-
Commentary
Early mobilization in the time of COVID-19
Rev Bras Ter Intensiva. 2020;32(4):484-486
Abstract
CommentaryEarly mobilization in the time of COVID-19
Rev Bras Ter Intensiva. 2020;32(4):484-486
DOI 10.5935/0103-507X.20200086
Views0INTRODUCTION It is essential to consider the deleterious secondary effects of coronavirus 2019 (COVID-19) disease and its consequences, especially in patients who develop the most severe forms. The survival of acute critical illness in the intensive care unit (ICU) may not reflect the patient’s quality of life after hospitalization.() A study with survivors of acute […]See moreViews0

Abstract
CommentaryEarly mobilization in the time of COVID-19
Rev Bras Ter Intensiva. 2020;32(4):484-486
DOI 10.5935/0103-507X.20200086
Views0INTRODUCTIONIt is essential to consider the deleterious secondary effects of coronavirus 2019 (COVID-19) disease and its consequences, especially in patients who develop the most severe forms. The survival of acute critical illness in the intensive care unit (ICU) may not reflect the patient’s quality of life after hospitalization.()A study with survivors of acute respiratory distress […]See more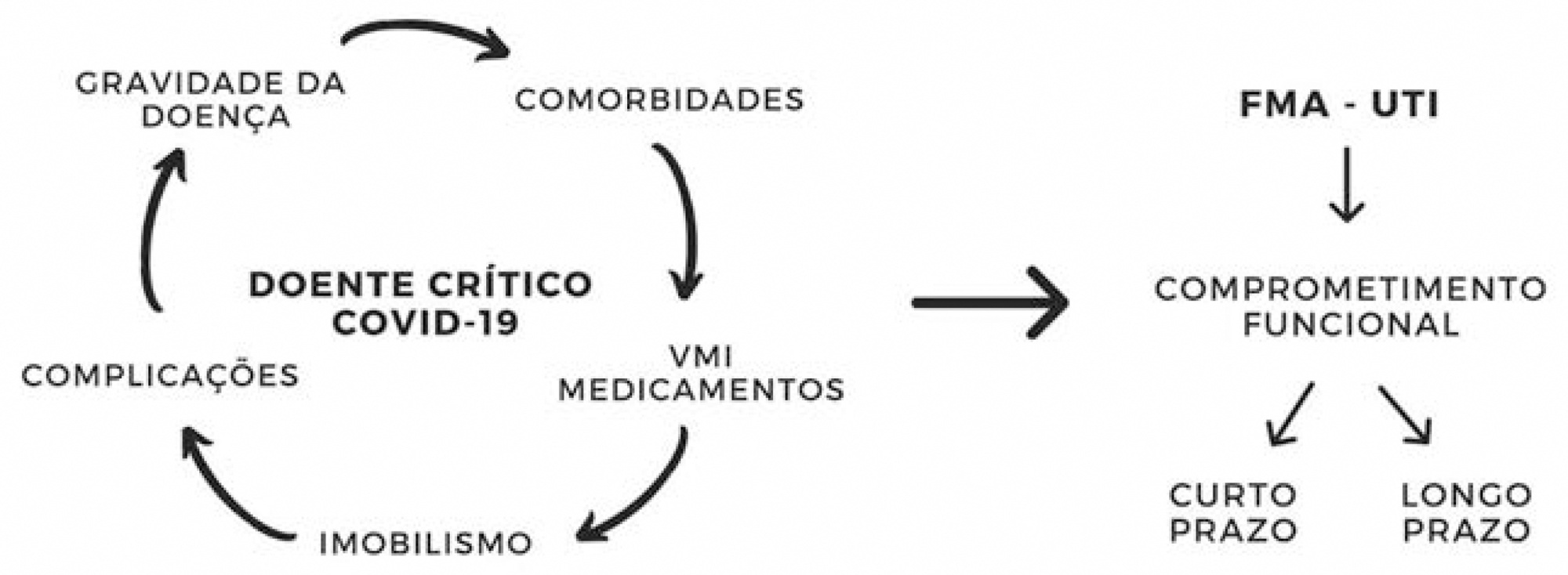
-
Original Article
Clinical characteristics and predictors of mechanical ventilation in patients with COVID-19 hospitalized in Southern Brazil
- Gisele Alsina Nader Bastos,
- Aline Zimmermann de Azambuja,
- Carisi Anne Polanczyk,
- Débora Dalmas Gräf,
- Isabelle Weschenfelder Zorzo, [ … ],
- Marcelo Comerlato Scotta

Abstract
Original ArticleClinical characteristics and predictors of mechanical ventilation in patients with COVID-19 hospitalized in Southern Brazil
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
- Gisele Alsina Nader Bastos,
- Aline Zimmermann de Azambuja,
- Carisi Anne Polanczyk,
- Débora Dalmas Gräf,
- Isabelle Weschenfelder Zorzo,
- Juçara Gasparetto Maccari,
- Lúcia Schnor Haygert,
- Luiz Antônio Nasi,
- Marcelo Basso Gazzana,
- Marina Bessel,
- Paulo Márcio Pitrez,
- Roselaine Pinheiro de Oliveira,
- Marcelo Comerlato Scotta
Views1Abstract
Objective:
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
Methods:
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Results:
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 – 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 – 55.6 p = 0.02).
Conclusion:
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Keywords:cohort studiesCoronavirus infectionsCOVID-19PandemicsRespiration, artificialrisk factorsSARS-CoV-2See moreViews1Abstract
Original ArticleClinical characteristics and predictors of mechanical ventilation in patients with COVID-19 hospitalized in Southern Brazil
Rev Bras Ter Intensiva. 2020;32(4):487-492
DOI 10.5935/0103-507X.20200082
- Gisele Alsina Nader Bastos,
- Aline Zimmermann de Azambuja,
- Carisi Anne Polanczyk,
- Débora Dalmas Gräf,
- Isabelle Weschenfelder Zorzo,
- Juçara Gasparetto Maccari,
- Lúcia Schnor Haygert,
- Luiz Antônio Nasi,
- Marcelo Basso Gazzana,
- Marina Bessel,
- Paulo Márcio Pitrez,
- Roselaine Pinheiro de Oliveira,
- Marcelo Comerlato Scotta
Views1Abstract
Objective:
This study aims to describe the clinical characteristics and predictors of mechanical ventilation of adult inpatients with COVID-19 in a single center.
Methods:
A retrospective cohort study was performed and included adult inpatients hospitalized from March 17th to May 3rd, 2020, who were diagnosed with SARS-CoV-2 infection. Clinical and demographic characteristics were extracted from electronic medical records.
Results:
Overall, 88 consecutive patients were included in this study. The median age of the patients was 63 years (IQR 49 – 71); 59 (67%) were male, 65 (86%) had a college degree and 67 (76%) had at least one comorbidity. Twenty-nine (33%) patients were admitted to the intensive care unit, 18 (20%) patients needed mechanical ventilation, and 9 (10.2%) died during hospitalization. The median length of stay in the intensive care unit and the median duration of mechanical ventilation was 23 and 29.5 days, respectively. An age ≥ 65 years was an independent risk factor for mechanical ventilation (OR 8.4 95%CI 1.3 – 55.6 p = 0.02).
Conclusion:
Our findings describe the first wave of Brazilian patients hospitalized for COVID-19. Age was the strongest predictor of respiratory insufficiency and the need for mechanical ventilation in our population.
Keywords:cohort studiesCoronavirus infectionsCOVID-19PandemicsRespiration, artificialrisk factorsSARS-CoV-2See more -
Original Article
Statistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo, [ … ],
- Fernando Godinho Zampieri
Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
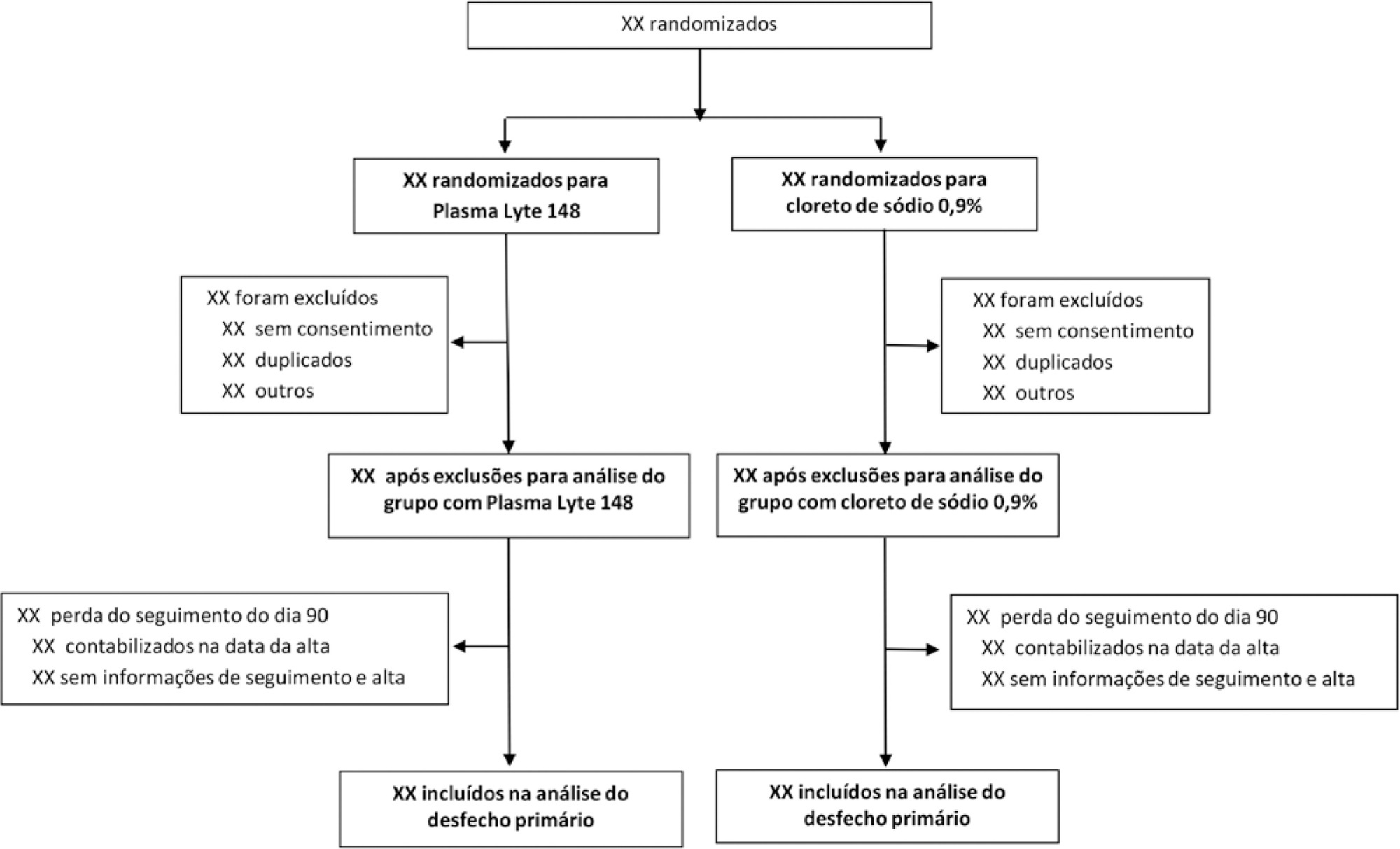
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
Views1Abstract
Original ArticleStatistical analysis plan for the Balanced Solution versus Saline in Intensive Care Study (BaSICS)
Rev Bras Ter Intensiva. 2020;32(4):493-505
DOI 10.5935/0103-507X.20200081
- Lucas Petri Damiani,
- Alexandre Biasi Cavalcanti ,
- Rodrigo Santos Biondi ,
- Flávio Geraldo Rezende de Freitas ,
- Rodrigo Cruvinel Figueiredo,
- Wilson José Lovato,
- Cristina Prata Amêndola,
- Ary Serpa Neto ,
- Jorge Luiz da Rocha Paranhos,
- Viviane Cordeiro Veiga ,
- Marco Antonio Vieira Guedes,
- Eraldo de Azevedo Lúcio,
- Lúcio Couto Oliveira Júnior,
- Thiago Costa Lisboa,
- Fabio Holanda Lacerda ,
- Tamiris Abait Miranda,
- Israel Silva Maia ,
- Cintia Magalhães Carvalho Grion ,
- Flavia Ribeiro Machado,
- Fernando Godinho Zampieri
Views1See moreAbstract
Objective:
To report the statistical analysis plan (first version) for the Balanced Solutions versus Saline in Intensive Care Study (BaSICS).
Methods:
BaSICS is a multicenter factorial randomized controlled trial that will assess the effects of Plasma-Lyte 148 versus 0.9% saline as the fluid of choice in critically ill patients, as well as the effects of a slow (333mL/h) versus rapid (999mL/h) infusion speed during fluid challenges, on important patient outcomes. The fluid type will be blinded for investigators, patients and the analyses. No blinding will be possible for the infusion speed for the investigators, but all analyses will be kept blinded during the analysis procedure.
Results:
BaSICS will have 90-day mortality as its primary endpoint, which will be tested using mixed-effects Cox proportional hazard models, considering sites as a random variable (frailty models) adjusted for age, organ dysfunction and admission type. Important secondary endpoints include renal replacement therapy up to 90 days, acute renal failure, organ dysfunction at days 3 and 7, and mechanical ventilation-free days within 28 days.
Conclusion:
This manuscript provides details on the first version of the statistical analysis plan for the BaSICS trial and will guide the study’s analysis when follow-up is finished.
