-
Commentaries
Goals of goal-directed sedation
Rev Bras Ter Intensiva. 2015;27(1):1-4
Abstract
CommentariesGoals of goal-directed sedation
Rev Bras Ter Intensiva. 2015;27(1):1-4
DOI 10.5935/0103-507X.20150001
Views1“Be stubborn about your goals and flexible about your methods” Although goal setting is traditional in motivational and behavioral sciences,() goal-directed (GD) approach is a relatively recent phenomenon that has dominated the intensive care world over the last 2 decades.() GD management, however, is not new to medicine.() The goals of blood pressure and blood […]See moreViews1

Abstract
CommentariesGoals of goal-directed sedation
Rev Bras Ter Intensiva. 2015;27(1):1-4
DOI 10.5935/0103-507X.20150001
Views1“Be stubborn about your goals and flexible about your methods” Although goal setting is traditional in motivational and behavioral sciences,() goal-directed (GD) approach is a relatively recent phenomenon that has dominated the intensive care world over the last 2 decades.() GD management, however, is not new to medicine.() The goals of blood pressure and blood […]See more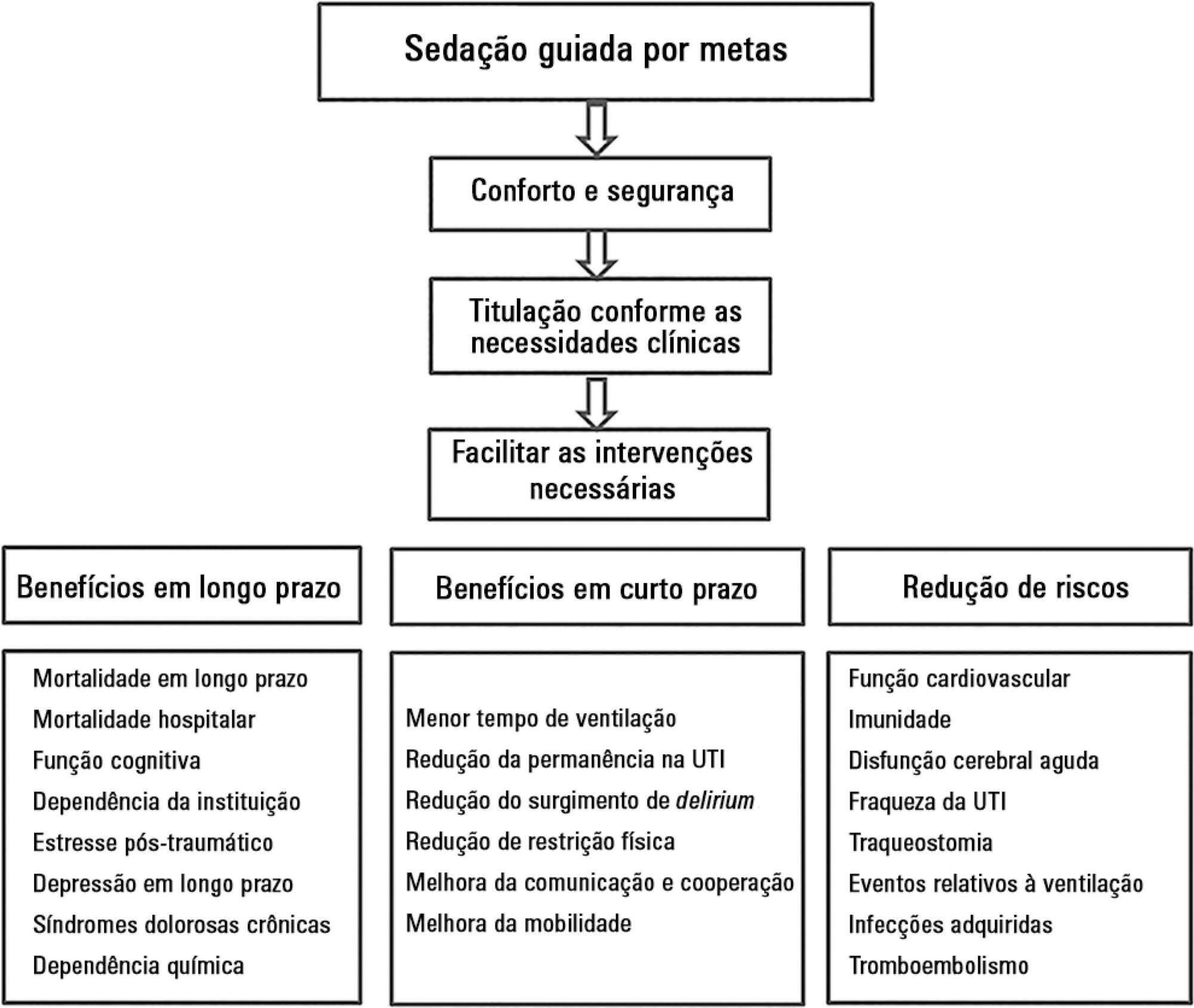
-
Commentaries
Shortage of intensive care specialists in the United States: recent insights and proposed solutions
Rev Bras Ter Intensiva. 2015;27(1):5-6
Abstract
CommentariesShortage of intensive care specialists in the United States: recent insights and proposed solutions
Rev Bras Ter Intensiva. 2015;27(1):5-6
DOI 10.5935/0103-507X.20150002
Views0Despite well-publicized projections of an impending and actual intensivist workforce crisis in the United States from critical care societies and the federal government for over a decade,(,) there continues to be a nationwide shortage of intensivists. Others, however, contend that workforce models, which base demand projections on intensive care unit (ICU) admission rather than true […]See moreViews0Abstract
CommentariesShortage of intensive care specialists in the United States: recent insights and proposed solutions
Rev Bras Ter Intensiva. 2015;27(1):5-6
DOI 10.5935/0103-507X.20150002
Views0Despite well-publicized projections of an impending and actual intensivist workforce crisis in the United States from critical care societies and the federal government for over a decade,(,) there continues to be a nationwide shortage of intensivists. Others, however, contend that workforce models, which base demand projections on intensive care unit (ICU) admission rather than true […]See more -
Commentaries
Caring for the critically ill in developing countries: a perspective from India
Rev Bras Ter Intensiva. 2015;27(1):7-9
Abstract
CommentariesCaring for the critically ill in developing countries: a perspective from India
Rev Bras Ter Intensiva. 2015;27(1):7-9
DOI 10.5935/0103-507X.20150003
Views0COSTS OF CAREHealth care facilities in India are either privately run institutions or publicly funded. Most intensive care unit (ICU) beds in India are in private hospitals. The relatively few ICU beds in public hospitals, which offer free treatment, constitute approximately 10% of the critical care facilities in India. Health insurance and social security are […]See moreViews0Abstract
CommentariesCaring for the critically ill in developing countries: a perspective from India
Rev Bras Ter Intensiva. 2015;27(1):7-9
DOI 10.5935/0103-507X.20150003
Views0COSTS OF CAREHealth care facilities in India are either privately run institutions or publicly funded. Most intensive care unit (ICU) beds in India are in private hospitals. The relatively few ICU beds in public hospitals, which offer free treatment, constitute approximately 10% of the critical care facilities in India. Health insurance and social security are […]See more -
Original Articles
What happens to the fluid balance during and after recovering from septic shock?
Rev Bras Ter Intensiva. 2015;27(1):10-17
Abstract
Original ArticlesWhat happens to the fluid balance during and after recovering from septic shock?
Rev Bras Ter Intensiva. 2015;27(1):10-17
DOI 10.5935/0103-507X.20150004
Views0See moreObjective:
We aimed to evaluate the cumulative fluid balance during the period of shock and determine what happens to fluid balance in the 7 days following recovery from shock.
Methods:
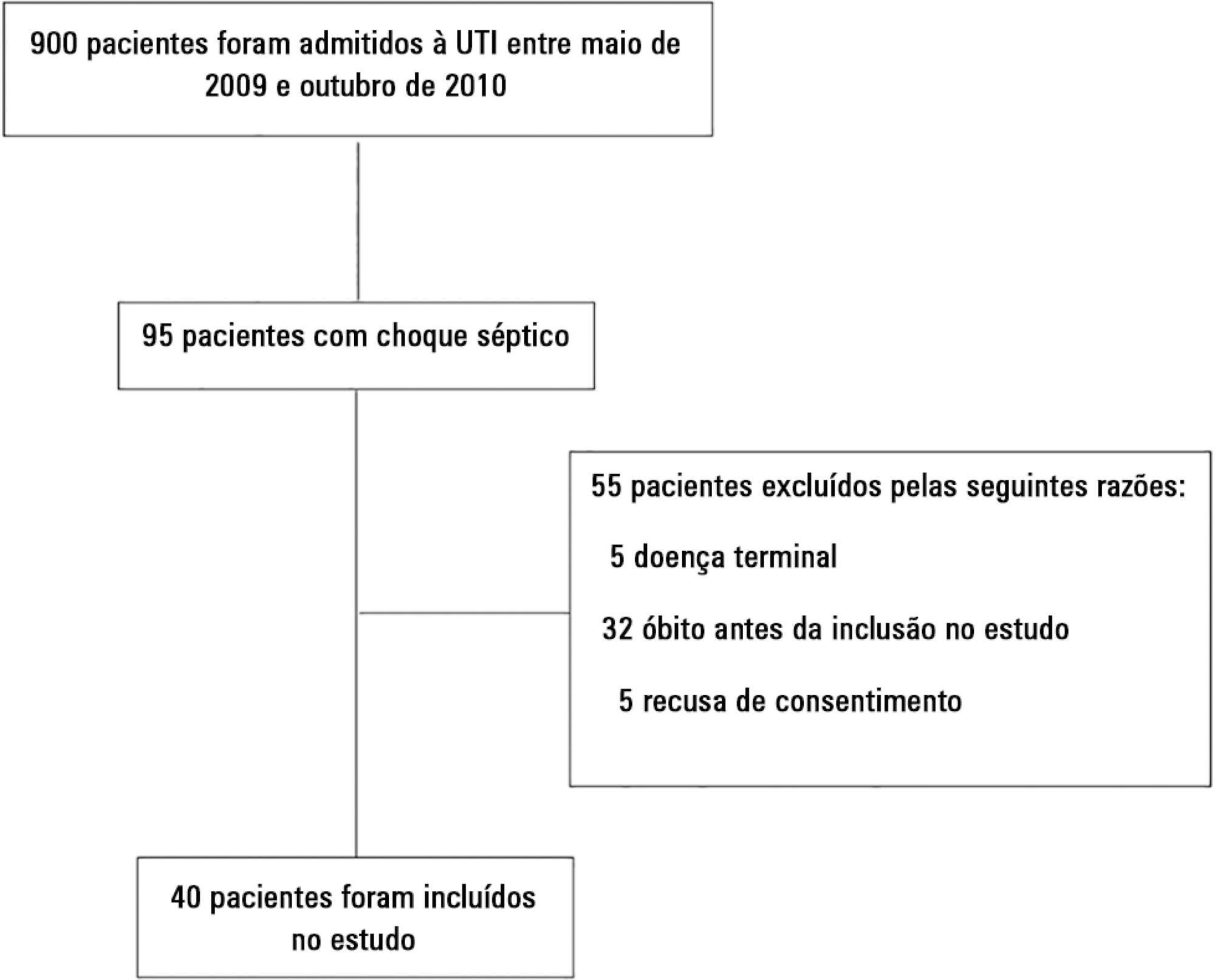
A prospective and observational study in septic shock patients. Patients with a mean arterial pressure ≥ 65mmHg and lactate < 2.0mEq/L were included < 12 hours after weaning from vasopressor, and this day was considered day 1. The daily fluid balance was registered during and for seven days after recovery from shock. Patients were divided into two groups according to the full cohort’s median cumulative fluid balance during the period of shock: Group 1 ≤ 4.4L (n = 20) and Group 2 > 4.4L (n = 20).
Results:
We enrolled 40 patients in the study. On study day 1, the cumulative fluid balance was 1.1 [0.6 – 3.4] L in Group 1 and 9.0 [6.7 – 13.8] L in Group 2. On study day 7, the cumulative fluid balance was 8.0 [4.5 – 12.4] L in Group 1 and 14.7 [12.7 – 20.6] L in Group 2 (p < 0.001 for both). Afterwards, recovery of shock fluid balance continued to increase in both groups. Group 2 had a more prolonged length of stay in the intensive care unit and hospital compared to Group 1.
Conclusion:
In conclusion, positive fluid balances are frequently seen in patients with septic shock and may be related to worse outcomes. During the shock period, even though the fluid balance was previously positive, it becomes more positive. After recovery from shock, the fluid balance continues to increase. The group with a more positive fluid balance group spent more time in the intensive care unit and hospital.
Views0Abstract
Original ArticlesWhat happens to the fluid balance during and after recovering from septic shock?
Rev Bras Ter Intensiva. 2015;27(1):10-17
DOI 10.5935/0103-507X.20150004
Views0See moreObjective:
We aimed to evaluate the cumulative fluid balance during the period of shock and determine what happens to fluid balance in the 7 days following recovery from shock.
Methods:
A prospective and observational study in septic shock patients. Patients with a mean arterial pressure ≥ 65mmHg and lactate < 2.0mEq/L were included < 12 hours after weaning from vasopressor, and this day was considered day 1. The daily fluid balance was registered during and for seven days after recovery from shock. Patients were divided into two groups according to the full cohort’s median cumulative fluid balance during the period of shock: Group 1 ≤ 4.4L (n = 20) and Group 2 > 4.4L (n = 20).
Results:
We enrolled 40 patients in the study. On study day 1, the cumulative fluid balance was 1.1 [0.6 – 3.4] L in Group 1 and 9.0 [6.7 – 13.8] L in Group 2. On study day 7, the cumulative fluid balance was 8.0 [4.5 – 12.4] L in Group 1 and 14.7 [12.7 – 20.6] L in Group 2 (p < 0.001 for both). Afterwards, recovery of shock fluid balance continued to increase in both groups. Group 2 had a more prolonged length of stay in the intensive care unit and hospital compared to Group 1.
Conclusion:
In conclusion, positive fluid balances are frequently seen in patients with septic shock and may be related to worse outcomes. During the shock period, even though the fluid balance was previously positive, it becomes more positive. After recovery from shock, the fluid balance continues to increase. The group with a more positive fluid balance group spent more time in the intensive care unit and hospital.
-
Original Articles
Patient stress in intensive care: comparison between a coronary care unit and a general postoperative unit
Rev Bras Ter Intensiva. 2015;27(1):18-25
Abstract
Original ArticlesPatient stress in intensive care: comparison between a coronary care unit and a general postoperative unit
Rev Bras Ter Intensiva. 2015;27(1):18-25
DOI 10.5935/0103-507X.20150005
Views0Objective:
To evaluate and compare stressors identified by patients of a coronary intensive care unit with those perceived by patients of a general postoperative intensive care unit.
Methods:
This cross-sectional and descriptive study was conducted in the coronary intensive care and general postoperative intensive care units of a private hospital. In total, 60 patients participated in the study, 30 in each intensive care unit. The stressor scale was used in the intensive care units to identify the stressors. The mean score of each item of the scale was calculated followed by the total stress score. The differences between groups were considered significant when p < 0.05.
Results:
The mean ages of patients were 55.63 ± 13.58 years in the coronary intensive care unit and 53.60 ± 17.47 years in the general postoperative intensive care unit. For patients in the coronary intensive care unit, the main stressors were “being in pain”, “being unable to fulfill family roles” and “being bored”. For patients in the general postoperative intensive care unit, the main stressors were “being in pain”, “being unable to fulfill family roles” and “not being able to communicate”. The mean total stress scores were 104.20 ± 30.95 in the coronary intensive care unit and 116.66 ± 23.72 (p = 0.085) in the general postoperative intensive care unit. When each stressor was compared separately, significant differences were noted only between three items. “Having nurses constantly doing things around your bed” was more stressful to the patients in the general postoperative intensive care unit than to those in the coronary intensive care unit (p = 0.013). Conversely, “hearing unfamiliar sounds and noises” and “hearing people talk about you” were the most stressful items for the patients in the coronary intensive care unit (p = 0.046 and 0.005, respectively).
Conclusion:
The perception of major stressors and the total stress score were similar between patients in the coronary intensive care and general postoperative intensive care units.
Keywords:Coronary care unitsCritical careHumanization of assistanceIntensive care unitsPostoperative periodstressSee moreViews0Abstract
Original ArticlesPatient stress in intensive care: comparison between a coronary care unit and a general postoperative unit
Rev Bras Ter Intensiva. 2015;27(1):18-25
DOI 10.5935/0103-507X.20150005
Views0Objective:
To evaluate and compare stressors identified by patients of a coronary intensive care unit with those perceived by patients of a general postoperative intensive care unit.
Methods:
This cross-sectional and descriptive study was conducted in the coronary intensive care and general postoperative intensive care units of a private hospital. In total, 60 patients participated in the study, 30 in each intensive care unit. The stressor scale was used in the intensive care units to identify the stressors. The mean score of each item of the scale was calculated followed by the total stress score. The differences between groups were considered significant when p < 0.05.
Results:
The mean ages of patients were 55.63 ± 13.58 years in the coronary intensive care unit and 53.60 ± 17.47 years in the general postoperative intensive care unit. For patients in the coronary intensive care unit, the main stressors were “being in pain”, “being unable to fulfill family roles” and “being bored”. For patients in the general postoperative intensive care unit, the main stressors were “being in pain”, “being unable to fulfill family roles” and “not being able to communicate”. The mean total stress scores were 104.20 ± 30.95 in the coronary intensive care unit and 116.66 ± 23.72 (p = 0.085) in the general postoperative intensive care unit. When each stressor was compared separately, significant differences were noted only between three items. “Having nurses constantly doing things around your bed” was more stressful to the patients in the general postoperative intensive care unit than to those in the coronary intensive care unit (p = 0.013). Conversely, “hearing unfamiliar sounds and noises” and “hearing people talk about you” were the most stressful items for the patients in the coronary intensive care unit (p = 0.046 and 0.005, respectively).
Conclusion:
The perception of major stressors and the total stress score were similar between patients in the coronary intensive care and general postoperative intensive care units.
Keywords:Coronary care unitsCritical careHumanization of assistanceIntensive care unitsPostoperative periodstressSee more -
Original Articles
The reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(1):26-35
Abstract
Original ArticlesThe reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
Views7See moreObjective:
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
Methods:
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
Results:
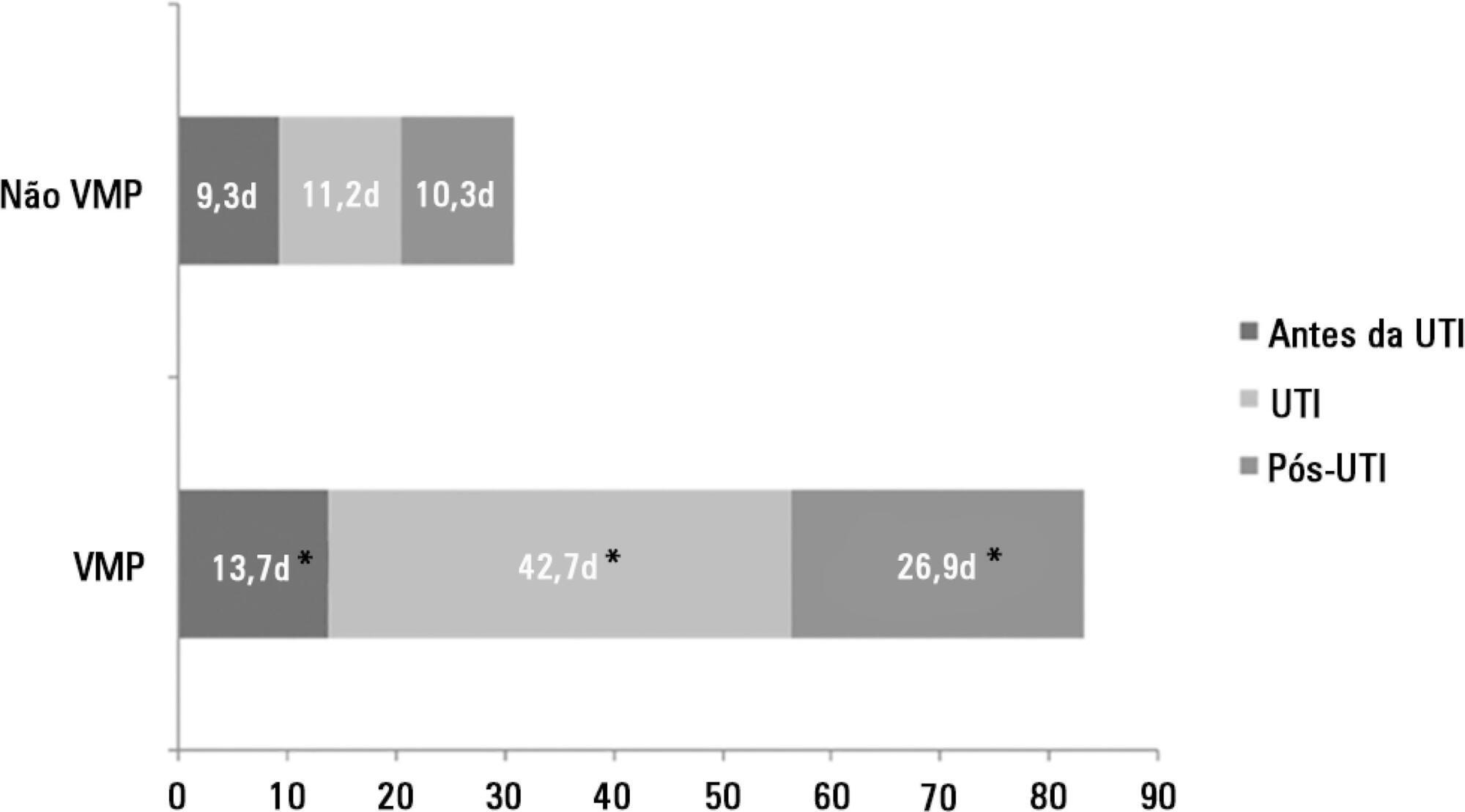
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
Conclusion:
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
Views7Abstract
Original ArticlesThe reality of patients requiring prolonged mechanical ventilation: a multicenter study
Rev Bras Ter Intensiva. 2015;27(1):26-35
DOI 10.5935/0103-507X.20150006
Views7See moreObjective:
The number of patients who require prolonged mechanical ventilation increased during the last decade, which generated a large population of chronically ill patients. This study established the incidence of prolonged mechanical ventilation in four intensive care units and reported different characteristics, hospital outcomes, and the impact of costs and services of prolonged mechanical ventilation patients (mechanical ventilation dependency ≥ 21 days) compared with non-prolonged mechanical ventilation patients (mechanical ventilation dependency < 21 days).
Methods:
This study was a multicenter cohort study of all patients who were admitted to four intensive care units. The main outcome measures were length of stay in the intensive care unit, hospital, complications during intensive care unit stay, and intensive care unit and hospital mortality.
Results:
There were 5,287 admissions to the intensive care units during study period. Some of these patients (41.5%) needed ventilatory support (n = 2,197), and 218 of the patients met criteria for prolonged mechanical ventilation (9.9%). Some complications developed during intensive care unit stay, such as muscle weakness, pressure ulcers, bacterial nosocomial sepsis, candidemia, pulmonary embolism, and hyperactive delirium, were associated with a significantly higher risk of prolonged mechanical ventilation. Prolonged mechanical ventilation patients had a significant increase in intensive care unit mortality (absolute difference = 14.2%, p < 0.001) and hospital mortality (absolute difference = 19.1%, p < 0.001). The prolonged mechanical ventilation group spent more days in the hospital after intensive care unit discharge (26.9 ± 29.3 versus 10.3 ± 20.4 days, p < 0.001) with higher costs.
Conclusion:
The classification of chronically critically ill patients according to the definition of prolonged mechanical ventilation adopted by our study (mechanical ventilation dependency ≥ 21 days) identified patients with a high risk for complications during intensive care unit stay, longer intensive care unit and hospital stays, high death rates, and higher costs.
-
Original Articles
Blood transfusions in septic shock: is 7.0g/dL really the appropriate threshold?
Rev Bras Ter Intensiva. 2015;27(1):36-43
Abstract
Original ArticlesBlood transfusions in septic shock: is 7.0g/dL really the appropriate threshold?
Rev Bras Ter Intensiva. 2015;27(1):36-43
DOI 10.5935/0103-507X.20150007
Views0See moreObjective:
To evaluate the immediate effects of red blood cell transfusion on central venous oxygen saturation and lactate levels in septic shock patients with different transfusion triggers.
Methods:
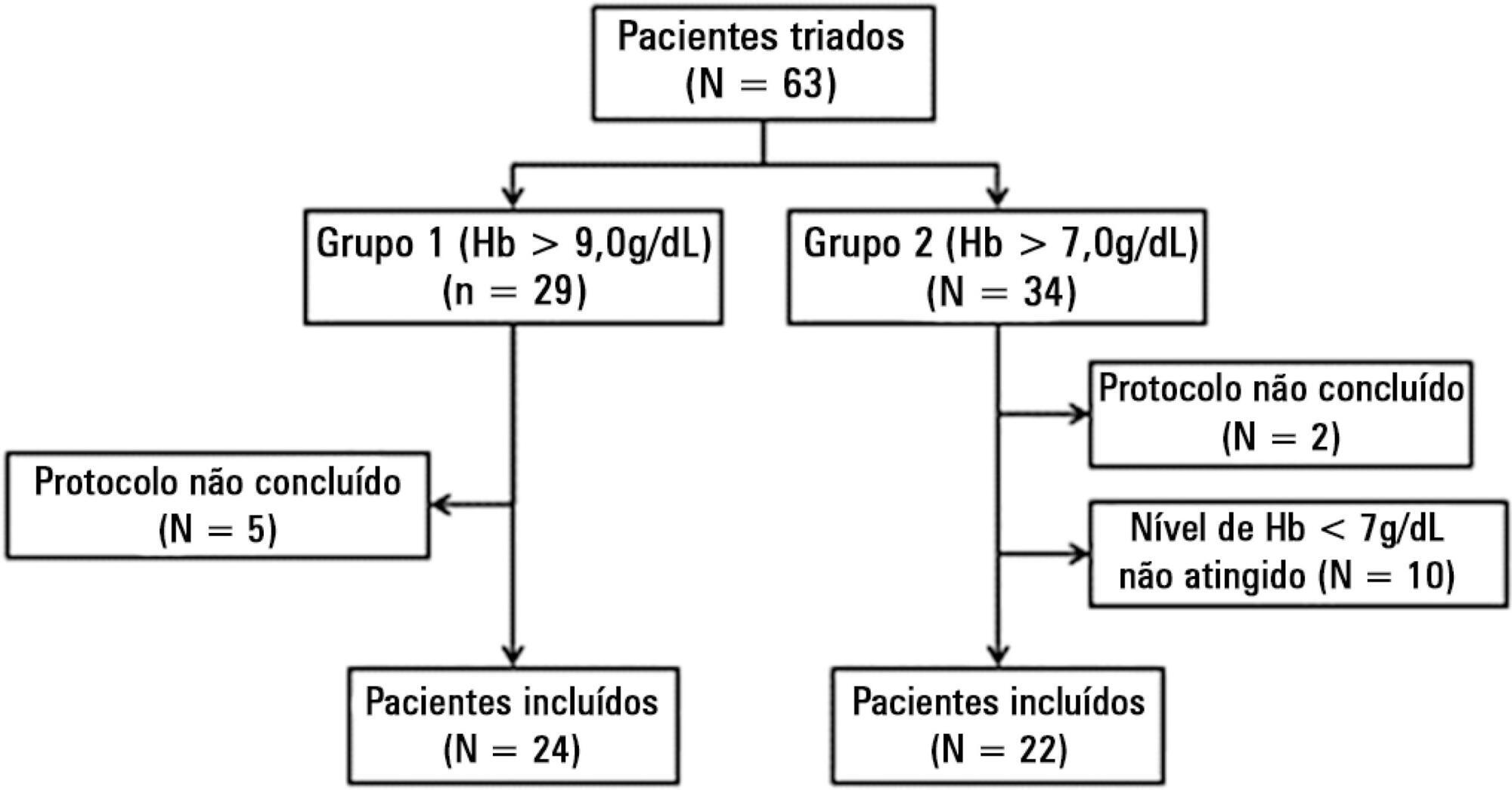
We included patients with a diagnosis of septic shock within the last 48 hours and hemoglobin levels below 9.0g/dL Patients were randomized for immediate transfusion with hemoglobin concentrations maintained above 9.0g/dL (Group Hb9) or to withhold transfusion unless hemoglobin felt bellow 7.0g/dL (Group Hb7). Hemoglobin, lactate, central venous oxygen saturation levels were determined before and one hour after each transfusion.
Results:
We included 46 patients and 74 transfusions. Patients in Group Hb7 had a significant reduction in median lactate from 2.44 (2.00 – 3.22) mMol/L to 2.21 (1.80 – 2.79) mMol/L, p = 0.005, which was not observed in Group Hb9 [1.90 (1.80 – 2.65) mMol/L to 2.00 (1.70 – 2.41) mMol/L, p = 0.23]. Central venous oxygen saturation levels increased in Group Hb7 [68.0 (64.0 – 72.0)% to 72.0 (69.0 – 75.0)%, p < 0.0001] but not in Group Hb9 [72.0 (69.0 - 74.0)% to 72.0 (71.0 - 73.0)%, p = 0.98]. Patients with elevated lactate or central venous oxygen saturation < 70% at baseline had a significant increase in these variables, regardless of baseline hemoglobin levels. Patients with normal values did not show a decrease in either group.
Conclusion:
Red blood cell transfusion increased central venous oxygen saturation and decreased lactate levels in patients with hypoperfusion regardless of their baseline hemoglobin levels. Transfusion did not appear to impair these variables in patients without hypoperfusion.
Views0Abstract
Original ArticlesBlood transfusions in septic shock: is 7.0g/dL really the appropriate threshold?
Rev Bras Ter Intensiva. 2015;27(1):36-43
DOI 10.5935/0103-507X.20150007
Views0See moreObjective:
To evaluate the immediate effects of red blood cell transfusion on central venous oxygen saturation and lactate levels in septic shock patients with different transfusion triggers.
Methods:
We included patients with a diagnosis of septic shock within the last 48 hours and hemoglobin levels below 9.0g/dL Patients were randomized for immediate transfusion with hemoglobin concentrations maintained above 9.0g/dL (Group Hb9) or to withhold transfusion unless hemoglobin felt bellow 7.0g/dL (Group Hb7). Hemoglobin, lactate, central venous oxygen saturation levels were determined before and one hour after each transfusion.
Results:
We included 46 patients and 74 transfusions. Patients in Group Hb7 had a significant reduction in median lactate from 2.44 (2.00 – 3.22) mMol/L to 2.21 (1.80 – 2.79) mMol/L, p = 0.005, which was not observed in Group Hb9 [1.90 (1.80 – 2.65) mMol/L to 2.00 (1.70 – 2.41) mMol/L, p = 0.23]. Central venous oxygen saturation levels increased in Group Hb7 [68.0 (64.0 – 72.0)% to 72.0 (69.0 – 75.0)%, p < 0.0001] but not in Group Hb9 [72.0 (69.0 - 74.0)% to 72.0 (71.0 - 73.0)%, p = 0.98]. Patients with elevated lactate or central venous oxygen saturation < 70% at baseline had a significant increase in these variables, regardless of baseline hemoglobin levels. Patients with normal values did not show a decrease in either group.
Conclusion:
Red blood cell transfusion increased central venous oxygen saturation and decreased lactate levels in patients with hypoperfusion regardless of their baseline hemoglobin levels. Transfusion did not appear to impair these variables in patients without hypoperfusion.
-
Original Articles
Causes of non-adherence to therapeutic guidelines in severe community-acquired pneumonia
Rev Bras Ter Intensiva. 2015;27(1):44-50
Abstract
Original ArticlesCauses of non-adherence to therapeutic guidelines in severe community-acquired pneumonia
Rev Bras Ter Intensiva. 2015;27(1):44-50
DOI 10.5935/0103-507X.20150008
Views0Objective:
To assess the adherence to Infectious Disease Society of America/American Thoracic Society guidelines and the causes of lack of adherence during empirical antibiotic prescription in severe pneumonia in Latin America.
Methods:
A clinical questionnaire was submitted to 36 physicians from Latin America; they were asked to indicate the empirical treatment in two fictitious cases of severe respiratory infection: community-acquired pneumonia and nosocomial pneumonia.
Results:
In the case of communityacquired pneumonia, 11 prescriptions of 36 (30.6%) were compliant with international guidelines. The causes for non-compliant treatment were monotherapy (16.0%), the unnecessary prescription of broad-spectrum antibiotics (40.0%) and the use of non-recommended antibiotics (44.0%).
Conclusion:
The compliance rate with the Infectious Disease Society of America/American Thoracic Society guidelines in the community-acquired pneumonia scenario was 30.6%; the most frequent cause of lack of compliance was the indication of monotherapy. In the case of nosocomial pneumonia, the compliance rate with the guidelines was 2.8%, and the most important cause of non-adherence was lack of combined antipseudomonal therapy. If the use of monotherapy with an antipseudomonal antibiotic was considered the correct option, the treatment would be adequate in 100% of the prescriptions.
Keywords:Advance directive adherenceAnti-bacterial agents/therapeutic useCommunity-acquired pneumonia/drug therapyPneumonia ventilator-associated/drug therapySee moreViews0Abstract
Original ArticlesCauses of non-adherence to therapeutic guidelines in severe community-acquired pneumonia
Rev Bras Ter Intensiva. 2015;27(1):44-50
DOI 10.5935/0103-507X.20150008
Views0Objective:
To assess the adherence to Infectious Disease Society of America/American Thoracic Society guidelines and the causes of lack of adherence during empirical antibiotic prescription in severe pneumonia in Latin America.
Methods:
A clinical questionnaire was submitted to 36 physicians from Latin America; they were asked to indicate the empirical treatment in two fictitious cases of severe respiratory infection: community-acquired pneumonia and nosocomial pneumonia.
Results:
In the case of communityacquired pneumonia, 11 prescriptions of 36 (30.6%) were compliant with international guidelines. The causes for non-compliant treatment were monotherapy (16.0%), the unnecessary prescription of broad-spectrum antibiotics (40.0%) and the use of non-recommended antibiotics (44.0%).
Conclusion:
The compliance rate with the Infectious Disease Society of America/American Thoracic Society guidelines in the community-acquired pneumonia scenario was 30.6%; the most frequent cause of lack of compliance was the indication of monotherapy. In the case of nosocomial pneumonia, the compliance rate with the guidelines was 2.8%, and the most important cause of non-adherence was lack of combined antipseudomonal therapy. If the use of monotherapy with an antipseudomonal antibiotic was considered the correct option, the treatment would be adequate in 100% of the prescriptions.
Keywords:Advance directive adherenceAnti-bacterial agents/therapeutic useCommunity-acquired pneumonia/drug therapyPneumonia ventilator-associated/drug therapySee more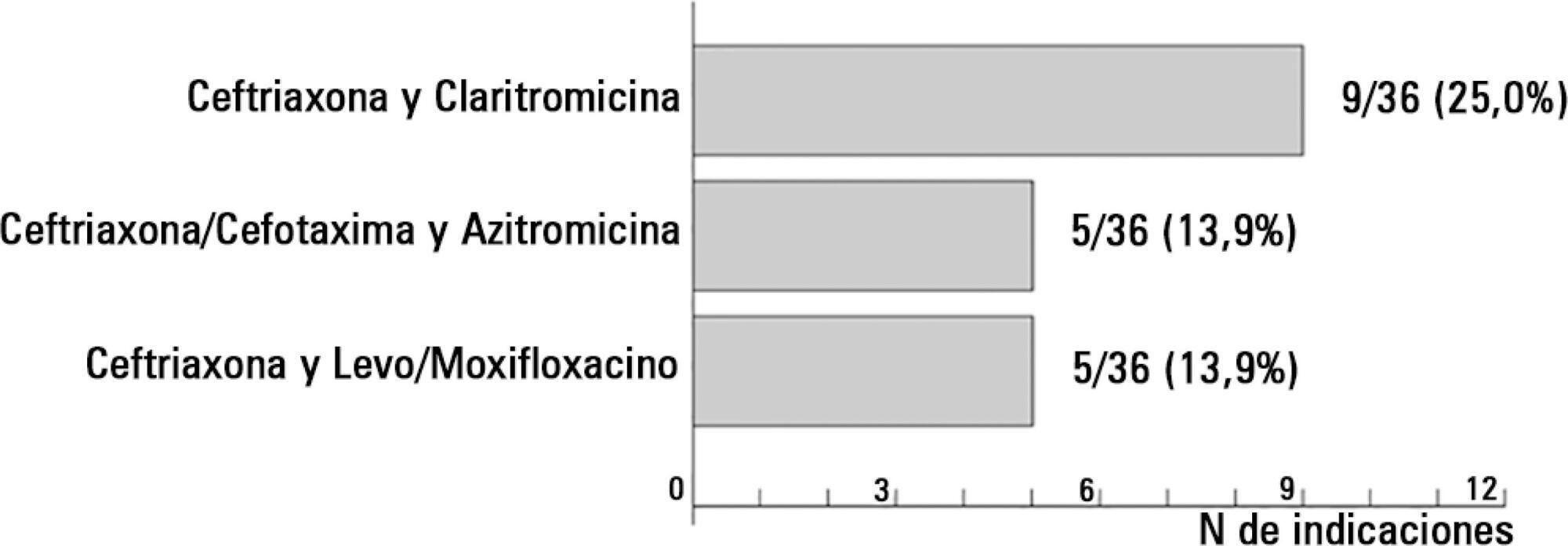
-
Original Articles
Septic shock: a major cause of hospital death after intensive care unit discharge
Rev Bras Ter Intensiva. 2015;27(1):51-56
Abstract
Original ArticlesSeptic shock: a major cause of hospital death after intensive care unit discharge
Rev Bras Ter Intensiva. 2015;27(1):51-56
DOI 10.5935/0103-507X.20150009
Views0See moreObjective:
To assess the causes and factors associated with the death of patients between intensive care unit discharge and hospital discharge.
Methods:
The present is a pilot, retrospective, observational cohort study. The records of all patients admitted to two units of a public/private university hospital from February 1, 2013 to April 30, 2013 were assessed. Demographic and clinical data, risk scores and outcomes were obtained from the Epimed monitoring system and confirmed in the electronic record system of the hospital. The relative risk and respective confidence intervals were calculated.
Results:
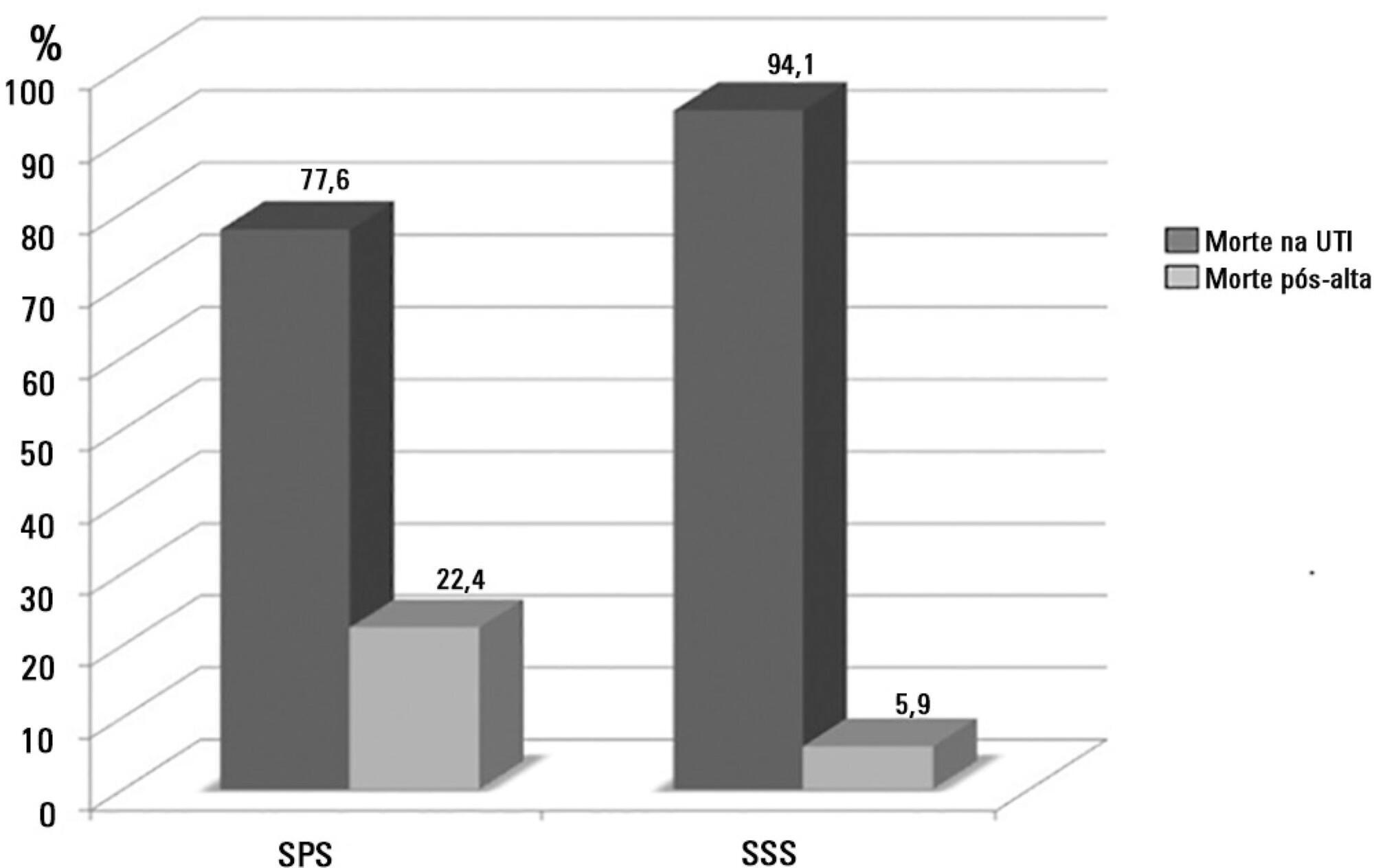
A total of 581 patients were evaluated. The mortality rate in the intensive care unit was 20.8% and in the hospital was 24.9%. Septic shock was the cause of death in 58.3% of patients who died after being discharged from the intensive care unit. Of the patients from the public health system, 73 (77.6%) died in the intensive care unit and 21 (22.4%) died in the hospital after being discharged from the unit. Of the patients from the Supplementary Health System, 48 (94.1%) died in the intensive care unit and 3 (5.9%) died in the hospital after being discharged from the unit (relative risk, 3.87%; 95% confidence interval, 1.21 – 12.36; p < 0.05). The post-discharge mortality rate was significantly higher in patients with intensive care unit hospitalization time longer than 6 days.
Conclusion:
The main cause of death of patients who were discharged from the intensive care unit and died in the ward before hospital discharge was septic shock. Coverage by the public healthcare system and longer hospitalization time in the intensive care unit were factors associated with death after discharge from the intensive care unit.
Views0Abstract
Original ArticlesSeptic shock: a major cause of hospital death after intensive care unit discharge
Rev Bras Ter Intensiva. 2015;27(1):51-56
DOI 10.5935/0103-507X.20150009
Views0See moreObjective:
To assess the causes and factors associated with the death of patients between intensive care unit discharge and hospital discharge.
Methods:
The present is a pilot, retrospective, observational cohort study. The records of all patients admitted to two units of a public/private university hospital from February 1, 2013 to April 30, 2013 were assessed. Demographic and clinical data, risk scores and outcomes were obtained from the Epimed monitoring system and confirmed in the electronic record system of the hospital. The relative risk and respective confidence intervals were calculated.
Results:
A total of 581 patients were evaluated. The mortality rate in the intensive care unit was 20.8% and in the hospital was 24.9%. Septic shock was the cause of death in 58.3% of patients who died after being discharged from the intensive care unit. Of the patients from the public health system, 73 (77.6%) died in the intensive care unit and 21 (22.4%) died in the hospital after being discharged from the unit. Of the patients from the Supplementary Health System, 48 (94.1%) died in the intensive care unit and 3 (5.9%) died in the hospital after being discharged from the unit (relative risk, 3.87%; 95% confidence interval, 1.21 – 12.36; p < 0.05). The post-discharge mortality rate was significantly higher in patients with intensive care unit hospitalization time longer than 6 days.
Conclusion:
The main cause of death of patients who were discharged from the intensive care unit and died in the ward before hospital discharge was septic shock. Coverage by the public healthcare system and longer hospitalization time in the intensive care unit were factors associated with death after discharge from the intensive care unit.
-
Original Articles
Management of severe community-acquired pneumonia in Brazil: a secondary analysis of an international survey
Rev Bras Ter Intensiva. 2015;27(1):57-63
Abstract
Original ArticlesManagement of severe community-acquired pneumonia in Brazil: a secondary analysis of an international survey
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
Views0Objective:
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
Methods:
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
Results:
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
Conclusion:
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Keywords:Antimicrobial agentsBrazilCommunity-acquired infectionsDiagnosisIntensive care unitsQuestionnairesRisk assessmentSepsisSee moreViews0Abstract
Original ArticlesManagement of severe community-acquired pneumonia in Brazil: a secondary analysis of an international survey
Rev Bras Ter Intensiva. 2015;27(1):57-63
DOI 10.5935/0103-507X.20150010
Views0Objective:
This study aimed to evaluate Brazilian physicians’ perceptions regarding the diagnosis, severity assessment, treatment and risk stratification of severe community-acquired pneumonia patients and to compare those perceptions to current guidelines.
Methods:
We conducted a cross-sectional international anonymous survey among a convenience sample of critical care, pulmonary, emergency and internal medicine physicians from Brazil between October and December 2008. The electronic survey evaluated physicians’ attitudes towards the diagnosis, risk assessment and therapeutic interventions for patients with severe community-acquired pneumonia.
Results:
A total of 253 physicians responded to the survey, with 66% from Southeast Brazil. The majority (60%) of the responding physicians had > 10 years of medical experience. The risk assessment of severe community-acquired pneumonia was very heterogeneous, with clinical evaluation as the most frequent approach. Although blood cultures were recognized as exhibiting a poor diagnostic performance, these cultures were performed by 75% of respondents. In contrast, the presence of urinary pneumococcal and Legionella antigens was evaluated by less than 1/3 of physicians. The vast majority of physicians (95%) prescribe antibiotics according to a guideline, with the combination of a 3rd/4th generation cephalosporin plus a macrolide as the most frequent choice.
Conclusion:
This Brazilian survey identified an important gap between guidelines and clinical practice and recommends the institution of educational programs that implement evidence-based strategies for the management of severe community-acquired pneumonia.
Keywords:Antimicrobial agentsBrazilCommunity-acquired infectionsDiagnosisIntensive care unitsQuestionnairesRisk assessmentSepsisSee more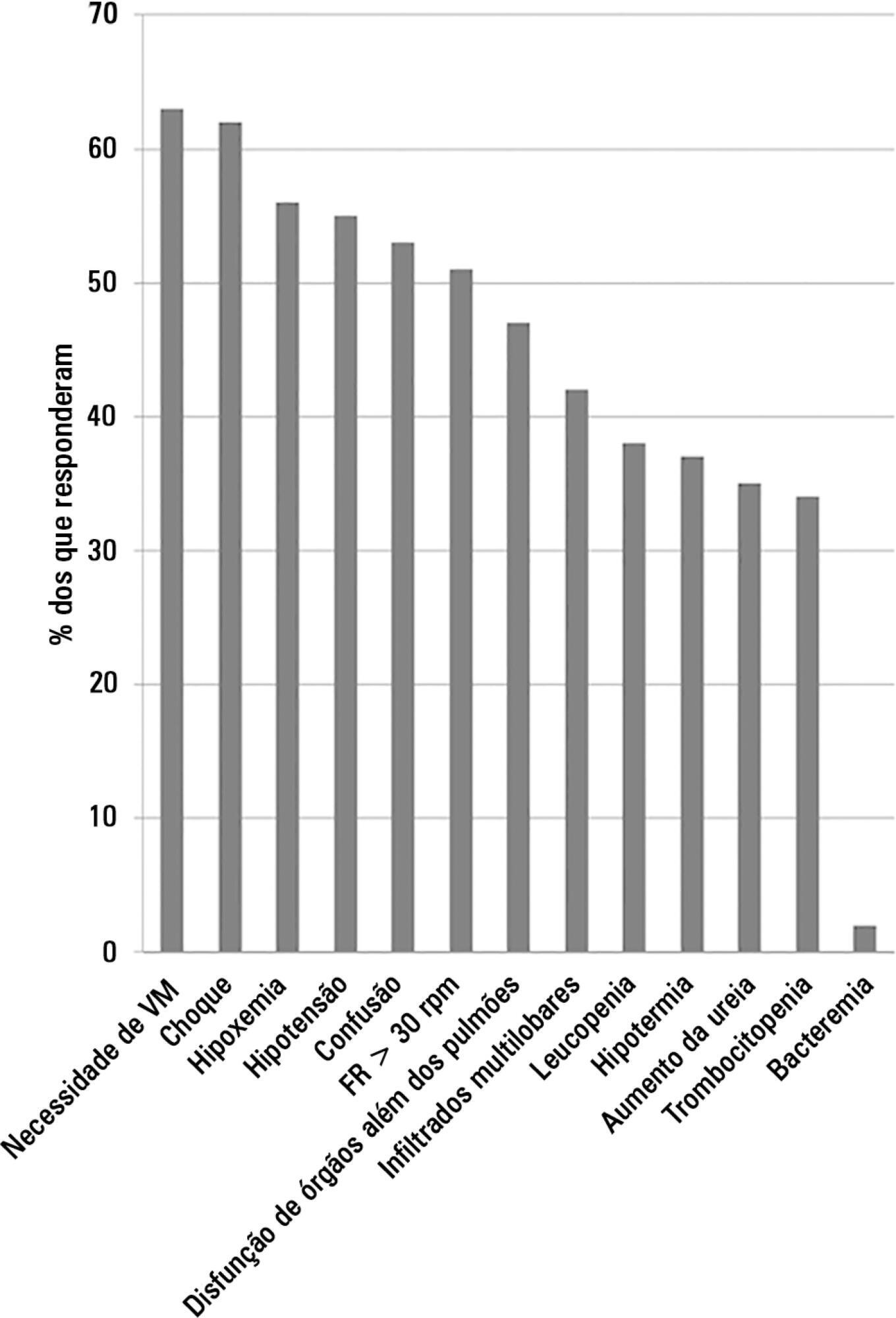
-
Original Articles
Swallowing rehabilitation of dysphagic tracheostomized patients under mechanical ventilation in intensive care units: a feasibility study
Rev Bras Ter Intensiva. 2015;27(1):64-71
Abstract
Original ArticlesSwallowing rehabilitation of dysphagic tracheostomized patients under mechanical ventilation in intensive care units: a feasibility study
Rev Bras Ter Intensiva. 2015;27(1):64-71
DOI 10.5935/0103-507X.20150011
Views0Objective:
The aim of the present study was to assess the feasibility of the early implementation of a swallowing rehabilitation program in tracheostomized patients under mechanical ventilation with dysphagia.
Methods:
This prospective study was conducted in the intensive care units of a university hospital. We included hemodynamically stable patients under mechanical ventilation for at least 48 hours following 48 hours of tracheostomy and with an appropriate level of consciousness. The exclusion criteria were previous surgery in the oral cavity, pharynx, larynx and/or esophagus, the presence of degenerative diseases or a past history of oropharyngeal dysphagia. All patients were submitted to a swallowing rehabilitation program. An oropharyngeal structural score, a swallowing functional score and an otorhinolaryngological structural and functional score were determined before and after swallowing therapy.
Results:
We included 14 patients. The mean duration of the rehabilitation program was 12.4 ± 9.4 days, with 5.0 ± 5.2 days under mechanical ventilation. Eleven patients could receive oral feeding while still in the intensive care unit after 4 (2 – 13) days of therapy. All scores significantly improved after therapy.
Conclusion:
In this small group of patients, we demonstrated that the early implementation of a swallowing rehabilitation program is feasible even in patients under mechanical ventilation.
Keywords:Deglutition disorders/rehabilitationDysphagiaIntensive care unitsRespiration, artificialtracheostomySee moreViews0Abstract
Original ArticlesSwallowing rehabilitation of dysphagic tracheostomized patients under mechanical ventilation in intensive care units: a feasibility study
Rev Bras Ter Intensiva. 2015;27(1):64-71
DOI 10.5935/0103-507X.20150011
Views0Objective:
The aim of the present study was to assess the feasibility of the early implementation of a swallowing rehabilitation program in tracheostomized patients under mechanical ventilation with dysphagia.
Methods:
This prospective study was conducted in the intensive care units of a university hospital. We included hemodynamically stable patients under mechanical ventilation for at least 48 hours following 48 hours of tracheostomy and with an appropriate level of consciousness. The exclusion criteria were previous surgery in the oral cavity, pharynx, larynx and/or esophagus, the presence of degenerative diseases or a past history of oropharyngeal dysphagia. All patients were submitted to a swallowing rehabilitation program. An oropharyngeal structural score, a swallowing functional score and an otorhinolaryngological structural and functional score were determined before and after swallowing therapy.
Results:
We included 14 patients. The mean duration of the rehabilitation program was 12.4 ± 9.4 days, with 5.0 ± 5.2 days under mechanical ventilation. Eleven patients could receive oral feeding while still in the intensive care unit after 4 (2 – 13) days of therapy. All scores significantly improved after therapy.
Conclusion:
In this small group of patients, we demonstrated that the early implementation of a swallowing rehabilitation program is feasible even in patients under mechanical ventilation.
Keywords:Deglutition disorders/rehabilitationDysphagiaIntensive care unitsRespiration, artificialtracheostomySee more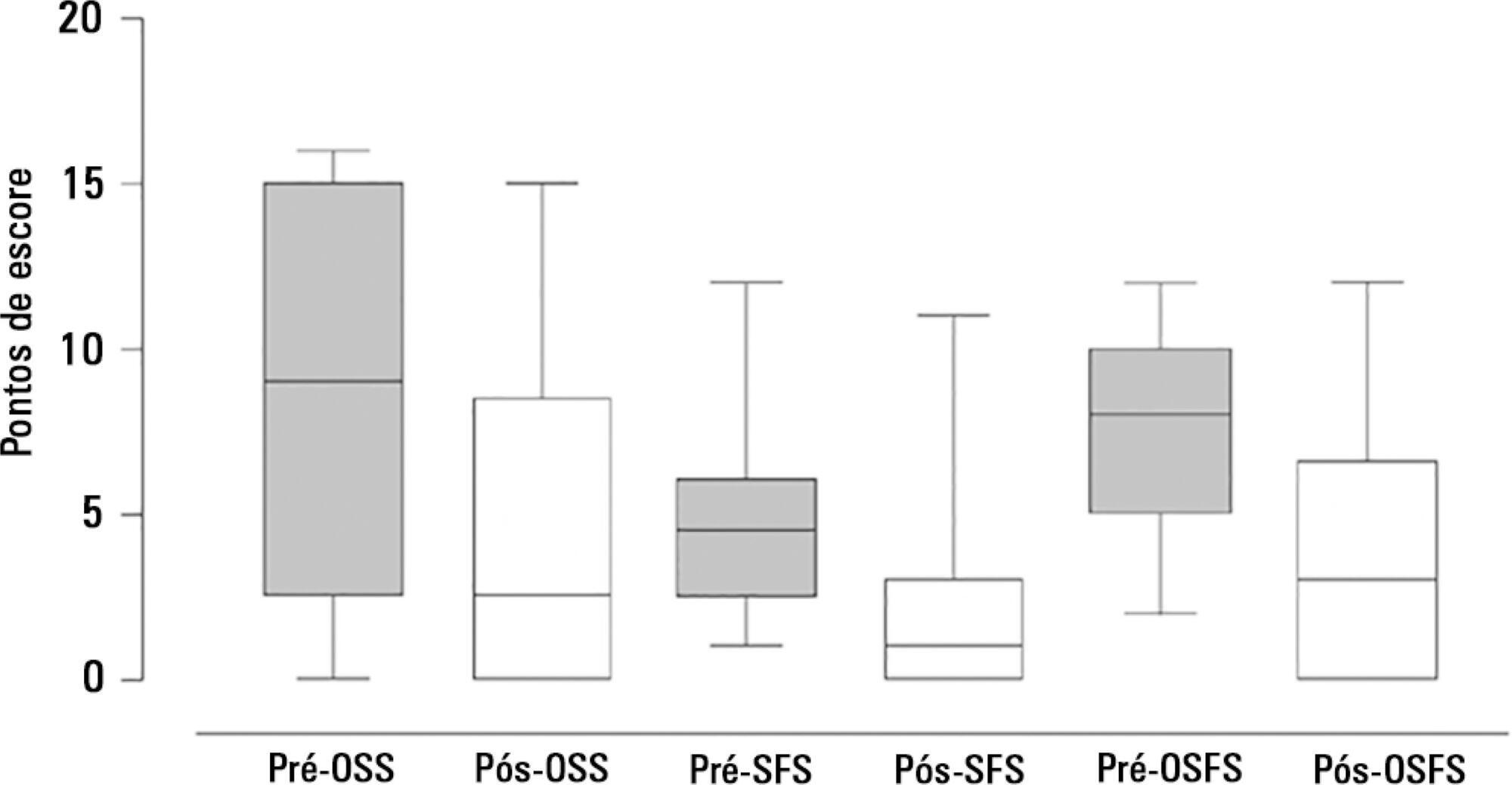
-
Review Article
Therapeutic hypothermia as a bridge to transplantation in patients with fulminant hepatic failure
Rev Bras Ter Intensiva. 2015;27(1):72-76
Abstract
Review ArticleTherapeutic hypothermia as a bridge to transplantation in patients with fulminant hepatic failure
Rev Bras Ter Intensiva. 2015;27(1):72-76
DOI 10.5935/0103-507X.20150012
Views0See moreThe most important topics in fulminant hepatic failure are cerebral edema and intracranial hypertension. Among all therapeutic options, systemic induced hypothermia to 33 – 34ºC has been reported to reduce the high pressure and increase the time during which patients can tolerate a graft. This review discusses the indications and adverse effects of hypothermia.
Views0Abstract
Review ArticleTherapeutic hypothermia as a bridge to transplantation in patients with fulminant hepatic failure
Rev Bras Ter Intensiva. 2015;27(1):72-76
DOI 10.5935/0103-507X.20150012
Views0See moreThe most important topics in fulminant hepatic failure are cerebral edema and intracranial hypertension. Among all therapeutic options, systemic induced hypothermia to 33 – 34ºC has been reported to reduce the high pressure and increase the time during which patients can tolerate a graft. This review discusses the indications and adverse effects of hypothermia.
-
Case Report
Recurrent rhabdomyolysis secondary to hyponatremia in a patient with primary psychogenic polydipsia
Rev Bras Ter Intensiva. 2015;27(1):77-81
Abstract
Case ReportRecurrent rhabdomyolysis secondary to hyponatremia in a patient with primary psychogenic polydipsia
Rev Bras Ter Intensiva. 2015;27(1):77-81
DOI 10.5935/0103-507X.20150013
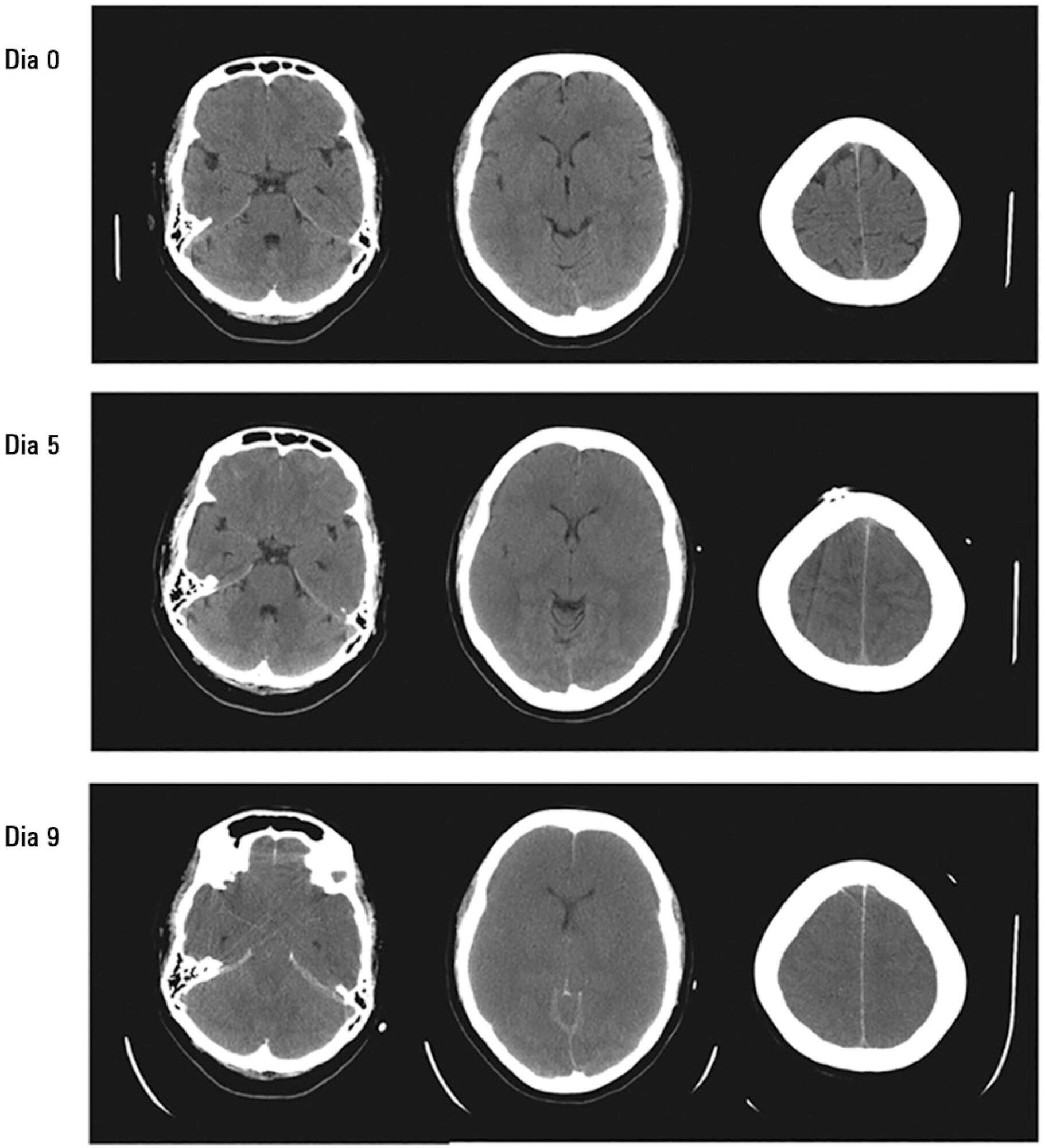
Views0Rhabdomyolysis is characterized by the destruction of skeletal muscle tissue, and its main causes are trauma, toxic substances and electrolyte disturbances. Among the latter is hyponatremia-induced rhabdomyolysis, a rare condition that occurs mainly in patients with psychogenic polydipsia. Psycogenic polydipsia mostly affects patients with schizophrenia, coursing with hyponatremia in almost 25% of the cases. It is also in this context that rhabdomyolysis secondary to hyponatremia occurs most often. In this article, the case of a 49-year-old male with a history of schizophrenia, medicated with clozapine, and brought to the emergency room in a state of coma and seizures is described. Severe hypoosmolar hyponatremia with cerebral edema was found on a computed tomography examination, and a subsequent diagnosis of hyponatremia secondary to psychogenic polydipsia was made. Hyponatremia correction therapy was started, and the patient was admitted to the intensive care unit. After the hyponatremia correction, the patient presented with analytical worsening, showing marked rhabdomyolysis with a creatine phosphokinase level of 44.058UI/L on day 3 of hospitalization. The condition showed a subsequent progressive improvement with therapy, with no occurrence of kidney damage. This case stresses the need for monitoring rhabdomyolysis markers in severe hyponatremia, illustrating the condition of rhabdomyolysis secondary to hyponatremia induced by psychogenic polydipsia, which should be considered in patients undergoing treatment with neuroleptics.
Keywords:Case reportsClozapineHyponatremiaMyelinolysis, central pontinePolydipsia, psychogenicRhabdomyolysisWater intoxicationSee moreViews0Abstract
Case ReportRecurrent rhabdomyolysis secondary to hyponatremia in a patient with primary psychogenic polydipsia
Rev Bras Ter Intensiva. 2015;27(1):77-81
DOI 10.5935/0103-507X.20150013
Views0Rhabdomyolysis is characterized by the destruction of skeletal muscle tissue, and its main causes are trauma, toxic substances and electrolyte disturbances. Among the latter is hyponatremia-induced rhabdomyolysis, a rare condition that occurs mainly in patients with psychogenic polydipsia. Psycogenic polydipsia mostly affects patients with schizophrenia, coursing with hyponatremia in almost 25% of the cases. It is also in this context that rhabdomyolysis secondary to hyponatremia occurs most often. In this article, the case of a 49-year-old male with a history of schizophrenia, medicated with clozapine, and brought to the emergency room in a state of coma and seizures is described. Severe hypoosmolar hyponatremia with cerebral edema was found on a computed tomography examination, and a subsequent diagnosis of hyponatremia secondary to psychogenic polydipsia was made. Hyponatremia correction therapy was started, and the patient was admitted to the intensive care unit. After the hyponatremia correction, the patient presented with analytical worsening, showing marked rhabdomyolysis with a creatine phosphokinase level of 44.058UI/L on day 3 of hospitalization. The condition showed a subsequent progressive improvement with therapy, with no occurrence of kidney damage. This case stresses the need for monitoring rhabdomyolysis markers in severe hyponatremia, illustrating the condition of rhabdomyolysis secondary to hyponatremia induced by psychogenic polydipsia, which should be considered in patients undergoing treatment with neuroleptics.
Keywords:Case reportsClozapineHyponatremiaMyelinolysis, central pontinePolydipsia, psychogenicRhabdomyolysisWater intoxicationSee more -
Letters to the Editor
To: Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review
Rev Bras Ter Intensiva. 2015;27(1):82-84
Abstract
Letters to the EditorTo: Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review
Rev Bras Ter Intensiva. 2015;27(1):82-84
DOI 10.5935/0103-507X.20150014
Views0To the Editor, We would like to discuss the recent publication titled “Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review.”() In this report, Lobo et al. noted that “the H1N1 influenza virus should be considered an etiologic agent of myocarditis”() and concluded that “the use of extracorporeal membrane oxygenation therapy […]See moreViews0Abstract
Letters to the EditorTo: Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review
Rev Bras Ter Intensiva. 2015;27(1):82-84
DOI 10.5935/0103-507X.20150014
Views0To the Editor, We would like to discuss the recent publication titled “Fulminant myocarditis associated with the H1N1 influenza virus: case report and literature review.”() In this report, Lobo et al. noted that “the H1N1 influenza virus should be considered an etiologic agent of myocarditis”() and concluded that “the use of extracorporeal membrane oxygenation therapy […]See more -
Author’s Response
AUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
Abstract
Author’s ResponseAUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
DOI 10.5935/0103-507X.20150015
Views0We thank Mattos and Nunes for their careful reading, comments and concerns about our study.() Since April 2011, the Brazilian Health Ministry has created a system devoted to the care for health technology assessment, which is called “Comissão Nacional de Incorporação de Tecnologias para o SUS (CONITEC)”. Moreover, the method for technology incorporation is positively […]See moreViews0Abstract
Author’s ResponseAUTHORS’ RESPONSE
Rev Bras Ter Intensiva. 2015;27(1):85-88
DOI 10.5935/0103-507X.20150015
Views0We thank Mattos and Nunes for their careful reading, comments and concerns about our study.() Since April 2011, the Brazilian Health Ministry has created a system devoted to the care for health technology assessment, which is called “Comissão Nacional de Incorporação de Tecnologias para o SUS (CONITEC)”. Moreover, the method for technology incorporation is positively […]See more
Volume Articles - Critical Care Science (CCS)
