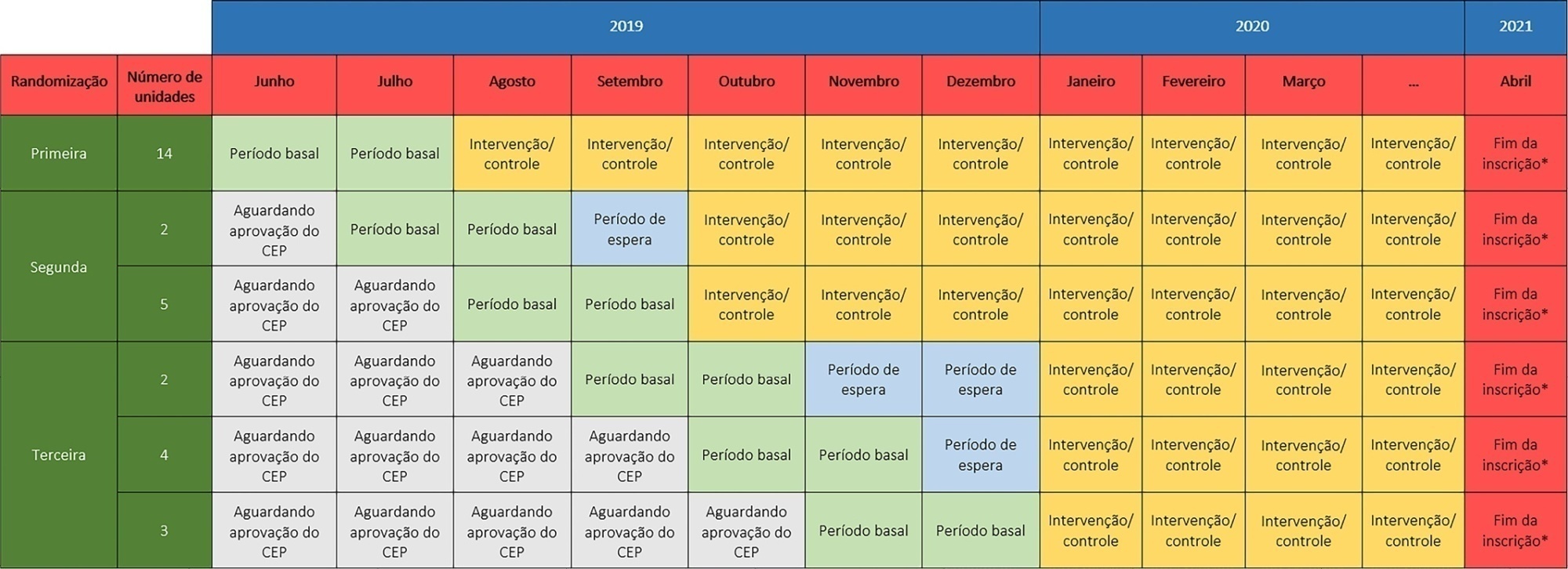
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):87-95
DOI 10.5935/0103-507x.20220003-en
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to assess whether a complex telemedicine intervention in intensive care units, which focuses on daily multidisciplinary rounds performed by remote intensivists, will reduce intensive care unit length of stay compared to usual care.
The TELESCOPE trial is a national, multicenter, controlled, open label, cluster randomized trial. The study tests the effectiveness of daily multidisciplinary rounds conducted by an intensivist through telemedicine in Brazilian intensive care units. The protocol was approved by the local Research Ethics Committee of the coordinating study center and by the local Research Ethics Committee from each of the 30 intensive care units, following Brazilian legislation. The trial is registered with ClinicalTrials. gov (NCT03920501). The primary outcome is intensive care unit length of stay, which will be analyzed accounting for the baseline period and cluster structure of the data and adjusted by prespecified covariates. Secondary exploratory outcomes included intensive care unit performance classification, in-hospital mortality, incidence of nosocomial infections, ventilator-free days at 28 days, rate of patients receiving oral or enteral feeding, rate of patients under light sedation or alert and calm, and rate of patients under normoxemia.
According to the trial’s best practice, we report our statistical analysis prior to locking the database and beginning analyses. We anticipate that this reporting practice will prevent analysis bias and improve the interpretation of the reported results.