Intensive care units Archives - Page 5 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
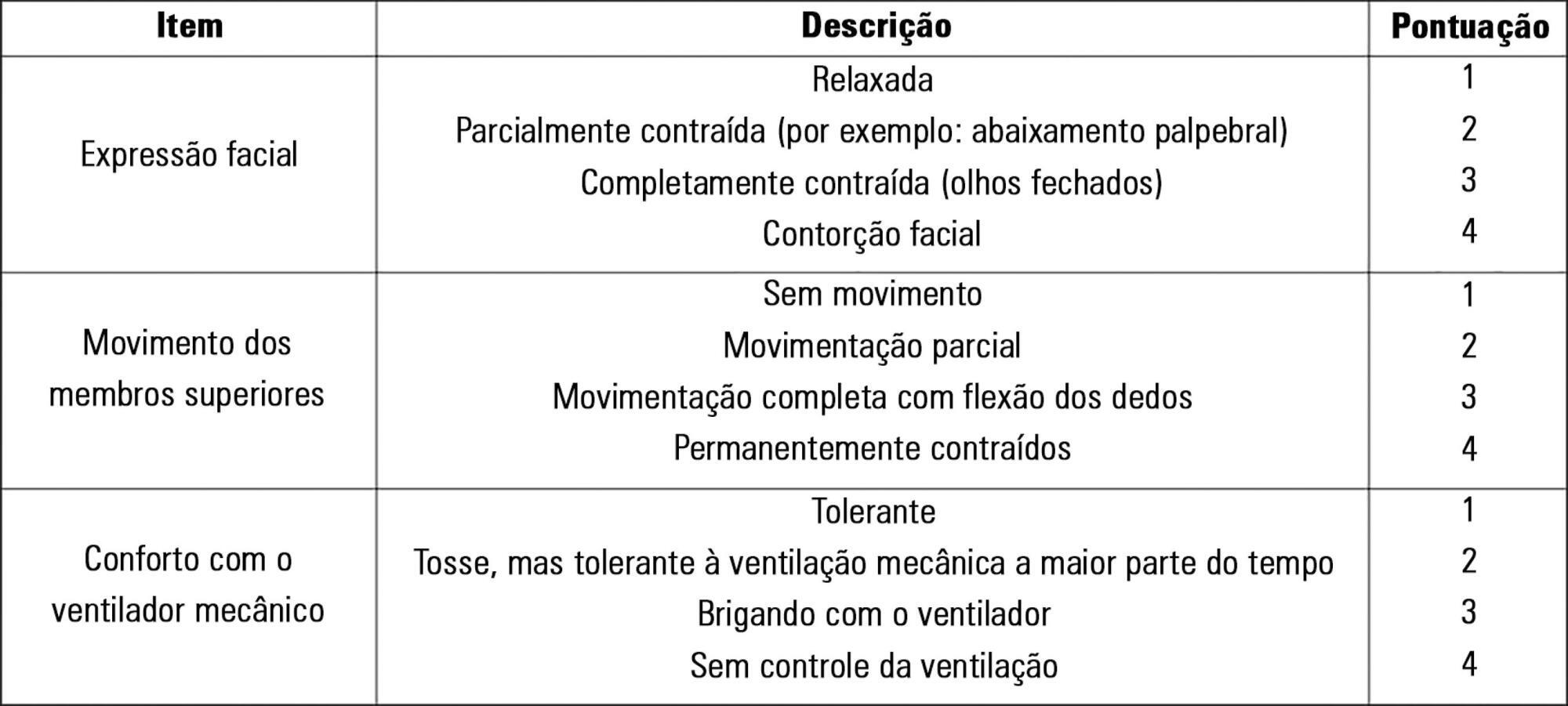
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):42-49
DOI 10.5935/0103-507X.20180009
To evaluate the validity and reliability of the Brazilian version of the Behavioral Pain Scale (BPS-Br) in victims of traumatic brain injury.
Observational prospective study with paired and repeated measures conducted at two intensive care units (clinical and surgical) of a large general hospital. The convenience sample consisted of adult victims of moderate or severe penetrating or blunt craniocerebral trauma who were sedated and mechanically ventilated. A total of 432 paired observations were performed by independent evaluators simultaneously, prior to eye cleaning, during eye cleaning, during tracheal aspiration and after tracheal aspiration. Sociodemographic, clinical, trauma-related, sedoanalgesia and physiological parameter data (heart rate, systolic and diastolic blood pressure) were collected. The discriminant validity was tested using the Friedman and Wilcoxon paired tests. The intraclass correlation coefficient and Cohen's Kappa coefficient were used to evaluate the reliability. The Spearman correlation test was used to test the association between clinical variables and BPS-Br scores during tracheal aspiration.
There was a significant increase in the physiological parameters during tracheal aspiration, but without correlation with the BPS-Br scores. Pain was significantly more intense during tracheal aspiration (p < 0.005). Satisfactory interobserver agreement was found, with an intraclass correlation coefficient of 0.95 (0.90 - 0.98) and Kappa coefficient of 0.70.
Brazilian version of the Behavioral Pain Scale scores increased during tracheal aspiration. The Brazilian version of the scale was valid and reliable for pain assessment of traumatic brain injury victims undergoing tracheal aspiration.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):50-56
DOI 10.5935/0103-507X.20180010
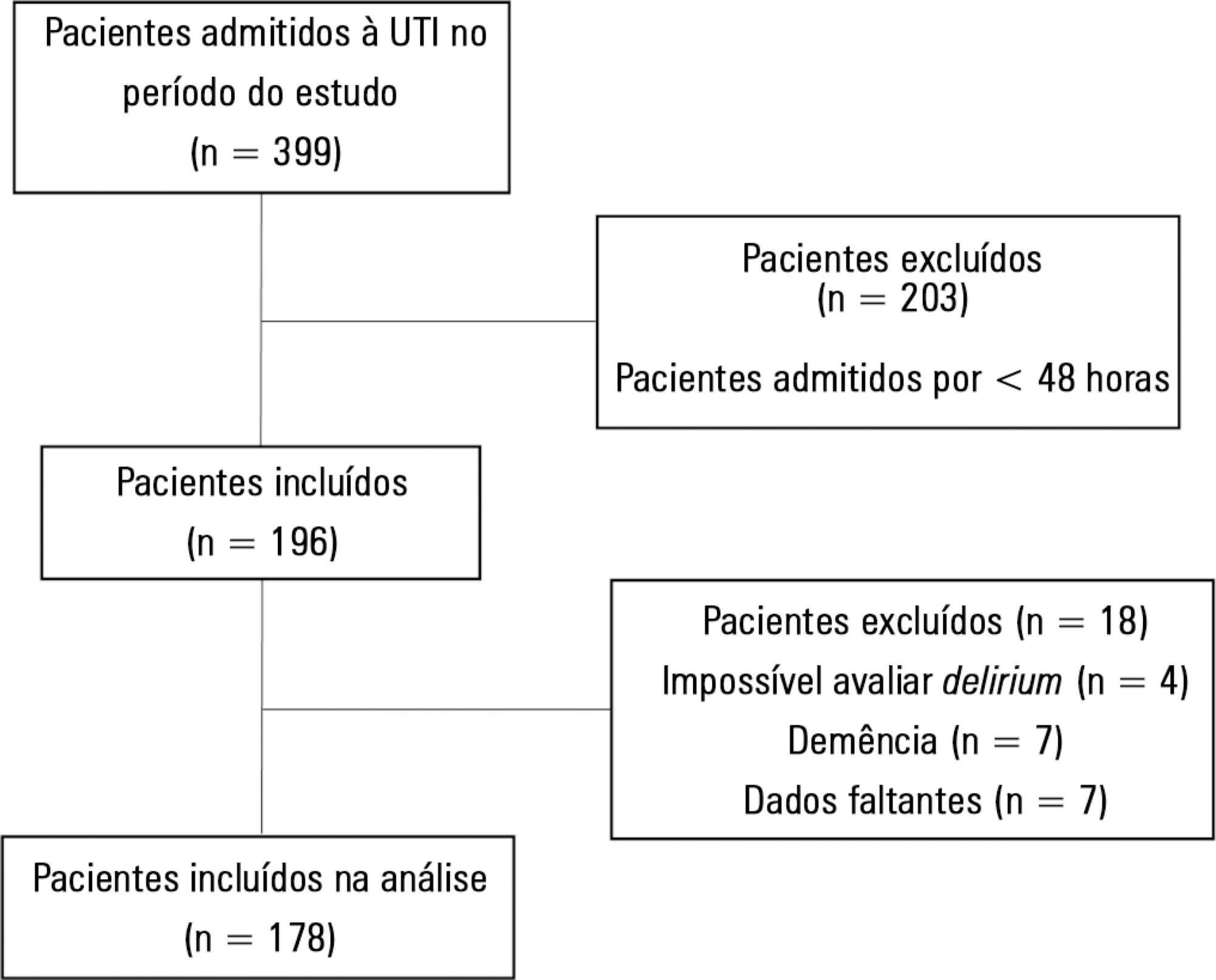
To describe the incidence of and risk factors for delirium in the intensive care unit of a tertiary care teaching hospital in Argentina and to conduct the first non-European study exploring the performance of the PREdiction of DELIRium in ICu patients (PRE-DELIRIC) model.
