Intensive care units Archives - Page 5 of 26 - Critical Care Science (CCS)

Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
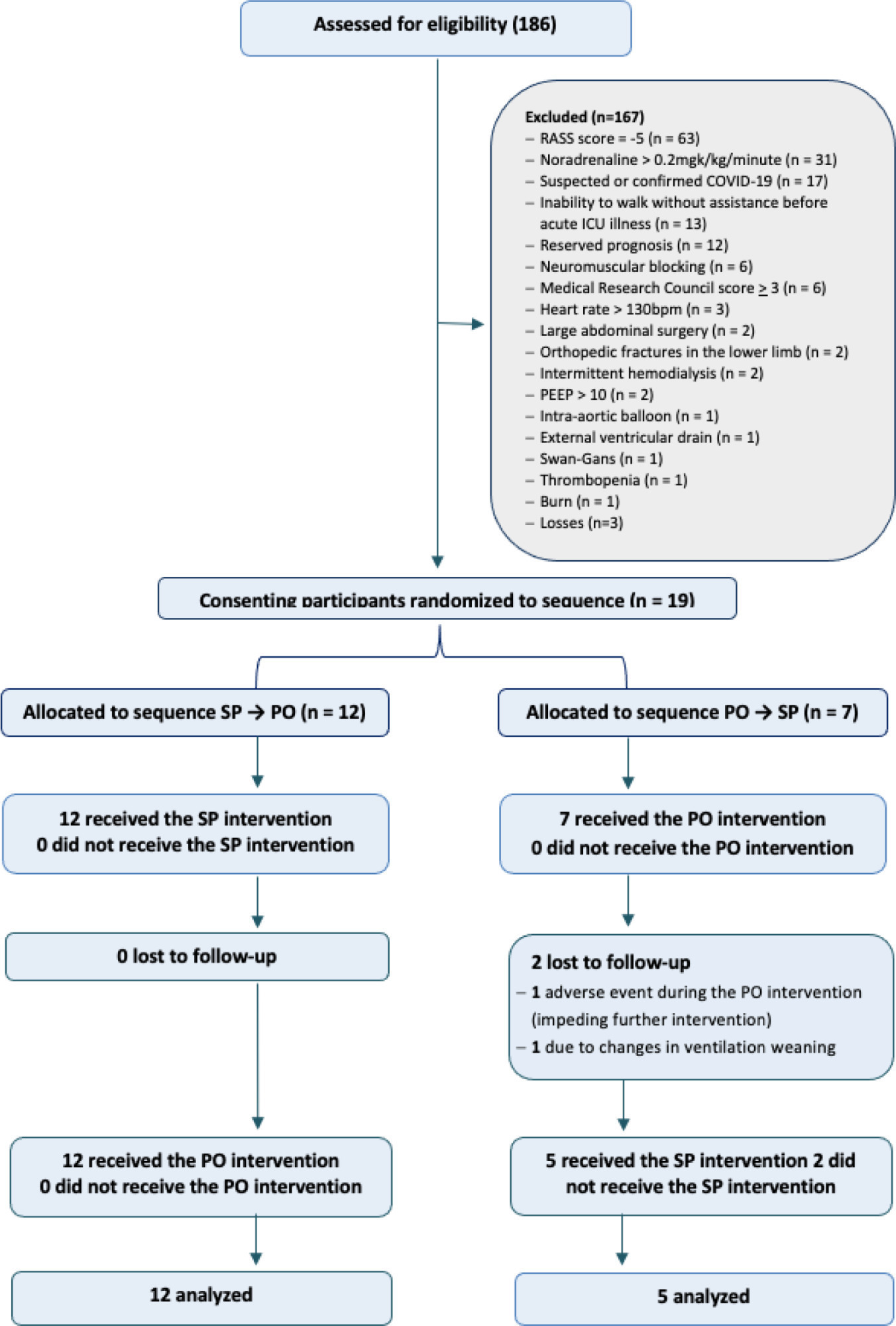
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(4):367-376
DOI 10.5935/2965-2774.20230069-pt
To assess the impact of different vertical positions on lung aeration in patients receiving invasive mechanical ventilation.
An open-label randomized crossover clinical trial was conducted between January and July 2020. Adults receiving invasive mechanical ventilation for > 24 hours and < 7 days with hemodynamic, respiratory and neurological stability were randomly assigned at a 1:1 ratio to the sitting position followed by passive orthostasis condition or the passive orthostasis followed by the sitting position condition. The primary outcome was lung aeration assessed using the lung ultrasound score (score ranges from 0 [better] to 36 [worse]).
A total of 186 subjects were screened; of these subjects, 19 were enrolled (57.8% male; mean age, 73.2 years). All participants were assigned to receive at least one verticalization protocol. Passive orthostasis resulted in mean lung ultrasound scores that did not differ significantly from the sitting position (11.0 versus 13.7; mean difference, -2.7; [95%CI -6.1 to 0.71; p = 0.11). Adverse events occurred in three subjects in the passive orthostasis group and in one in the sitting position group (p = 0.99).
This analysis did not find significant differences in lung aeration between the sitting and passive orthostasis groups. A randomized crossover clinical trial assessing the impact of vertical positioning on lung aeration in patients receiving invasive mechanical ventilation is feasible. Unfortunately, the study was interrupted due to the need to treat COVID-19 patients.
Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
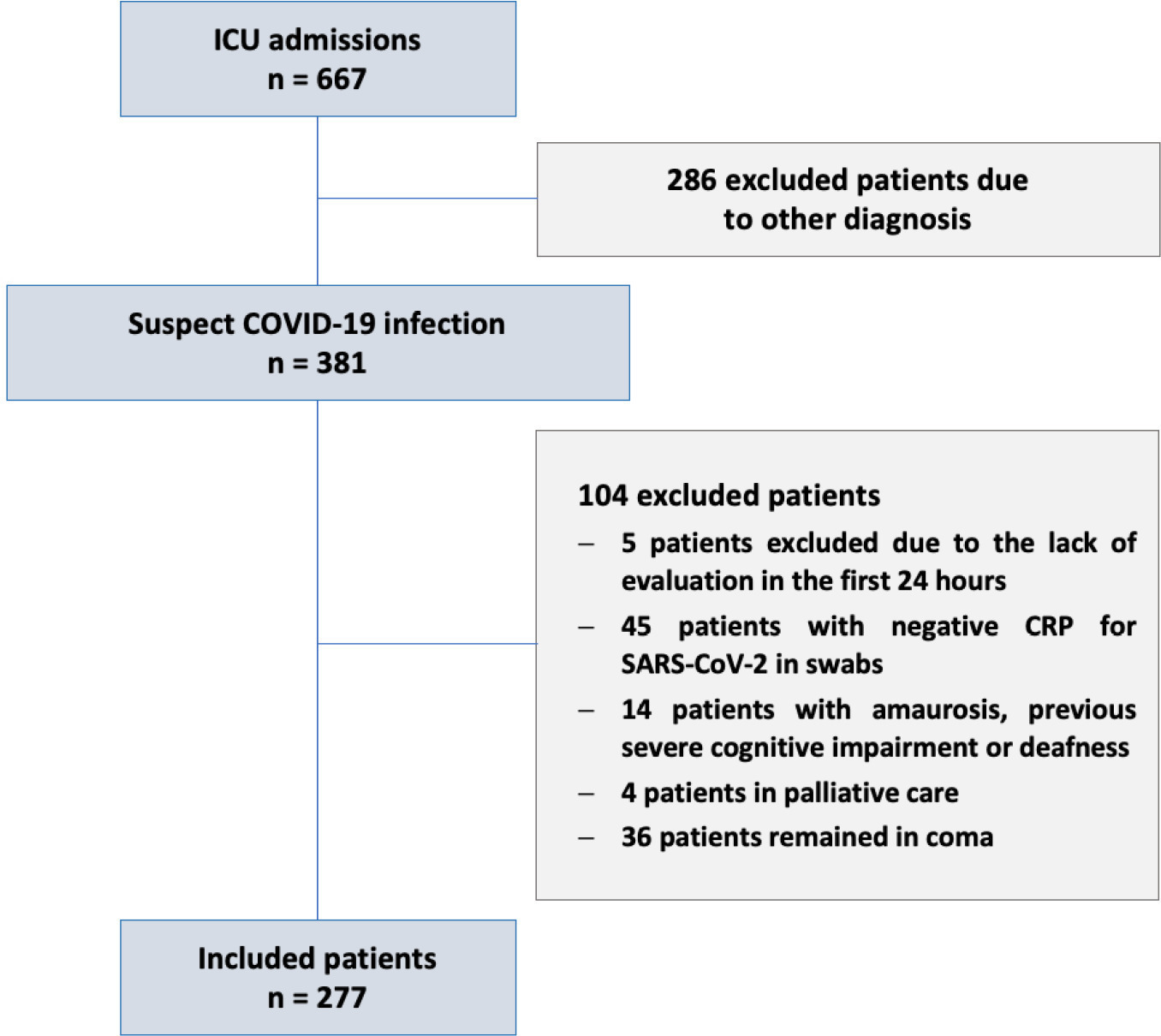
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Crit Care Sci. 2023;35(4):394-401
DOI 10.5935/2965-2774.20230170-pt
To investigate the impact of delirium severity in critically ill COVID-19 patients and its association with outcomes.
This prospective cohort study was performed in two tertiary intensive care units in Rio de Janeiro, Brazil. COVID-19 patients were evaluated daily during the first 7 days of intensive care unit stay using the Richmond Agitation Sedation Scale, Confusion Assessment Method for Intensive Care Unit (CAM-ICU) and Confusion Method Assessment for Intensive Care Unit-7 (CAM-ICU-7). Delirium severity was correlated with outcomes and one-year mortality.
Among the 277 COVID-19 patients included, delirium occurred in 101 (36.5%) during the first 7 days of intensive care unit stay, and it was associated with a higher length of intensive care unit stay in days (IQR 13 [7 - 25] versus 6 [4 - 12]; p < 0.001), higher hospital mortality (25.74% versus 5.11%; p < 0.001) and additional higher one-year mortality (5.3% versus 0.6%, p < 0.001). Delirium was classified by CAM-ICU-7 in terms of severity, and higher scores were associated with higher in-hospital mortality (17.86% versus 34.38% versus 38.46%, 95%CI, p value < 0.001). Severe delirium was associated with a higher risk of progression to coma (OR 7.1; 95%CI 1.9 - 31.0; p = 0.005) and to mechanical ventilation (OR 11.09; 95%CI 2.8 - 58.5; p = 0.002) in the multivariate analysis, adjusted by severity and frailty.
In patients admitted with COVID-19 in the intensive care unit, delirium was an independent risk factor for the worst prognosis, including mortality. The delirium severity assessed by the CAM-ICU-7 during the first week in the intensive care unit was associated with poor outcomes, including progression to coma and to mechanical ventilation.
Abstract
Crit Care Sci. 2023;35(3):320-327
DOI 10.5935/2965-2774.20230165-pt
To translate and cross-culturally adapt the Cornell Assessment of Pediatric Delirium anchor points from English to Brazilian Portuguese.
For the translation and cross-cultural adaptation of the anchor points, all steps recommended internationally were followed after authorization for use by the lead author. The stages were as follows: translation of the original version into Portuguese by two bilingual translators who were native speakers of the target language, synthesis of the versions, reverse translation by two translators who were native speakers of the source language, review and synthesis of the back-translation, review by a committee of experts and preparation of the final version.
The translation and cross-cultural adaptation of the anchor points was conducted in accordance with recommendations. The linguistic and semantic issues that arose were discussed by a committee of judges, with 91.8% agreement, as determined using a Likert scale, after changes by consensus. After reanalysis by the authors, there were no changes, resulting in the final version, which was easy to understand and administer.
The translation and cross-cultural adaptation of the anchor points of the Cornell Assessment of Pediatric Delirium scale into Portuguese spoken in Brazil were successful, maintaining the linguistic and semantic properties of the original instrument. The table of anchor points is easy to understand and will be helpful during the assessment of children younger than 24 months using the Cornell Assessment of Pediatric Delirium scale.
Abstract
Crit Care Sci. 2023;35(3):320-327
DOI 10.5935/2965-2774.20230165-pt
To translate and cross-culturally adapt the Cornell Assessment of Pediatric Delirium anchor points from English to Brazilian Portuguese.
For the translation and cross-cultural adaptation of the anchor points, all steps recommended internationally were followed after authorization for use by the lead author. The stages were as follows: translation of the original version into Portuguese by two bilingual translators who were native speakers of the target language, synthesis of the versions, reverse translation by two translators who were native speakers of the source language, review and synthesis of the back-translation, review by a committee of experts and preparation of the final version.
The translation and cross-cultural adaptation of the anchor points was conducted in accordance with recommendations. The linguistic and semantic issues that arose were discussed by a committee of judges, with 91.8% agreement, as determined using a Likert scale, after changes by consensus. After reanalysis by the authors, there were no changes, resulting in the final version, which was easy to understand and administer.
The translation and cross-cultural adaptation of the anchor points of the Cornell Assessment of Pediatric Delirium scale into Portuguese spoken in Brazil were successful, maintaining the linguistic and semantic properties of the original instrument. The table of anchor points is easy to understand and will be helpful during the assessment of children younger than 24 months using the Cornell Assessment of Pediatric Delirium scale.
Abstract
Crit Care Sci. 2023;35(3):266-272
DOI 10.5935/2965-2774.20230223-pt
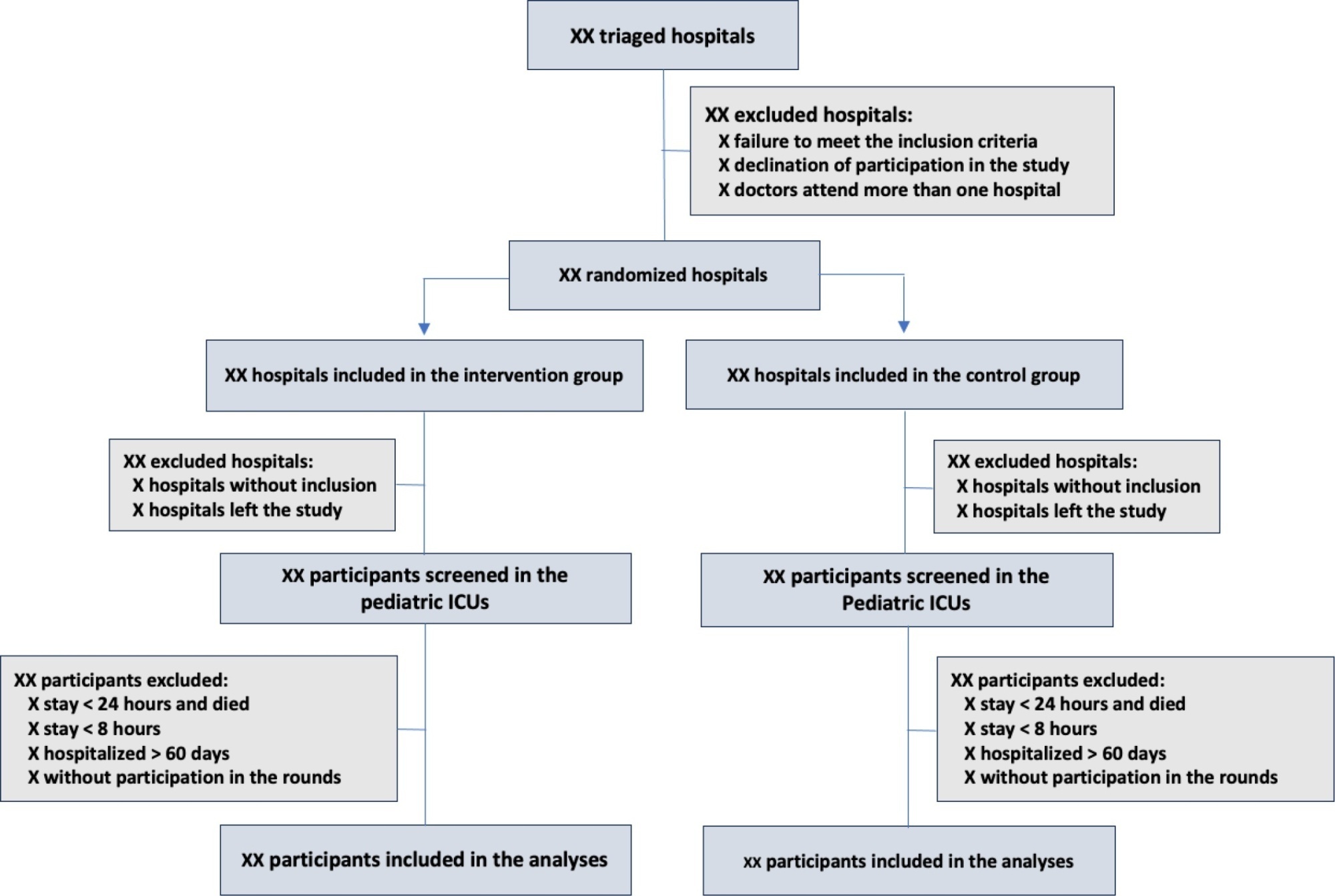
The objective of this study is to present the protocol of a cluster randomized clinical trial to be conducted through the TeleICU project - Qualification of Intensive Care by Telemedicine. The study will consist of a cluster randomized clinical trial, open label, in pediatric intensive care units, with an allocation ratio of 1:1, to compare the intervention group (support of Telemedicine for patients admitted to the pediatric intensive care unit) with a control group (pediatric intensive care unit usual care). The study proposed to select 16 pediatric intensive care units, including 100 participants per site, with a total of 1,600 participants. The intervention group will receive telerounds from Monday to Friday and will have specialists and continuing education activities available. The primary outcome measure will be the length of stay in the pediatric intensive care unit, defined as the difference between the date of discharge of the participant and the date of admission to the intensive care unit. The secondary outcomes will be mortality rate, invasive mechanical ventilation-free days, days using antibiotics, days using vasoactive drugs and days using sedoanalgesia. This study will be conducted in accordance with Resolution 466/12 of the National Health Council, with approval by the Research Ethics Committee of the institutions involved. The present study has the potential to reproduce studies on Telemedicine in intensive care and may make important contributions to care in intensive care units in Brazil and other settings. If Telemedicine shows positive clinical care results compared to conventional treatment, more pediatric patients may benefit.
ClinicalTrials.gov registry: NCT05260710
Abstract
Crit Care Sci. 2023;35(3):266-272
DOI 10.5935/2965-2774.20230223-pt
The objective of this study is to present the protocol of a cluster randomized clinical trial to be conducted through the TeleICU project - Qualification of Intensive Care by Telemedicine. The study will consist of a cluster randomized clinical trial, open label, in pediatric intensive care units, with an allocation ratio of 1:1, to compare the intervention group (support of Telemedicine for patients admitted to the pediatric intensive care unit) with a control group (pediatric intensive care unit usual care). The study proposed to select 16 pediatric intensive care units, including 100 participants per site, with a total of 1,600 participants. The intervention group will receive telerounds from Monday to Friday and will have specialists and continuing education activities available. The primary outcome measure will be the length of stay in the pediatric intensive care unit, defined as the difference between the date of discharge of the participant and the date of admission to the intensive care unit. The secondary outcomes will be mortality rate, invasive mechanical ventilation-free days, days using antibiotics, days using vasoactive drugs and days using sedoanalgesia. This study will be conducted in accordance with Resolution 466/12 of the National Health Council, with approval by the Research Ethics Committee of the institutions involved. The present study has the potential to reproduce studies on Telemedicine in intensive care and may make important contributions to care in intensive care units in Brazil and other settings. If Telemedicine shows positive clinical care results compared to conventional treatment, more pediatric patients may benefit.
ClinicalTrials.gov registry: NCT05260710
Abstract
Crit Care Sci. 2023;35(3):273-280
DOI 10.5935/2965-2774.20230359-pt
To describe the role of physiotherapists in assisting patients suspected to have or diagnosed with COVID-19 hospitalized in intensive care units in Brazil regarding technical training, working time, care practice, labor conditions and remuneration.
An analytical cross-sectional survey was carried out through an electronic questionnaire distributed to physiotherapists who worked in the care of patients with COVID-19 in Brazilian intensive care units.
A total of 657 questionnaires were completed by physiotherapists from the five regions of the country, with 85.3% working in adult, 5.4% in neonatal, 5.3% in pediatric and 3.8% in mixed intensive care units (pediatric and neonatal). In intensive care units with a physiotherapists available 24 hours/day, physiotherapists worked more frequently (90.6%) in the assembly, titration, and monitoring of noninvasive ventilation (p = 0.001). Most intensive care units with 12-hour/day physiotherapists (25.8%) did not apply any protocol compared to intensive care units with 18-hour/day physiotherapy (9.9%) versus 24 hours/day (10.2%) (p = 0.032). Most of the respondents (51.0%) received remuneration 2 or 3 times the minimum wage, and only 25.1% received an additional payment for working with patients suspected to have or diagnosed with COVID-19; 85.7% of them did not experience a lack of personal protective equipment.
Intensive care units with 24-hour/day physiotherapists had higher percentages of protocols and noninvasive ventilation for patients with COVID-19. The use of specific resources varied between the types of intensive care units and hospitals and in relation to the physiotherapists’ labor conditions. This study showed that most professionals had little experience in intensive care and low wages.
Abstract
Crit Care Sci. 2023;35(3):273-280
DOI 10.5935/2965-2774.20230359-pt
To describe the role of physiotherapists in assisting patients suspected to have or diagnosed with COVID-19 hospitalized in intensive care units in Brazil regarding technical training, working time, care practice, labor conditions and remuneration.
An analytical cross-sectional survey was carried out through an electronic questionnaire distributed to physiotherapists who worked in the care of patients with COVID-19 in Brazilian intensive care units.
A total of 657 questionnaires were completed by physiotherapists from the five regions of the country, with 85.3% working in adult, 5.4% in neonatal, 5.3% in pediatric and 3.8% in mixed intensive care units (pediatric and neonatal). In intensive care units with a physiotherapists available 24 hours/day, physiotherapists worked more frequently (90.6%) in the assembly, titration, and monitoring of noninvasive ventilation (p = 0.001). Most intensive care units with 12-hour/day physiotherapists (25.8%) did not apply any protocol compared to intensive care units with 18-hour/day physiotherapy (9.9%) versus 24 hours/day (10.2%) (p = 0.032). Most of the respondents (51.0%) received remuneration 2 or 3 times the minimum wage, and only 25.1% received an additional payment for working with patients suspected to have or diagnosed with COVID-19; 85.7% of them did not experience a lack of personal protective equipment.
Intensive care units with 24-hour/day physiotherapists had higher percentages of protocols and noninvasive ventilation for patients with COVID-19. The use of specific resources varied between the types of intensive care units and hospitals and in relation to the physiotherapists’ labor conditions. This study showed that most professionals had little experience in intensive care and low wages.
Abstract
Crit Care Sci. 2023;35(3):290-301
DOI 10.5935/2965-2774.20230388-pt
To determine the prevalence and factors associated with the physical rehabilitation of critically ill children in Brazilian pediatric intensive care units.
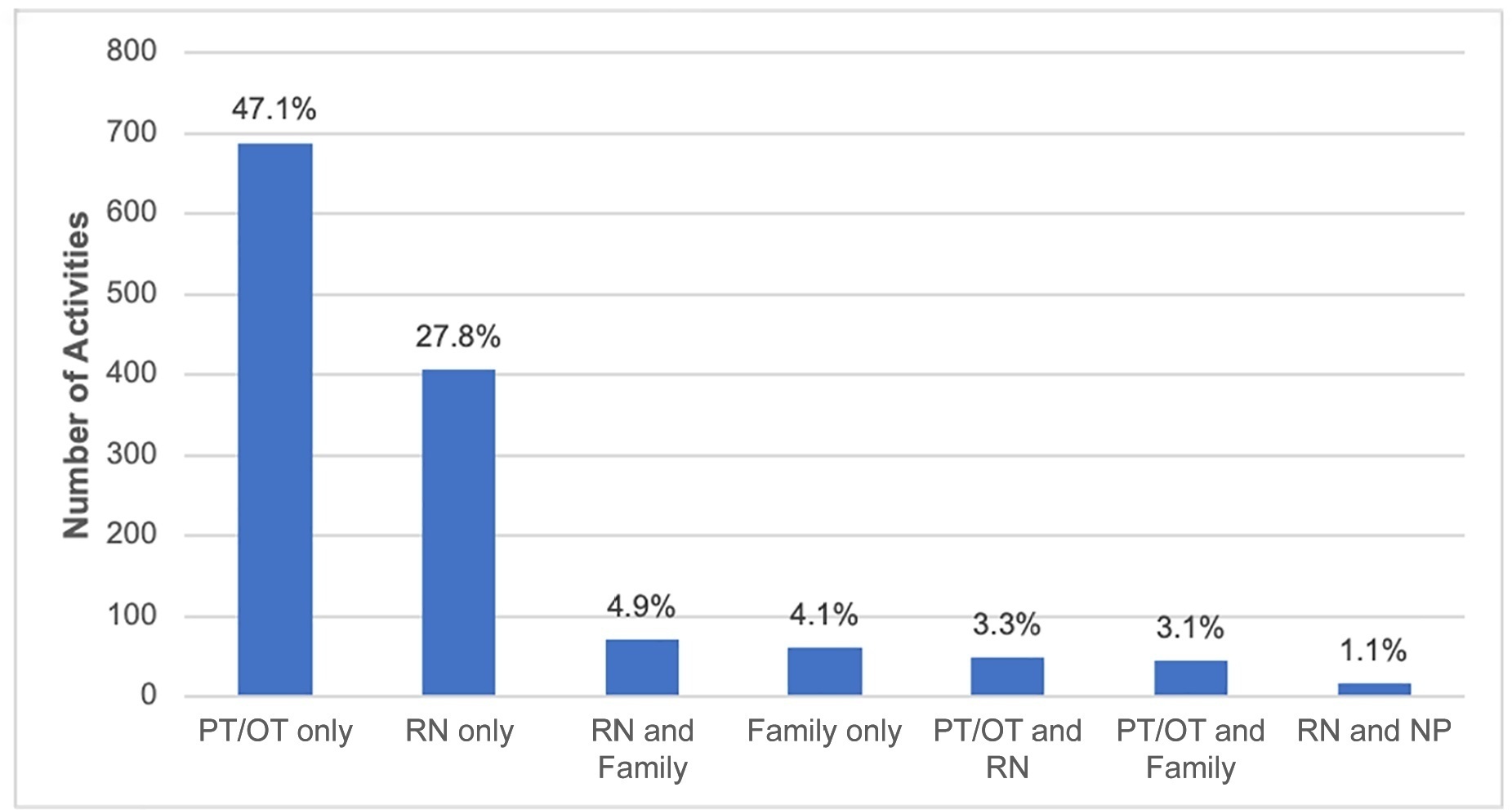
A 2-day, cross-sectional, multicenter point prevalence study comprising 27 pediatric intensive care units (out of 738) was conducted in Brazil in April and June 2019. This Brazilian study was part of a large multinational study called Prevalence of Acute Rehabilitation for Kids in the PICU (PARK-PICU). The primary outcome was the prevalence of mobility provided by physical therapy or occupational therapy. Clinical data on patient mobility, potential mobility safety events, and mobilization barriers were prospectively collected in patients admitted for ≥ 72 hours.
Children under the age of 3 years comprised 68% of the patient population. The prevalence of therapist-provided mobility was 74%, or 277 out of the 375 patient-days. Out-of-bed mobility was most positively associated with family presence (adjusted odds ratios 3.31;95%CI 1.70 - 6.43) and most negatively associated with arterial lines (adjusted odds ratios 0.16; 95%CI 0.05 - 0.57). Barriers to mobilization were reported on 27% of patient-days, the most common being lack of physician order (n = 18). Potential safety events occurred in 3% of all mobilization events.
Therapist-provided mobility in Brazilian pediatric intensive care units is frequent. Family presence was high and positively associated with out-of-bed mobility. The presence of physiotherapists 24 hours a day in Brazilian pediatric intensive care units may have a substantial impact on the mobilization of critically ill children.
Abstract
Crit Care Sci. 2023;35(3):290-301
DOI 10.5935/2965-2774.20230388-pt
To determine the prevalence and factors associated with the physical rehabilitation of critically ill children in Brazilian pediatric intensive care units.
A 2-day, cross-sectional, multicenter point prevalence study comprising 27 pediatric intensive care units (out of 738) was conducted in Brazil in April and June 2019. This Brazilian study was part of a large multinational study called Prevalence of Acute Rehabilitation for Kids in the PICU (PARK-PICU). The primary outcome was the prevalence of mobility provided by physical therapy or occupational therapy. Clinical data on patient mobility, potential mobility safety events, and mobilization barriers were prospectively collected in patients admitted for ≥ 72 hours.
Children under the age of 3 years comprised 68% of the patient population. The prevalence of therapist-provided mobility was 74%, or 277 out of the 375 patient-days. Out-of-bed mobility was most positively associated with family presence (adjusted odds ratios 3.31;95%CI 1.70 - 6.43) and most negatively associated with arterial lines (adjusted odds ratios 0.16; 95%CI 0.05 - 0.57). Barriers to mobilization were reported on 27% of patient-days, the most common being lack of physician order (n = 18). Potential safety events occurred in 3% of all mobilization events.
Therapist-provided mobility in Brazilian pediatric intensive care units is frequent. Family presence was high and positively associated with out-of-bed mobility. The presence of physiotherapists 24 hours a day in Brazilian pediatric intensive care units may have a substantial impact on the mobilization of critically ill children.
Abstract
Crit Care Sci. 2023;35(3):302-310
DOI 10.5935/2965-2774.20230141-pt
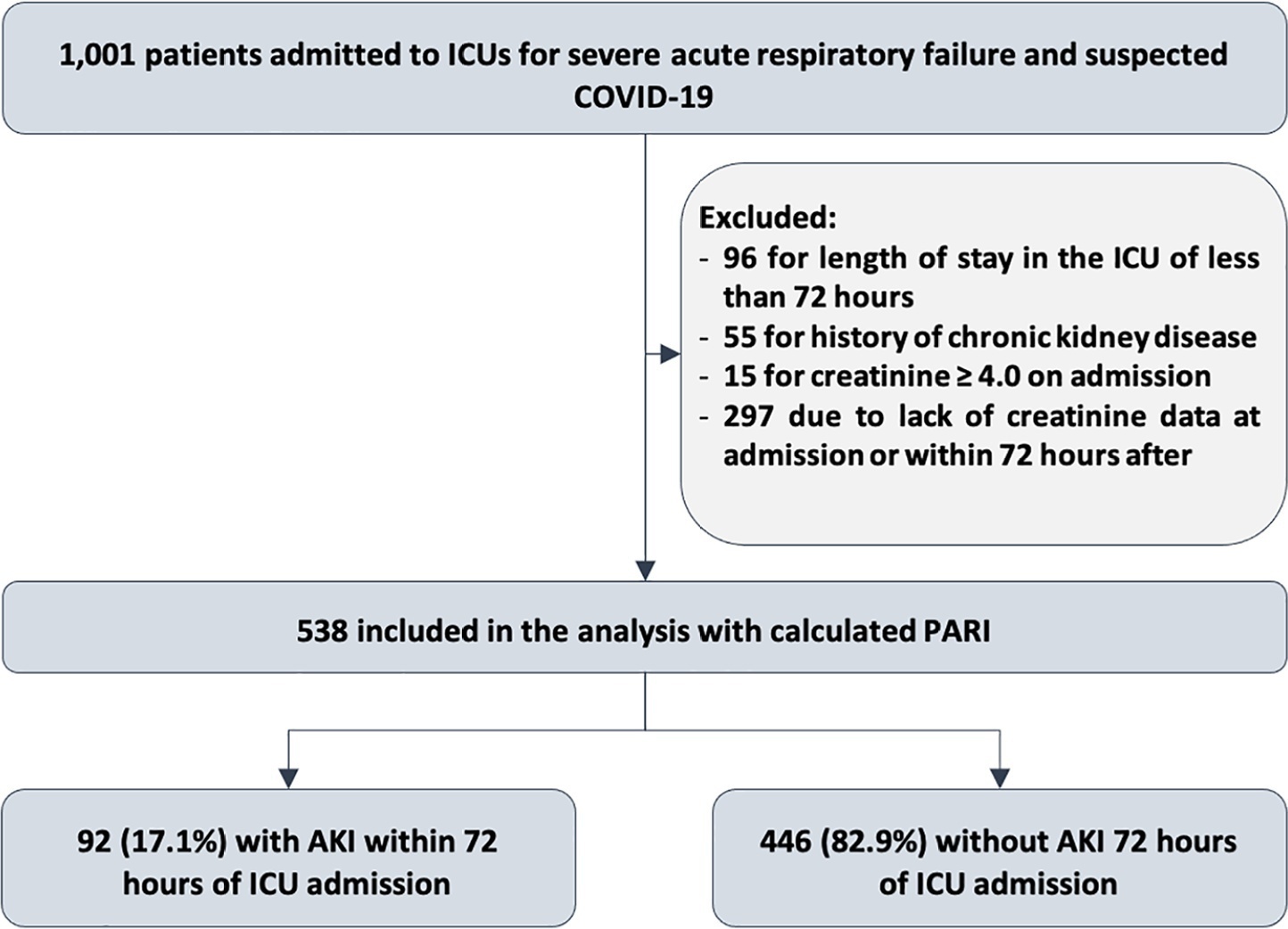
To evaluate the accuracy of the persistent AKI risk index (PARI) in predicting acute kidney injury within 72 hours after admission to the intensive care unit, persistent acute kidney injury, renal replacement therapy, and death within 7 days in patients hospitalized due to acute respiratory failure.
This study was done in a cohort of diagnoses of consecutive adult patients admitted to the intensive care unit of eight hospitals in Curitiba, Brazil, between March and September 2020 due to acute respiratory failure secondary to suspected COVID-19. The COVID-19 diagnosis was confirmed or refuted by RT-PCR for the detection of SARS-CoV-2. The ability of PARI to predict acute kidney injury at 72 hours, persistent acute kidney injury, renal replacement therapy, and death within 7 days was analyzed by ROC curves in comparison to delta creatinine, SOFA, and APACHE II.
Of the 1,001 patients in the cohort, 538 were included in the analysis. The mean age was 62 ± 17 years, 54.8% were men, and the median APACHE II score was 12. At admission, the median SOFA score was 3, and 83.3% had no renal dysfunction. After admission to the intensive care unit, 17.1% had acute kidney injury within 72 hours, and through 7 days, 19.5% had persistent acute kidney injury, 5% underwent renal replacement therapy, and 17.1% died. The PARI had an area under the ROC curve of 0.75 (0.696 - 0.807) for the prediction of acute kidney injury at 72 hours, 0.71 (0.613 - 0.807) for renal replacement therapy, and 0.64 (0.565 - 0.710) for death.
The PARI has acceptable accuracy in predicting acute kidney injury within 72 hours and renal replacement therapy within 7 days of admission to the intensive care unit, but it is not significantly better than the other scores.
Abstract
Crit Care Sci. 2023;35(3):302-310
DOI 10.5935/2965-2774.20230141-pt
To evaluate the accuracy of the persistent AKI risk index (PARI) in predicting acute kidney injury within 72 hours after admission to the intensive care unit, persistent acute kidney injury, renal replacement therapy, and death within 7 days in patients hospitalized due to acute respiratory failure.
This study was done in a cohort of diagnoses of consecutive adult patients admitted to the intensive care unit of eight hospitals in Curitiba, Brazil, between March and September 2020 due to acute respiratory failure secondary to suspected COVID-19. The COVID-19 diagnosis was confirmed or refuted by RT-PCR for the detection of SARS-CoV-2. The ability of PARI to predict acute kidney injury at 72 hours, persistent acute kidney injury, renal replacement therapy, and death within 7 days was analyzed by ROC curves in comparison to delta creatinine, SOFA, and APACHE II.
Of the 1,001 patients in the cohort, 538 were included in the analysis. The mean age was 62 ± 17 years, 54.8% were men, and the median APACHE II score was 12. At admission, the median SOFA score was 3, and 83.3% had no renal dysfunction. After admission to the intensive care unit, 17.1% had acute kidney injury within 72 hours, and through 7 days, 19.5% had persistent acute kidney injury, 5% underwent renal replacement therapy, and 17.1% died. The PARI had an area under the ROC curve of 0.75 (0.696 - 0.807) for the prediction of acute kidney injury at 72 hours, 0.71 (0.613 - 0.807) for renal replacement therapy, and 0.64 (0.565 - 0.710) for death.
The PARI has acceptable accuracy in predicting acute kidney injury within 72 hours and renal replacement therapy within 7 days of admission to the intensive care unit, but it is not significantly better than the other scores.
Abstract
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
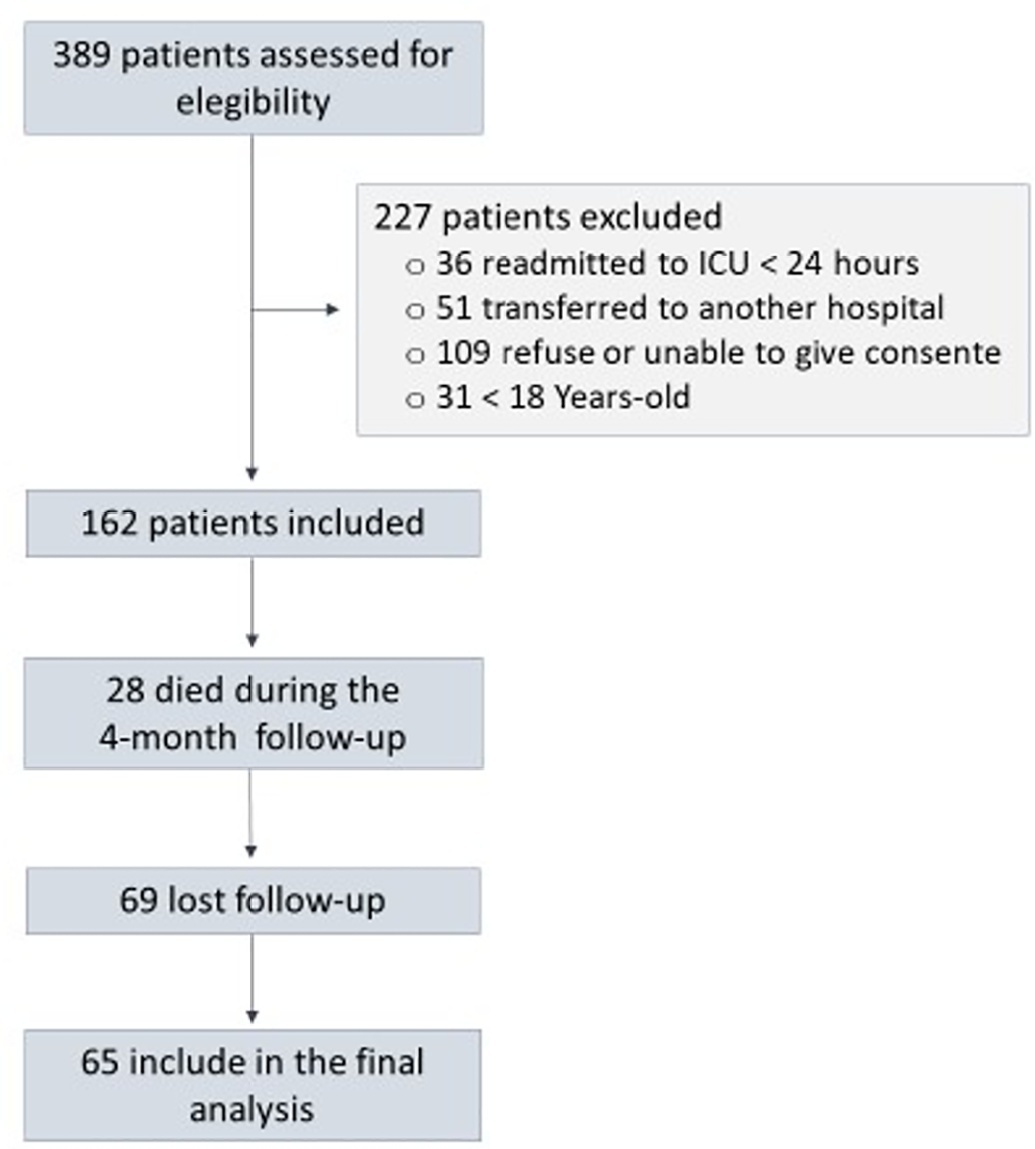
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.
Abstract
Crit Care Sci. 2023;35(2):147-155
DOI 10.5935/2965-2774.20230422-pt
To assess factors associated with long-term neuropsychiatric outcomes, including biomarkers measured after discharge from the intensive care unit.
A prospective cohort study was performed with 65 intensive care unit survivors. The cognitive evaluation was performed through the Mini-Mental State Examination, the symptoms of anxiety and depression were evaluated using the Hospital Anxiety and Depression Scale, and posttraumatic stress disorder was evaluated using the Impact of Event Scale-6. Plasma levels of amyloid-beta (1-42) [Aβ (1-42)], Aβ (1-40), interleukin (IL)-10, IL-6, IL-33, IL-4, IL-5, tumor necrosis factor alpha, C-reactive protein, and brain-derived neurotrophic factor were measured at intensive care unit discharge.
Of the variables associated with intensive care, only delirium was independently related to the occurrence of long-term cognitive impairment. In addition, higher levels of IL-10 and IL-6 were associated with cognitive dysfunction. Only IL-6 was independently associated with depression. Mechanical ventilation, IL-33 levels, and C-reactive protein levels were independently associated with anxiety. No variables were independently associated with posttraumatic stress disorder.
Cognitive dysfunction, as well as symptoms of depression, anxiety, and posttraumatic stress disorder, are present in patients who survive a critical illness, and some of these outcomes are associated with the levels of inflammatory biomarkers measured at discharge from the intensive care unit.