-
Original Article
Value of the urea/creatinine index in isolated urine to estimate severe protein hypercatabolism in ventilated patients
- Dino Moretti ,
- Melisa D. Ré,
- Nicolás Sebastián Rocchetti ,
- Daniel H. Bagilet,
- Claudio Jesús Settecase, [ … ],
- Marta B. Quaglino
Abstract
Original ArticleValue of the urea/creatinine index in isolated urine to estimate severe protein hypercatabolism in ventilated patients
Rev Bras Ter Intensiva. 2020;32(4):506-513
DOI 10.5935/0103-507X.20200087
- Dino Moretti ,
- Melisa D. Ré,
- Nicolás Sebastián Rocchetti ,
- Daniel H. Bagilet,
- Claudio Jesús Settecase,
- Martin G. Buncuga,
- Marta B. Quaglino
Views0See moreABSTRACT
Objective:
To study the ability of the urea/creatinine index to identify severe protein catabolism from the isolated urine of critically ventilated patients.
Methods:
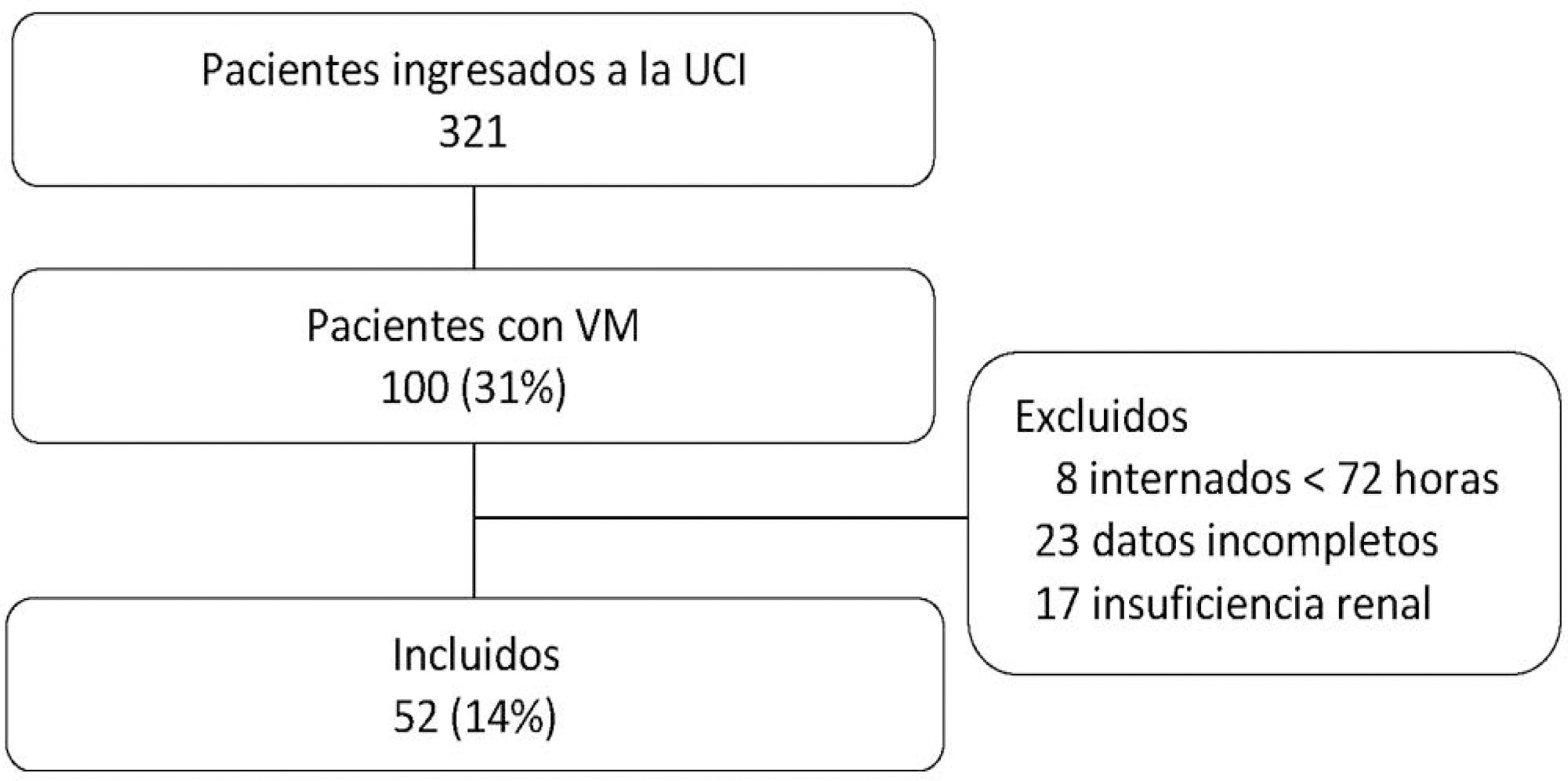
This was a prospective, observational study. It included 52 patients without kidney failure. Variables: total urinary nitrogen estimated from the urea in 24-hour urine on the second (T1) and fourth days (T2) and urea/creatinine index in isolated urine before 24-hour urine collection.
Results:
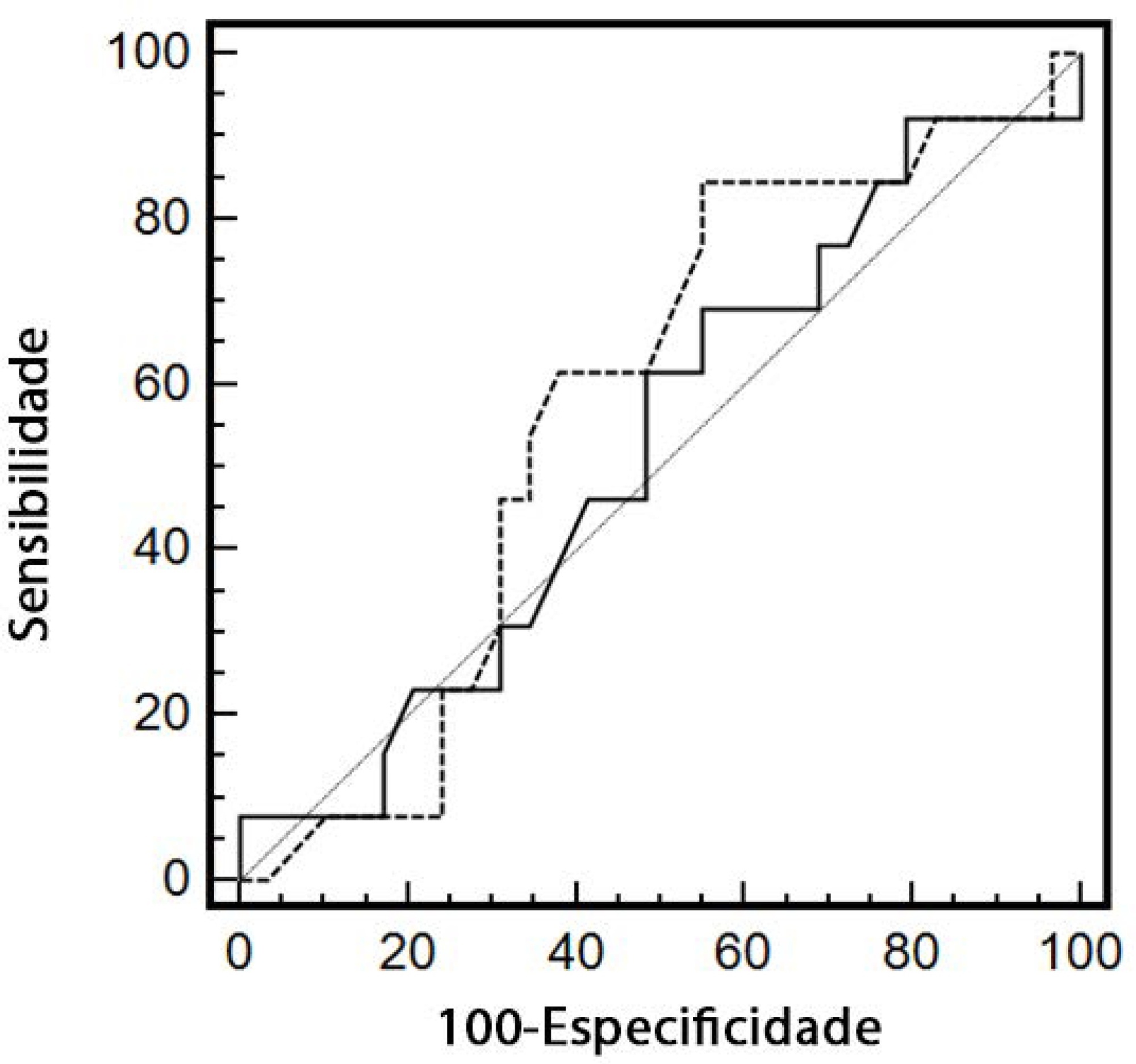
Severe protein hypercatabolism (estimated total urinary nitrogen > 15g) was present in 14 patients (26.9%) at T1 and in 29 (55.7%) at T2. Eighty-four percent of patients had low nutritional risk by the Nutrition Risk in the Critically Ill score. At T1, the Pearson correlation between the estimated total urinary nitrogen and the urea/creatinine index was 0.272 (p = 0.051), and at T2 it was 0.276 (p = 0.048). The urea/creatinine index at T2 had a tendency to better discriminate severe protein hypercatabolism than Acute Physiology and Chronic Health Evaluation II and Nutrition Risk in the Critically Ill (AUC 0.741 versus 0.669 and 0.656, 95%CI: 0.602 – 0.880; 0.519 – 0.818 and 0.506 – 0.806, respectively). The optimal cutoff value of the urea/creatinine index for the diagnosis of severe protein hypercatabolism was 16.15, with a sensitivity of 79.31% (95%CI: 59.74 – 91.29), specificity of 60.87% (95%CI: 38.78 – 79.53), positive predictive value 71.88% (95%CI: 53.02 – 85.60), negative predictive value 70.0% (95%CI: 45.67 – 87.18), LR (+) 2.03 (95%CI: 1.18 – 3.49), and LR (-) 0.34 (95%CI: 0.16 – 0.74).
Conclusion:
The urea/creatinine index measured on the fourth day has a certain ability to estimate severe protein hypercatabolism (as defined by estimated total urinary nitrogen) but does not replace total urinary nitrogen in critically ventilated patients without kidney failure. Due to its reasonable sensitivity, it could be used as a screen to identify which patients to take a 24-hour urine sample from.
Views0Abstract
Original ArticleValue of the urea/creatinine index in isolated urine to estimate severe protein hypercatabolism in ventilated patients
Rev Bras Ter Intensiva. 2020;32(4):506-513
DOI 10.5935/0103-507X.20200087
- Dino Moretti ,
- Melisa D. Ré,
- Nicolás Sebastián Rocchetti ,
- Daniel H. Bagilet,
- Claudio Jesús Settecase,
- Martin G. Buncuga,
- Marta B. Quaglino
Views0See moreABSTRACT
Objective:
To study the ability of the urea/creatinine index to identify severe protein catabolism from the isolated urine of critically ventilated patients.
Methods:
This was a prospective, observational study. It included 52 patients without kidney failure. Variables: total urinary nitrogen estimated from the urea in 24-hour urine on the second (T1) and fourth days (T2) and urea/creatinine index in isolated urine before 24-hour urine collection.
Results:
Severe protein hypercatabolism (estimated total urinary nitrogen > 15g) was present in 14 patients (26.9%) at T1 and in 29 (55.7%) at T2. Eighty-four percent of patients had low nutritional risk by the Nutrition Risk in the Critically Ill score. At T1, the Pearson correlation between the estimated total urinary nitrogen and the urea/creatinine index was 0.272 (p = 0.051), and at T2 it was 0.276 (p = 0.048). The urea/creatinine index at T2 had a tendency to better discriminate severe protein hypercatabolism than Acute Physiology and Chronic Health Evaluation II and Nutrition Risk in the Critically Ill (AUC 0.741 versus 0.669 and 0.656, 95%CI: 0.602 – 0.880; 0.519 – 0.818 and 0.506 – 0.806, respectively). The optimal cutoff value of the urea/creatinine index for the diagnosis of severe protein hypercatabolism was 16.15, with a sensitivity of 79.31% (95%CI: 59.74 – 91.29), specificity of 60.87% (95%CI: 38.78 – 79.53), positive predictive value 71.88% (95%CI: 53.02 – 85.60), negative predictive value 70.0% (95%CI: 45.67 – 87.18), LR (+) 2.03 (95%CI: 1.18 – 3.49), and LR (-) 0.34 (95%CI: 0.16 – 0.74).
Conclusion:
The urea/creatinine index measured on the fourth day has a certain ability to estimate severe protein hypercatabolism (as defined by estimated total urinary nitrogen) but does not replace total urinary nitrogen in critically ventilated patients without kidney failure. Due to its reasonable sensitivity, it could be used as a screen to identify which patients to take a 24-hour urine sample from.
- Dino Moretti
-
Original Article
Incidence of low-triiodothyronine syndrome in patients with septic shock
- Matias German Cornu ,
- Andrés Luciano Nicolas Martinuzzi ,
- Pedro Roel,
- Laura Sanhueza,
- Mariana Elisabeth Sepúlveda, [ … ],
- Melina Gulino
Abstract
Original ArticleIncidence of low-triiodothyronine syndrome in patients with septic shock
Rev Bras Ter Intensiva. 2020;32(4):514-520
DOI 10.5935/0103-507X.20200088
- Matias German Cornu ,
- Andrés Luciano Nicolas Martinuzzi ,
- Pedro Roel,
- Laura Sanhueza,
- Mariana Elisabeth Sepúlveda,
- Martin Sergio Orozco,
- Carlos Arturo Sánchez,
- Melina Gulino
Views0See moreABSTRACT
Objective:
Low levels of thyroid hormones have been associated with poor clinical outcomes. This metabolic situation, designated euthyroid sick syndrome, has been interpreted as a state of adaptation to different pathological processes, characterized by the decrease in plasma triiodothyronine. The present study seeks to determine the incidence of this disorder in patients with septic shock and its relationship with other severity indices and clinical outcomes.
Methods:
This prospective analytical study evaluated patients admitted to the intensive care unit with septic shock between April 2018 and July 2019. Variables associated with septic shock and thyroid profile were recorded at the time of the septic shock diagnosis and 7, 14, and 21 days later.
Results:
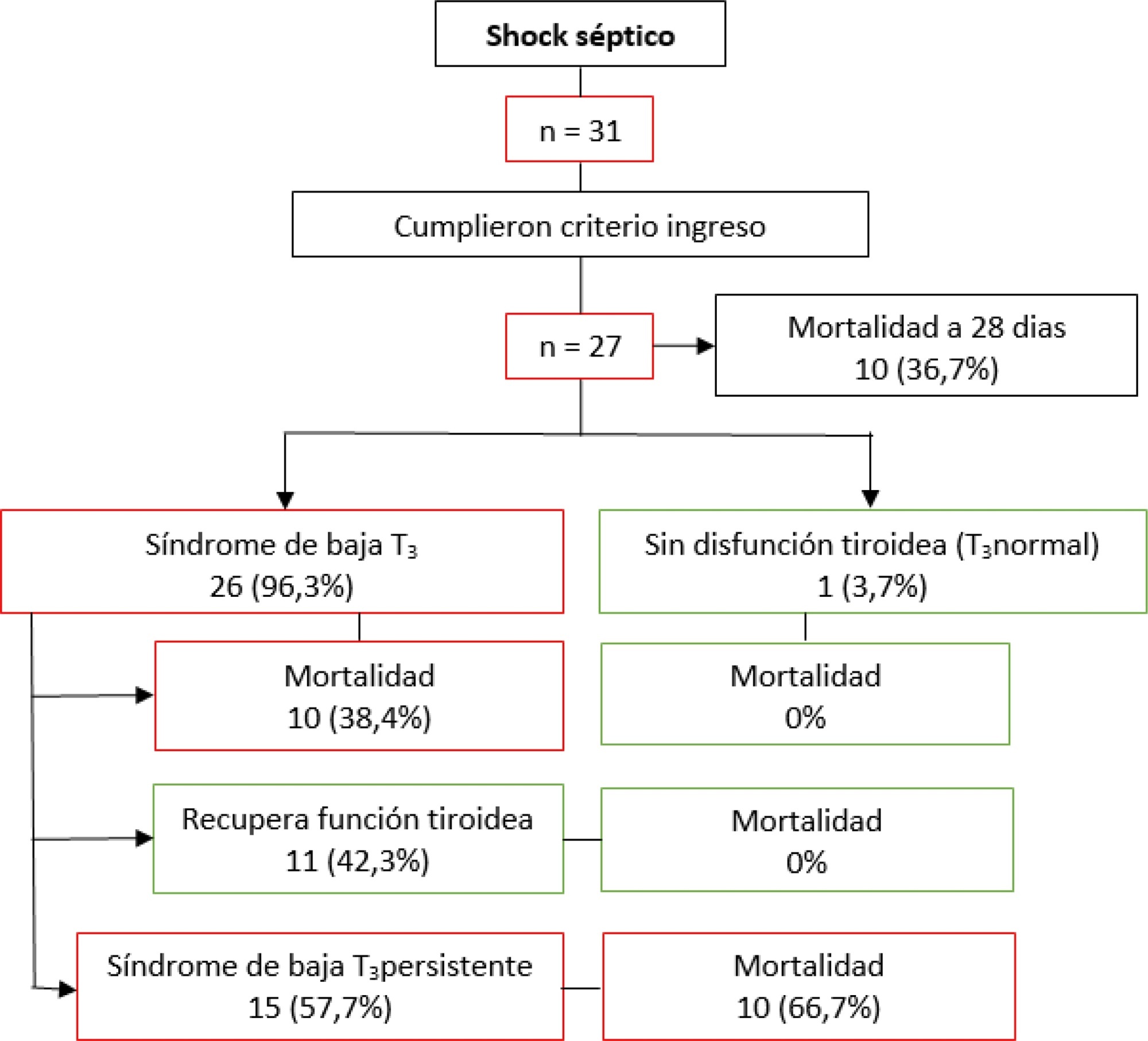
A total of 27 patients who met the inclusion criteria were analyzed. The incidence of an altered thyroid axis was 96.3%, with a mortality at 28 days of 36.7%. Patients without hormonal alteration did not present negative outcomes. Among those with low triiodothyronine, 42.3% recovered their thyroid function within 28 days, in whom mortality was 0%; 57.7% did not recover their thyroid function, in whom mortality was 66.7%. Those whose thyroid axis was altered and who did not normalize its function required more doses of vasoactives and had deteriorated lactate clearance.
Conclusion:
Patients with septic shock have a high incidence of alteration of the thyroid axis, and this dysfunction is associated with higher mortality.
Views0Abstract
Original ArticleIncidence of low-triiodothyronine syndrome in patients with septic shock
Rev Bras Ter Intensiva. 2020;32(4):514-520
DOI 10.5935/0103-507X.20200088
- Matias German Cornu ,
- Andrés Luciano Nicolas Martinuzzi ,
- Pedro Roel,
- Laura Sanhueza,
- Mariana Elisabeth Sepúlveda,
- Martin Sergio Orozco,
- Carlos Arturo Sánchez,
- Melina Gulino
Views0See moreABSTRACT
Objective:
Low levels of thyroid hormones have been associated with poor clinical outcomes. This metabolic situation, designated euthyroid sick syndrome, has been interpreted as a state of adaptation to different pathological processes, characterized by the decrease in plasma triiodothyronine. The present study seeks to determine the incidence of this disorder in patients with septic shock and its relationship with other severity indices and clinical outcomes.
Methods:
This prospective analytical study evaluated patients admitted to the intensive care unit with septic shock between April 2018 and July 2019. Variables associated with septic shock and thyroid profile were recorded at the time of the septic shock diagnosis and 7, 14, and 21 days later.
Results:
A total of 27 patients who met the inclusion criteria were analyzed. The incidence of an altered thyroid axis was 96.3%, with a mortality at 28 days of 36.7%. Patients without hormonal alteration did not present negative outcomes. Among those with low triiodothyronine, 42.3% recovered their thyroid function within 28 days, in whom mortality was 0%; 57.7% did not recover their thyroid function, in whom mortality was 66.7%. Those whose thyroid axis was altered and who did not normalize its function required more doses of vasoactives and had deteriorated lactate clearance.
Conclusion:
Patients with septic shock have a high incidence of alteration of the thyroid axis, and this dysfunction is associated with higher mortality.
- Matias German Cornu
-
Original Article
Comparison of SAPS 3 performance in patients with and without solid tumor admitted to an intensive care unit in Brazil: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(4):521-527
Abstract
Original ArticleComparison of SAPS 3 performance in patients with and without solid tumor admitted to an intensive care unit in Brazil: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(4):521-527
DOI 10.5935/0103-507X.20200089
Views1See moreABSTRACT
Objective:
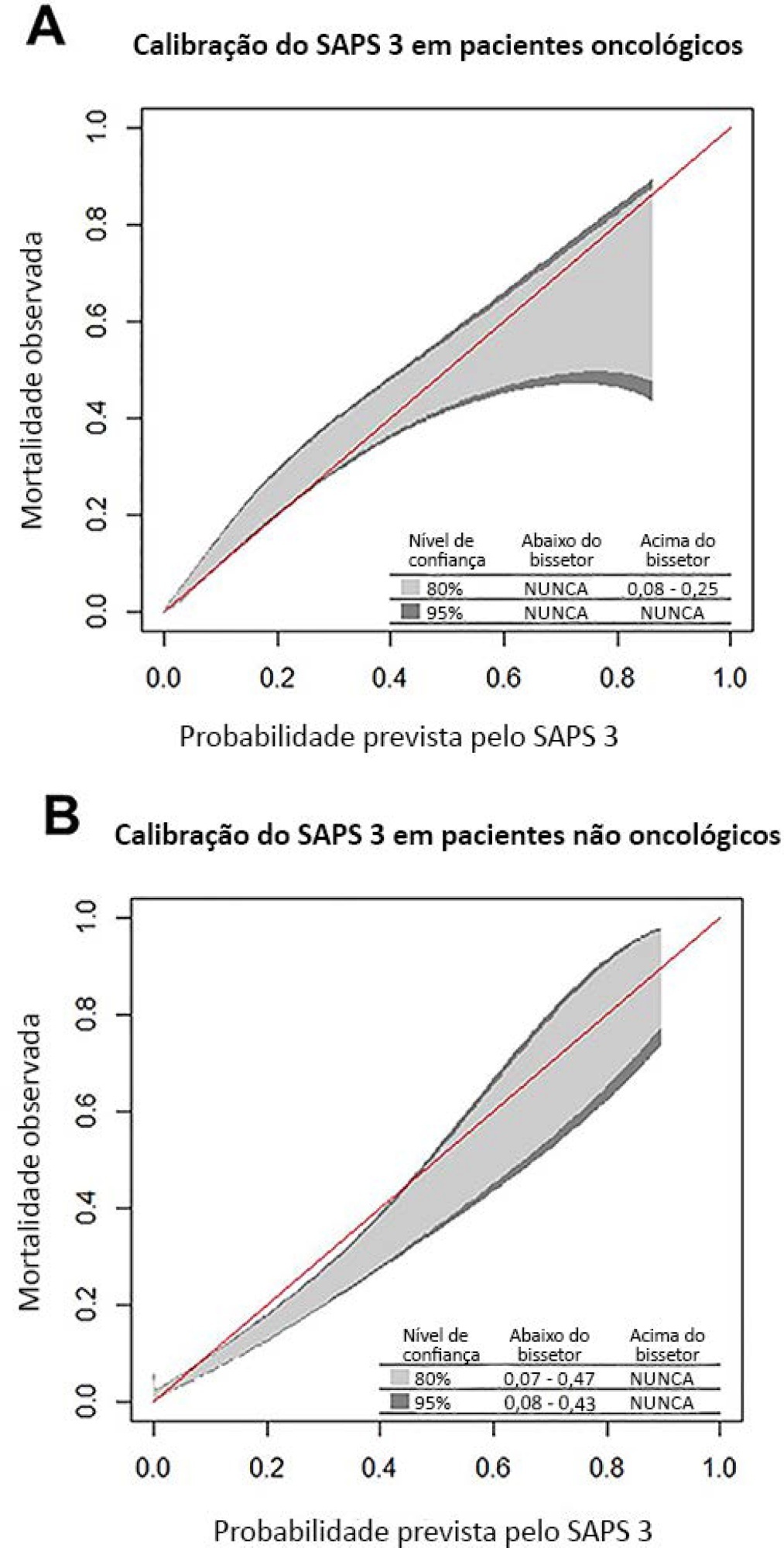
To compare the performance of the Simplified Acute Physiology Score 3 (SAPS 3) in patients with and without solid cancer who were admitted to the intensive care unit of a comprehensive oncological hospital in Brazil.
Methods:
We performed a retrospective cohort analysis of our administrative database of the first admission of adult patients to the intensive care unit from 2012 to 2016. The patients were categorized according to the presence of solid cancer. We evaluated discrimination using the area under the Receiver Operating Characteristic curve (AUROC) and calibration using the calibration belt approach.
Results:
We included 7,254 patients (41.5% had cancer, and 12.1% died during hospitalization). Oncological patients had higher hospital mortality than nononcological patients (14.1% versus 10.6%, respectively; p < 0.001). SAPS 3 discrimination was better for oncological patients (AUROC = 0.85) than for nononcological patients (AUROC = 0.79) (p < 0.001). After we applied the calibration belt in oncological patients, the SAPS 3 matched the average observed rates with a confidence level of 95%. In nononcological patients, the SAPS 3 overestimated mortality in those with a low-middle risk. Calibration was affected by the time period only for nononcological patients.
Conclusion:
SAPS 3 performed differently between oncological and nononcological patients in our single-center cohort, and variation over time (mainly calibration) was observed. This finding should be taken into account when evaluating severity-of-illness score performance.
Views1Abstract
Original ArticleComparison of SAPS 3 performance in patients with and without solid tumor admitted to an intensive care unit in Brazil: a retrospective cohort study
Rev Bras Ter Intensiva. 2020;32(4):521-527
DOI 10.5935/0103-507X.20200089
Views1See moreABSTRACT
Objective:
To compare the performance of the Simplified Acute Physiology Score 3 (SAPS 3) in patients with and without solid cancer who were admitted to the intensive care unit of a comprehensive oncological hospital in Brazil.
Methods:
We performed a retrospective cohort analysis of our administrative database of the first admission of adult patients to the intensive care unit from 2012 to 2016. The patients were categorized according to the presence of solid cancer. We evaluated discrimination using the area under the Receiver Operating Characteristic curve (AUROC) and calibration using the calibration belt approach.
Results:
We included 7,254 patients (41.5% had cancer, and 12.1% died during hospitalization). Oncological patients had higher hospital mortality than nononcological patients (14.1% versus 10.6%, respectively; p < 0.001). SAPS 3 discrimination was better for oncological patients (AUROC = 0.85) than for nononcological patients (AUROC = 0.79) (p < 0.001). After we applied the calibration belt in oncological patients, the SAPS 3 matched the average observed rates with a confidence level of 95%. In nononcological patients, the SAPS 3 overestimated mortality in those with a low-middle risk. Calibration was affected by the time period only for nononcological patients.
Conclusion:
SAPS 3 performed differently between oncological and nononcological patients in our single-center cohort, and variation over time (mainly calibration) was observed. This finding should be taken into account when evaluating severity-of-illness score performance.
-
Original Article
Mechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte, [ … ],
- Bruno Adler Maccagnan Pinheiro Besen
Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
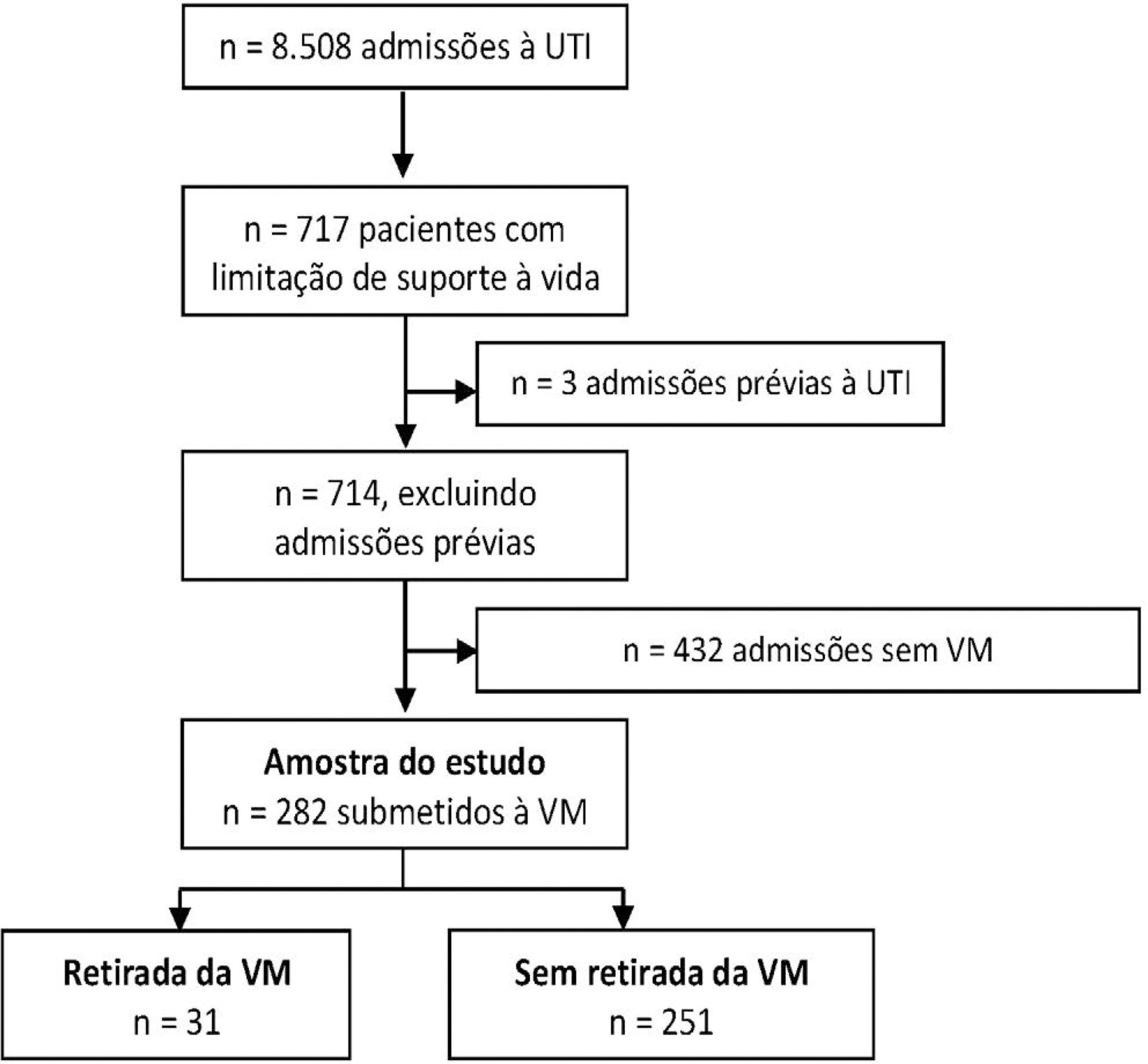
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
Views1Abstract
Original ArticleMechanical ventilation withdrawal as a palliative procedure in a Brazilian intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):528-534
DOI 10.5935/0103-507X.20200090
- Fábio Holanda Lacerda ,
- Pedro Garcia Checoli,
- Carla Marchini Dias da Silva,
- Carlos Eduardo Brandão,
- Daniel Neves Forte,
- Bruno Adler Maccagnan Pinheiro Besen
Views1See moreAbstract
Objective:
To describe the characteristics and outcomes of patients undergoing mechanical ventilation withdrawal and to compare them to mechanically ventilated patients with limitations (withhold or withdrawal) of life-sustaining therapies but who did not undergo mechanical ventilation withdrawal.
Methods:
This was a retrospective cohort study from January 2014 to December 2018 of mechanically ventilated patients with any organ support limitation admitted to a single intensive care unit. We compared patients who underwent mechanical ventilation withdrawal and those who did not regarding intensive care unit and hospital mortality and length of stay in both an unadjusted analysis and a propensity score matched subsample. We also analyzed the time from mechanical ventilation withdrawal to death.
Results:
Out of 282 patients with life-sustaining therapy limitations, 31 (11%) underwent mechanical ventilation withdrawal. There was no baseline difference between groups. Intensive care unit and hospital mortality rates were 71% versus 57% and 93% versus 80%, respectively, among patients who underwent mechanical ventilation withdrawal and those who did not. The median intensive care unit length of stay was 7 versus 8 days (p = 0.6), and the hospital length of stay was 9 versus 15 days (p = 0.015). Hospital mortality was not significantly different (25/31; 81% versus 29/31; 93%; p = 0.26) after matching. The median time from mechanical ventilation withdrawal until death was 2 days [0 – 5], and 10/31 (32%) patients died within 24 hours after mechanical ventilation withdrawal.
Conclusion:
In this Brazilian report, mechanical ventilation withdrawal represented 11% of all patients with treatment limitations and was not associated with increased hospital mortality after propensity score matching on relevant covariates.
- Fábio Holanda Lacerda
-
Original Article
Viability and validity of the bispectral index to measure sleep in patients in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):535-541
Abstract
Original ArticleViability and validity of the bispectral index to measure sleep in patients in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):535-541
DOI 10.5935/0103-507X.20200083
Views0Abstract
Objective:
To investigate the viability of the bispectral index in the sleep evaluation of critically ill patients and to quantify the associations of sleep parameters measured by this index with the Richards-Campbell Sleep Questionnaire and environmental noise.
Methods:
This was a cross-sectional observational study that evaluated critically ill adults with diseases of low or moderate severity. The following were measured: total sleep volume and time, deep sleep volume and time, continuous sleep volume and time, sleep onset latency, and environmental sound pressure level. The subjective perception of sleep was evaluated with the Richards-Campbell Sleep Questionnaire the morning after each night of observation.
Results:
Patients had a low total sleep time (234 minutes), a predominance of superficial sleep stages, and little deep sleep (1.7 minutes). The total, deep, and continuous sleep volumes were 3,679, 9.4, and 3,143 (bispectral index units × minutes), respectively. The sleep latency was 94 minutes. The mean score of the Richards-Campbell Sleep Questionnaire was 57.9. Total sleep volume, total sleep time, and continuous sleep volume were weakly correlated with the Richards-Campbell Sleep Questionnaire depth of sleep domain score, overall sleep quality domain score, and total score. Total volume, total time, and continuous volume were moderately correlated with the occurrence of awakenings domain score.
Conclusion:
The bispectral index is an instrument with limited viability to monitor the sleep of lucid patients and patients with low to moderate disease severity in the intensive care unit. Patients with higher total sleep volume, total sleep time, and continuous sleep volume had better overall sleep perception.
Keywords:Consciousness monitorsIntensive care unitsSleepSleep deprivationSleep disorders, circadian rhythmSleep initiation and maintenance disordersSee moreViews0Abstract
Original ArticleViability and validity of the bispectral index to measure sleep in patients in the intensive care unit
Rev Bras Ter Intensiva. 2020;32(4):535-541
DOI 10.5935/0103-507X.20200083
Views0Abstract
Objective:
To investigate the viability of the bispectral index in the sleep evaluation of critically ill patients and to quantify the associations of sleep parameters measured by this index with the Richards-Campbell Sleep Questionnaire and environmental noise.
Methods:
This was a cross-sectional observational study that evaluated critically ill adults with diseases of low or moderate severity. The following were measured: total sleep volume and time, deep sleep volume and time, continuous sleep volume and time, sleep onset latency, and environmental sound pressure level. The subjective perception of sleep was evaluated with the Richards-Campbell Sleep Questionnaire the morning after each night of observation.
Results:
Patients had a low total sleep time (234 minutes), a predominance of superficial sleep stages, and little deep sleep (1.7 minutes). The total, deep, and continuous sleep volumes were 3,679, 9.4, and 3,143 (bispectral index units × minutes), respectively. The sleep latency was 94 minutes. The mean score of the Richards-Campbell Sleep Questionnaire was 57.9. Total sleep volume, total sleep time, and continuous sleep volume were weakly correlated with the Richards-Campbell Sleep Questionnaire depth of sleep domain score, overall sleep quality domain score, and total score. Total volume, total time, and continuous volume were moderately correlated with the occurrence of awakenings domain score.
Conclusion:
The bispectral index is an instrument with limited viability to monitor the sleep of lucid patients and patients with low to moderate disease severity in the intensive care unit. Patients with higher total sleep volume, total sleep time, and continuous sleep volume had better overall sleep perception.
Keywords:Consciousness monitorsIntensive care unitsSleepSleep deprivationSleep disorders, circadian rhythmSleep initiation and maintenance disordersSee more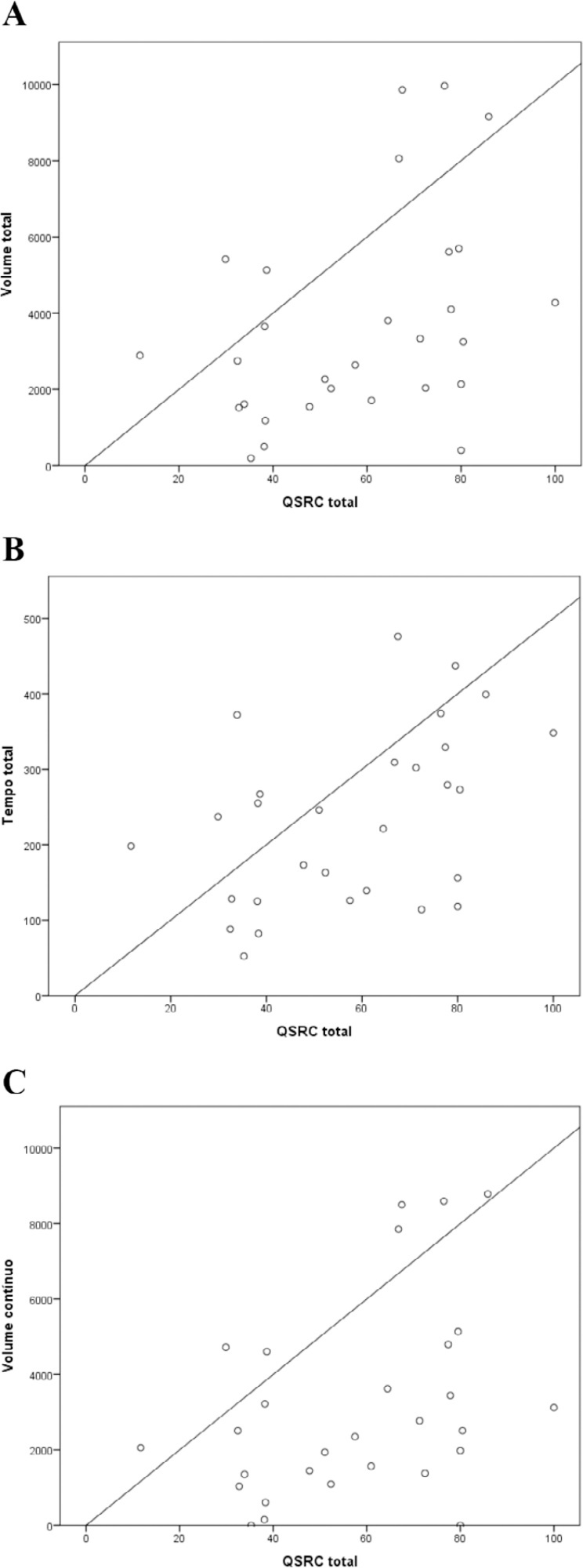
-
Original Article
Outcomes after intra-aortic balloon pump insertion in cardiac surgery patients
- George Samanidis ,
- Georgios Georgiopoulos,
- Stefanos Bousounis,
- Panagiotis Zoumpourlis,
- Konstantinos Perreas
Abstract
Original ArticleOutcomes after intra-aortic balloon pump insertion in cardiac surgery patients
Rev Bras Ter Intensiva. 2020;32(4):542-550
DOI 10.5935/0103-507X.20200091
- George Samanidis ,
- Georgios Georgiopoulos,
- Stefanos Bousounis,
- Panagiotis Zoumpourlis,
- Konstantinos Perreas
Views0ABSTRACT
Objective:
To assess whether preoperative versus intraoperative insertion of an intra-aortic balloon pump is associated with lower 30-day mortality or reduced length of hospital stay among patients who had an intra-aortic balloon pump inserted for cardiac surgery.
Methods:
This was an observational study of patients who had an intra-aortic balloon pump inserted in the preoperative or intraoperative period of cardiac surgery in our department between 2000 and 2012. We assessed the association between preoperative versus intraoperative insertion of an intra-aortic balloon pump and 30-day mortality in a multivariable logistic regression analysis, including preoperative New York Heart Association class, postoperative atrial fibrillation, reoperation, postoperative creatinine and isolated coronary bypass grafting as cofactors. We used a multivariate linear model to assess whether a preoperative versus intraoperative intra-aortic balloon pump was associated with length of postoperative hospital stay, adjusting for reoperation, isolated coronary bypass grafting, heart valve surgery, sex, age, cardiopulmonary bypass time, aortic cross-clamp time, preoperative patients’ status (elective, urgency or emergency surgery) and preoperative myocardial infarction.
Results:
Overall, 7,540 consecutive patients underwent open heart surgery in our department, and an intra-aortic balloon pump was inserted pre- or intraoperatively in 322 (4.2%) patients. The mean age was 67 ± 10.2 years old, the 30-day mortality was 12.7%, and the median length of hospital stay was 9 days (7 – 13). Preoperative versus intraoperative intra-aortic balloon pump insertion did not affect the incidence of 30-day mortality (adjusted OR = 0.69; 95% CI, 0.15 – 3.12; p = 0.63) and length of postoperative hospital stay (β = 5.3; 95%CI, -1.6 to 12.8; p = 0.13).
Conclusion:
Preoperative insertion of an intra-aortic balloon pump was not associated with a lower 30-day mortality or reduced length of postoperative hospital stay compared to intraoperative insertion.
Keywords:Cardiac output, lowHeart surgeryIntra-aortic balloon pumpMortalityVentricular dysfunction, leftSee moreViews0Abstract
Original ArticleOutcomes after intra-aortic balloon pump insertion in cardiac surgery patients
Rev Bras Ter Intensiva. 2020;32(4):542-550
DOI 10.5935/0103-507X.20200091
- George Samanidis ,
- Georgios Georgiopoulos,
- Stefanos Bousounis,
- Panagiotis Zoumpourlis,
- Konstantinos Perreas
Views0ABSTRACT
Objective:
To assess whether preoperative versus intraoperative insertion of an intra-aortic balloon pump is associated with lower 30-day mortality or reduced length of hospital stay among patients who had an intra-aortic balloon pump inserted for cardiac surgery.
Methods:
This was an observational study of patients who had an intra-aortic balloon pump inserted in the preoperative or intraoperative period of cardiac surgery in our department between 2000 and 2012. We assessed the association between preoperative versus intraoperative insertion of an intra-aortic balloon pump and 30-day mortality in a multivariable logistic regression analysis, including preoperative New York Heart Association class, postoperative atrial fibrillation, reoperation, postoperative creatinine and isolated coronary bypass grafting as cofactors. We used a multivariate linear model to assess whether a preoperative versus intraoperative intra-aortic balloon pump was associated with length of postoperative hospital stay, adjusting for reoperation, isolated coronary bypass grafting, heart valve surgery, sex, age, cardiopulmonary bypass time, aortic cross-clamp time, preoperative patients’ status (elective, urgency or emergency surgery) and preoperative myocardial infarction.
Results:
Overall, 7,540 consecutive patients underwent open heart surgery in our department, and an intra-aortic balloon pump was inserted pre- or intraoperatively in 322 (4.2%) patients. The mean age was 67 ± 10.2 years old, the 30-day mortality was 12.7%, and the median length of hospital stay was 9 days (7 – 13). Preoperative versus intraoperative intra-aortic balloon pump insertion did not affect the incidence of 30-day mortality (adjusted OR = 0.69; 95% CI, 0.15 – 3.12; p = 0.63) and length of postoperative hospital stay (β = 5.3; 95%CI, -1.6 to 12.8; p = 0.13).
Conclusion:
Preoperative insertion of an intra-aortic balloon pump was not associated with a lower 30-day mortality or reduced length of postoperative hospital stay compared to intraoperative insertion.
Keywords:Cardiac output, lowHeart surgeryIntra-aortic balloon pumpMortalityVentricular dysfunction, leftSee more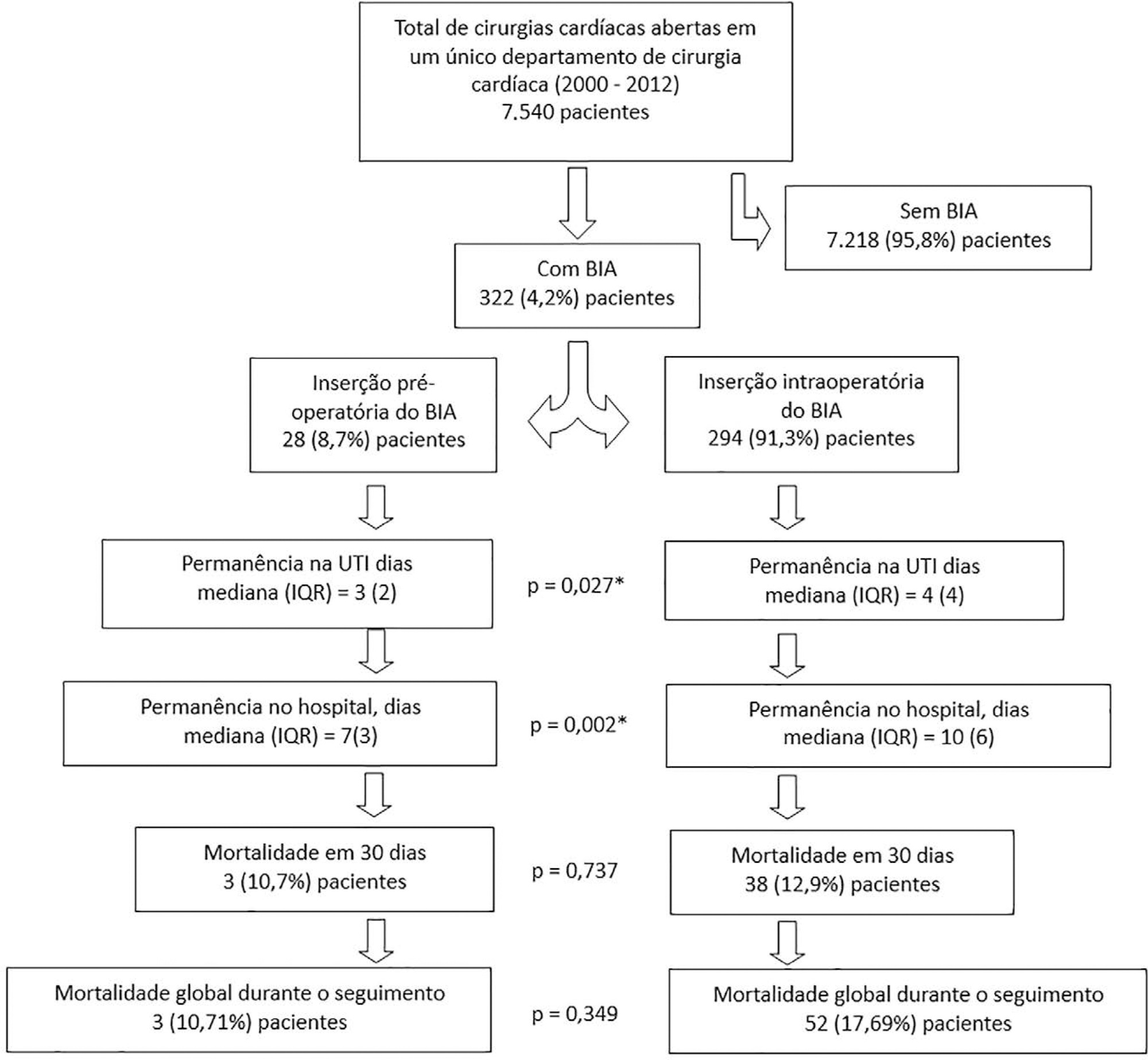
- George Samanidis
-
Original Article
Clinical outcome of children with fluid-refractory septic shock treated with dopamine or epinephrine. A retrospective study at a pediatric emergency department in Argentina
- Guillermo Kohn-Loncarica ,
- Ana Fustiñana,
- César Santos,
- Guadalupe Paniagua Lantelli,
- Hernan Rowensztein, [ … ],
- Sebastián González-Dambrauskas
Abstract
Original ArticleClinical outcome of children with fluid-refractory septic shock treated with dopamine or epinephrine. A retrospective study at a pediatric emergency department in Argentina
Rev Bras Ter Intensiva. 2020;32(4):551-556
DOI 10.5935/0103-507X.20200092
- Guillermo Kohn-Loncarica ,
- Ana Fustiñana,
- César Santos,
- Guadalupe Paniagua Lantelli,
- Hernan Rowensztein,
- Sebastián González-Dambrauskas
Views0See moreAbstract
Objective:
To analyze the clinical outcome of children with fluid-refractory septic shock initially treated with dopamine or epinephrine.
Methods:
A retrospective cohort study was conducted at a pediatric emergency department of a tertiary hospital. Population: children admitted because of fluid-refractory septic shock. Clinical outcome was compared between two groups: Dopamine and Epinephrine. Variables evaluated were use of invasive mechanical ventilation, days of inotropic therapy, length of hospital stay, intensive care stay, and mortality. For numerical and categorical variables, we used measures of central tendency. They were compared by the Mann-Whitney U-test and the (2 test.
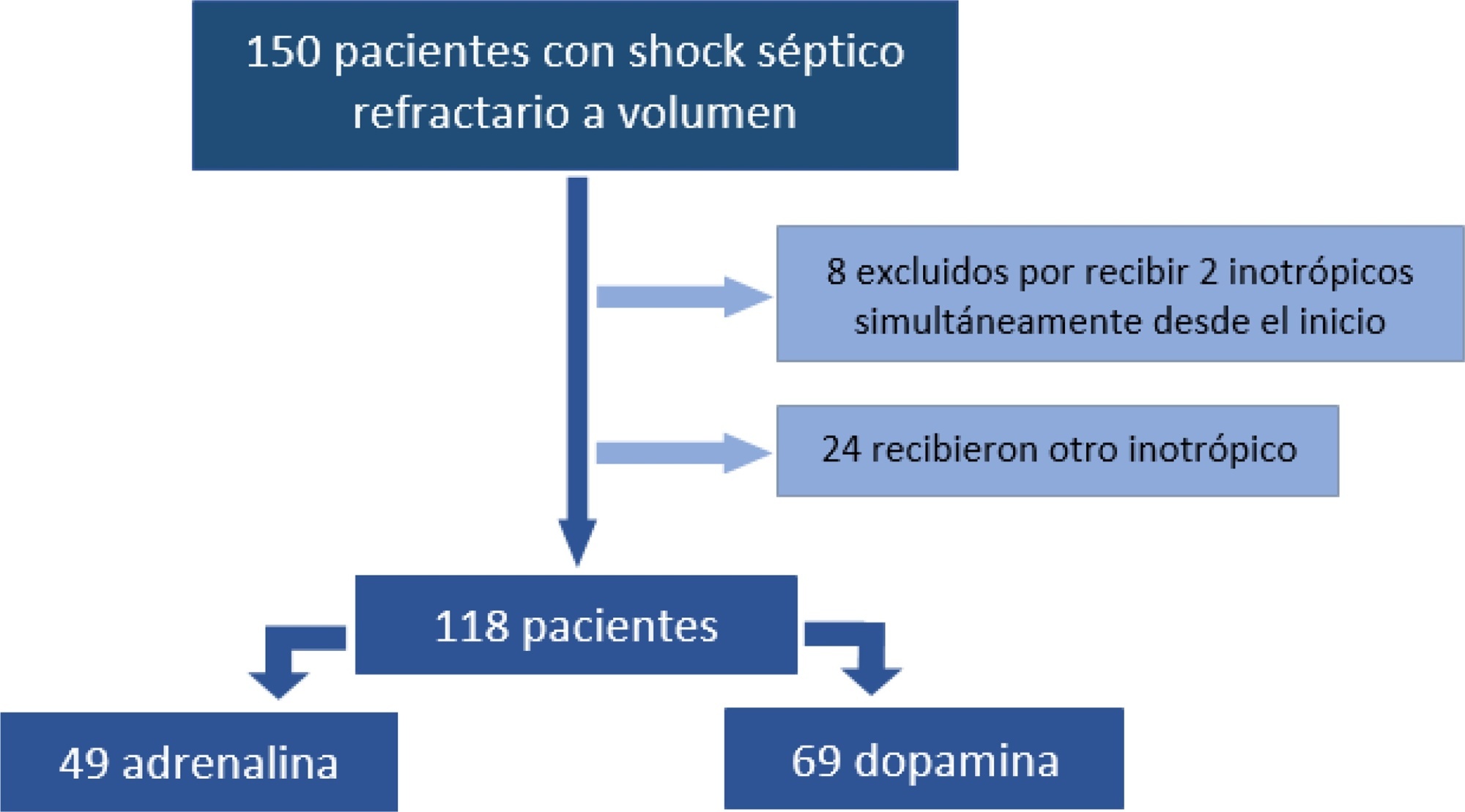
Results:
We included 118 patients. A total of 58.5% received dopamine and 41.5% received epinephrine. The rate of invasive mechanical ventilation was 38.8% for epinephrine versus 40.6% for dopamine (p = 0.84), with a median of 4 days for the Epinephrine Group and 5.5 for the Dopamine Group (p = 0.104). Median time of inotropic therapy was 2 days for both groups (p = 0.714). Median hospital stay was 11 and 13 days for the Epinephrine and Dopamine groups, respectively (p = 0.554), and median stay in intensive care was 4 days (0 – 81 days) in both groups (p = 0.748). Mortality was 5% for the Epinephrine Group versus 9% for the Dopamine Group (p = 0.64).
Conclusions:
At our center, no differences in use of invasive mechanical ventilation, time of inotropic therapy, length of hospital stay, length of intensive care unit stay, or mortality were observed in children admitted to the pediatric emergency department with a diagnosis of fluid-refractory septic shock initially treated with dopamine versus epinephrine.
Views0Abstract
Original ArticleClinical outcome of children with fluid-refractory septic shock treated with dopamine or epinephrine. A retrospective study at a pediatric emergency department in Argentina
Rev Bras Ter Intensiva. 2020;32(4):551-556
DOI 10.5935/0103-507X.20200092
- Guillermo Kohn-Loncarica ,
- Ana Fustiñana,
- César Santos,
- Guadalupe Paniagua Lantelli,
- Hernan Rowensztein,
- Sebastián González-Dambrauskas
Views0See moreAbstract
Objective:
To analyze the clinical outcome of children with fluid-refractory septic shock initially treated with dopamine or epinephrine.
Methods:
A retrospective cohort study was conducted at a pediatric emergency department of a tertiary hospital. Population: children admitted because of fluid-refractory septic shock. Clinical outcome was compared between two groups: Dopamine and Epinephrine. Variables evaluated were use of invasive mechanical ventilation, days of inotropic therapy, length of hospital stay, intensive care stay, and mortality. For numerical and categorical variables, we used measures of central tendency. They were compared by the Mann-Whitney U-test and the (2 test.
Results:
We included 118 patients. A total of 58.5% received dopamine and 41.5% received epinephrine. The rate of invasive mechanical ventilation was 38.8% for epinephrine versus 40.6% for dopamine (p = 0.84), with a median of 4 days for the Epinephrine Group and 5.5 for the Dopamine Group (p = 0.104). Median time of inotropic therapy was 2 days for both groups (p = 0.714). Median hospital stay was 11 and 13 days for the Epinephrine and Dopamine groups, respectively (p = 0.554), and median stay in intensive care was 4 days (0 – 81 days) in both groups (p = 0.748). Mortality was 5% for the Epinephrine Group versus 9% for the Dopamine Group (p = 0.64).
Conclusions:
At our center, no differences in use of invasive mechanical ventilation, time of inotropic therapy, length of hospital stay, length of intensive care unit stay, or mortality were observed in children admitted to the pediatric emergency department with a diagnosis of fluid-refractory septic shock initially treated with dopamine versus epinephrine.
- Guillermo Kohn-Loncarica
-
Original Article
Impact of the use of nephrotoxic drugs in critically ill pediatric patients
Rev Bras Ter Intensiva. 2020;32(4):557-563
Abstract
Original ArticleImpact of the use of nephrotoxic drugs in critically ill pediatric patients
Rev Bras Ter Intensiva. 2020;32(4):557-563
DOI 10.5935/0103-507X.20200093
Views0Abstract
Objective:
To evaluate the association between the use of nephrotoxic drugs and acute kidney injury in critically ill pediatric patients.
Methods:
This was a retrospective cohort study involving all children admitted to the intensive care unit of a pediatric hospital during a 1-year period. Acute kidney injury was defined according to the KDIGO classification. Patients with a length of hospital stay longer than 48 hours and an age between 1 month and 14 years were included. Patients with acute or chronic nephropathy, uropathy, congenital or acquired heart disease, chronic use of nephrotoxic drugs, rhabdomyolysis and tumor lysis syndrome were excluded. Patients were classified according to the use of nephrotoxic drugs during their stay at the pediatric intensive care unit.
Results:
The sample consisted of 226 children, of whom 37.1% used nephrotoxic drugs, 42.4% developed acute kidney injury, and 7.5% died. The following drugs, when used alone, were associated with acute kidney injury: acyclovir (p < 0.001), vancomycin (p < 0.001), furosemide (p < 0.001) and ganciclovir (p = 0.008). The concomitant use of two or more nephrotoxic drugs was characterized as an independent marker of renal dysfunction (p < 0.001). After discharge from the pediatric intensive care unit, renal function monitoring in the ward was inadequate in 19.8% of cases.
Conclusion:
It is necessary for intensivist physicians to have knowledge of the main nephrotoxic drugs to predict, reduce or avoid damage to their patients.
Keywords:Acute kidney injuryChildDrug-related side effects and adverse reactionsIntensive care units, pediatricToxicitySee moreViews0Abstract
Original ArticleImpact of the use of nephrotoxic drugs in critically ill pediatric patients
Rev Bras Ter Intensiva. 2020;32(4):557-563
DOI 10.5935/0103-507X.20200093
Views0Abstract
Objective:
To evaluate the association between the use of nephrotoxic drugs and acute kidney injury in critically ill pediatric patients.
Methods:
This was a retrospective cohort study involving all children admitted to the intensive care unit of a pediatric hospital during a 1-year period. Acute kidney injury was defined according to the KDIGO classification. Patients with a length of hospital stay longer than 48 hours and an age between 1 month and 14 years were included. Patients with acute or chronic nephropathy, uropathy, congenital or acquired heart disease, chronic use of nephrotoxic drugs, rhabdomyolysis and tumor lysis syndrome were excluded. Patients were classified according to the use of nephrotoxic drugs during their stay at the pediatric intensive care unit.
Results:
The sample consisted of 226 children, of whom 37.1% used nephrotoxic drugs, 42.4% developed acute kidney injury, and 7.5% died. The following drugs, when used alone, were associated with acute kidney injury: acyclovir (p < 0.001), vancomycin (p < 0.001), furosemide (p < 0.001) and ganciclovir (p = 0.008). The concomitant use of two or more nephrotoxic drugs was characterized as an independent marker of renal dysfunction (p < 0.001). After discharge from the pediatric intensive care unit, renal function monitoring in the ward was inadequate in 19.8% of cases.
Conclusion:
It is necessary for intensivist physicians to have knowledge of the main nephrotoxic drugs to predict, reduce or avoid damage to their patients.
Keywords:Acute kidney injuryChildDrug-related side effects and adverse reactionsIntensive care units, pediatricToxicitySee more -
Original Article
Hemodynamically stable oliguric patients usually do not respond to fluid challenge
- Vinicius Brenner Felice,
- Thiago Costa Lisboa,
- Lucas Vieira de Souza,
- Luana Canevese Sell,
- Gilberto Friedman
Abstract
Original ArticleHemodynamically stable oliguric patients usually do not respond to fluid challenge
Rev Bras Ter Intensiva. 2020;32(4):564-570
DOI 10.5935/0103-507X.20200094
- Vinicius Brenner Felice,
- Thiago Costa Lisboa,
- Lucas Vieira de Souza,
- Luana Canevese Sell,
- Gilberto Friedman
Views0See moreABSTRACT
Objective:
To evaluate renal responsiveness in oliguric critically ill patients after a fluid challenge.
Methods:
We conducted a prospective observational study in one university intensive care unit. Patients with urine output < 0.5mL/kg/h for 3 hours with a mean arterial pressure > 60mmHg received a fluid challenge. We examined renal fluid responsiveness (defined as urine output > 0.5mL/kg/h for 3 hours) after fluid challenge.
Results:
Forty-two patients (age 67 ± 13 years; APACHE II score 16 ± 6) were evaluated. Patient characteristics were similar between renal responders and renal nonresponders. Thirteen patients (31%) were renal responders. Hemodynamic or perfusion parameters were not different between those who did and those who did not increase urine output before the fluid challenge. The areas under the receiver operating characteristic curves were calculated for mean arterial pressure, heart rate, creatinine, urea, creatinine clearance, urea/creatinine ratio and lactate before the fluid challenge. None of these parameters were sensitive or specific enough to predict reversal of oliguria.
Conclusion:
After achieving hemodynamic stability, oliguric patients did not increase urine output after a fluid challenge. Systemic hemodynamic, perfusion or renal parameters were weak predictors of urine responsiveness. Our results suggest that volume replacement to correct oliguria in patients without obvious hypovolemia should be done with caution.
Views0Abstract
Original ArticleHemodynamically stable oliguric patients usually do not respond to fluid challenge
Rev Bras Ter Intensiva. 2020;32(4):564-570
DOI 10.5935/0103-507X.20200094
- Vinicius Brenner Felice,
- Thiago Costa Lisboa,
- Lucas Vieira de Souza,
- Luana Canevese Sell,
- Gilberto Friedman
Views0See moreABSTRACT
Objective:
To evaluate renal responsiveness in oliguric critically ill patients after a fluid challenge.
Methods:
We conducted a prospective observational study in one university intensive care unit. Patients with urine output < 0.5mL/kg/h for 3 hours with a mean arterial pressure > 60mmHg received a fluid challenge. We examined renal fluid responsiveness (defined as urine output > 0.5mL/kg/h for 3 hours) after fluid challenge.
Results:
Forty-two patients (age 67 ± 13 years; APACHE II score 16 ± 6) were evaluated. Patient characteristics were similar between renal responders and renal nonresponders. Thirteen patients (31%) were renal responders. Hemodynamic or perfusion parameters were not different between those who did and those who did not increase urine output before the fluid challenge. The areas under the receiver operating characteristic curves were calculated for mean arterial pressure, heart rate, creatinine, urea, creatinine clearance, urea/creatinine ratio and lactate before the fluid challenge. None of these parameters were sensitive or specific enough to predict reversal of oliguria.
Conclusion:
After achieving hemodynamic stability, oliguric patients did not increase urine output after a fluid challenge. Systemic hemodynamic, perfusion or renal parameters were weak predictors of urine responsiveness. Our results suggest that volume replacement to correct oliguria in patients without obvious hypovolemia should be done with caution.
-
Original Article
Impact of implementing a protocol of respiratory care measures and optimization of mechanical ventilation in potential lung donors
- Marco Guillermo Bezzi ,
- Carla Candela Brovia,
- Juan Manuel Carballo,
- Maia Inés Elías,
- Agustina Belén Moreno, [ … ],
- Silvina Borello
Abstract
Original ArticleImpact of implementing a protocol of respiratory care measures and optimization of mechanical ventilation in potential lung donors
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
- Marco Guillermo Bezzi ,
- Carla Candela Brovia,
- Juan Manuel Carballo,
- Maia Inés Elías,
- Agustina Belén Moreno,
- Vanesa Romina Ruiz ,
- Fernanda Cordiviola,
- David Barbieri,
- Adriana Fariña,
- Silvina Borello
Views0ABSTRACT
Objective:
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
Methods:
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Results:
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 – 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.
Keywords:brain deathDonor selectionLung transplantationorgan transplantationRespiration, artificialTissue and organ procurementSee moreViews0Abstract
Original ArticleImpact of implementing a protocol of respiratory care measures and optimization of mechanical ventilation in potential lung donors
Rev Bras Ter Intensiva. 2020;32(4):571-577
DOI 10.5935/0103-507X.20200095
- Marco Guillermo Bezzi ,
- Carla Candela Brovia,
- Juan Manuel Carballo,
- Maia Inés Elías,
- Agustina Belén Moreno,
- Vanesa Romina Ruiz ,
- Fernanda Cordiviola,
- David Barbieri,
- Adriana Fariña,
- Silvina Borello
Views0ABSTRACT
Objective:
To describe the results from the implementation of a respiratory care and mechanical ventilation protocol on potential lung donors who met the conditions for procurement. The secondary objective is to compare the results with historical data.
Methods:
This was a retrospective, observational study. It included potential donors suitable for procurement of organs who had brain death and were hospitalized in critical care units of the Autonomous City of Buenos Aires from April 2017 to March 2018. Main variables: number of potential lung donors that reached the objective of procurement, rate of lungs procured, and rate of implanted lungs. Values of p < 0.05 were considered significant.
Results:
Thirty potential lung donors were included, and 23 (88.5%; 95%CI 69.8 – 97.6) met the oxygenation objective. Twenty potential lung donors donated organs, of whom eight donated lungs, with which four double lung transplants and eight single lung transplants were performed. Seven of 12 lungs were procured and implanted in the preprotocol period, while all 12 were under the protocol (p = 0.38). The implantation rate was 58.3% (7/12) in the historical control period and 100% (12/12) (p = 0.04) in the study period.
Keywords:brain deathDonor selectionLung transplantationorgan transplantationRespiration, artificialTissue and organ procurementSee more
- Marco Guillermo Bezzi
-
Original Article
Are the Pediatric Index of Mortality 2 and 3 equal predictors of mortality? An intensive care unit-based concordance study
- Daniela Patino-Hernandez ,
- Alba Deyanira Quiñonez López,
- César Augusto Zuluaga,
- Ángel Alberto García,
- Oscar Mauricio Muñoz-Velandia
Abstract
Original ArticleAre the Pediatric Index of Mortality 2 and 3 equal predictors of mortality? An intensive care unit-based concordance study
Rev Bras Ter Intensiva. 2020;32(4):578-584
DOI 10.5935/0103-507X.20200096
- Daniela Patino-Hernandez ,
- Alba Deyanira Quiñonez López,
- César Augusto Zuluaga,
- Ángel Alberto García,
- Oscar Mauricio Muñoz-Velandia
Views0ABSTRACT
Objective:
To determine the concordance of mortality risk classification through the use of the Pediatric Index of Mortality (PIM) 2 and 3.
Methods:
Through a retrospective cohort, we evaluated patients admitted to the pediatric intensive care unit between April 2016 and December 2018. We calculated the mortality risk with the PIM 2 and 3. Analyses were carried out to determine the concordance between the risk classification obtained with both scales using unweighted and linearly weighted kappa.
Results:
A total of 722 subjects were included, and 66.6% had a chronic condition. The overall mortality was 3.7%. The global kappa concordance coefficient for classifying patients according to risk with the PIM 2 and 3 was moderate at 0.48 (95%CI 0.43 – 0.53). After linear weighting, concordance was substantial at 0.64 (95%CI 0.59 – 0.69). For cardiac surgery patients, concordance for risk classification was fair at 0.30 (95%CI 0.21 – 0.39), and after linear weighting, concordance was only moderate at 0.49 (95%CI 0.39 – 0.59). The PIM 3 assigned a lower risk than the PIM 2 in 44.8% of patients in this subgroup.
Conclusion:
Our study proves that the PIM 2 and 3 are not clinically equivalent and should not be used interchangeably for quality evaluation across pediatric intensive care units. Validation studies must be performed before using the PIM 2 or PIM 3 in specific settings.
Keywords:Cardiac surgeryInfant, newbornIntensive care units, pediatricMortalityPediatric Index of MortalitySee moreViews0Abstract
Original ArticleAre the Pediatric Index of Mortality 2 and 3 equal predictors of mortality? An intensive care unit-based concordance study
Rev Bras Ter Intensiva. 2020;32(4):578-584
DOI 10.5935/0103-507X.20200096
- Daniela Patino-Hernandez ,
- Alba Deyanira Quiñonez López,
- César Augusto Zuluaga,
- Ángel Alberto García,
- Oscar Mauricio Muñoz-Velandia
Views0ABSTRACT
Objective:
To determine the concordance of mortality risk classification through the use of the Pediatric Index of Mortality (PIM) 2 and 3.
Methods:
Through a retrospective cohort, we evaluated patients admitted to the pediatric intensive care unit between April 2016 and December 2018. We calculated the mortality risk with the PIM 2 and 3. Analyses were carried out to determine the concordance between the risk classification obtained with both scales using unweighted and linearly weighted kappa.
Results:
A total of 722 subjects were included, and 66.6% had a chronic condition. The overall mortality was 3.7%. The global kappa concordance coefficient for classifying patients according to risk with the PIM 2 and 3 was moderate at 0.48 (95%CI 0.43 – 0.53). After linear weighting, concordance was substantial at 0.64 (95%CI 0.59 – 0.69). For cardiac surgery patients, concordance for risk classification was fair at 0.30 (95%CI 0.21 – 0.39), and after linear weighting, concordance was only moderate at 0.49 (95%CI 0.39 – 0.59). The PIM 3 assigned a lower risk than the PIM 2 in 44.8% of patients in this subgroup.
Conclusion:
Our study proves that the PIM 2 and 3 are not clinically equivalent and should not be used interchangeably for quality evaluation across pediatric intensive care units. Validation studies must be performed before using the PIM 2 or PIM 3 in specific settings.
Keywords:Cardiac surgeryInfant, newbornIntensive care units, pediatricMortalityPediatric Index of MortalitySee more - Daniela Patino-Hernandez
-
Review Article
Oxidative stress and decreased tissue HSP70 are involved in the genesis of sepsis: HSP70 as a therapeutic target
Rev Bras Ter Intensiva. 2020;32(4):585-591
Abstract
Review ArticleOxidative stress and decreased tissue HSP70 are involved in the genesis of sepsis: HSP70 as a therapeutic target
Rev Bras Ter Intensiva. 2020;32(4):585-591
DOI 10.5935/0103-507X.20200084
Views0See moreAbstract
Sepsis is a systemic infection that causes multiple organ dysfunction. HSP70 is a protein responsive to cell stress, in particular oxidative stress. Therefore, this literature review sought to investigate the roles of HSP70 and oxidative stress in the pathophysiology of sepsis and the possibility of HSP70 as a therapeutic target. HSP70 exerts a protective effect when located in cells (iHSP70), and its decrease, as well as its increase in the extracellular environment (eHSP70), under oxidative stress is a biomarker of sepsis severity. In addition, therapies that increase iHSP70 and treatment with HSP70 promote sepsis improvement.
Views0Abstract
Review ArticleOxidative stress and decreased tissue HSP70 are involved in the genesis of sepsis: HSP70 as a therapeutic target
Rev Bras Ter Intensiva. 2020;32(4):585-591
DOI 10.5935/0103-507X.20200084
Views0See moreAbstract
Sepsis is a systemic infection that causes multiple organ dysfunction. HSP70 is a protein responsive to cell stress, in particular oxidative stress. Therefore, this literature review sought to investigate the roles of HSP70 and oxidative stress in the pathophysiology of sepsis and the possibility of HSP70 as a therapeutic target. HSP70 exerts a protective effect when located in cells (iHSP70), and its decrease, as well as its increase in the extracellular environment (eHSP70), under oxidative stress is a biomarker of sepsis severity. In addition, therapies that increase iHSP70 and treatment with HSP70 promote sepsis improvement.
-
Review Article
Efficacy and safety of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage: a systematic review
- Alex Goes Santos-Teles ,
- Clara Ramalho,
- João Gabriel Rosa Ramos,
- Rogério da Hora Passos,
- André Gobatto, [ … ],
- Juliana Ribeiro Caldas
Abstract
Review ArticleEfficacy and safety of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage: a systematic review
Rev Bras Ter Intensiva. 2020;32(4):592-602
DOI 10.5935/0103-507X.20200097
- Alex Goes Santos-Teles ,
- Clara Ramalho,
- João Gabriel Rosa Ramos,
- Rogério da Hora Passos,
- André Gobatto,
- Suzete Farias,
- Paulo Benígno Pena Batista,
- Juliana Ribeiro Caldas
Views0See moreABSTRACT
Objective:
To systematically review the current evidence on the efficacy of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage.
Methods:
The Pubmed®, Cochrane and Embase databases were screened for articles published from April 2001 to February 2019. Two independent reviewers performed the methodological quality screening and data extraction of the studies.
Results:
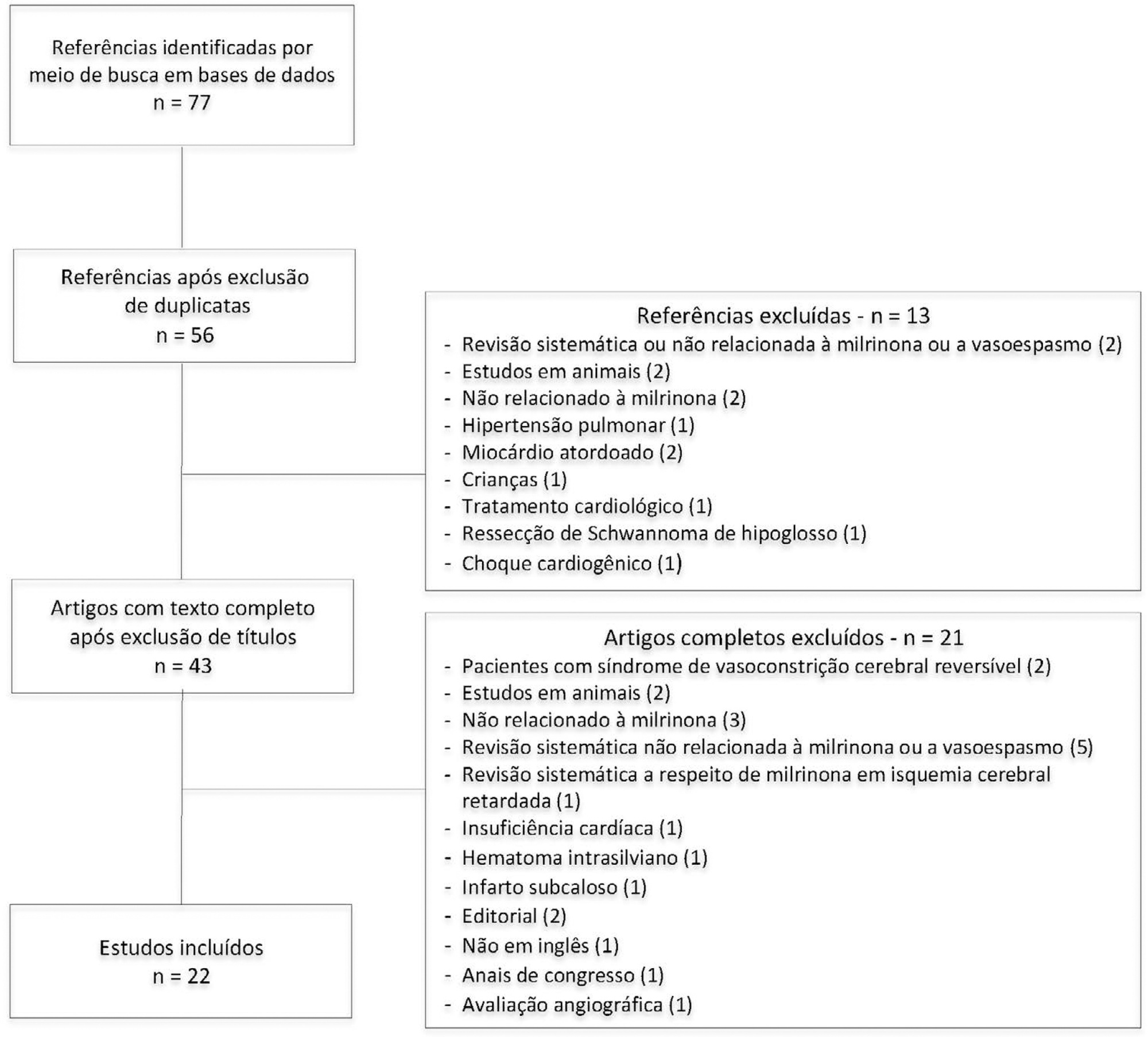
Twenty-two studies were found to be relevant, and only one of these was a randomized control trial. Studies showed marked heterogeneity and weaknesses in key methodological criteria. Most patients presented with moderate to severe vasospasm. Angiography was the main method of diagnosing vasospasm. Intra-arterial administration of milrinone was performed in three studies, intravenous administration was performed in nine studies, and both routes of administration in six studies; the intrathecal route was used in two studies, the cisternal route in one study and endovascular administration in one study. The side effects of milrinone were described in six studies. Twenty-one studies indicated resolution of vasospasm.
Conclusion:
The current evidence indicates that milrinone may have a role in treatment of vasospasm after aneurysmal subarachnoid hemorrhage. However, only one randomized control trial was performed, with a low quality level. Our findings indicate the need for future randomized control trials with patient-centered outcomes to provide definitive recommendations.
Views0Abstract
Review ArticleEfficacy and safety of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage: a systematic review
Rev Bras Ter Intensiva. 2020;32(4):592-602
DOI 10.5935/0103-507X.20200097
- Alex Goes Santos-Teles ,
- Clara Ramalho,
- João Gabriel Rosa Ramos,
- Rogério da Hora Passos,
- André Gobatto,
- Suzete Farias,
- Paulo Benígno Pena Batista,
- Juliana Ribeiro Caldas
Views0See moreABSTRACT
Objective:
To systematically review the current evidence on the efficacy of milrinone in the treatment of cerebral vasospasm after subarachnoid hemorrhage.
Methods:
The Pubmed®, Cochrane and Embase databases were screened for articles published from April 2001 to February 2019. Two independent reviewers performed the methodological quality screening and data extraction of the studies.
Results:
Twenty-two studies were found to be relevant, and only one of these was a randomized control trial. Studies showed marked heterogeneity and weaknesses in key methodological criteria. Most patients presented with moderate to severe vasospasm. Angiography was the main method of diagnosing vasospasm. Intra-arterial administration of milrinone was performed in three studies, intravenous administration was performed in nine studies, and both routes of administration in six studies; the intrathecal route was used in two studies, the cisternal route in one study and endovascular administration in one study. The side effects of milrinone were described in six studies. Twenty-one studies indicated resolution of vasospasm.
Conclusion:
The current evidence indicates that milrinone may have a role in treatment of vasospasm after aneurysmal subarachnoid hemorrhage. However, only one randomized control trial was performed, with a low quality level. Our findings indicate the need for future randomized control trials with patient-centered outcomes to provide definitive recommendations.
- Alex Goes Santos-Teles
-
Case Report
Cerebral hemorrhage during the active phase of SARS-CoV-2 infection in a patient with amyloid angiopathy: case report
- Amanda Ayako Minemura Ordinola,
- Samir Sari Osmar,
- Victor Hugo Rocha Marussi,
- Salomón Soriano Ordinola Rojas ,
- Alex Machado Baeta, [ … ],
- Viviane Cordeiro Veiga
Abstract
Case ReportCerebral hemorrhage during the active phase of SARS-CoV-2 infection in a patient with amyloid angiopathy: case report
Rev Bras Ter Intensiva. 2020;32(4):603-605
DOI 10.5935/0103-507X.20200098
- Amanda Ayako Minemura Ordinola,
- Samir Sari Osmar,
- Victor Hugo Rocha Marussi,
- Salomón Soriano Ordinola Rojas ,
- Alex Machado Baeta,
- Feres Eduardo Chaddad Neto,
- Viviane Cordeiro Veiga
Views0ABSTRACT
The neurological changes associated with COVID-19 have been frequently described, especially in cases of greater severity, and are related to multifactorial causes, such as endothelial dysfunction, inflammatory mediator release (cytokine storm), endothelial dysfunction and hypoxemia. We report the case of a female patient, 88 years old, with cerebral hemorrhage associated with amyloid angiopathy in the context of SARS-CoV-2 infection.
Keywords:Cerebral amyloid angiopathyCerebral hemorrhageCoronavirus infectionsCOVID-19Critical careIntensive care unitsSARS-CoV-2See moreViews0Abstract
Case ReportCerebral hemorrhage during the active phase of SARS-CoV-2 infection in a patient with amyloid angiopathy: case report
Rev Bras Ter Intensiva. 2020;32(4):603-605
DOI 10.5935/0103-507X.20200098
- Amanda Ayako Minemura Ordinola,
- Samir Sari Osmar,
- Victor Hugo Rocha Marussi,
- Salomón Soriano Ordinola Rojas ,
- Alex Machado Baeta,
- Feres Eduardo Chaddad Neto,
- Viviane Cordeiro Veiga
Views0ABSTRACT
The neurological changes associated with COVID-19 have been frequently described, especially in cases of greater severity, and are related to multifactorial causes, such as endothelial dysfunction, inflammatory mediator release (cytokine storm), endothelial dysfunction and hypoxemia. We report the case of a female patient, 88 years old, with cerebral hemorrhage associated with amyloid angiopathy in the context of SARS-CoV-2 infection.
Keywords:Cerebral amyloid angiopathyCerebral hemorrhageCoronavirus infectionsCOVID-19Critical careIntensive care unitsSARS-CoV-2See more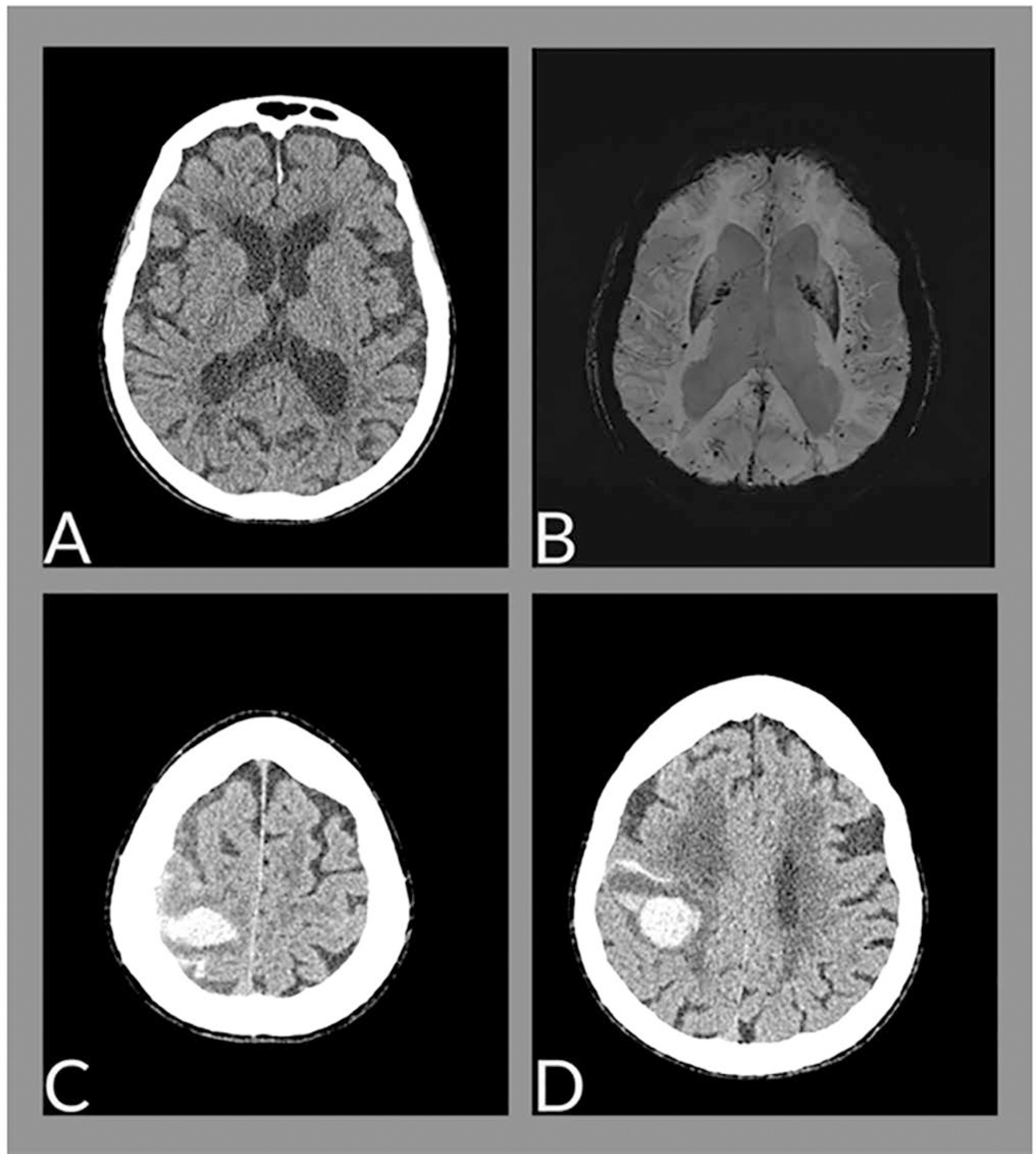
-
Case Report
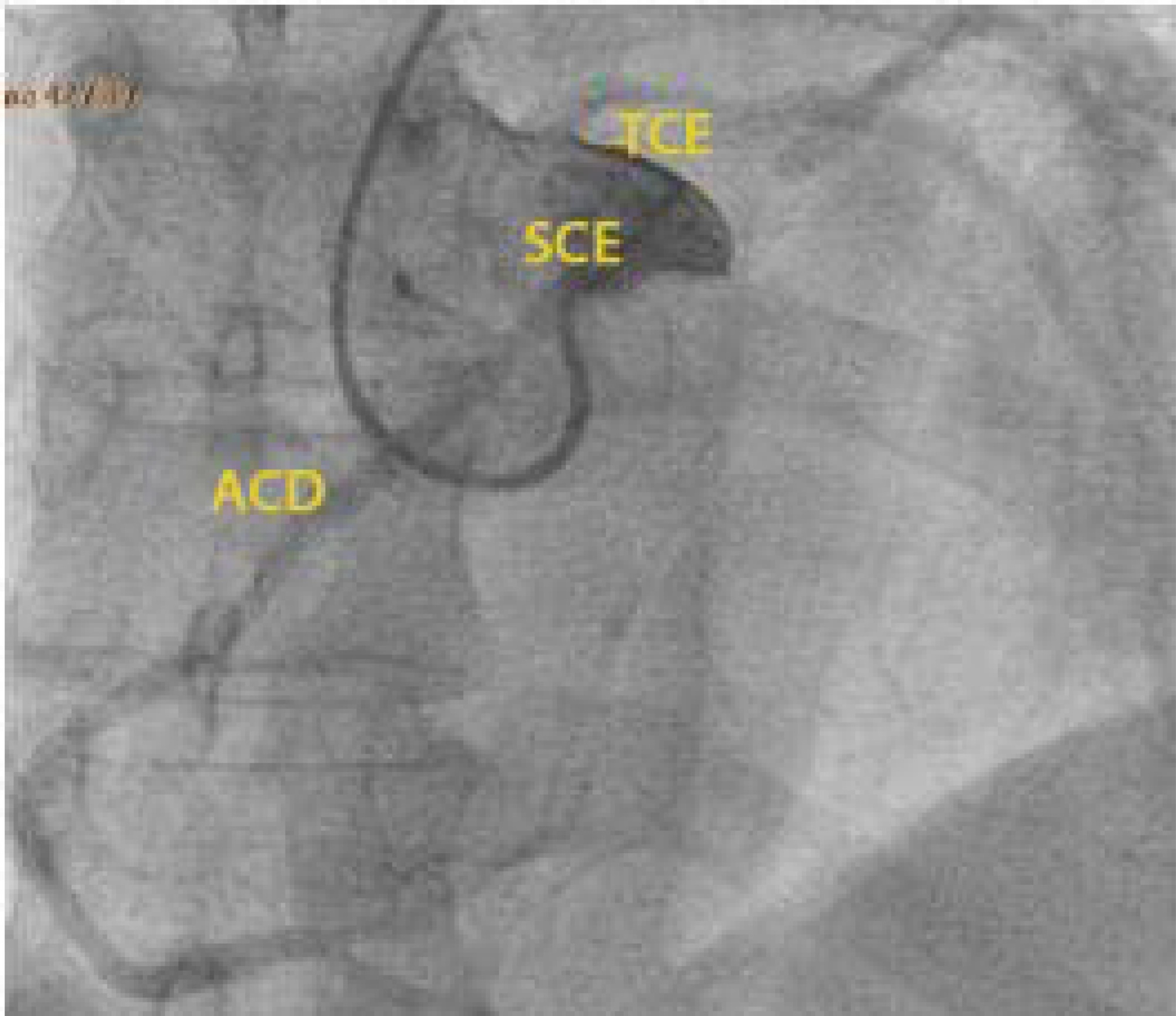
Cardiac arrest due to an anomalous aortic origin of a coronary artery: are older patients really safe?
Rev Bras Ter Intensiva. 2020;32(4):606-610
Abstract
Case ReportCardiac arrest due to an anomalous aortic origin of a coronary artery: are older patients really safe?
Rev Bras Ter Intensiva. 2020;32(4):606-610
DOI 10.5935/0103-507X.20200099
Views0See moreABSTRACT
The authors report a rare case of successful Advanced Life Support in the context of cardiac arrest due to the presence of an anomalous aortic origin of the right coronary artery in a 49-year-old patient. The patient was admitted due to chest pain and dyspnea, with rapid evolution of pulseless ventricular tachycardia and cardiopulmonary arrest. Acute myocardial infarction was considered, and in the absence of a hemodynamic laboratory in the hospital, thrombolysis was performed. Subsequently, coronary angiography revealed no angiographic lesions in the coronary arteries and an anomalous right coronary artery originating from the opposite sinus of Valsalva. Coronary computed tomography angiography confirmed this finding and determined the course between the pulmonary artery and the aorta. The patient underwent cardiac surgery with a bypass graft to the right coronary artery, with no recurrent episodes of arrythmia.
Views0Abstract
Case ReportCardiac arrest due to an anomalous aortic origin of a coronary artery: are older patients really safe?
Rev Bras Ter Intensiva. 2020;32(4):606-610
DOI 10.5935/0103-507X.20200099
Views0See moreABSTRACT
The authors report a rare case of successful Advanced Life Support in the context of cardiac arrest due to the presence of an anomalous aortic origin of the right coronary artery in a 49-year-old patient. The patient was admitted due to chest pain and dyspnea, with rapid evolution of pulseless ventricular tachycardia and cardiopulmonary arrest. Acute myocardial infarction was considered, and in the absence of a hemodynamic laboratory in the hospital, thrombolysis was performed. Subsequently, coronary angiography revealed no angiographic lesions in the coronary arteries and an anomalous right coronary artery originating from the opposite sinus of Valsalva. Coronary computed tomography angiography confirmed this finding and determined the course between the pulmonary artery and the aorta. The patient underwent cardiac surgery with a bypass graft to the right coronary artery, with no recurrent episodes of arrythmia.
-
Letter to the Editor
To: Complementary of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
Rev Bras Ter Intensiva. 2020;32(4):611-612
Abstract
Letter to the EditorTo: Complementary of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
Rev Bras Ter Intensiva. 2020;32(4):611-612
DOI 10.5935/0103-507X.20200100
Views0To the Editor We have read the article “Complementarity of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients” by Oliveira et al.() with great interest. The authors found excellent agreement between the modified Nutrition Risk in the Critically Ill (NUTRIC) score and the NUTRIC […]See moreViews0Abstract
Letter to the EditorTo: Complementary of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients
Rev Bras Ter Intensiva. 2020;32(4):611-612
DOI 10.5935/0103-507X.20200100
Views0To the Editor We have read the article “Complementarity of modified NUTRIC score with or without C-reactive protein and subjective global assessment in predicting mortality in critically ill patients” by Oliveira et al.() with great interest. The authors found excellent agreement between the modified Nutrition Risk in the Critically Ill (NUTRIC) score and the NUTRIC […]See more -
Author’s Response
Reply to: Adequacy of enteral nutrition support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
- Cecília Flávia Lopes Couto,
- Ângela Dariano,
- Cassiano Texeira,
- Carolina Hauber da Silva,
- Anelise Bertotti Torbes, [ … ],
- Gilberto Friedman
Abstract
Author’s ResponseReply to: Adequacy of enteral nutrition support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2020;32(4):613-613
DOI 10.5935/0103-507X.20200101
- Cecília Flávia Lopes Couto,
- Ângela Dariano,
- Cassiano Texeira,
- Carolina Hauber da Silva,
- Anelise Bertotti Torbes,
- Gilberto Friedman
Views0To the Editor In our study “Adequacy of enteral nutrition support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study”() the sample size was calculated to assess the short-term effects, and in this sense, it is not a pilot study. However, we had no information […]See moreViews0Abstract
Author’s ResponseReply to: Adequacy of enteral nutrition support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2020;32(4):613-613
DOI 10.5935/0103-507X.20200101
- Cecília Flávia Lopes Couto,
- Ângela Dariano,
- Cassiano Texeira,
- Carolina Hauber da Silva,
- Anelise Bertotti Torbes,
- Gilberto Friedman
Views0To the Editor In our study “Adequacy of enteral nutrition support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study”() the sample size was calculated to assess the short-term effects, and in this sense, it is not a pilot study. However, we had no information […]See more -
Erratum
Erratum
Rev Bras Ter Intensiva. 2020;32(4):614-614
Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(4):614-614
DOI 10.5935/0103-507X.20200102
Views0In the article Prevalence of burnout among intensive care physicians: a systematic review, with DOI number: 10.5935/0103-507X.20200076, published in the journal Revista Brasileira de Terapia Intensiva, 32(3):458-467, on page 458:Where it read:[…]See moreViews0Abstract
ErratumErratum
Rev Bras Ter Intensiva. 2020;32(4):614-614
DOI 10.5935/0103-507X.20200102
Views0In the article Prevalence of burnout among intensive care physicians: a systematic review, with DOI number: 10.5935/0103-507X.20200076, published in the journal Revista Brasileira de Terapia Intensiva, 32(3):458-467, on page 458:Where it read:[…]See more
Volume Articles - Critical Care Science (CCS)