Prospective observational study in a 20-bed intensive care unit of a tertiary care teaching hospital in Buenos Aires, Argentina. The PRE-DELIRIC model was applied to 178 consecutive patients within 24 hours of admission to the intensive care unit; delirium was assessed with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
The mean age was 64.3 ± 17.9 years. The median time of stay in the intensive care unit was 6 (range, 2 - 56) days. Of the total number of patients, 49/178 (27.5%) developed delirium, defined as a positive CAM-ICU assessment, during their stay in the intensive care unit. Patients in the delirium group were significantly older and had a significantly higher Acute Physiological and Chronic Health Evaluation II (APACHE II) score. The mortality rate in the intensive care unit was 14.6%; no significant difference was observed between the two groups. Predictive factors for the development of delirium were increased age, prolonged intensive care unit stay, and opioid use. The area under the curve for the PRE-DELIRIC model was 0.83 (95%CI; 0.77 - 0.90).
The observed incidence of delirium highlights the importance of this problem in the intensive care unit setting. In this first study conducted outside Europe, PRE-DELIRIC accurately predicted the development of delirium.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):50-56
DOI 10.5935/0103-507X.20180010
To describe the incidence of and risk factors for delirium in the intensive care unit of a tertiary care teaching hospital in Argentina and to conduct the first non-European study exploring the performance of the PREdiction of DELIRium in ICu patients (PRE-DELIRIC) model.
Prospective observational study in a 20-bed intensive care unit of a tertiary care teaching hospital in Buenos Aires, Argentina. The PRE-DELIRIC model was applied to 178 consecutive patients within 24 hours of admission to the intensive care unit; delirium was assessed with the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU).
The mean age was 64.3 ± 17.9 years. The median time of stay in the intensive care unit was 6 (range, 2 - 56) days. Of the total number of patients, 49/178 (27.5%) developed delirium, defined as a positive CAM-ICU assessment, during their stay in the intensive care unit. Patients in the delirium group were significantly older and had a significantly higher Acute Physiological and Chronic Health Evaluation II (APACHE II) score. The mortality rate in the intensive care unit was 14.6%; no significant difference was observed between the two groups. Predictive factors for the development of delirium were increased age, prolonged intensive care unit stay, and opioid use. The area under the curve for the PRE-DELIRIC model was 0.83 (95%CI; 0.77 - 0.90).
The observed incidence of delirium highlights the importance of this problem in the intensive care unit setting. In this first study conducted outside Europe, PRE-DELIRIC accurately predicted the development of delirium.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):98-111
DOI 10.5935/0103-507X.20180016
The follow-up of patients who are discharged from intensive care units follows distinct flows in different parts of the world. Outpatient clinics or post-intensive care clinics represent one of the forms of follow-up, with more than 20 years of experience in some countries. Qualitative studies that followed up patients in these outpatient clinics suggest more encouraging results than quantitative studies, demonstrating improvements in intermediate outcomes, such as patient and family satisfaction. More important results, such as mortality and improvement in the quality of life of patients and their families, have not yet been demonstrated. In addition, which patients should be indicated for these outpatient clinics? How long should they be followed up? Can we expect an improvement of clinical outcomes in these followed-up patients? Are outpatient clinics cost-effective? These are only some of the questions that arise from this form of follow-up of the survivors of intensive care units. This article aims to review all aspects relating to the organization and performance of post-intensive care outpatient clinics and to provide an overview of studies that evaluated clinical outcomes related to this practice.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):317-326
DOI 10.5935/0103-507X.20180052
To characterize the transport of severely ill patients with extracorporeal respiratory or cardiovascular support.
A series of 18 patients in the state of São Paulo, Brazil is described. All patients were consecutively evaluated by a multidisciplinary team at the hospital of origin. The patients were rescued, and extracorporeal membrane oxygenation support was provided on site. The patients were then transported to referral hospitals for extracorporeal membrane oxygenation support. Data were retrieved from a prospectively collected database.
From 2011 to 2017, 18 patients aged 29 (25 - 31) years with a SAPS 3 of 84 (68 - 92) and main primary diagnosis of leptospirosis and influenza A (H1N1) virus were transported to three referral hospitals in São Paulo. A median distance of 39 (15 - 82) km was traveled on each rescue mission during a period of 360 (308 - 431) min. A median of one (0 - 2) nurse, three (2 - 3) physicians, and one (0 - 1) physical therapist was present per rescue. Seventeen rescues were made by ambulance, and one rescue was made by helicopter. The observed complications were interruption in the energy supply to the pump in two cases (11%) and oxygen saturation < 70% in two cases. Thirteen patients (72%) survived and were discharged from the hospital. Among the nonsurvivors, there were two cases of brain death, two cases of multiple organ dysfunction syndrome, and one case of irreversible pulmonary fibrosis.
Transportation with extracorporeal support occurred without serious complications, and the hospital survival rate was high.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):338-346
DOI 10.5935/0103-507X.20180057
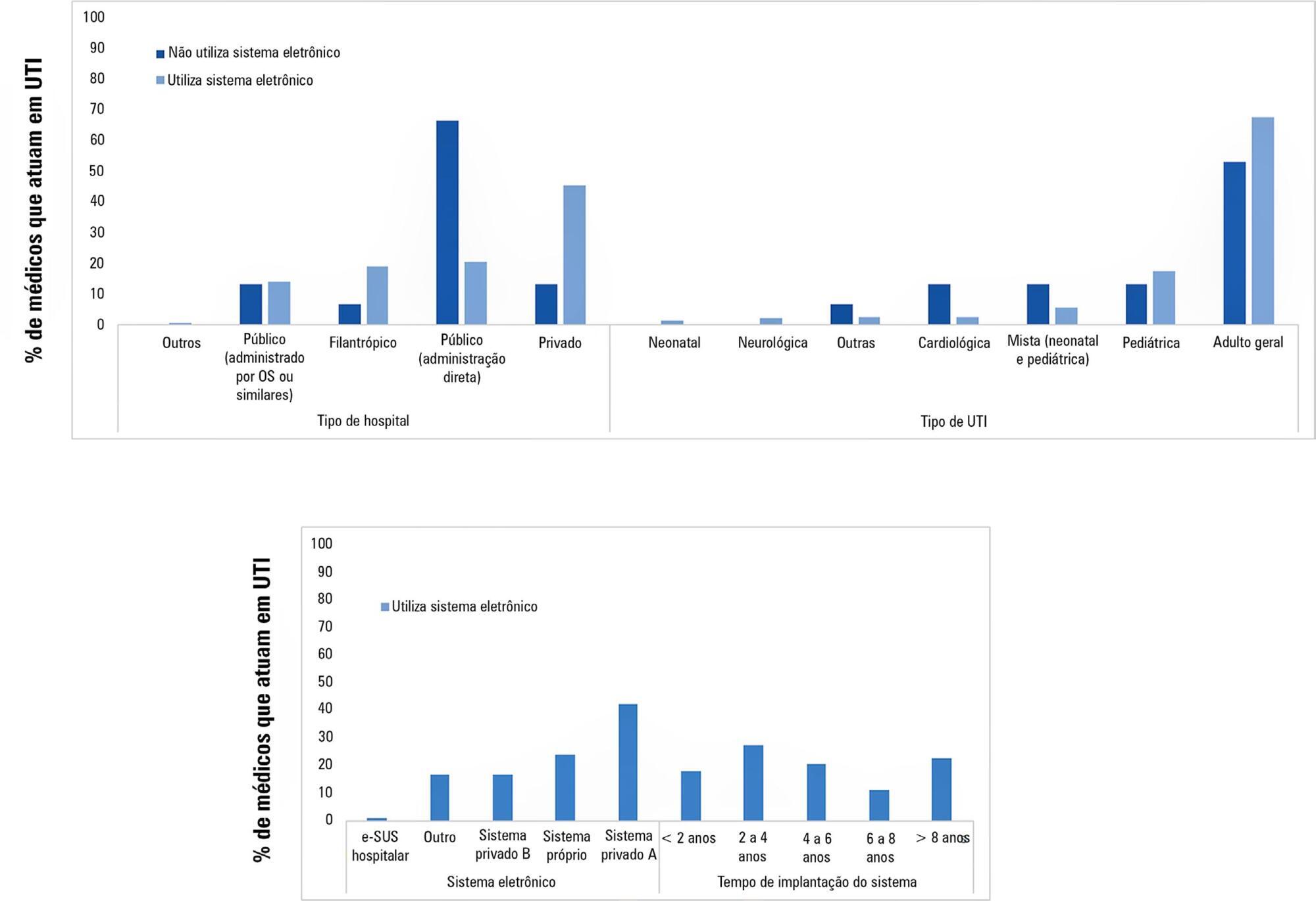
To examine the prevalence of the use of electronic medical record systems in Brazilian intensive care units and the perceptions of intensive care physicians regarding the contribution of electronic medical record systems toward improving safety and quality in clinical practice.
Using an online questionnaire, physicians working in Brazilian intensive care units answered questions about the use of electronic medical record systems in the hospitals in which they worked. They were asked about the types of electronic medical record systems used and their levels of satisfaction with these systems in terms of improving quality and safety.
Of the 4,772 invitations sent, 204 physicians responded to the questionnaire. Most used electronic medical record and prescription systems (92.6%), worked in private hospitals (43.1%), worked in general adult intensive care units (66.7%) and used Private System A (39.2%); most systems had been used for between 2 and 4 years (25.5%). Furthermore, the majority (84.6%) believed that the electronic system provided better quality than a paper system, and 76.7% believed that electronic systems provided greater safety than paper systems.
Electronic medical record systems seem to be widely used by the Brazilian intensive care physicians who responded to the questionnaire and, according to the data, seem to provide greater quality and safety than do paper records.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):338-346
DOI 10.5935/0103-507X.20180057
To examine the prevalence of the use of electronic medical record systems in Brazilian intensive care units and the perceptions of intensive care physicians regarding the contribution of electronic medical record systems toward improving safety and quality in clinical practice.
Using an online questionnaire, physicians working in Brazilian intensive care units answered questions about the use of electronic medical record systems in the hospitals in which they worked. They were asked about the types of electronic medical record systems used and their levels of satisfaction with these systems in terms of improving quality and safety.
Of the 4,772 invitations sent, 204 physicians responded to the questionnaire. Most used electronic medical record and prescription systems (92.6%), worked in private hospitals (43.1%), worked in general adult intensive care units (66.7%) and used Private System A (39.2%); most systems had been used for between 2 and 4 years (25.5%). Furthermore, the majority (84.6%) believed that the electronic system provided better quality than a paper system, and 76.7% believed that electronic systems provided greater safety than paper systems.
Electronic medical record systems seem to be widely used by the Brazilian intensive care physicians who responded to the questionnaire and, according to the data, seem to provide greater quality and safety than do paper records.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):219-225
DOI 10.5935/0103-507X.20180036
To review the evidence on the safety of neuromuscular electrical stimulation when used in the intensive care unit.
A systematic review was conducted; a literature search was performed of the MEDLINE (via PubMed), PEDro, Cochrane CENTRAL and EMBASE databases, and a further manual search was performed among the references cited in randomized studies. Randomized clinical trials that compared neuromuscular electrical stimulation to a control or placebo group in the intensive care unit and reporting on the technique safety in the outcomes were included. Hemodynamic variables and information on adverse effects were considered safety parameters. Articles were independently analyzed by two reviewers, and the data analysis was descriptive.
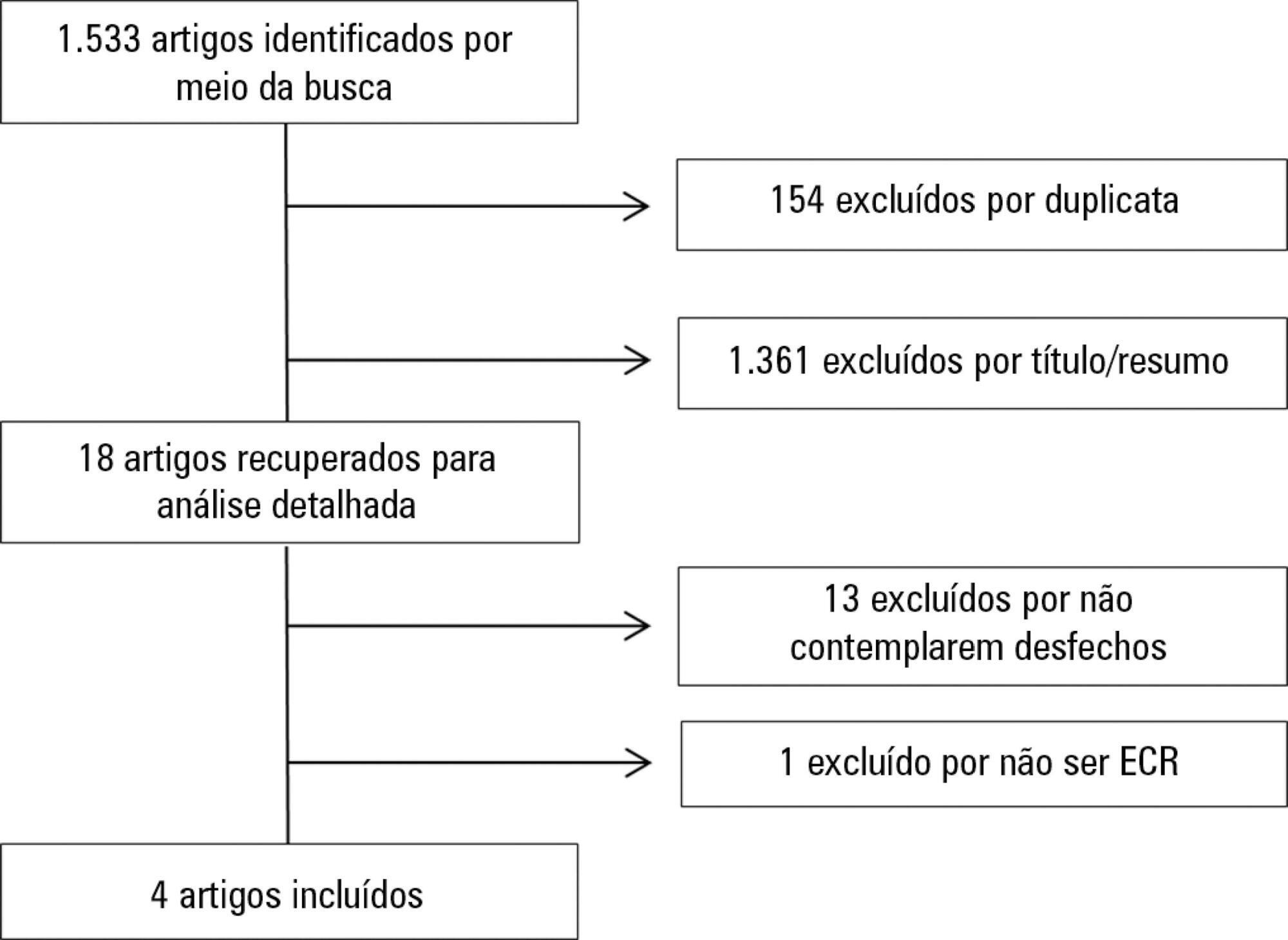
The initial search located 1,533 articles, from which only four randomized clinical trials were included. Two studies assessed safety based on hemodynamic variables, and only one study reported an increase in heart rate, respiratory rate and blood lactate, without clinical relevance. The other two studies assessed safety based on reported adverse effects. In one, 15% of patients described a prickling sensation, without any clinically relevant abnormalities. In the other, one patient suffered a superficial burn due to improper parameter configuration.
Neuromuscular electrical stimulation is safe for critically ill patients; however, it should be applied by duly trained professionals and with proper evidence-based parameters.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):219-225
DOI 10.5935/0103-507X.20180036
To review the evidence on the safety of neuromuscular electrical stimulation when used in the intensive care unit.
A systematic review was conducted; a literature search was performed of the MEDLINE (via PubMed), PEDro, Cochrane CENTRAL and EMBASE databases, and a further manual search was performed among the references cited in randomized studies. Randomized clinical trials that compared neuromuscular electrical stimulation to a control or placebo group in the intensive care unit and reporting on the technique safety in the outcomes were included. Hemodynamic variables and information on adverse effects were considered safety parameters. Articles were independently analyzed by two reviewers, and the data analysis was descriptive.
The initial search located 1,533 articles, from which only four randomized clinical trials were included. Two studies assessed safety based on hemodynamic variables, and only one study reported an increase in heart rate, respiratory rate and blood lactate, without clinical relevance. The other two studies assessed safety based on reported adverse effects. In one, 15% of patients described a prickling sensation, without any clinically relevant abnormalities. In the other, one patient suffered a superficial burn due to improper parameter configuration.
Neuromuscular electrical stimulation is safe for critically ill patients; however, it should be applied by duly trained professionals and with proper evidence-based parameters.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):201-207
DOI 10.5935/0103-507X.20180040
To clinically and demographically characterize potential organ donors admitted to a general intensive care unit and analyze data on donated organs.
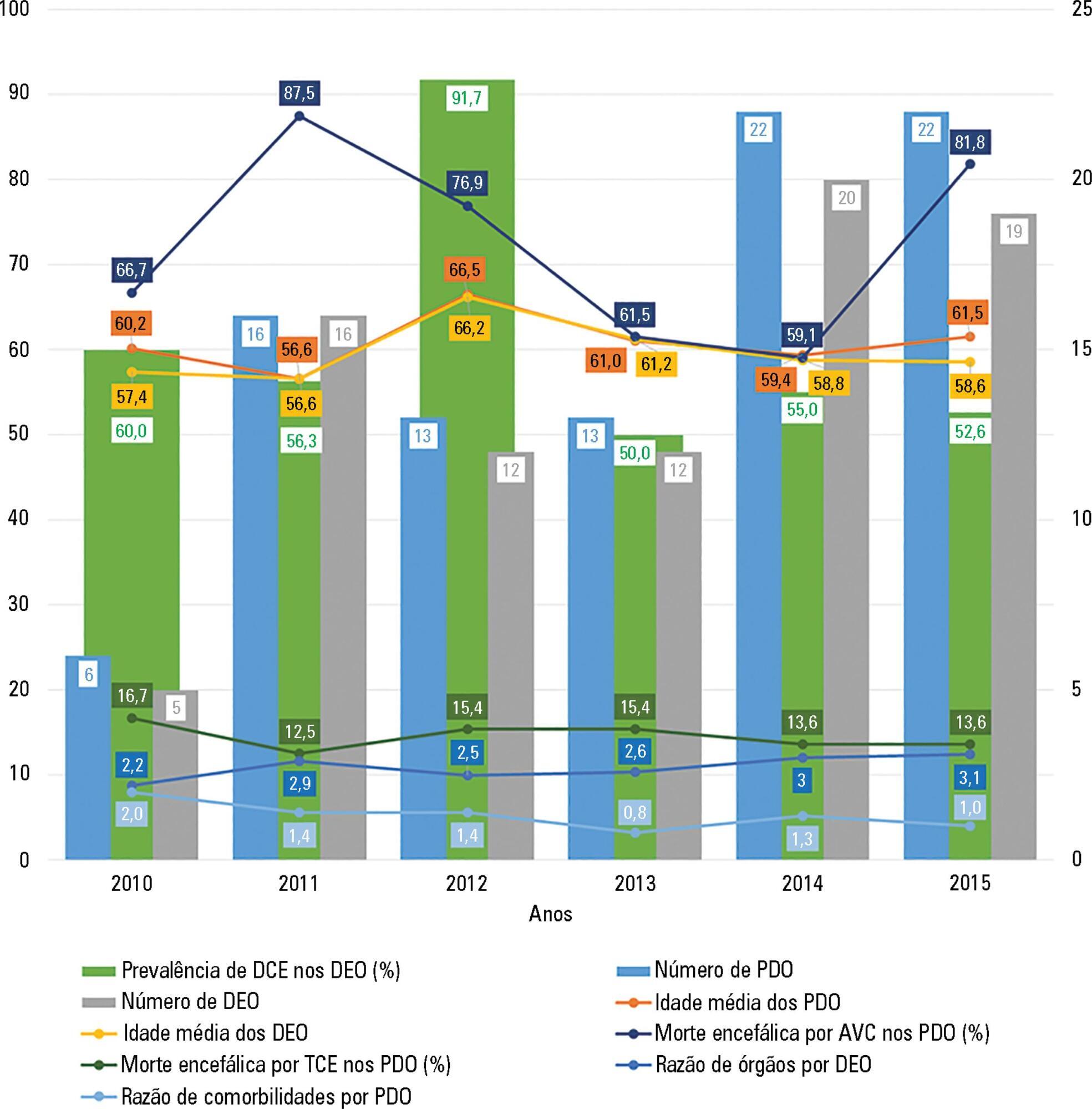
This retrospective study was conducted from 2010 to 2015 and analyzed demographic and clinical variables and the number of harvested organs and tissues.
A total of 92 potential organ donors were identified, of whom eight were non-effective donors and 84 were effective donors (59.5% were expanded criteria donors). The mean age of the potential donors was 60.7 years, and the majority were men. Hemorrhagic stroke accounted for 55.4% of brain deaths. The most common blood type among the donors was A Rh+ (43.5%), and the most common comorbidity was arterial hypertension (43.3%). The most frequently collected organs were the kidneys (84.5%) and liver (66.7%). The average number of organs harvested per donor was 2.8, and this ratio was smaller for donors with expanded criteria compared to other donors.
In most cases, potential organ donors died of brain death, were older than middle age, were male and were victims of a hemorrhagic stroke. The majority of the donors were expanded criteria donors and donated an average of two to three organs. The organs donated most frequently were the kidneys and liver.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):201-207
DOI 10.5935/0103-507X.20180040
To clinically and demographically characterize potential organ donors admitted to a general intensive care unit and analyze data on donated organs.
This retrospective study was conducted from 2010 to 2015 and analyzed demographic and clinical variables and the number of harvested organs and tissues.
A total of 92 potential organ donors were identified, of whom eight were non-effective donors and 84 were effective donors (59.5% were expanded criteria donors). The mean age of the potential donors was 60.7 years, and the majority were men. Hemorrhagic stroke accounted for 55.4% of brain deaths. The most common blood type among the donors was A Rh+ (43.5%), and the most common comorbidity was arterial hypertension (43.3%). The most frequently collected organs were the kidneys (84.5%) and liver (66.7%). The average number of organs harvested per donor was 2.8, and this ratio was smaller for donors with expanded criteria compared to other donors.
In most cases, potential organ donors died of brain death, were older than middle age, were male and were victims of a hemorrhagic stroke. The majority of the donors were expanded criteria donors and donated an average of two to three organs. The organs donated most frequently were the kidneys and liver.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):264-285
DOI 10.5935/0103-507X.20180058
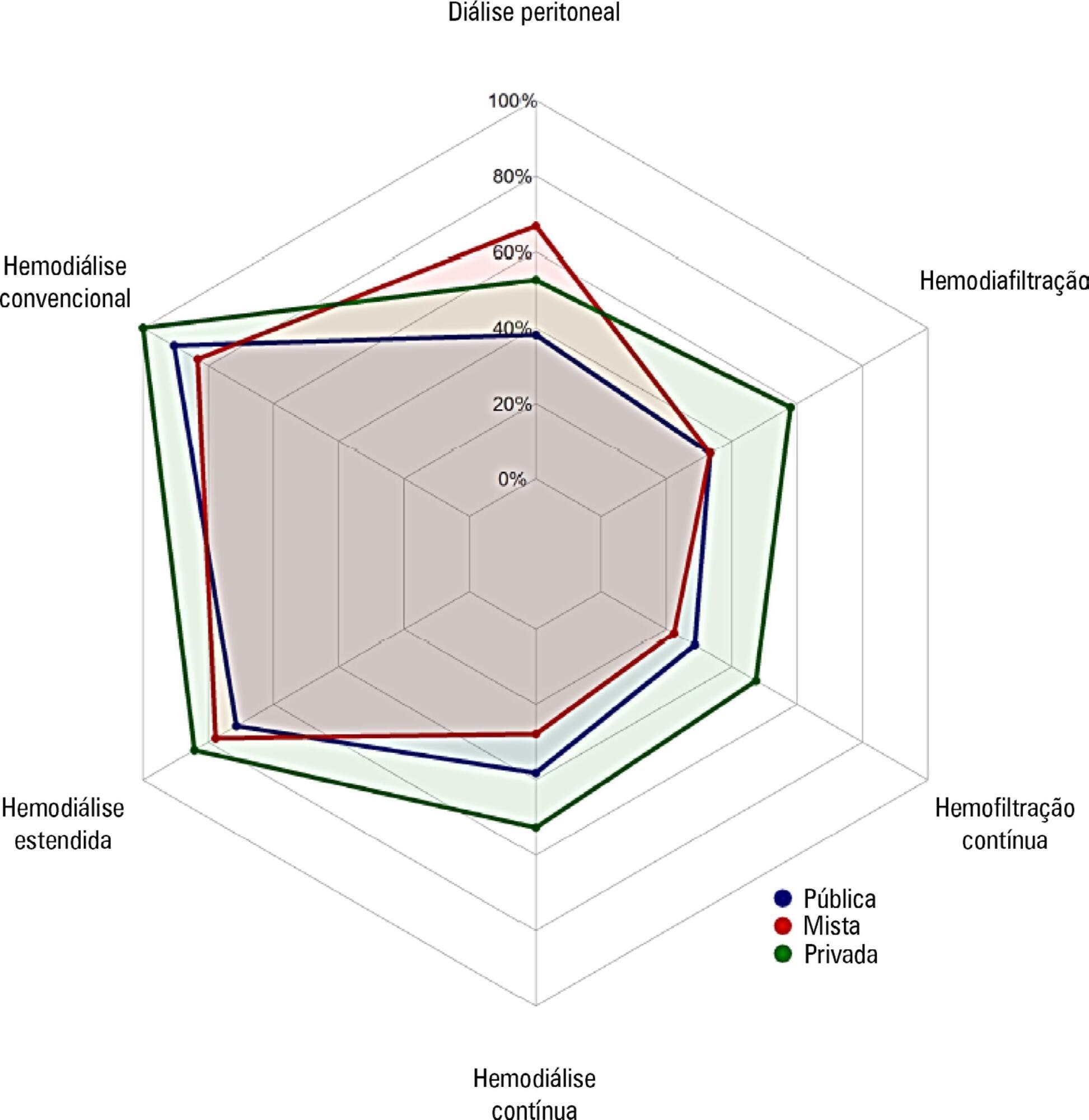
To investigate the existing capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial.
A questionnaire was provided to the chairs of 61 intensive care units enrolled in a randomized clinical trial in Brazil. A total of 124 physicians completed the questionnaire.
Approximately 15% of the patients admitted to the analyzed intensive care units received renal replacement therapy at the time of data collection. At least one renal replacement method was available in all of the analyzed units. Continuous methods were available more frequently at the private units than at the public units. The time from indication to onset of treatment was longer at the public units than at private units. The main obstacles to treatment initiation at public intensive care units were related to the availability of equipment and personnel, while the main bottleneck at private units was the nephrologist assessment. A considerable proportion of the participants stated that they would change their approach to renal replacement therapy if there were no limitations on the availability of methods in their units.
There was wide variation in the availability of resources for renal replacement therapy and in the management of acute kidney injury in Brazilian intensive care units. This information should be taken into account when planning clinical trials focused on this topic in Brazil.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):264-285
DOI 10.5935/0103-507X.20180058
To investigate the existing capacity for renal replacement therapy and site-specific practices for managing acute kidney injury at centers participating in the BaSICS trial.
A questionnaire was provided to the chairs of 61 intensive care units enrolled in a randomized clinical trial in Brazil. A total of 124 physicians completed the questionnaire.
Approximately 15% of the patients admitted to the analyzed intensive care units received renal replacement therapy at the time of data collection. At least one renal replacement method was available in all of the analyzed units. Continuous methods were available more frequently at the private units than at the public units. The time from indication to onset of treatment was longer at the public units than at private units. The main obstacles to treatment initiation at public intensive care units were related to the availability of equipment and personnel, while the main bottleneck at private units was the nephrologist assessment. A considerable proportion of the participants stated that they would change their approach to renal replacement therapy if there were no limitations on the availability of methods in their units.
There was wide variation in the availability of resources for renal replacement therapy and in the management of acute kidney injury in Brazilian intensive care units. This information should be taken into account when planning clinical trials focused on this topic in Brazil.