Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Glauco Adrieno Westphal"
We found (28) results for your search.Abstract
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
OBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student's t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):334-340
DOI 10.1590/S0103-507X2012000400007
OBJECTIVE: To assess the effect of the application of a managed protocol for the maintenance care of deceased potential multiple organ donors at two hospitals. METHODS: A before (Phase 1)/after (Phase 2) study conducted at two general hospitals, which included consecutively potential donors admitted to two intensive care units. In Phase 1 (16 months), the data were collected retrospectively, and the maintenance care measures of the potential donors were instituted by the intensivists. In Phase 2 (12 months), the data collection was prospective, and a managed protocol was used for maintenance care. The two phases were compared in terms of their demographic variables, physiological variables at diagnosis of brain death and the end of the process, time to performance of brain death confirmatory test and end of the process, adherence to bundles of maintenance care essential measures, losses due to cardiac arrest, family refusal, contraindications, and the conversion rate of potential into actual donors. Student's t- and chi-square tests were used, and p-value < 0.05 was considered to be significant. RESULTS: A total of 42 potential donors were identified (18 in Phase 1 and 24 in Phase 2). The time interval between the first clinical assessment and the recovery decreased in Phase 2 (Phase 1: 35.0±15.5 hours versus Phase 2: 24.6±6.2 hours; p = 0.023). Adherence increased to 10 out of the 19 essential items of maintenance care, and losses due to cardiac arrest also decreased in Phase 2 (Phase 1: 27.8 versus 0% in Phase 2; p = 0.006), while the convertion rate increased (Phase 1: 44.4 versus 75% in Phase 2; p = 0.044). The losses due to family refusal and medical contraindication did not vary. CONCLUSION: The adoption of a managed protocol focused on the application of essential measures for the care of potential deceased donors might reduce the loss of potential donors due to cardiac arrest.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
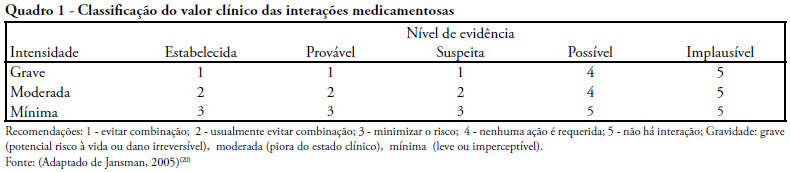
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):349-354
DOI 10.1590/S0103-507X2008000400006
OBJECTIVES: Drug interactions occur when effects and/or toxicity of a drug are affected by presence of another drug. They are usually unpredictable and undesirable. A study was conducted to verify the prevalence and clinical value of potential drug interactions in intensive care units METHODS: All patients, of three intensive care units were included in a cross-sectional study, over a period of two months. Patients with less than a 2 days length of stay were excluded. Data were collected from twenty-four hour prescriptions and all possible paired combinations drug-drug were recorded. Prevalence and clinical value (significance) were checked at the end of follow-up. RESULTS: One hundred and forty patients were analyzed, 67.1% presented with some significant potential drug interactions and of the 1069 prescriptions, 39.2% disclosed the same potential. Of 188 different potential drug interactions, 29 were considered highly significant. Univariate analysis showed that in the group with significant potential drug interactions a higher number of different drugs, drugs/day had been used, there were more prescribing physicians and extended stay in intensive care units. Adjusted to the multivariate logistic regression model, only the number of drugs/day correlated with increased risk of significant potential drug interaction (p = 0.0011) and, furthermore that use of more than 6 drugs/day increased relative risk by 9.8 times. CONCLUSIONS: Critically ill patients are submitted to high risk of potential drug interactions and the number of drugs/day has a high positive predictive value for these interactions. Therefore, it is imperative that critical care physicians be constantly alert to recognize this problem and provide appropriate mechanisms for management, thereby reducing adverse outcomes.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):36-40
DOI 10.1590/S0103-507X2011000100007
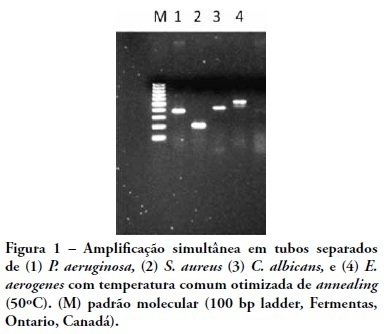
INTRODUCTION: Sepsis is a systemic inflammatory response related to high mortality rates in the hospital environment. Delayed etiological diagnosis and inadequate antimicrobial therapy are associated with treatment failures. Molecular tests based on polymerase chain reaction are regarded as faster and more accurate procedures than culture techniques for microbial identification, providing a higher rate of therapeutic success. OBJECTIVE: To develop a panel of primers for DNA fragments of sepsis-related microorganisms. METHODS: Primers for amplification of Enterobacter spp., Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus and Candida spp. were designed and tested for sensitivity and specificity on the basis of their respective standard strains. RESULTS: The intended specificity was obtained for P. aeruginosa, S. aureus and Candida spp primers. Sensitivity tests showed a threshold for detection from 5 ng to 500 fg in blood samples contaminated with microbial DNA. CONCLUSIONS: The molecular panel presented offers the advantage of a flexible 'open' system when compared to other multiplex detection methods.
Abstract
Rev Bras Ter Intensiva. 2011;23(1):36-40
DOI 10.1590/S0103-507X2011000100007
INTRODUCTION: Sepsis is a systemic inflammatory response related to high mortality rates in the hospital environment. Delayed etiological diagnosis and inadequate antimicrobial therapy are associated with treatment failures. Molecular tests based on polymerase chain reaction are regarded as faster and more accurate procedures than culture techniques for microbial identification, providing a higher rate of therapeutic success. OBJECTIVE: To develop a panel of primers for DNA fragments of sepsis-related microorganisms. METHODS: Primers for amplification of Enterobacter spp., Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus and Candida spp. were designed and tested for sensitivity and specificity on the basis of their respective standard strains. RESULTS: The intended specificity was obtained for P. aeruginosa, S. aureus and Candida spp primers. Sensitivity tests showed a threshold for detection from 5 ng to 500 fg in blood samples contaminated with microbial DNA. CONCLUSIONS: The molecular panel presented offers the advantage of a flexible 'open' system when compared to other multiplex detection methods.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):374-380
DOI 10.5935/0103-507X.20200065
To evaluate whether the decrease in blood pressure caused by the increase in the positive end-expiratory pressure corresponds to the pulse pressure variation as an indicator of fluid responsiveness.
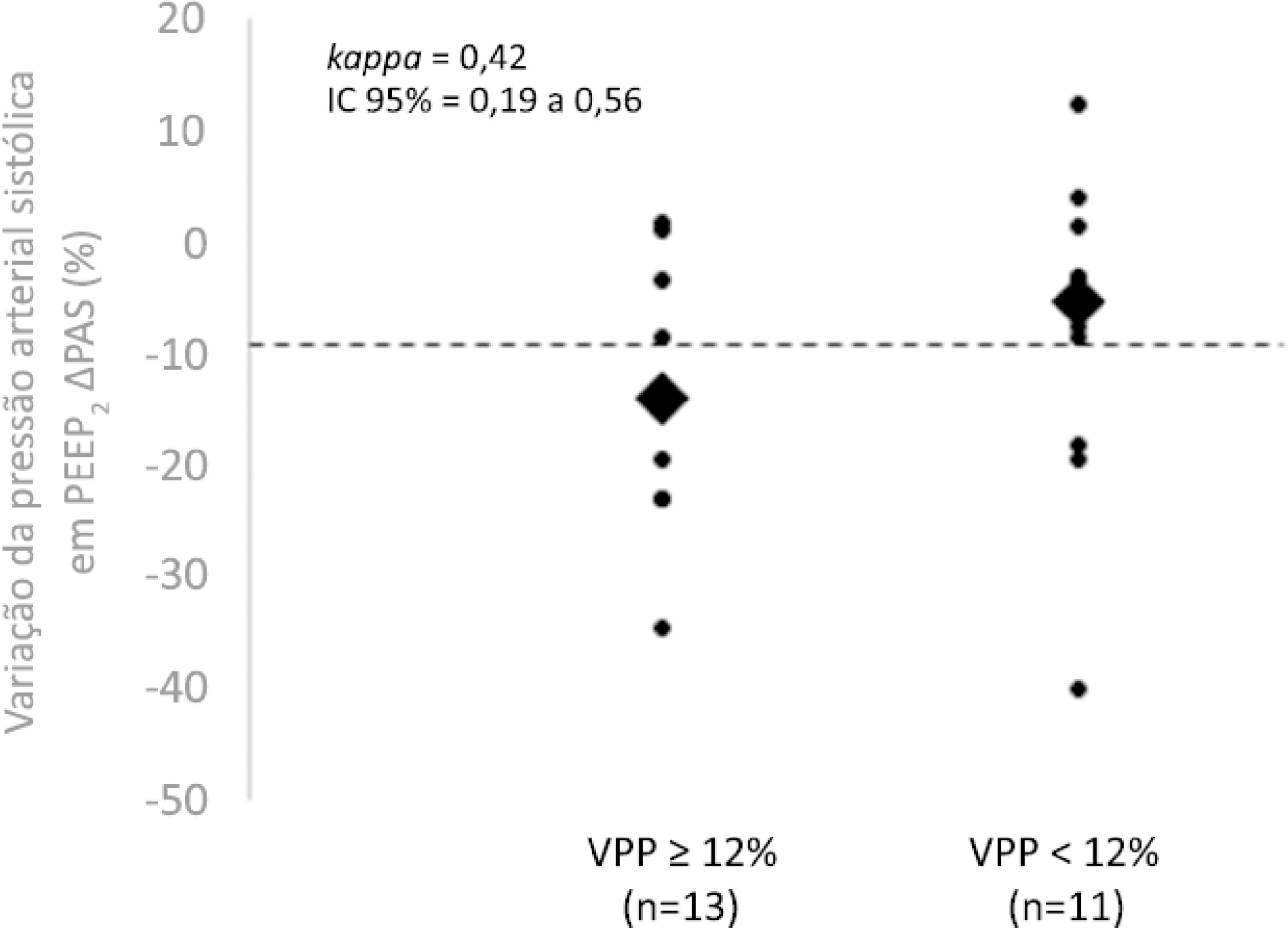
This exploratory study prospectively included 24 patients with septic shock who were mechanically ventilated and subjected to three stages of elevation of the positive end-expiratory pressure: from 5 to 10cmH2O (positive end-expiratory pressure level 1), from 10 to 15cmH2O (positive end-expiratory pressure level 2), and from 15 to 20cmH2O (positive end-expiratory pressure level 3). Changes in systolic blood pressure, mean arterial pressure, and pulse pressure variation were evaluated during the three maneuvers. The patients were classified as responsive (pulse pressure variation ≥ 12%) or unresponsive to volume replacement (pulse pressure variation < 12%).
The best performance at identifying patients with pulse pressure variation ≥ 12% was observed at the positive end-expiratory pressure level 2: -9% systolic blood pressure variation (area under the curve 0.73; 95%CI: 0.49 - 0.79; p = 0.04), with a sensitivity of 63% and specificity of 80%. Concordance was low between the variable with the best performance (variation in systolic blood pressure) and pulse pressure variation ≥ 12% (kappa = 0.42; 95%CI: 0.19 - 0.56). The systolic blood pressure was < 90mmHg at positive end-expiratory pressure level 2 in 29.2% of cases and at positive end-expiratory pressure level 3 in 41.63% of cases.
Variations in blood pressure in response to the increase in positive end-expiratory pressure do not reliably reflect the behavior of the pulse pressure as a measure to identify the fluid responsiveness status.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):374-380
DOI 10.5935/0103-507X.20200065
To evaluate whether the decrease in blood pressure caused by the increase in the positive end-expiratory pressure corresponds to the pulse pressure variation as an indicator of fluid responsiveness.
This exploratory study prospectively included 24 patients with septic shock who were mechanically ventilated and subjected to three stages of elevation of the positive end-expiratory pressure: from 5 to 10cmH2O (positive end-expiratory pressure level 1), from 10 to 15cmH2O (positive end-expiratory pressure level 2), and from 15 to 20cmH2O (positive end-expiratory pressure level 3). Changes in systolic blood pressure, mean arterial pressure, and pulse pressure variation were evaluated during the three maneuvers. The patients were classified as responsive (pulse pressure variation ≥ 12%) or unresponsive to volume replacement (pulse pressure variation < 12%).
The best performance at identifying patients with pulse pressure variation ≥ 12% was observed at the positive end-expiratory pressure level 2: -9% systolic blood pressure variation (area under the curve 0.73; 95%CI: 0.49 - 0.79; p = 0.04), with a sensitivity of 63% and specificity of 80%. Concordance was low between the variable with the best performance (variation in systolic blood pressure) and pulse pressure variation ≥ 12% (kappa = 0.42; 95%CI: 0.19 - 0.56). The systolic blood pressure was < 90mmHg at positive end-expiratory pressure level 2 in 29.2% of cases and at positive end-expiratory pressure level 3 in 41.63% of cases.
Variations in blood pressure in response to the increase in positive end-expiratory pressure do not reliably reflect the behavior of the pulse pressure as a measure to identify the fluid responsiveness status.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):403-409
DOI 10.5935/0103-507X.20190050
Brain death, defined as the complete and irreversible loss of brain functions, has a history that is linked to the emergence of intensive care units and the advancement of artificial ventilatory support. In Brazil, by federal law, the criteria for the diagnosis of brain death have been defined by the Federal Council of Medicine since 1997 and apply to the entire Brazilian territory. Resolution 2,173/2017 of the Federal Council of Medicine updated the criteria for diagnosing brain death. These changes include the following: the requirement for the patient to meet specific physiological prerequisites and for the physician to provide optimized care to the patient before starting the procedures for diagnosing brain death and to perform complementary tests, as well as the need for specific training for physicians who make this diagnosis. Other changes include the reduction of the time interval between the two clinical examinations, the possibility of continuing procedures in the presence of unilateral ear or eye injury, the performance of a single apnea test and the creation of a statement of brain death determination that includes the recording of all procedures in a single document. This document, despite the controversy surrounding it, increases the safety necessary when establishing a diagnosis of such importance and has positive implications that extend beyond the patient and the physician to reach the entire health system.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
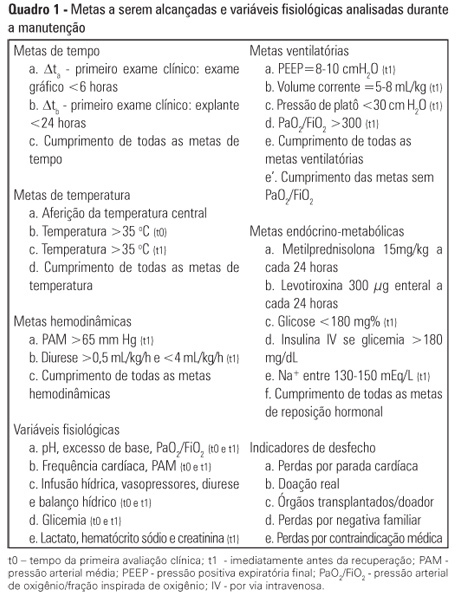
Brain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient's metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
Abstract
Rev Bras Ter Intensiva. 2011;23(4):410-425
DOI 10.1590/S0103-507X2011000400005
Brain death (BD) alters the pathophysiology of patients and may damage the kidneys, the lungs, the heart and the liver. To obtain better quality transplant organs, intensive care physicians in charge of the maintenance of deceased donors should attentively monitor these organs. Careful hemodynamic, ventilatory and bronchial clearance management minimizes the loss of kidneys and lungs. The evaluation of cardiac function and morphology supports the transplant viability assessment of the heart. The monitoring of liver function, the management of the patient's metabolic status and the evaluation of viral serology are fundamental for organ selection by the transplant teams and for the care of the transplant recipient
Abstract
Rev Bras Ter Intensiva. 2018;30(4):414-422
DOI 10.5935/0103-507X.20180059
To describe the improvements of an early warning system for the identification of septic patients on the time to diagnosis, antibiotic delivery, and mortality.
This was an observational cohort study that describes the successive improvements made over a period of 10 years using an early warning system to detect sepsis, including systematic active manual surveillance, electronic alerts via a telephonist, and alerts sent directly to the mobile devices of nurses. For all periods, after an alert was triggered, early treatment was instituted according to the institutional sepsis guidelines.
In total, 637 patients with sepsis were detected over the study period. The median triage-to-diagnosis time was reduced from 19:20 (9:10 - 38:15) hours to 12:40 (2:50 - 23:45) hours when the manual surveillance method was used (p = 0.14), to 2:10 (1:25 - 2:20) hours when the alert was sent automatically to the hospital telephone service (p = 0.014), and to 1:00 (0:30 - 1:10) hour when the alert was sent directly to the nurse's mobile phone (p = 0.016). The diagnosis-to-antibiotic time was reduced to 1:00 (0:55 - 1:30) hours when the alert was sent to the telephonist and to 0:45 (0:30 - 1:00) minutes when the alert was sent directly to the nurse's mobile phone (p = 0.02), with the maintenance of similar values over the following years. There was no difference in the time of treatment between survivors and non-survivors.
Electronic systems help reduce the triage-to-diagnosis time and diagnosis-to-antibiotic time in patients with sepsis.
Abstract
Rev Bras Ter Intensiva. 2018;30(4):414-422
DOI 10.5935/0103-507X.20180059
To describe the improvements of an early warning system for the identification of septic patients on the time to diagnosis, antibiotic delivery, and mortality.
This was an observational cohort study that describes the successive improvements made over a period of 10 years using an early warning system to detect sepsis, including systematic active manual surveillance, electronic alerts via a telephonist, and alerts sent directly to the mobile devices of nurses. For all periods, after an alert was triggered, early treatment was instituted according to the institutional sepsis guidelines.
In total, 637 patients with sepsis were detected over the study period. The median triage-to-diagnosis time was reduced from 19:20 (9:10 - 38:15) hours to 12:40 (2:50 - 23:45) hours when the manual surveillance method was used (p = 0.14), to 2:10 (1:25 - 2:20) hours when the alert was sent automatically to the hospital telephone service (p = 0.014), and to 1:00 (0:30 - 1:10) hour when the alert was sent directly to the nurse's mobile phone (p = 0.016). The diagnosis-to-antibiotic time was reduced to 1:00 (0:55 - 1:30) hours when the alert was sent to the telephonist and to 0:45 (0:30 - 1:00) minutes when the alert was sent directly to the nurse's mobile phone (p = 0.02), with the maintenance of similar values over the following years. There was no difference in the time of treatment between survivors and non-survivors.
Electronic systems help reduce the triage-to-diagnosis time and diagnosis-to-antibiotic time in patients with sepsis.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
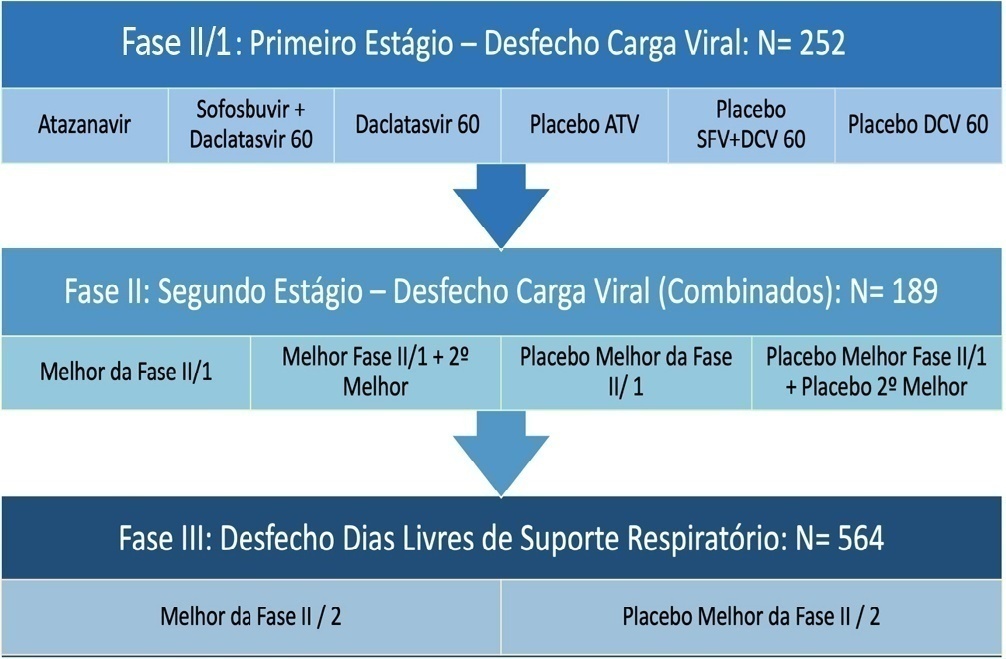
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier:
Abstract
Rev Bras Ter Intensiva. 2022;34(1):44-55
DOI 10.5935/0103-507X.20220002-en
Repurposed drugs are important in resource-limited settings because the interventions are more rapidly available, have already been tested safely in other populations and are inexpensive. Repurposed drugs are an effective solution, especially for emerging diseases such as COVID-19. The REVOLUTIOn trial has the objective of evaluating three repurposed antiviral drugs, atazanavir, daclatasvir and sofosbuvir, already used for HIV- and hepatitis C virus-infected patients in a randomized, placebo-controlled, adaptive, multiarm, multistage study. The drugs will be tested simultaneously in a Phase II trial to first identify whether any of these drugs alone or in combination reduce the viral load. If they do, a Phase III trial will be initiated to investigate if these medications are capable of increasing the number of days free respiratory support. Participants must be hospitalized adults aged ≥ 18 years with initiation of symptoms ≤ 9 days and SpO2 ≤ 94% in room air or a need for supplemental oxygen to maintain an SpO2 > 94%. The expected total sample size ranges from 252 to 1,005 participants, depending on the number of stages that will be completed in the study. Hence, the protocol is described here in detail together with the statistical analysis plan. In conclusion, the REVOLUTIOn trial is designed to provide evidence on whether atazanavir, daclatasvir or sofosbuvir decrease the SARS-CoV-2 load in patients with COVID-19 and increase the number of days patients are free of respiratory support. In this protocol paper, we describe the rationale, design, and status of the trial.
ClinicalTrials.gov identifier: