
You searched for:"Helio Penna Guimaraes"
We found (25) results for your search.-
Special Article
The II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
- Maicon Falavigna
 ,
, - Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
Special ArticleThe II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
Crit Care Sci. 2023;35(3):243-255
DOI 10.5935/2965-2774.20230136-pt
- Maicon Falavigna ,
- Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Felipe Dal-Pizzol ,
- Rosemeri Maurici da Silva ,
- Luciano César Pontes de Azevedo ,
- Maria Beatriz Souza Dias,
- José Luiz Gomes do Amaral ,
- Gilson Pires Dorneles ,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- Flávia Ribeiro Machado ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Suena Medeiros Parahiba ,
- Regis Goulart Rosa ,
- Vania Cristina Canuto Santos ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Cinara Stein ,
- Carlos Roberto Ribeiro de Carvalho
Views22ABSTRACT
Objective:
To update the recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
Experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
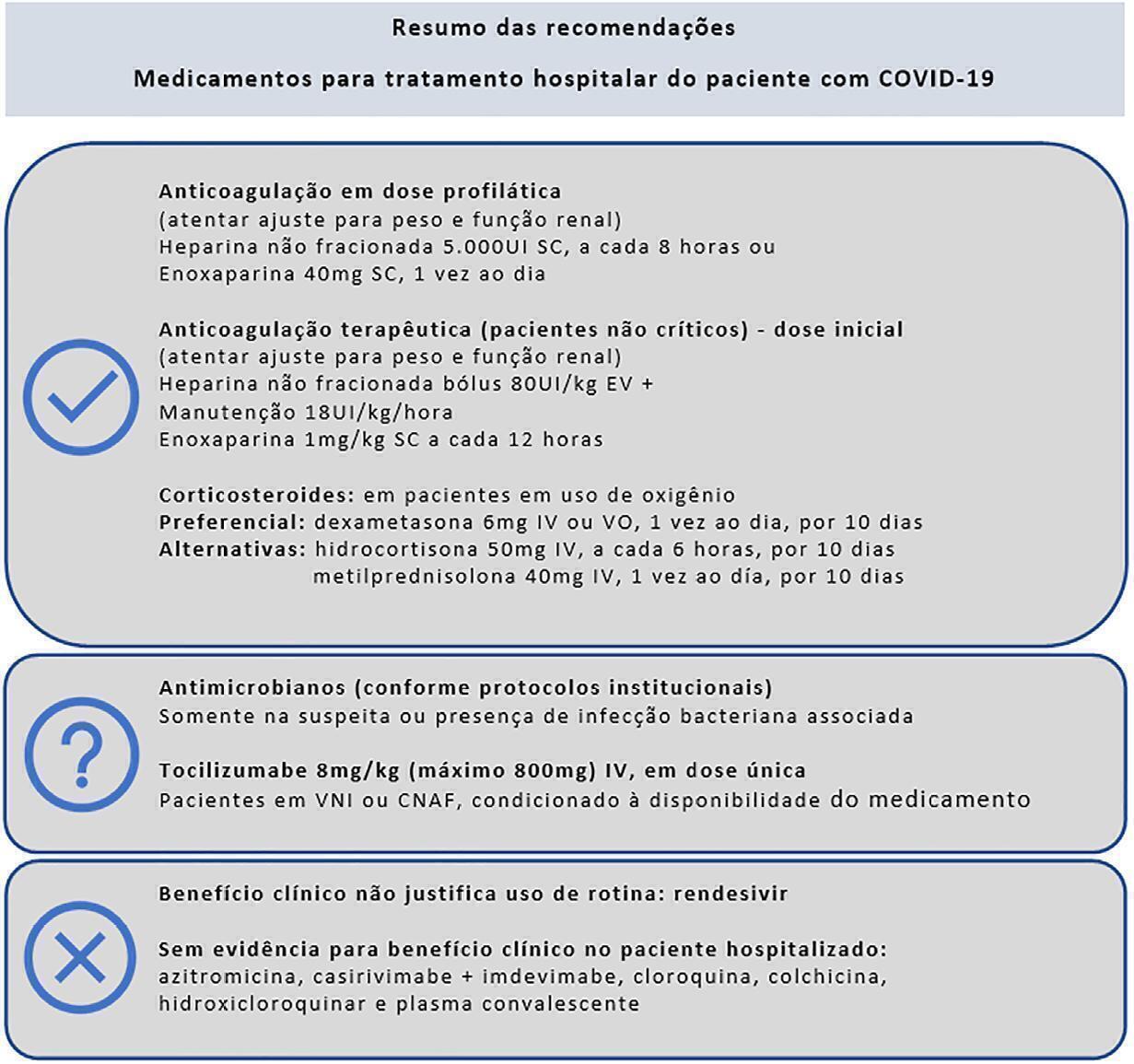
Twenty-one recommendations were generated, including strong recommendations for the use of corticosteroids in patients using supplemental oxygen and conditional recommendations for the use of tocilizumab and baricitinib for patients on supplemental oxygen or on noninvasive ventilation and anticoagulants to prevent thromboembolism. Due to suspension of use authorization, it was not possible to make recommendations regarding the use of casirivimab + imdevimab. Strong recommendations against the use of azithromycin in patients without suspected bacterial infection, hydroxychloroquine, convalescent plasma, colchicine, and lopinavir + ritonavir and conditional recommendations against the use of ivermectin and remdesivir were made.
Conclusion:
New recommendations for the treatment of hospitalized patients with COVID-19 were generated, such as those for tocilizumab and baricitinib. Corticosteroids and prophylaxis for thromboembolism are still recommended, the latter with conditional recommendation. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and to promote resource economy.
Keywords:BrazilCoronavirus infectionsCOVID-19COVID-19/drug therapyHealth planning guidelinesSARS-CoV-2See moreViews22

Abstract
Special ArticleThe II Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19 Joint Guidelines of the Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia and Sociedade Brasileira de Reumatologia
Crit Care Sci. 2023;35(3):243-255
DOI 10.5935/2965-2774.20230136-pt
- Maicon Falavigna ,
- Cintia Laura Pereira de Araujo ,
- Alexandre Naime Barbosa ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Felipe Dal-Pizzol ,
- Rosemeri Maurici da Silva ,
- Luciano César Pontes de Azevedo ,
- Maria Beatriz Souza Dias,
- José Luiz Gomes do Amaral ,
- Gilson Pires Dorneles ,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- Flávia Ribeiro Machado ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Suena Medeiros Parahiba ,
- Regis Goulart Rosa ,
- Vania Cristina Canuto Santos ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Cinara Stein ,
- Carlos Roberto Ribeiro de Carvalho
Views22ABSTRACT
Objective:
To update the recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
Experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Twenty-one recommendations were generated, including strong recommendations for the use of corticosteroids in patients using supplemental oxygen and conditional recommendations for the use of tocilizumab and baricitinib for patients on supplemental oxygen or on noninvasive ventilation and anticoagulants to prevent thromboembolism. Due to suspension of use authorization, it was not possible to make recommendations regarding the use of casirivimab + imdevimab. Strong recommendations against the use of azithromycin in patients without suspected bacterial infection, hydroxychloroquine, convalescent plasma, colchicine, and lopinavir + ritonavir and conditional recommendations against the use of ivermectin and remdesivir were made.
Conclusion:
New recommendations for the treatment of hospitalized patients with COVID-19 were generated, such as those for tocilizumab and baricitinib. Corticosteroids and prophylaxis for thromboembolism are still recommended, the latter with conditional recommendation. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and to promote resource economy.
Keywords:BrazilCoronavirus infectionsCOVID-19COVID-19/drug therapyHealth planning guidelinesSARS-CoV-2See more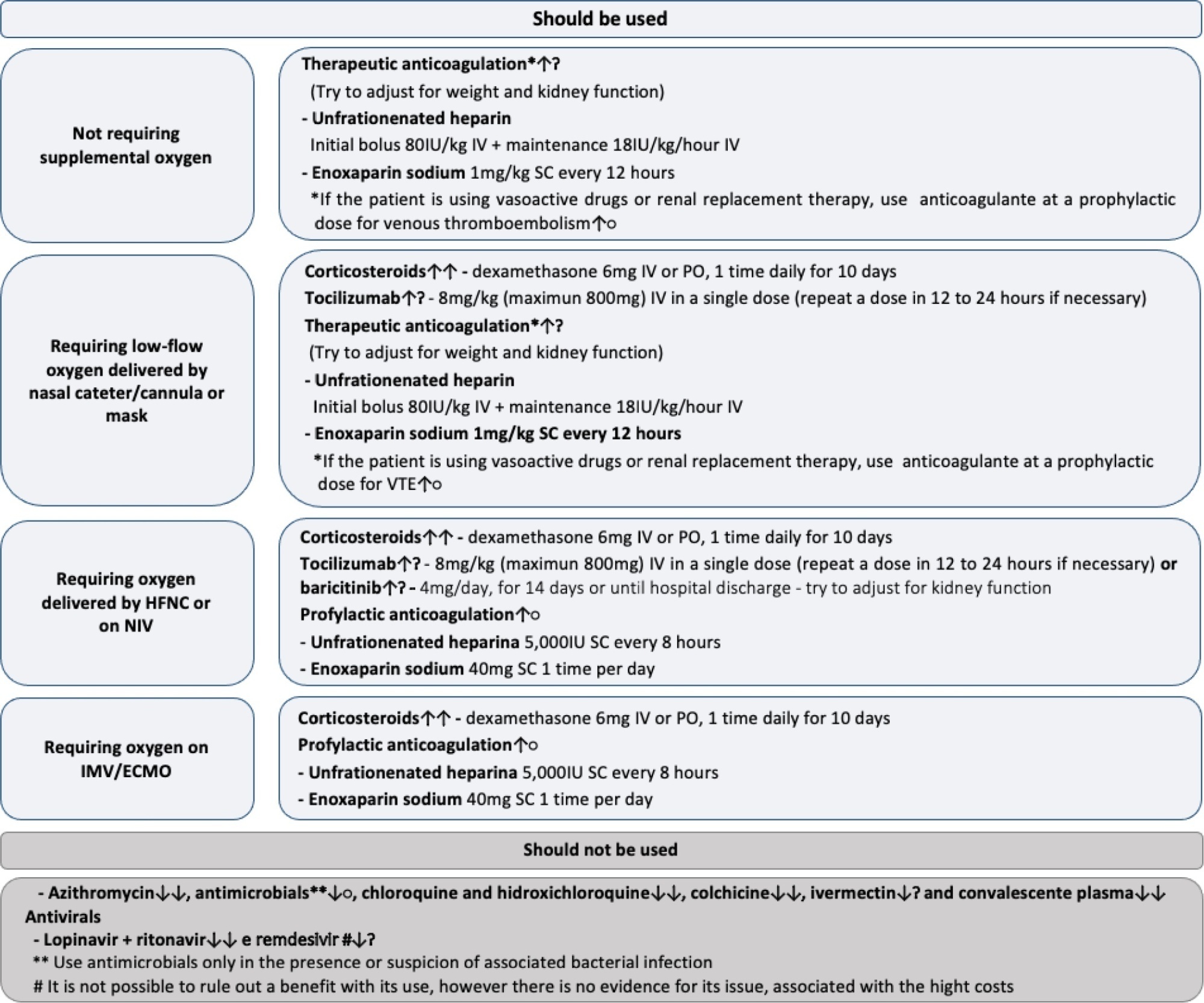
- Maicon Falavigna
-
Original Article
A nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa , [ … ],
- Ricardo Luiz Cordioli
Abstract
Original ArticleA nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa ,
- Ricardo Luiz Cordioli
Views1ABSTRACT
Objective:
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
Methods:
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Results:
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 – 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 – 3) versus 5 (2 – 24) hours; p < 0.001].
