Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Cassiano Teixeira"
We found (45) results for your search.Abstract
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 - 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Abstract
Crit Care Sci. 2023;35(1):31-36
DOI 10.5935/2965-2774.20230113-pt
To evaluate the impact of an educational website on satisfaction and symptoms of anxiety and depression among family members of critically ill adult patients.
We embedded an analysis of website access in a cohort study conducted in intensive care units with flexible visiting hours in Brazil. Family members were guided to access an educational website designed to help them understand the processes and emotions associated with an intensive care unit stay. Subjects were evaluated for baseline data within the first 48 hours following enrollment and outcome assessment at up to 7 days after patient discharge from the intensive care unit, death, or until the 30th day of the study. The main outcomes were satisfaction using the Critical Care Family Needs Inventory and the presence of anxiety and depression symptoms using the Hospital Anxiety and Depression Scale.
A total of 532 family members were evaluated during the study period. Of these, 61 (11.5%) accessed the website. After adjustments, family members who accessed the website had significantly better mean Critical Care Family Needs Inventory scores (152.8 versus 145.2, p = 0.01) and a lower prevalence of probable clinical anxiety (prevalence ratio 0.35; 95%CI 0.14 - 0.89) than family members who did not access the website. There were no differences regarding symptoms of depression.
Access to an educational website was associated with higher family satisfaction with care and a lower prevalence of clinical anxiety.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
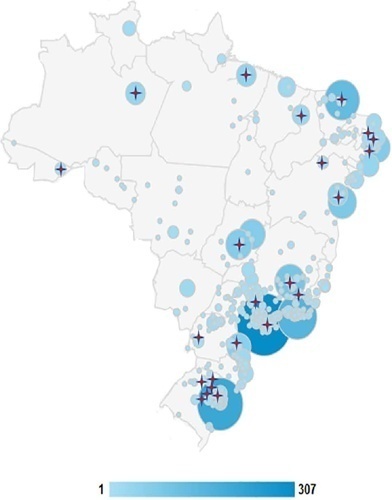
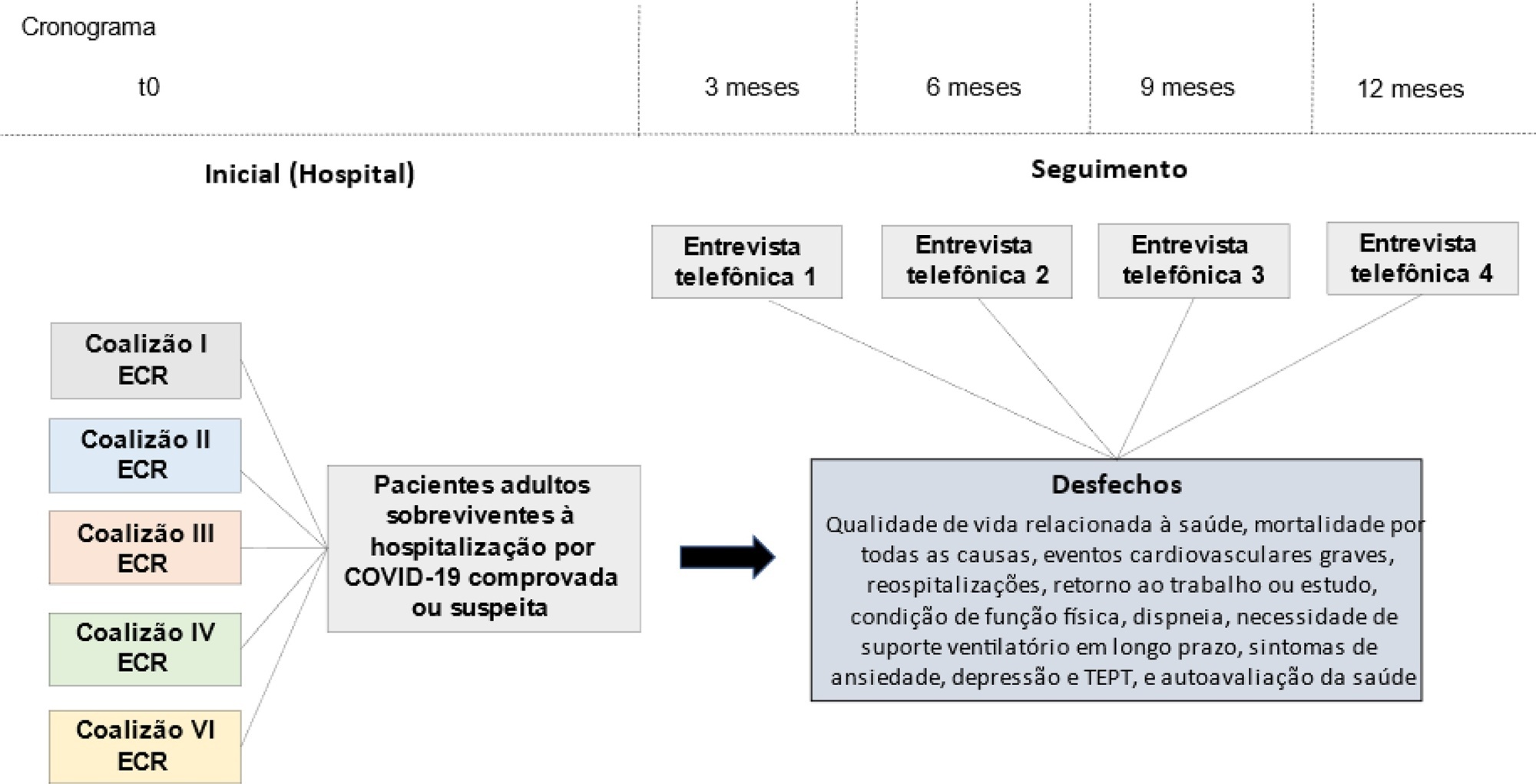
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Abstract
Rev Bras Ter Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
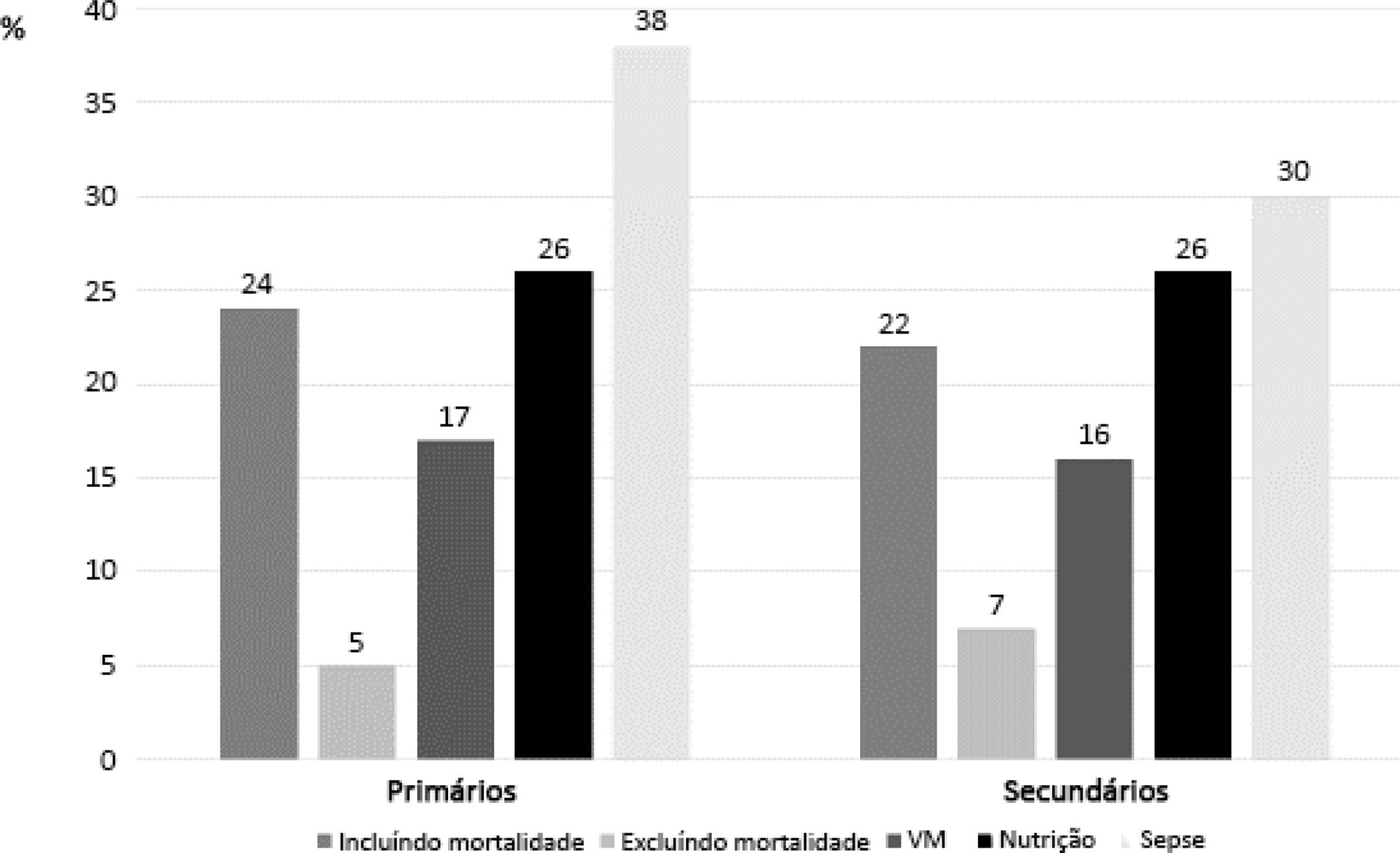
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):312-319
DOI 10.5935/0103-507X.20210040
Randomized clinical trials in intensive care prioritize disease-focused outcomes rather than patient-centered outcomes. A paradigm shift considering the evaluation of measures after hospital discharge and measures focused on quality of life and common symptoms, such as pain and dyspnea, could better reflect the wishes of patients and their families. However, barriers related to the systematization of the interpretation of these outcomes, the heterogeneity of measurement instruments and the greater difficulty in performing the studies, to date, seem to hinder this change. In addition, the joint participation of patients, families, researchers, and clinicians in the definition of study outcomes is not yet a reality.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):315-320
DOI 10.1590/S0103-507X2010000400001
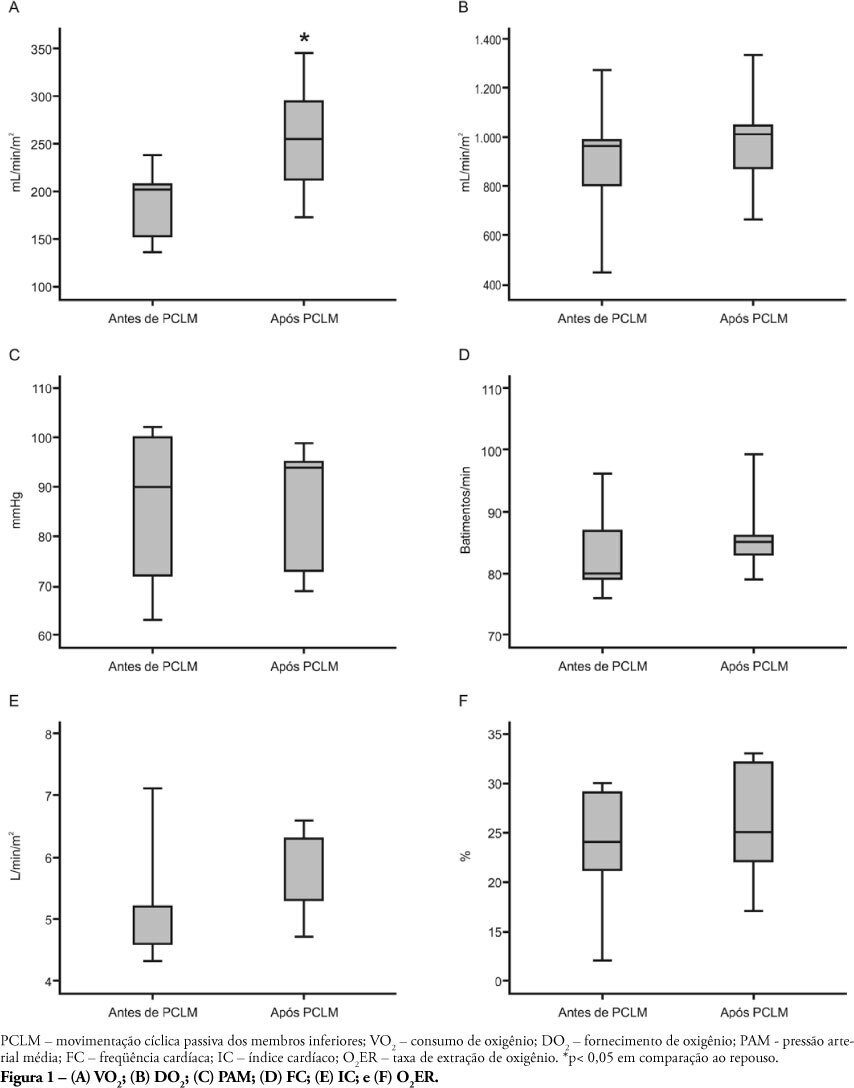
OBJECTIVE: Limb movements, passively performed by a physiotherapist, have been shown to result in significant increases in critically ill patients' metabolic and hemodynamic variables. This study objective was to determine whether passive cycling leg movement increases hemodynamic and metabolic variables in sedated mechanical ventilation dependent patients. METHODS: Five sedated mechanical ventilation dependent patients in a 18-bed intensive care unit of a university hospital were evaluated. Passive cycling leg movements were performed for 10min at a 30 movements/min rate. Complete hemodynamical data were recorded and arterial and mixed venous blood sample were collected 5 minutes before and after 5 minutes after the maneuver completion. RESULTS: All patients had increased oxygen consumption (VO2). The VO2 increase occurred with a concomitant drop in mixed venous blood saturation (SvO2), likely from both oxygen extraction ratio (O2ER) and cardiac index (CI) increase. CONCLUSION: passive cycling leg movements may influence hemodynamical and metabolic status in sedated mechanical ventilation-dependent patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):315-320
DOI 10.1590/S0103-507X2010000400001
OBJECTIVE: Limb movements, passively performed by a physiotherapist, have been shown to result in significant increases in critically ill patients' metabolic and hemodynamic variables. This study objective was to determine whether passive cycling leg movement increases hemodynamic and metabolic variables in sedated mechanical ventilation dependent patients. METHODS: Five sedated mechanical ventilation dependent patients in a 18-bed intensive care unit of a university hospital were evaluated. Passive cycling leg movements were performed for 10min at a 30 movements/min rate. Complete hemodynamical data were recorded and arterial and mixed venous blood sample were collected 5 minutes before and after 5 minutes after the maneuver completion. RESULTS: All patients had increased oxygen consumption (VO2). The VO2 increase occurred with a concomitant drop in mixed venous blood saturation (SvO2), likely from both oxygen extraction ratio (O2ER) and cardiac index (CI) increase. CONCLUSION: passive cycling leg movements may influence hemodynamical and metabolic status in sedated mechanical ventilation-dependent patients.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
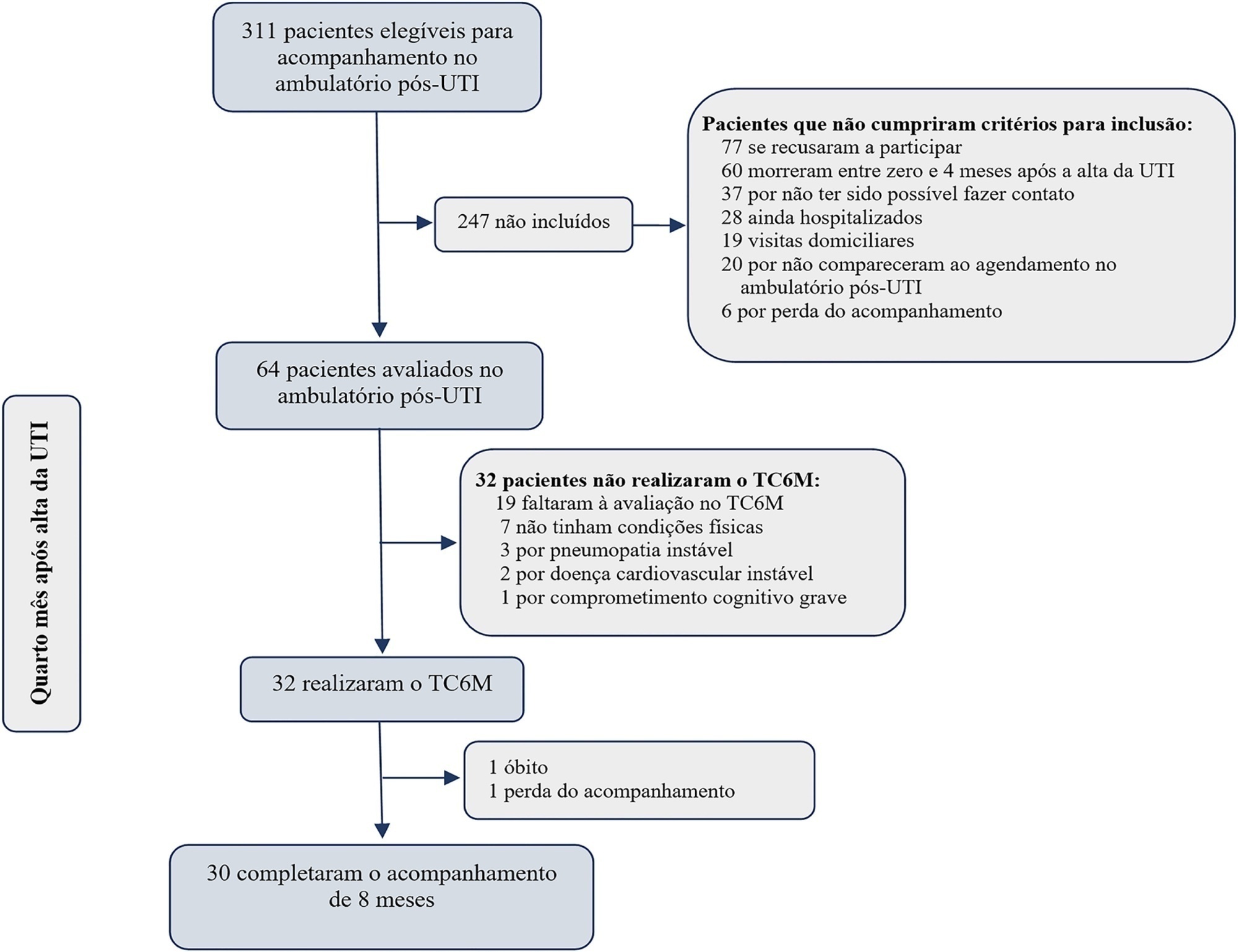
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):374-383
DOI 10.5935/0103-507X.20210056
To evaluate the ability of the 6-Minute Walk Test to predict long-term physical functional status improvement among intensive care unit survivors.
Thirty-two intensive care unit survivors were prospectively evaluated from February 2017 to August 2018 in a post-intensive care unit outpatient clinic in Brazil. Individuals with intensive care unit stays > 72 hours (emergency admissions) or > 120 hours (elective admissions) attending the post-intensive care unit clinic four months after intensive care unit discharge were consecutively enrolled. The association between the 6-Minute Walk Test distance at baseline and physical functional status was assessed over 8 months using the Barthel Index.
The mean 6-Minute Walk Test distance was significantly lower in intensive care unit survivors than in the general population (405m versus 557m; p < 0.001). Age (β = -4.0; p < 0.001) and muscle weakness (β = -99.7; p = 0.02) were associated with the 6-Minute Walk Test distance. A 6-Minute Walk Test distance was associated with improvement in physical functional status over the 8-month follow-up (odds ratio for each 10m of 1.07; 95%CI 1.01 - 1.16; p = 0.03). The area under the Receiver Operating Characteristic curve for the 6-Minute Walk Test prediction of physical functional status improvement was 0.72 (95%CI 0.53 - 0.88).
The 6-Minute Walk Test performed 4 months after intensive care unit discharge predicted long-term physical functional status among intensive care unit survivors with moderate accuracy.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2022;34(3):374-379
DOI 10.5935/0103-507X.20220114-en
To compare the perceptions of patients’ relatives with the perceptions of health professionals regarding a flexible visitation model in intensive care units.
Cross-sectional study. This study was carried out with patients’ relatives and members of the care team of a clinical-surgical intensive care unit with a flexible visitation model (12 hours/day) from September to December 2018. The evaluation of the flexible visitation policy was carried out through an open visitation instrument composed of 22 questions divided into three domains (evaluation of family stress, provision of information, and interference in the work of the team).
Ninety-five accompanying relatives and 95 members of the care team were analyzed. The perceptions of relatives regarding the decrease in anxiety and stress with flexible visitation was higher than the perceptions of the team (91.6% versus 58.9%, p < 0.001), and the family also had a more positive perception regarding the provision of information (86.3% versus 64.2%, p < 0.001). The care team believed that the presence of the relative made it difficult to provide care to the patient and caused work interruptions (46.3% versus 6.3%, p < 0.001).
Family members and staff-intensive care unit teams have different perceptions about flexible visits in the intensive care unit. However, a positive view regarding the perception of decreased anxiety and stress among the family members and greater information and contributions to patient recovery predominates.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):386-392
DOI 10.5935/0103-507X.20190051
The improvement in cardiopulmonary resuscitation quality has reduced the mortality of individuals treated for cardiac arrest. However, survivors have a high risk of severe brain damage in cases of return of spontaneous circulation. Data suggest that cases of cardiac arrest in critically ill patients with non-shockable rhythms have only a 6% chance of returning of spontaneous circulation, and of these, only one-third recover their autonomy. Should we, therefore, opt for a procedure in which the chance of survival is minimal and the risk of hospital death or severe and definitive brain damage is approximately 70%? Is it worth discussing patient resuscitation in cases of cardiac arrest? Would this discussion bring any benefit to the patients and their family members? Advanced discussions on do-not-resuscitate are based on the ethical principle of respect for patient autonomy, as the wishes of family members and physicians often do not match those of patients. In addition to the issue of autonomy, advanced discussions can help the medical and care team anticipate future problems and, thus, better plan patient care. Our opinion is that discussions regarding the resuscitation of critically ill patients should be performed for all patients within the first 24 to 48 hours after admission to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):398-403
DOI 10.1590/S0103-507X2009000400010
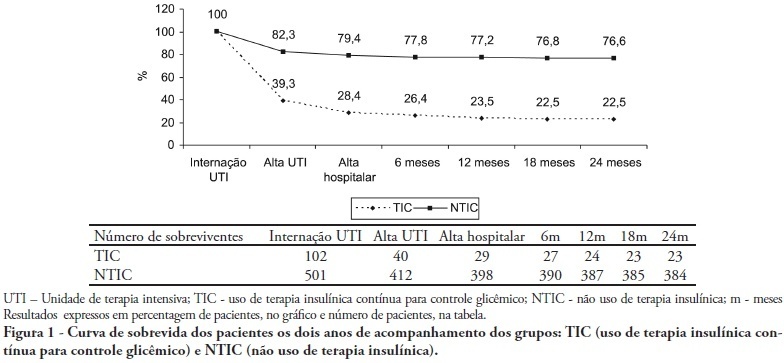
OBJECTIVES: Stress-induced hyperglycemia is frequent in critically ill patients and has been associated with increased mortality and morbidity (both in diabetic and non-diabetic patients). This study objective was to evaluate the profile and long-term prognosis of critically ill patients undergoing tight glucose-control. METHODS: Prospective cohort. All patients admitted to the intensive care unit over 1-year were enrolled. We analyzed demographic data, therapeutic intervention, and short- (during the stay) and long-term (2 years after discharge) mortality. The patients were categorized in 2 groups: tight glucose control and non-tight glucose-control, based on the unit staff decision. RESULTS: From the 603 enrolled patients, 102 (16.9%) underwent tight control (glucose <150 mg/dL) while 501 patients (83.1%) non-tight control. Patients in the TGC-group were more severely ill than those in the non-tight control group [APACHE II score (14 ± 3 versus 11 ± 4, P=0.04), SOFA (4.9 ± 3.2 versus 3.5 ± 3.4, P<0.001) and TISS-24h (25.7 ± 6.9 versus 21.1 ± 7.2, P< 0.001)]. The tight control group patients also had worse prognosis: [acute renal failure (51% versus 18.5%, P<0.001), critical illness neuropathy (16.7% versus 5.6%, P<0.001)] and increased mortality (during the ICU-stay [60.7% versus 17.7%, P<0.001] and within 2-years of the discharge [77.5% versus 23.4%; P<0.001]). CONCLUSION: Critically ill patients needing tight glucose control during the unit stay have more severe disease and have worse short and long-term prognosis.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):398-403
DOI 10.1590/S0103-507X2009000400010
OBJECTIVES: Stress-induced hyperglycemia is frequent in critically ill patients and has been associated with increased mortality and morbidity (both in diabetic and non-diabetic patients). This study objective was to evaluate the profile and long-term prognosis of critically ill patients undergoing tight glucose-control. METHODS: Prospective cohort. All patients admitted to the intensive care unit over 1-year were enrolled. We analyzed demographic data, therapeutic intervention, and short- (during the stay) and long-term (2 years after discharge) mortality. The patients were categorized in 2 groups: tight glucose control and non-tight glucose-control, based on the unit staff decision. RESULTS: From the 603 enrolled patients, 102 (16.9%) underwent tight control (glucose <150 mg/dL) while 501 patients (83.1%) non-tight control. Patients in the TGC-group were more severely ill than those in the non-tight control group [APACHE II score (14 ± 3 versus 11 ± 4, P=0.04), SOFA (4.9 ± 3.2 versus 3.5 ± 3.4, P<0.001) and TISS-24h (25.7 ± 6.9 versus 21.1 ± 7.2, P< 0.001)]. The tight control group patients also had worse prognosis: [acute renal failure (51% versus 18.5%, P<0.001), critical illness neuropathy (16.7% versus 5.6%, P<0.001)] and increased mortality (during the ICU-stay [60.7% versus 17.7%, P<0.001] and within 2-years of the discharge [77.5% versus 23.4%; P<0.001]). CONCLUSION: Critically ill patients needing tight glucose control during the unit stay have more severe disease and have worse short and long-term prognosis.