Critical care Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2011;23(1):62-67
DOI 10.1590/S0103-507X2011000100011
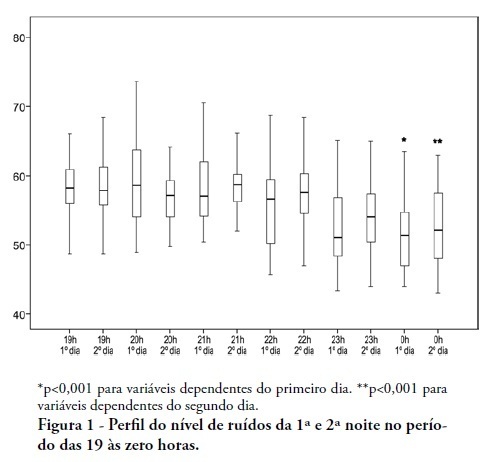
OBJECTIVES: To identify the main causes of stress in patients staying in a coronary unit and to assess the influence of noise levels on their perception of stress. METHODS: This was a prospective, descriptive and quantitative study conducted between June and November 2009 in the Coronary Unit of the Hospital de Clínicas da Universidade Estadual de Campinas. The Intensive Care Unit Environmental Stressor Scale was used on the first, second and third days of hospitalization to identify stressors. The noise level was measured on the first and second nights using an Instrutherm DEC-460 decibel meter. RESULTS: Overall, 32 clinical heart disease patients were included. The median Intensive Care Unit Environmental Stressor Scale scores were 67.5, 60.5 and 59.5 for the first, second and third days, respectively. The differences were not statistically significant. The highest noise level (a median of 58.7 dB) was detected on the second night at 9:00 pm; the lowest level (51.5 dB) was measured on the first night at 12:00 am. In a multiple linear regression model, the first-night noise level had a 33% correlation with the second-day stress scale score, and for the second night, the correlation with the third-day stress scale score was 32.8% (p = 0.001). CONCLUSION: Patients admitted into a coronary unit have an increased perception of stress. Higher noise levels are also responsible for the perception of stress in these patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):62-67
DOI 10.1590/S0103-507X2011000100011
OBJECTIVES: To identify the main causes of stress in patients staying in a coronary unit and to assess the influence of noise levels on their perception of stress. METHODS: This was a prospective, descriptive and quantitative study conducted between June and November 2009 in the Coronary Unit of the Hospital de Clínicas da Universidade Estadual de Campinas. The Intensive Care Unit Environmental Stressor Scale was used on the first, second and third days of hospitalization to identify stressors. The noise level was measured on the first and second nights using an Instrutherm DEC-460 decibel meter. RESULTS: Overall, 32 clinical heart disease patients were included. The median Intensive Care Unit Environmental Stressor Scale scores were 67.5, 60.5 and 59.5 for the first, second and third days, respectively. The differences were not statistically significant. The highest noise level (a median of 58.7 dB) was detected on the second night at 9:00 pm; the lowest level (51.5 dB) was measured on the first night at 12:00 am. In a multiple linear regression model, the first-night noise level had a 33% correlation with the second-day stress scale score, and for the second night, the correlation with the third-day stress scale score was 32.8% (p = 0.001). CONCLUSION: Patients admitted into a coronary unit have an increased perception of stress. Higher noise levels are also responsible for the perception of stress in these patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):68-77
DOI 10.1590/S0103-507X2011000100012
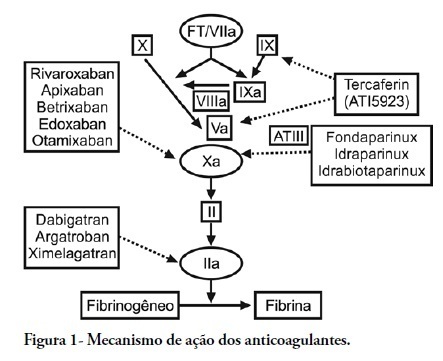
Thromboembolic events commonly occur in critically ill patients, and although they do not consistently present with specific signs and symptoms, they are associated with high morbity and mortality. Antithrombotic agents are the mainstay of the prevention and treatment of venous thromboembolism, and they are also used for stroke prevention in atrial fibrillation, embolism prevention in heart failure, and anticoagulation of prosthetic valves. These drugs have been combined with antiplatelet therapy for the prevention of secondary acute coronary syndrome. Antithrombotic agents such as Aspirin, clopidogrel, vitamin K antagonists and fondaparinux, an indirect Factor Xa inhibitor, are already incorporated into our clinical practice. New small-molecule, selective Factor Xa and thrombin inhibitors that simultaneously inhibit free plasma and clot-associated factor activities have received considerable attention recently. These new oral anticoagulants are in various phases of clinical development. dabigatran, rivaroxaban and apixaban are in more advanced phases of clinical development and are already available in a number of countries. This review article highlights the studies describing the use of these three anticoagulants in an intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):68-77
DOI 10.1590/S0103-507X2011000100012
Thromboembolic events commonly occur in critically ill patients, and although they do not consistently present with specific signs and symptoms, they are associated with high morbity and mortality. Antithrombotic agents are the mainstay of the prevention and treatment of venous thromboembolism, and they are also used for stroke prevention in atrial fibrillation, embolism prevention in heart failure, and anticoagulation of prosthetic valves. These drugs have been combined with antiplatelet therapy for the prevention of secondary acute coronary syndrome. Antithrombotic agents such as Aspirin, clopidogrel, vitamin K antagonists and fondaparinux, an indirect Factor Xa inhibitor, are already incorporated into our clinical practice. New small-molecule, selective Factor Xa and thrombin inhibitors that simultaneously inhibit free plasma and clot-associated factor activities have received considerable attention recently. These new oral anticoagulants are in various phases of clinical development. dabigatran, rivaroxaban and apixaban are in more advanced phases of clinical development and are already available in a number of countries. This review article highlights the studies describing the use of these three anticoagulants in an intensive care setting.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):351-357
DOI 10.1590/S0103-507X2010000400007
OBJECTIVE: To identify the relevant differences between portable blood glucose meter readings in different sampling accesses blood and laboratory analysis. METHODS: Quantitative validity study. Daily samples were collected from capillary blood, central venous access catheter and arterial catheter and the blood glucose values checked using portable blood glucose meter and laboratory analysis. The findings were analyzed with the Statistical Package for the Social Sciences - SPSS software. RESULTS: Central venous catheter samples blood glucose meter readings were found to have the best correlation with the laboratory analysis results, considered as the gold-standard. CONCLUSION: Hemodynamically unstable patients' capillary blood samples may provide false blood glucose results, and lead to inappropriate insulin solution management. Therefore, ideal blood glucose sampling is relevant to prevent insulin solution management errors.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):351-357
DOI 10.1590/S0103-507X2010000400007
OBJECTIVE: To identify the relevant differences between portable blood glucose meter readings in different sampling accesses blood and laboratory analysis. METHODS: Quantitative validity study. Daily samples were collected from capillary blood, central venous access catheter and arterial catheter and the blood glucose values checked using portable blood glucose meter and laboratory analysis. The findings were analyzed with the Statistical Package for the Social Sciences - SPSS software. RESULTS: Central venous catheter samples blood glucose meter readings were found to have the best correlation with the laboratory analysis results, considered as the gold-standard. CONCLUSION: Hemodynamically unstable patients' capillary blood samples may provide false blood glucose results, and lead to inappropriate insulin solution management. Therefore, ideal blood glucose sampling is relevant to prevent insulin solution management errors.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):270-273
DOI 10.1590/S0103-507X2010000300009
OBJECTIVE: To evaluate the prevalence of gastrointestinal complications and protein-calorie adequacy in critical patients using enteral nutrition therapy. METHODS: This was a retrospective study in the intensive care unit of the Hospital das Clinicas of the Universidade Federal de Pernambuco involving analysis of nutritional records evaluating the most frequent gastrointestinal complications during the patients' hospitalization and protein-calorie supply requirements. It was considered offered, the volume and formula effectively received by the patient on the last hospitalization day. The SPSS version 13 software was used for statistical analysis. RESULTS: The sample consisted of 77 patients aged in average 54.7 ± 18.1 years who were predominantly female (54.5%). The diet offered was appropriate and all patients had some type of gastrointestinal complications, being high gastric residuals the most prevalent (39%), followed by constipation (36.4%). CONCLUSION: Despite the high prevalence of gastrointestinal complications, no mismatches were observed in protein-calorie intake. Multidisciplinary approaches to these complications should be standardized in order to provide their early resolution.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):270-273
DOI 10.1590/S0103-507X2010000300009
OBJECTIVE: To evaluate the prevalence of gastrointestinal complications and protein-calorie adequacy in critical patients using enteral nutrition therapy. METHODS: This was a retrospective study in the intensive care unit of the Hospital das Clinicas of the Universidade Federal de Pernambuco involving analysis of nutritional records evaluating the most frequent gastrointestinal complications during the patients' hospitalization and protein-calorie supply requirements. It was considered offered, the volume and formula effectively received by the patient on the last hospitalization day. The SPSS version 13 software was used for statistical analysis. RESULTS: The sample consisted of 77 patients aged in average 54.7 ± 18.1 years who were predominantly female (54.5%). The diet offered was appropriate and all patients had some type of gastrointestinal complications, being high gastric residuals the most prevalent (39%), followed by constipation (36.4%). CONCLUSION: Despite the high prevalence of gastrointestinal complications, no mismatches were observed in protein-calorie intake. Multidisciplinary approaches to these complications should be standardized in order to provide their early resolution.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
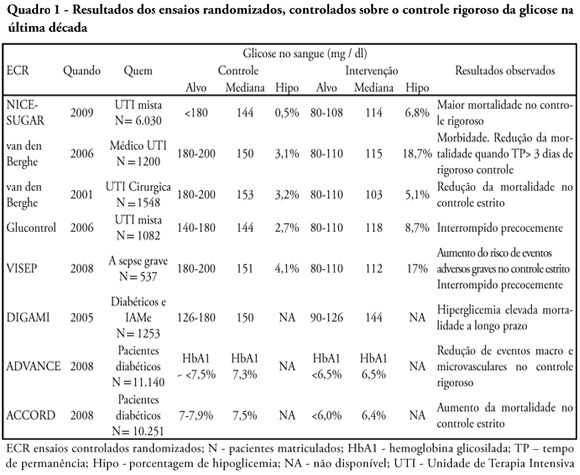
Glucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient's safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
Glucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient's safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):324-331
DOI 10.1590/S0103-507X2009000300014
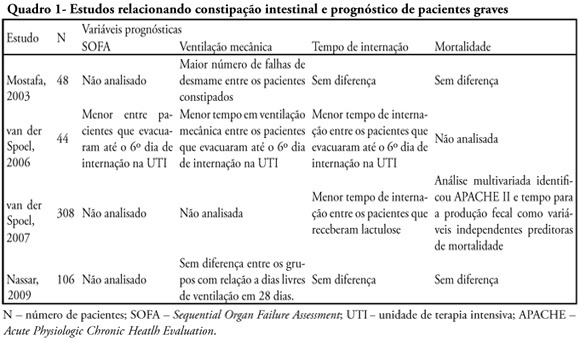
Constipation is a common complication identified among critically ill patients. Its incidence is highly variable due to lack of definition of such patients. Besides the already known consequences of constipation, in recent years it was observed that this complication may also be related to worse prognosis of critically ill patients. This review endeavors to describe the main available scientific evidence showing that constipation is a prognostic marker and a clinical representation of intestinal dysfunction, in addition to eventually interfering in the prognosis with treatment. Ogilvie syndrome, a major cause of morbidity and mortality in intensive care units was also reviewed. Considering the above cases it was concluded that more attention to this disorder is required in intensive care units as well as development of protocols for diagnosis and management of critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2009;21(3):324-331
DOI 10.1590/S0103-507X2009000300014
Constipation is a common complication identified among critically ill patients. Its incidence is highly variable due to lack of definition of such patients. Besides the already known consequences of constipation, in recent years it was observed that this complication may also be related to worse prognosis of critically ill patients. This review endeavors to describe the main available scientific evidence showing that constipation is a prognostic marker and a clinical representation of intestinal dysfunction, in addition to eventually interfering in the prognosis with treatment. Ogilvie syndrome, a major cause of morbidity and mortality in intensive care units was also reviewed. Considering the above cases it was concluded that more attention to this disorder is required in intensive care units as well as development of protocols for diagnosis and management of critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
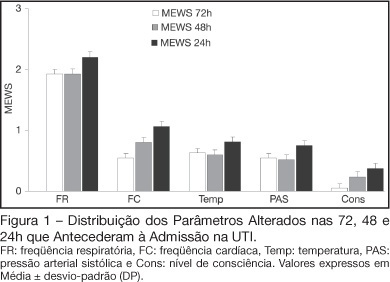
BACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission - 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):124-127
DOI 10.1590/S0103-507X2008000200002
BACKGROUND AND OBJECTIVES: Prognosis of patients in the intensive care unit (ICU) has a relation with their severity just before admission. The Modified Early Warning Score (MEWS) was used to evaluate the severe condition of patients 12, 24 and 72 hours before admission in the ICU, assess the most prevalent parameters and correlate the MEWS before ICU with the outcome (survival versus death). METHODS: Retrospective analyses of 65 patients consecutively admitted to the ICU from July to October, 2006 evaluating the physiological parameters 72 hours prior to admission. RESULTS: APACHE II mean was 22.2 ± 7.9 points, mortality was 54.6% and standardized mortality ratio means was 1.24. MEWS means were 3.7 ± 0.2; 4.0 ± 0.2 and 5.1 ± 0.2 points, calculated 72, 48 and 24 hours previous to ICU admission, respectively. An increasing percentage of patients with MEWS > 3 points within 72, 48 and 24 hours before admission - 43.8%, 59.4% and 73.4%, respectively was recorded. Among the included physiological parameters respiratory rate contributed the most to the MEWS. Highest mortality was found in patients with MEWS > 3 points already found 72 hours before admission. Patients who died presented with a significant increase in the MEWS 24 hours prior to admission to the ICU (in relation to the MEWS recorded 72 hours before) but the situation was not identified in survivors. CONCLUSIONS: MEWS closely identified the severity of patients admitted to the ICU, suggesting that it can be a reliable score, useful in the situations preceding the ICU.