Conclusion:
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Keywords:BrazilCoronavirus infectionsCOVID-19Emergency servicehospitalHospital administrationIntensive care unitsPandemicsPhysiciansPractice patternsSurveys and questionnairesSee moreViews1Abstract
Original ArticleA nationwide survey on health resources and clinical practices during the early COVID-19 pandemic in Brazil
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
- Pedro Paulo Zanella do Amaral Campos ,
- Guilherme Martins de Souza ,
- Thais Midega ,
- Hélio Penna Guimarães ,
- Thiago Domingos Corrêa ,
- Ricardo Luiz Cordioli
Views1ABSTRACT
Objective:
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
Methods:
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Results:
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 – 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 – 3) versus 5 (2 – 24) hours; p < 0.001].
Conclusion:
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Keywords:BrazilCoronavirus infectionsCOVID-19Emergency servicehospitalHospital administrationIntensive care unitsPandemicsPhysiciansPractice patternsSurveys and questionnairesSee more - Pedro Paulo Zanella do Amaral Campos
-
Special Article
Brazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
- Maicon Falavigna ,
- Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
Special ArticleBrazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
Rev Bras Ter Intensiva. 2022;34(1):1-12
DOI 10.5935/0103-507X.20220001-en
- Maicon Falavigna ,
- Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Clóvis Arns da Cunha ,
- Felipe Dal-Pizzol ,
- Maria Beatriz Souza Dias,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- José Tadeu Monteiro ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Clementina Corah Lucas Prado,
- Vania Cristina Canuto Santos ,
- Rosemeri Maurici da Silva ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ávila Teixeira Vidal ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Flávia Ribeiro Machado ,
- Carlos Roberto Ribeiro de Carvalho
Views7See moreABSTRACT
Objective:
Several therapies are being used or proposed for COVID-19, and many lack appropriate evaluations of their effectiveness and safety. The purpose of this document is to develop recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
A group of 27 experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Sixteen recommendations were generated. They include strong recommendations for the use of corticosteroids in patients using supplemental oxygen, the use of anticoagulants at prophylactic doses to prevent thromboembolism and the nonuse of antibiotics in patients without suspected bacterial infection. It was not possible to make a recommendation regarding the use of tocilizumab in patients hospitalized with COVID-19 using oxygen due to uncertainties regarding the availability of and access to the drug. Strong recommendations against the use of hydroxychloroquine, convalescent plasma, colchicine, lopinavir + ritonavir and antibiotics in patients without suspected bacterial infection and also conditional recommendations against the use of casirivimab + imdevimab, ivermectin and rendesivir were made.
Conclusion:
To date, few therapies have proven effective in the treatment of hospitalized patients with COVID-19, and only corticosteroids and prophylaxis for thromboembolism are recommended. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and promote economical resource use.
Views7Abstract
Special ArticleBrazilian Guidelines for the pharmacological treatment of patients hospitalized with COVID-19: Joint guideline of Associação Brasileira de Medicina de Emergência, Associação de Medicina Intensiva Brasileira, Associação Médica Brasileira, Sociedade Brasileira de Angiologia e Cirurgia Vascular, Sociedade Brasileira de Infectologia, Sociedade Brasileira de Pneumologia e Tisiologia, Sociedade Brasileira de Reumatologia
Rev Bras Ter Intensiva. 2022;34(1):1-12
DOI 10.5935/0103-507X.20220001-en
- Maicon Falavigna ,
- Cinara Stein ,
- José Luiz Gomes do Amaral ,
- Luciano Cesar Pontes de Azevedo ,
- Karlyse Claudino Belli ,
- Verônica Colpani ,
- Clóvis Arns da Cunha ,
- Felipe Dal-Pizzol ,
- Maria Beatriz Souza Dias,
- Juliana Carvalho Ferreira ,
- Ana Paula da Rocha Freitas,
- Débora Dalmas Gräf ,
- Hélio Penna Guimarães ,
- Suzana Margareth Ajeje Lobo ,
- José Tadeu Monteiro ,
- Michelle Silva Nunes ,
- Maura Salaroli de Oliveira ,
- Clementina Corah Lucas Prado,
- Vania Cristina Canuto Santos ,
- Rosemeri Maurici da Silva ,
- Marcone Lima Sobreira ,
- Viviane Cordeiro Veiga ,
- Ávila Teixeira Vidal ,
- Ricardo Machado Xavier ,
- Alexandre Prehn Zavascki ,
- Flávia Ribeiro Machado ,
- Carlos Roberto Ribeiro de Carvalho
Views7See moreABSTRACT
Objective:
Several therapies are being used or proposed for COVID-19, and many lack appropriate evaluations of their effectiveness and safety. The purpose of this document is to develop recommendations to support decisions regarding the pharmacological treatment of patients hospitalized with COVID-19 in Brazil.
Methods:
A group of 27 experts, including representatives of the Ministry of Health and methodologists, created this guideline. The method used for the rapid development of guidelines was based on the adoption and/or adaptation of existing international guidelines (GRADE ADOLOPMENT) and supported by the e-COVID-19 RecMap platform. The quality of the evidence and the preparation of the recommendations followed the GRADE method.
Results:
Sixteen recommendations were generated. They include strong recommendations for the use of corticosteroids in patients using supplemental oxygen, the use of anticoagulants at prophylactic doses to prevent thromboembolism and the nonuse of antibiotics in patients without suspected bacterial infection. It was not possible to make a recommendation regarding the use of tocilizumab in patients hospitalized with COVID-19 using oxygen due to uncertainties regarding the availability of and access to the drug. Strong recommendations against the use of hydroxychloroquine, convalescent plasma, colchicine, lopinavir + ritonavir and antibiotics in patients without suspected bacterial infection and also conditional recommendations against the use of casirivimab + imdevimab, ivermectin and rendesivir were made.
Conclusion:
To date, few therapies have proven effective in the treatment of hospitalized patients with COVID-19, and only corticosteroids and prophylaxis for thromboembolism are recommended. Several drugs were considered ineffective and should not be used to provide the best treatment according to the principles of evidence-based medicine and promote economical resource use.
- Maicon Falavigna
-
Original Article
Resuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti , [ … ],
- Flavia Ribeiro Machado
Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
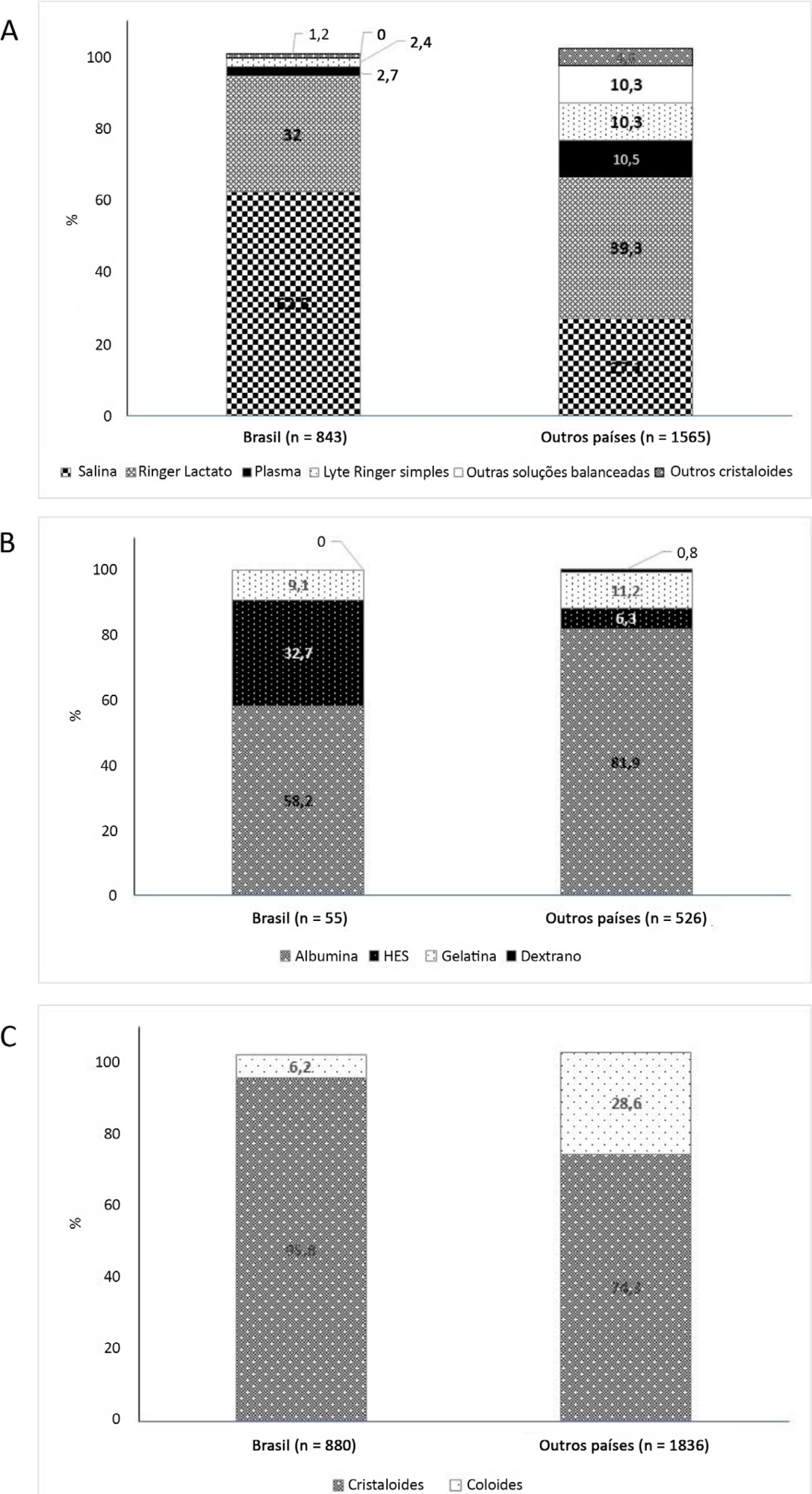
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
Views1Abstract
Original ArticleResuscitation fluid practices in Brazilian intensive care units: a secondary analysis of Fluid-TRIPS
Rev Bras Ter Intensiva. 2021;33(2):206-218
DOI 10.5935/0103-507X.20210028
- Flavio Geraldo Rezende de Freitas ,
- Naomi Hammond,
- Yang Li,
- Luciano Cesar Pontes de Azevedo,
- Alexandre Biasi Cavalcanti ,
- Leandro Taniguchi ,
- André Gobatto,
- André Miguel Japiassú ,
- Antonio Tonete Bafi,
- Bruno Franco Mazza,
- Danilo Teixeira Noritomi,
- Felipe Dal-Pizzol ,
- Fernando Bozza ,
- Jorge Ibrahin Figueira Salluh ,
- Glauco Adrieno Westphal ,
- Márcio Soares ,
- Murillo Santucci César de Assunção ,
- Thiago Lisboa,
- Suzana Margarete Ajeje Lobo,
- Achilles Rohlfs Barbosa,
- Adriana Fonseca Ventura,
- Ailson Faria de Souza,
- Alexandre Francisco Silva,
- Alexandre Toledo,
- Aline Reis,
- Allan Cembranel,
- Alvaro Rea Neto,
- Ana Lúcia Gut,
- Ana Patricia Pierre Justo,
- Ana Paula Santos,
- André Campos D. de Albuquerque,
- André Scazufka,
- Antonio Babo Rodrigues,
- Bruno Bonaccorsi Fernandino,
- Bruno Goncalves Silva,
- Bruno Sarno Vidal,
- Bruno Valle Pinheiro,
- Bruno Vilela Costa Pinto,
- Carlos Augusto Ramos Feijo,
- Carlos de Abreu Filho,
- Carlos Eduardo da Costa Nunes Bosso,
- Carlos Eduardo Nassif Moreira,
- Carlos Henrique Ferreira Ramos,
- Carmen Tavares,
- Cidamaiá Arantes,
- Cintia Grion,
- Ciro Leite Mendes,
- Claudio Kmohan,
- Claudio Piras,
- Cristine Pilati Pileggi Castro,
- Cyntia Lins,
- Daniel Beraldo,
- Daniel Fontes,
- Daniela Boni,
- Débora Castiglioni,
- Denise de Moraes Paisani,
- Durval Ferreira Fonseca Pedroso,
- Ederson Roberto Mattos,
- Edgar de Brito Sobrinho,
- Edgar M. V. Troncoso,
- Edison Moraes Rodrigues Filho,
- Eduardo Enrico Ferrari Nogueira,
- Eduardo Leme Ferreira,
- Eduardo Souza Pacheco,
- Euzebio Jodar,
- Evandro L. A. Ferreira,
- Fabiana Fernandes de Araujo,
- Fabiana Schuelter Trevisol,
- Fábio Ferreira Amorim,
- Fabio Poianas Giannini,
- Fabrício Primitivo Matos Santos,
- Fátima Buarque,
- Felipe Gallego Lima,
- Fernando Antonio Alvares da Costa,
- Fernando Cesar dos Anjos Sad,
- Fernando G. Aranha,
- Fernando Ganem,
- Flavio Callil,
- Francisco Flávio Costa Filho,
- Frederico Toledo Campo Dall´Arto,
- Geovani Moreno,
- Gilberto Friedman,
- Giulliana Martines Moralez,
- Guilherme Abdalla da Silva,
- Guilherme Costa,
- Guilherme Silva Cavalcanti,
- Guilherme Silva Cavalcanti,
- Gustavo Navarro Betônico,
- Gustavo Navarro Betônico,
- Hélder Reis,
- Helia Beatriz N. Araujo,
- Helio Anjos Hortiz Júnior,
- Helio Penna Guimaraes,
- Hugo Urbano,
- Israel Maia,
- Ivan Lopes Santiago Filho,
- Jamil Farhat Júnior,
- Janu Rangel Alvarez,
- Joel Tavares Passos,
- Jorge Eduardo da Rocha Paranhos,
- José Aurelio Marques,
- José Gonçalves Moreira Filho,
- Jose Neto Andrade,
- José Onofre de C Sobrinho,
- Jose Terceiro de Paiva Bezerra,
- Juliana Apolônio Alves,
- Juliana Ferreira,
- Jussara Gomes,
- Karina Midori Sato,
- Karine Gerent,
- Kathia Margarida Costa Teixeira,
- Katia Aparecida Pessoa Conde,
- Laércia Ferreira Martins,
- Lanese Figueirêdo,
- Leila Rezegue,
- Leonardo Tcherniacovsk,
- Leone Oliveira Ferraz,
- Liane Cavalcante,
- Ligia Rabelo,
- Lilian Miilher,
- Lisiane Garcia,
- Luana Tannous,
- Ludhmila Abrahão Hajjar,
- Luís Eduardo Miranda Paciência,
- Luiz Monteiro da Cruz Neto,
- Macia Valeria Bley,
- Marcelo Ferreira Sousa,
- Marcelo Lourencini Puga,
- Marcelo Luz Pereira Romano,
- Marciano Nobrega,
- Marcio Arbex,
- Márcio Leite Rodrigues,
- Márcio Osório Guerreiro,
- Marcone Rocha,
- Maria Angela Pangoni Alves,
- Maria Angela Pangoni Alves,
- Maria Doroti Rosa,
- Mariza D’Agostino Dias,
- Miquéias Martins,
- Mirella de Oliveira,
- Miriane Melo Silveira Moretti,
- Mirna Matsui,
- Octavio Messender,
- Orlando Luís de Andrade Santarém,
- Patricio Júnior Henrique da Silveira,
- Paula Frizera Vassallo,
- Paulo Antoniazzi,
- Paulo César Gottardo,
- Paulo Correia,
- Paulo Ferreira,
- Paulo Torres,
- Pedro Gabrile M. de Barros e Silva,
- Rafael Foernges,
- Rafael Gomes,
- Rafael Moraes,
- Raimundo Nonato filho,
- Renato Luis Borba,
- Renato V Gomes,
- Ricardo Cordioli,
- Ricardo Lima,
- Ricardo Pérez López,
- Ricardo Rath de Oliveira Gargioni,
- Richard Rosenblat,
- Roberta Machado de Souza,
- Roberto Almeida,
- Roberto Camargo Narciso,
- Roberto Marco,
- Roberto waltrick,
- Rodrigo Biondi,
- Rodrigo Figueiredo,
- Rodrigo Santana Dutra,
- Roseane Batista,
- Rouge Felipe,
- Rubens Sergio da Silva Franco,
- Sandra Houly,
- Sara Socorro Faria,
- Sergio Felix Pinto,
- Sergio Luzzi,
- Sergio Sant’ana,
- Sergio Sonego Fernandes,
- Sérgio Yamada,
- Sérgio Zajac,
- Sidiner Mesquita Vaz,
- Silvia Aparecida Bezerra Bezerra,
- Tatiana Bueno Tardivo Farhat,
- Thiago Martins Santos,
- Tiago Smith,
- Ulysses V. A. Silva,
- Valnei Bento Damasceno,
- Vandack Nobre,
- Vicente Cés de Souza Dantas,
- Vivian Menezes Irineu,
- Viviane Bogado,
- Wagner Nedel,
- Walther Campos Filho,
- Weidson Dantas,
- William Viana,
- Wilson de Oliveira Filho,
- Wilson Martins Delgadinho,
- Simon Finfer,
- Flavia Ribeiro Machado
Views1See moreAbstract
Objective:
To describe fluid resuscitation practices in Brazilian intensive care units and to compare them with those of other countries participating in the Fluid-TRIPS.
Methods:
This was a prospective, international, cross-sectional, observational study in a convenience sample of intensive care units in 27 countries (including Brazil) using the Fluid-TRIPS database compiled in 2014. We described the patterns of fluid resuscitation use in Brazil compared with those in other countries and identified the factors associated with fluid choice.
Results:
On the study day, 3,214 patients in Brazil and 3,493 patients in other countries were included, of whom 16.1% and 26.8% (p < 0.001) received fluids, respectively. The main indication for fluid resuscitation was impaired perfusion and/or low cardiac output (Brazil: 71.7% versus other countries: 56.4%, p < 0.001). In Brazil, the percentage of patients receiving crystalloid solutions was higher (97.7% versus 76.8%, p < 0.001), and 0.9% sodium chloride was the most commonly used crystalloid (62.5% versus 27.1%, p < 0.001). The multivariable analysis suggested that the albumin levels were associated with the use of both crystalloids and colloids, whereas the type of fluid prescriber was associated with crystalloid use only.
Conclusion:
Our results suggest that crystalloids are more frequently used than colloids for fluid resuscitation in Brazil, and this discrepancy in frequencies is higher than that in other countries. Sodium chloride (0.9%) was the crystalloid most commonly prescribed. Serum albumin levels and the type of fluid prescriber were the factors associated with the choice of crystalloids or colloids for fluid resuscitation.
- Flavio Geraldo Rezende de Freitas
-
Review Articles
Usefulness of Extended-FAST (EFAST-Extended Focused Assessment with Sonography for Trauma) in critical care setting
Rev Bras Ter Intensiva. 2010;22(3):291-299
Abstract
Review ArticlesUsefulness of Extended-FAST (EFAST-Extended Focused Assessment with Sonography for Trauma) in critical care setting
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
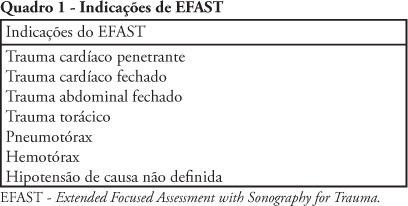
Views0See moreTrauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients’ management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.
Views0Abstract
Review ArticlesUsefulness of Extended-FAST (EFAST-Extended Focused Assessment with Sonography for Trauma) in critical care setting
Rev Bras Ter Intensiva. 2010;22(3):291-299
DOI 10.1590/S0103-507X2010000300012
Views0See moreTrauma is the leading cause of death in people below 45 years-old in Brazil, and responsible for one third of all intensive care unit admissions. The increasing knowledge on ultrasound diagnosis methods and its availability for life-threatening injuries (such as cardiac tamponade and abdominal cavity solid organs rupture leading to hemorrhagic shock) diagnosis and monitoring, lead to the development o the FAST (Focused Assessment with Sonography for Trauma) protocol, aimed to be used both in the emergency and intensive care unit settings. Due to its reproducibility, lack of radiation exposure, and bedside feasibility, this technology is being increasingly accepted. A new protocol extension, the Extended-FAST, provides valuable information for improved patients’ management, extending its availability from the abdominal conditions to other diagnosis such as hemothorax, pleural effusion and pneumothorax. We must underline that this technique is able to replace computed tomography and diagnostic peritoneal wash, and do not delay surgical procedure instead of perform this exam . Thus, its careful appraisal in connection with the clinical information should guide the therapeutic approaches, specially in inhospitable sites such as intensive care units in war zones, rural or distant places, were other imagery methods are not available.
-
Review Articles
Intensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
Abstract
Review ArticlesIntensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
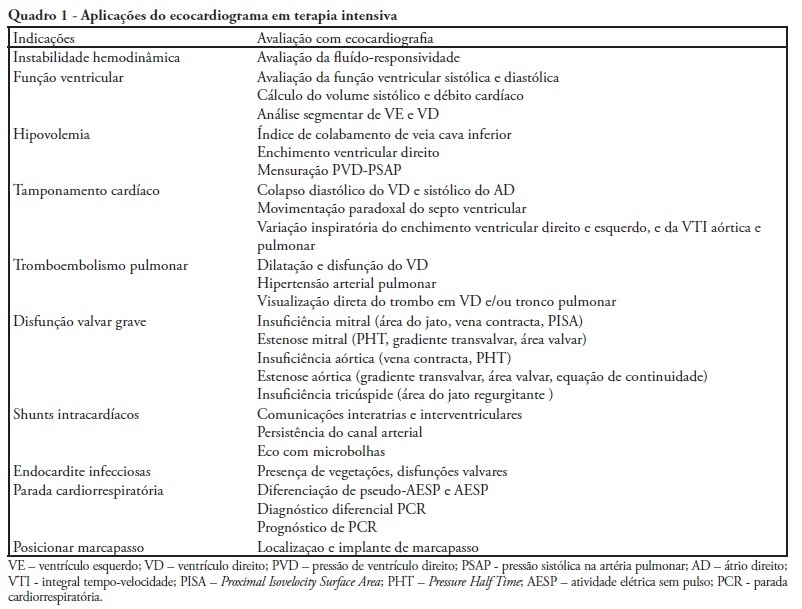
Views0See moreDuring the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
Views0Abstract
Review ArticlesIntensive care bedside echocardiography: true or a distant dream?
Rev Bras Ter Intensiva. 2009;21(4):437-445
DOI 10.1590/S0103-507X2009000400015
Views0See moreDuring the last few years, technological development and acquired experience advanced and the echocardiogram has become an important and useful tool in intensive care unit environment. Data obtained from semi quantitative Doppler echocardiography (transthoracic and transesophageal) evaluation has contributed to an appropriate patient monitoring and management. Echocardiography as a diagnostic, prognostic and monitoring method for fluid responsiveness assessment has become available nowadays since hand-carried ultrasound devices are portable and cheaper. Adequate training and development of appropriateness criteria for use of echocardiography in intensive care unit may lead to a standard use as a bedside tool.
-
Review Articles
Therapeutical hypothermia after cardiopulmonary resuscitation: evidences and practical issues
Rev Bras Ter Intensiva. 2009;21(1):65-71
Abstract
Review ArticlesTherapeutical hypothermia after cardiopulmonary resuscitation: evidences and practical issues
Rev Bras Ter Intensiva. 2009;21(1):65-71
DOI 10.1590/S0103-507X2009000100010
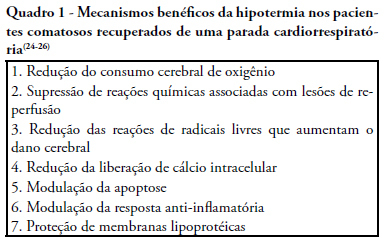
Views0See moreCardiac arrest survivors frequently suffer from ischemic brain injury associated with poor neurological outcome and death. Therapeutic hypothermia improves outcomes in comatose survivors after resuscitation from out-of-hospital cardiac arrest. Considering its formal recommendation as a therapy, post-return of spontaneous circulation after cardiac arrest, the objective of this study was to review the clinical aspects of therapeutic hypothermia. Non-systematic review of articles using the keywords “cardiac arrest, cardiopulmonary resuscitation, cooling, hypothermia, post resuscitation syndrome” in the Med-Line database was performed. References of these articles were also reviewed. Unconscious adult patients with spontaneous circulation after out-of-hospital ventricular fibrillation or pulseless ventricular tachycardia should be cooled. Moreover, for any other rhythm or in the intra-hospital scenario, such cooling may also be beneficial. There are different ways of promoting hypothermia. The cooling system should be adjusted as soon as possible to the target temperature. Mild therapeutic hypothermia should be administered under close control, using neuromuscular blocking drugs to avoid shivering. The rewarming process should be slow, and reach 36º C, usually in no less then 8 hours. When temperature increases to more than 35º C, sedation, analgesia, and paralysis could be discontinued. The expected complications of hypothermia may be pneumonia, sepsis, cardiac arrhythmias, and coagulopathy. In spite of potential complications which require rigorous control, only six patients need to be treated to save one life.
Views0Abstract
Review ArticlesTherapeutical hypothermia after cardiopulmonary resuscitation: evidences and practical issues
Rev Bras Ter Intensiva. 2009;21(1):65-71
DOI 10.1590/S0103-507X2009000100010
Views0See moreCardiac arrest survivors frequently suffer from ischemic brain injury associated with poor neurological outcome and death. Therapeutic hypothermia improves outcomes in comatose survivors after resuscitation from out-of-hospital cardiac arrest. Considering its formal recommendation as a therapy, post-return of spontaneous circulation after cardiac arrest, the objective of this study was to review the clinical aspects of therapeutic hypothermia. Non-systematic review of articles using the keywords “cardiac arrest, cardiopulmonary resuscitation, cooling, hypothermia, post resuscitation syndrome” in the Med-Line database was performed. References of these articles were also reviewed. Unconscious adult patients with spontaneous circulation after out-of-hospital ventricular fibrillation or pulseless ventricular tachycardia should be cooled. Moreover, for any other rhythm or in the intra-hospital scenario, such cooling may also be beneficial. There are different ways of promoting hypothermia. The cooling system should be adjusted as soon as possible to the target temperature. Mild therapeutic hypothermia should be administered under close control, using neuromuscular blocking drugs to avoid shivering. The rewarming process should be slow, and reach 36º C, usually in no less then 8 hours. When temperature increases to more than 35º C, sedation, analgesia, and paralysis could be discontinued. The expected complications of hypothermia may be pneumonia, sepsis, cardiac arrhythmias, and coagulopathy. In spite of potential complications which require rigorous control, only six patients need to be treated to save one life.
-
Original Articles
Central and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
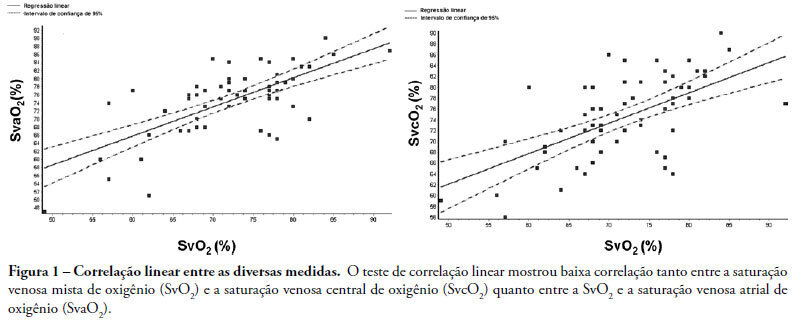
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Views0Abstract
Original ArticlesCentral and mixed venous oxygen saturation in septic shock: is there a clinically relevant difference?
Rev Bras Ter Intensiva. 2008;20(4):398-404
DOI 10.1590/S0103-507X2008000400013
Views0See moreINTRODUCTION: Central venous oxygen saturation (SvcO2) has been proposed as an alternative for mixed venous oxygen saturation (SvO2), with a variable level of acceptance according to available data. This study aimed to evaluate possible differences between SvO2 and SvcO2 or atrial venous saturation (SvaO2), with emphasis on the role of cardiac output and their impact on clinical management of the septic patient. METHODS: This is an observational, prospective study of patients with septic shock monitored by pulmonary artery catheter. Blood was obtained simultaneously for SvcO2, SvO2 and SvaO2 determination. Linear correlation (significant if p<0.05) and agreement analysis (Bland-Altman) were performed with samples and subgroups according to cardiac output. Moreover, agreement about clinical management based on these samples was evaluated. RESULTS: Sixty one measurements from 23 patients were obtained, median age of 65.0 (49.0-75.0) years and mean APACHE II of 27.7±6.3. Mean values of SvO2, SvcO2 and SvaO2 were 72.20±8.26%, 74.61±7.60% and 74.64±8.47%. Linear correlation test showed a weak correlation between SvO2 and SvcO2 (r=0.61, p<0.0001) and also between SvO2 and SvaO2 (r=0.70, p<0.0001). Agreements between SvcO2/SvO2 and SvaO2/SvO2 were -2.40±1.96 (-16.20 and 11.40) and -2.40±1.96 (-15.10 and 10.20), respectively, with no difference in the cardiac output subgroups. No agreement was found in clinical management for 27.8% of the cases, both for SvcO2/SvO2 and for SvaO2/SvO2. CONCLUSION: This study showed that the correlation and agreement between SvO2 and SvcO2 is weak and may lead to different clinical management.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis