-
Editorial
Categorical measurements of subjectiveness: is there still a role for the ASA classification?
Rev Bras Ter Intensiva. 2015;27(2):89-91
Abstract
EditorialCategorical measurements of subjectiveness: is there still a role for the ASA classification?
Rev Bras Ter Intensiva. 2015;27(2):89-91
DOI 10.5935/0103-507X.20150016
Views0In 1941, Saklad proposed a classification system that attempted to assess and measure a patient’s physiologic reserve before a surgical procedure.() After undergoing a few modifications, it became widely known as the American Society of Anesthesiologists (ASA) physical status classification system.() It became widely used and became part of the routine pre-operative assessment in many […]See moreViews0

Abstract
EditorialCategorical measurements of subjectiveness: is there still a role for the ASA classification?
Rev Bras Ter Intensiva. 2015;27(2):89-91
DOI 10.5935/0103-507X.20150016
Views0In 1941, Saklad proposed a classification system that attempted to assess and measure a patient’s physiologic reserve before a surgical procedure.() After undergoing a few modifications, it became widely known as the American Society of Anesthesiologists (ASA) physical status classification system.() It became widely used and became part of the routine pre-operative assessment in many […]See more -
Commentaries
Should microcirculation monitoring be used to guide fluid resuscitation in severe sepsis and septic shock?
Rev Bras Ter Intensiva. 2015;27(2):92-95
Abstract
CommentariesShould microcirculation monitoring be used to guide fluid resuscitation in severe sepsis and septic shock?
Rev Bras Ter Intensiva. 2015;27(2):92-95
DOI 10.5935/0103-507X.20150017
Views0Tissue hypoperfusion and subsequent limited oxygen transport are critical features conducting to organ failure during shock states. Therefore, early identification of tissue hypoperfusion and adequate resuscitation are key for improving the probability of survival after septic shock.(,) However, how to identify organ perfusion abnormalities at the bedside and select the type and amount of fluids […]See moreViews0Abstract
CommentariesShould microcirculation monitoring be used to guide fluid resuscitation in severe sepsis and septic shock?
Rev Bras Ter Intensiva. 2015;27(2):92-95
DOI 10.5935/0103-507X.20150017
Views0Tissue hypoperfusion and subsequent limited oxygen transport are critical features conducting to organ failure during shock states. Therefore, early identification of tissue hypoperfusion and adequate resuscitation are key for improving the probability of survival after septic shock.(,) However, how to identify organ perfusion abnormalities at the bedside and select the type and amount of fluids […]See more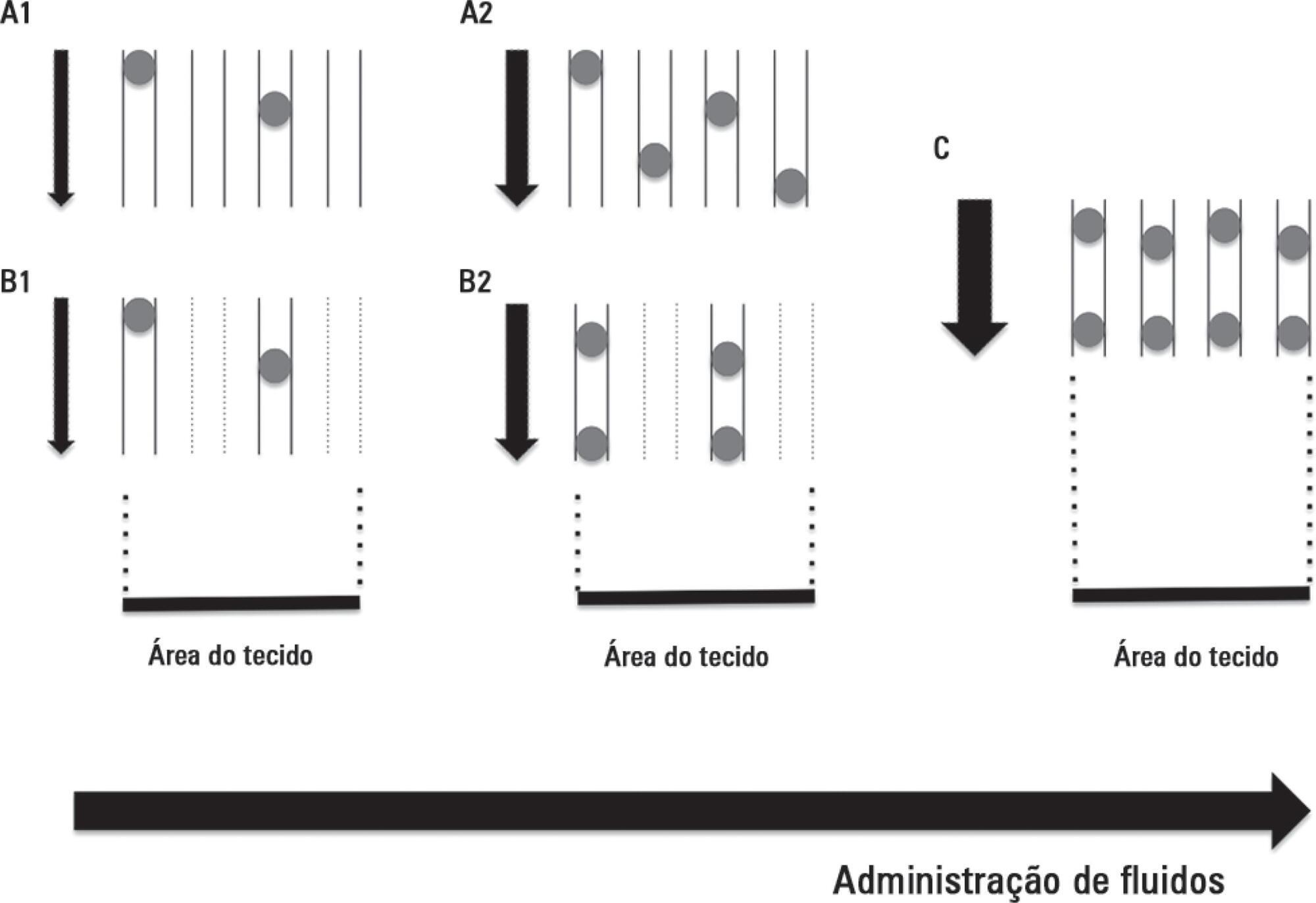
-
Commentaries
Systematic screening is essential for early diagnosis of severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(2):96-101
Abstract
CommentariesSystematic screening is essential for early diagnosis of severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(2):96-101
DOI 10.5935/0103-507X.20150018
Views0SEPSIS, EARLY INTERVENTIONS AND MORTALITYFor over a decade, after studies showing the benefit of early goal-directed therapy() and the publication of the first Survival Sepsis Campaign (SSC) guidelines in 2004,() several other pieces of evidence have demonstrated the importance of early treatment in reducing mortality among patients with severe sepsis or septic shock.(–) This evidence […]See moreViews0Abstract
CommentariesSystematic screening is essential for early diagnosis of severe sepsis and septic shock
Rev Bras Ter Intensiva. 2015;27(2):96-101
DOI 10.5935/0103-507X.20150018
Views0SEPSIS, EARLY INTERVENTIONS AND MORTALITYFor over a decade, after studies showing the benefit of early goal-directed therapy() and the publication of the first Survival Sepsis Campaign (SSC) guidelines in 2004,() several other pieces of evidence have demonstrated the importance of early treatment in reducing mortality among patients with severe sepsis or septic shock.(–) This evidence […]See more -
Commentaries
Optimizing perioperative mechanical ventilation as a key quality improvement target
Rev Bras Ter Intensiva. 2015;27(2):102-104
Abstract
CommentariesOptimizing perioperative mechanical ventilation as a key quality improvement target
Rev Bras Ter Intensiva. 2015;27(2):102-104
DOI 10.5935/0103-507X.20150019
Views0BACKGROUNDThe occurrence of postoperative pulmonary complications is strongly associated with increased hospital mortality and prolonged postoperative hospital stay.(,) Postoperative pulmonary complications could, at least in part be prevented by using so-called lung protective mechanical ventilation strategies, which may include use of low tidal volume (VT), positive end-expiratory pressure (PEEP) and low oxygen fractions (FiO2).()[…]See moreViews0Abstract
CommentariesOptimizing perioperative mechanical ventilation as a key quality improvement target
Rev Bras Ter Intensiva. 2015;27(2):102-104
DOI 10.5935/0103-507X.20150019
Views0BACKGROUNDThe occurrence of postoperative pulmonary complications is strongly associated with increased hospital mortality and prolonged postoperative hospital stay.(,) Postoperative pulmonary complications could, at least in part be prevented by using so-called lung protective mechanical ventilation strategies, which may include use of low tidal volume (VT), positive end-expiratory pressure (PEEP) and low oxygen fractions (FiO2).()[…]See more -
Original Articles
American Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
Abstract
Original ArticlesAmerican Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
DOI 10.5935/0103-507X.20150020
Views0See moreABSTRACT
Objective:
The European Surgical Outcomes Study described mortality following in-patient surgery. Several factors were identified that were able to predict poor outcomes in a multivariate analysis. These included age, procedure urgency, severity and type and the American Association of Anaesthesia score. This study describes in greater detail the relationship between the American Association of Anaesthesia score and postoperative mortality.
Methods:
Patients in this 7-day cohort study were enrolled in April 2011. Consecutive patients aged 16 years and older undergoing inpatient non-cardiac surgery with a recorded American Association of Anaesthesia score in 498 hospitals across 28 European nations were included and followed up for a maximum of 60 days. The primary endpoint was in-hospital mortality. Decision tree analysis with the CHAID (SPSS) system was used to delineate nodes associated with mortality.
Results:
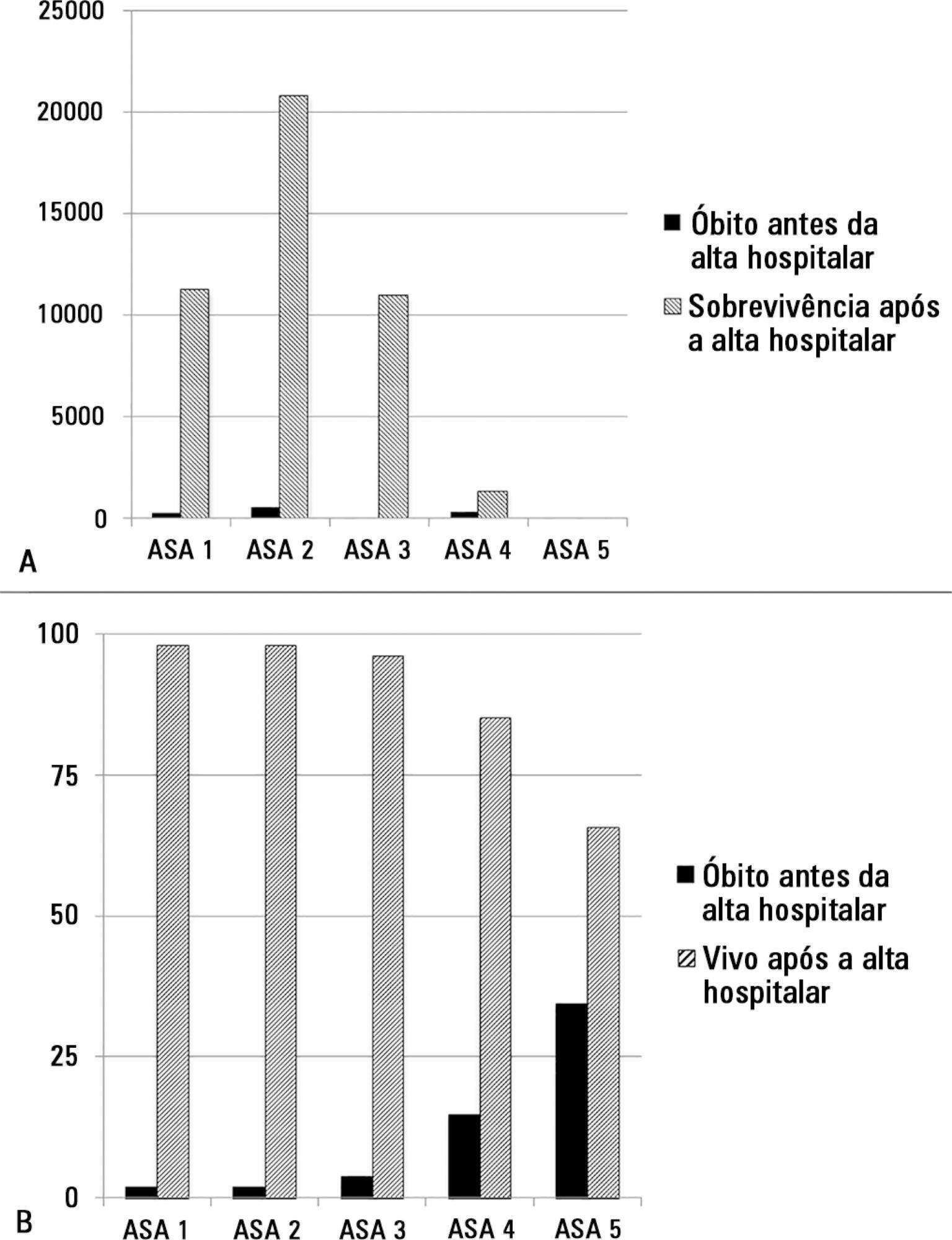
The study enrolled 46,539 patients. Due to missing values, 873 patients were excluded, resulting in the analysis of 45,666 patients. Increasing American Association of Anaesthesia scores were associated with increased admission rates to intensive care and higher mortality rates. Despite a progressive relationship with mortality, discrimination was poor, with an area under the ROC curve of 0.658 (95% CI 0.642 – 0.6775). Using regression trees (CHAID), we identified four discrete American Association of Anaesthesia nodes associated with mortality, with American Association of Anaesthesia 1 and American Association of Anaesthesia 2 compressed into the same node.
Conclusion:
The American Association of Anaesthesia score can be used to determine higher risk groups of surgical patients, but clinicians cannot use the score to discriminate between grades 1 and 2. Overall, the discriminatory power of the model was less than acceptable for widespread use.
Views0Abstract
Original ArticlesAmerican Society of Anesthesiologists Score: still useful after 60 years? Results of the EuSOS Study
Rev Bras Ter Intensiva. 2015;27(2):105-112
DOI 10.5935/0103-507X.20150020
Views0See moreABSTRACT
Objective:
The European Surgical Outcomes Study described mortality following in-patient surgery. Several factors were identified that were able to predict poor outcomes in a multivariate analysis. These included age, procedure urgency, severity and type and the American Association of Anaesthesia score. This study describes in greater detail the relationship between the American Association of Anaesthesia score and postoperative mortality.
Methods:
Patients in this 7-day cohort study were enrolled in April 2011. Consecutive patients aged 16 years and older undergoing inpatient non-cardiac surgery with a recorded American Association of Anaesthesia score in 498 hospitals across 28 European nations were included and followed up for a maximum of 60 days. The primary endpoint was in-hospital mortality. Decision tree analysis with the CHAID (SPSS) system was used to delineate nodes associated with mortality.
Results:
The study enrolled 46,539 patients. Due to missing values, 873 patients were excluded, resulting in the analysis of 45,666 patients. Increasing American Association of Anaesthesia scores were associated with increased admission rates to intensive care and higher mortality rates. Despite a progressive relationship with mortality, discrimination was poor, with an area under the ROC curve of 0.658 (95% CI 0.642 – 0.6775). Using regression trees (CHAID), we identified four discrete American Association of Anaesthesia nodes associated with mortality, with American Association of Anaesthesia 1 and American Association of Anaesthesia 2 compressed into the same node.
Conclusion:
The American Association of Anaesthesia score can be used to determine higher risk groups of surgical patients, but clinicians cannot use the score to discriminate between grades 1 and 2. Overall, the discriminatory power of the model was less than acceptable for widespread use.
-
Original Articles
Decompressive craniectomy in severe traumatic brain injury: prognostic factors and complications
Rev Bras Ter Intensiva. 2015;27(2):113-118
Abstract
Original ArticlesDecompressive craniectomy in severe traumatic brain injury: prognostic factors and complications
Rev Bras Ter Intensiva. 2015;27(2):113-118
DOI 10.5935/0103-507X.20150021
Views0ABSTRACT
Objective:
To analyze the clinical characteristics, complications and factors associated with the prognosis of severe traumatic brain injury among patients who undergo a decompressive craniectomy.
Methods:
Retrospective study of patients seen in an intensive care unit with severe traumatic brain injury in whom a decompressive craniectomy was performed between the years 2003 and 2012. Patients were followed until their discharge from the intensive care unit. Their clinical-tomographic characteristics, complications, and factors associated with prognosis (univariate and multivariate analysis) were analyzed.
Results:
A total of 64 patients were studied. Primary and lateral decompressive craniectomies were performed for the majority of patients. A high incidence of complications was found (78% neurological and 52% nonneurological). A total of 42 patients (66%) presented poor outcomes, and 22 (34%) had good neurological outcomes. Of the patients who survived, 61% had good neurological outcomes. In the univariate analysis, the factors significantly associated with poor neurological outcome were postdecompressive craniectomy intracranial hypertension, greater severity and worse neurological state at admission. In the multivariate analysis, only postcraniectomy intracranial hypertension was significantly associated with a poor outcome.
Conclusion:
This study involved a very severe and difficult to manage group of patients with high morbimortality. Intracranial hypertension was a main factor of poor outcome in this population.
Keywords:Brain injuriesCraniocerebral trauma/complicationsDecompressive craniectomy/adverse effectsIntracranial hypertension/etiologySee moreViews0Abstract
Original ArticlesDecompressive craniectomy in severe traumatic brain injury: prognostic factors and complications
Rev Bras Ter Intensiva. 2015;27(2):113-118
DOI 10.5935/0103-507X.20150021
Views0ABSTRACT
Objective:
To analyze the clinical characteristics, complications and factors associated with the prognosis of severe traumatic brain injury among patients who undergo a decompressive craniectomy.
Methods:
Retrospective study of patients seen in an intensive care unit with severe traumatic brain injury in whom a decompressive craniectomy was performed between the years 2003 and 2012. Patients were followed until their discharge from the intensive care unit. Their clinical-tomographic characteristics, complications, and factors associated with prognosis (univariate and multivariate analysis) were analyzed.
Results:
A total of 64 patients were studied. Primary and lateral decompressive craniectomies were performed for the majority of patients. A high incidence of complications was found (78% neurological and 52% nonneurological). A total of 42 patients (66%) presented poor outcomes, and 22 (34%) had good neurological outcomes. Of the patients who survived, 61% had good neurological outcomes. In the univariate analysis, the factors significantly associated with poor neurological outcome were postdecompressive craniectomy intracranial hypertension, greater severity and worse neurological state at admission. In the multivariate analysis, only postcraniectomy intracranial hypertension was significantly associated with a poor outcome.
Conclusion:
This study involved a very severe and difficult to manage group of patients with high morbimortality. Intracranial hypertension was a main factor of poor outcome in this population.
Keywords:Brain injuriesCraniocerebral trauma/complicationsDecompressive craniectomy/adverse effectsIntracranial hypertension/etiologySee more -
Original Articles
Fiber optic bronchoscopy-assisted percutaneous tracheostomy: a decade of experience at a university hospital
Rev Bras Ter Intensiva. 2015;27(2):119-124
Abstract
Original ArticlesFiber optic bronchoscopy-assisted percutaneous tracheostomy: a decade of experience at a university hospital
Rev Bras Ter Intensiva. 2015;27(2):119-124
DOI 10.5935/0103-507X.20150022
Views0See moreABSTRACT
Objective:
To evaluate the efficacy and safety of percutaneous tracheostomy by means of single-step dilation with fiber optic bronchoscopy assistance in critical care patients under mechanical ventilation.
Methods:
Between the years 2004 and 2014, 512 patients with indication of tracheostomy according to clinical criteria, were prospectively and consecutively included in our study. One-third of them were high-risk patients. Demographic variables, APACHE II score, and days on mechanical ventilation prior to percutaneous tracheostomy were recorded. The efficacy of the procedure was evaluated according to an execution success rate and based on the necessity of switching to an open surgical technique. Safety was evaluated according to post-operative and operative complication rates.
Results:
The mean age of the group was 64 ± 18 years (203 women and 309 males). The mean APACHE II score was 21 ± 3. Patients remained an average of 11 ± 3 days on mechanical ventilation before percutaneous tracheostomy was performed. All procedures were successfully completed without the need to switch to an open surgical technique. Eighteen patients (3.5%) presented procedure complications. Five patients experienced transient desaturation, 4 presented low blood pressure related to sedation, and 9 presented minor bleeding, but none required a transfusion. No serious complications or deaths associated with the procedure were recorded. Eleven patients (2.1%) presented post-operative complications. Seven presented minor and transitory bleeding of the percutaneous tracheostomy stoma, 2 suffered displacement of the tracheostomy cannula, and 2 developed a superficial infection of the stoma.
Conclusion:
Percutaneous tracheostomy using the single-step dilation technique with fiber optic bronchoscopy assistance seems to be effective and safe in critically ill patients under mechanical ventilation when performed by experienced intensive care specialists using a standardized procedure.
Views0Abstract
Original ArticlesFiber optic bronchoscopy-assisted percutaneous tracheostomy: a decade of experience at a university hospital
Rev Bras Ter Intensiva. 2015;27(2):119-124
DOI 10.5935/0103-507X.20150022
Views0See moreABSTRACT
Objective:
To evaluate the efficacy and safety of percutaneous tracheostomy by means of single-step dilation with fiber optic bronchoscopy assistance in critical care patients under mechanical ventilation.
Methods:
Between the years 2004 and 2014, 512 patients with indication of tracheostomy according to clinical criteria, were prospectively and consecutively included in our study. One-third of them were high-risk patients. Demographic variables, APACHE II score, and days on mechanical ventilation prior to percutaneous tracheostomy were recorded. The efficacy of the procedure was evaluated according to an execution success rate and based on the necessity of switching to an open surgical technique. Safety was evaluated according to post-operative and operative complication rates.
Results:
The mean age of the group was 64 ± 18 years (203 women and 309 males). The mean APACHE II score was 21 ± 3. Patients remained an average of 11 ± 3 days on mechanical ventilation before percutaneous tracheostomy was performed. All procedures were successfully completed without the need to switch to an open surgical technique. Eighteen patients (3.5%) presented procedure complications. Five patients experienced transient desaturation, 4 presented low blood pressure related to sedation, and 9 presented minor bleeding, but none required a transfusion. No serious complications or deaths associated with the procedure were recorded. Eleven patients (2.1%) presented post-operative complications. Seven presented minor and transitory bleeding of the percutaneous tracheostomy stoma, 2 suffered displacement of the tracheostomy cannula, and 2 developed a superficial infection of the stoma.
Conclusion:
Percutaneous tracheostomy using the single-step dilation technique with fiber optic bronchoscopy assistance seems to be effective and safe in critically ill patients under mechanical ventilation when performed by experienced intensive care specialists using a standardized procedure.
-
Original Articles
Psychosocial factors and prevalence of burnout syndrome among nursing workers in intensive care units
Rev Bras Ter Intensiva. 2015;27(2):125-133
Abstract
Original ArticlesPsychosocial factors and prevalence of burnout syndrome among nursing workers in intensive care units
Rev Bras Ter Intensiva. 2015;27(2):125-133
DOI 10.5935/0103-507X.20150023
Views0See moreABSTRACT
Objective:
To evaluate the prevalence of burnout syndrome among nursing workers in intensive care units and establish associations with psychosocial factors.
Methods:
This descriptive study evaluated 130 professionals, including nurses, nursing technicians, and nursing assistants, who performed their activities in intensive care and coronary care units in 2 large hospitals in the city of Rio de Janeiro, Brazil. Data were collected in 2011 using a self-reported questionnaire. The Maslach Burnout Inventory was used to evaluate the burnout syndrome dimensions, and the Self Reporting Questionnaire was used to evaluate common mental disorders.
Results:
The prevalence of burnout syndrome was 55.3% (n = 72). In the quadrants of the demand-control model, low-strain workers exhibited a prevalence of 64.5% of suspected cases of burnout, whereas high-strain workers exhibited a prevalence of 72.5% of suspected cases (p = 0.006). The prevalence of suspected cases of common mental disorders was 27.7%; of these, 80.6% were associated with burnout syndrome (< 0.0001). The multivariate analysis adjusted for gender, age, educational level, weekly work duration, income, and thoughts about work during free time indicated that the categories associated with intermediate stress levels - active work (OR = 0.26; 95%CI = 0.09 - 0.69) and passive work (OR = 0.22; 95%CI = 0.07 - 0.63) - were protective factors for burnout syndrome.
Conclusion:
Psychosocial factors were associated with the development of burnout syndrome in this group. These results underscore the need for the development of further studies aimed at intervention and the prevention of the syndrome.
Views0Abstract
Original ArticlesPsychosocial factors and prevalence of burnout syndrome among nursing workers in intensive care units
Rev Bras Ter Intensiva. 2015;27(2):125-133
DOI 10.5935/0103-507X.20150023
Views0See moreABSTRACT
Objective:
To evaluate the prevalence of burnout syndrome among nursing workers in intensive care units and establish associations with psychosocial factors.
Methods:
This descriptive study evaluated 130 professionals, including nurses, nursing technicians, and nursing assistants, who performed their activities in intensive care and coronary care units in 2 large hospitals in the city of Rio de Janeiro, Brazil. Data were collected in 2011 using a self-reported questionnaire. The Maslach Burnout Inventory was used to evaluate the burnout syndrome dimensions, and the Self Reporting Questionnaire was used to evaluate common mental disorders.
Results:
The prevalence of burnout syndrome was 55.3% (n = 72). In the quadrants of the demand-control model, low-strain workers exhibited a prevalence of 64.5% of suspected cases of burnout, whereas high-strain workers exhibited a prevalence of 72.5% of suspected cases (p = 0.006). The prevalence of suspected cases of common mental disorders was 27.7%; of these, 80.6% were associated with burnout syndrome (< 0.0001). The multivariate analysis adjusted for gender, age, educational level, weekly work duration, income, and thoughts about work during free time indicated that the categories associated with intermediate stress levels - active work (OR = 0.26; 95%CI = 0.09 - 0.69) and passive work (OR = 0.22; 95%CI = 0.07 - 0.63) - were protective factors for burnout syndrome.
Conclusion:
Psychosocial factors were associated with the development of burnout syndrome in this group. These results underscore the need for the development of further studies aimed at intervention and the prevention of the syndrome.
-
Original Articles
Implementation and results of a new ECMO program for lung transplantation and acute respiratory distress
Rev Bras Ter Intensiva. 2015;27(2):134-140
Abstract
Original ArticlesImplementation and results of a new ECMO program for lung transplantation and acute respiratory distress
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
Views0ABSTRACT
Objective:
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
Methods:
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Results:
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range – IQR: 2 – 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 – 25), and had an intensive care unit stay of 31.5 days (IQR: 19 – 53) and a median hospital stay of 60 days (IQR: 36 – 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 – 14), median mechanical ventilation time of 25 days (IQR: 13 – 37), a 31 day stay in therapy (IQR: 11 – 38), a 32 day stay in the hospital (IQR: 11 – 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
Conclusion:
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive care unitsLung transplantationPrimary graft dysfunctionRespiratory insufficiencySee moreViews0Abstract
Original ArticlesImplementation and results of a new ECMO program for lung transplantation and acute respiratory distress
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
Views0ABSTRACT
Objective:
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
Methods:
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Results:
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range – IQR: 2 – 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 – 25), and had an intensive care unit stay of 31.5 days (IQR: 19 – 53) and a median hospital stay of 60 days (IQR: 36 – 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 – 14), median mechanical ventilation time of 25 days (IQR: 13 – 37), a 31 day stay in therapy (IQR: 11 – 38), a 32 day stay in the hospital (IQR: 11 – 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
Conclusion:
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationIntensive care unitsLung transplantationPrimary graft dysfunctionRespiratory insufficiencySee more -
Original Articles
A gradient-boosted model analysis of the impact of body mass index on the short-term outcomes of critically ill medical patients
Rev Bras Ter Intensiva. 2015;27(2):141-148
Abstract
Original ArticlesA gradient-boosted model analysis of the impact of body mass index on the short-term outcomes of critically ill medical patients
Rev Bras Ter Intensiva. 2015;27(2):141-148
DOI 10.5935/0103-507X.20150025
Views0See moreABSTRACT
Objective:
To evaluate the impact of body mass index on the short-term prognosis of non-surgical critically ill patients while controlling for performance status and comorbidities.
Methods:
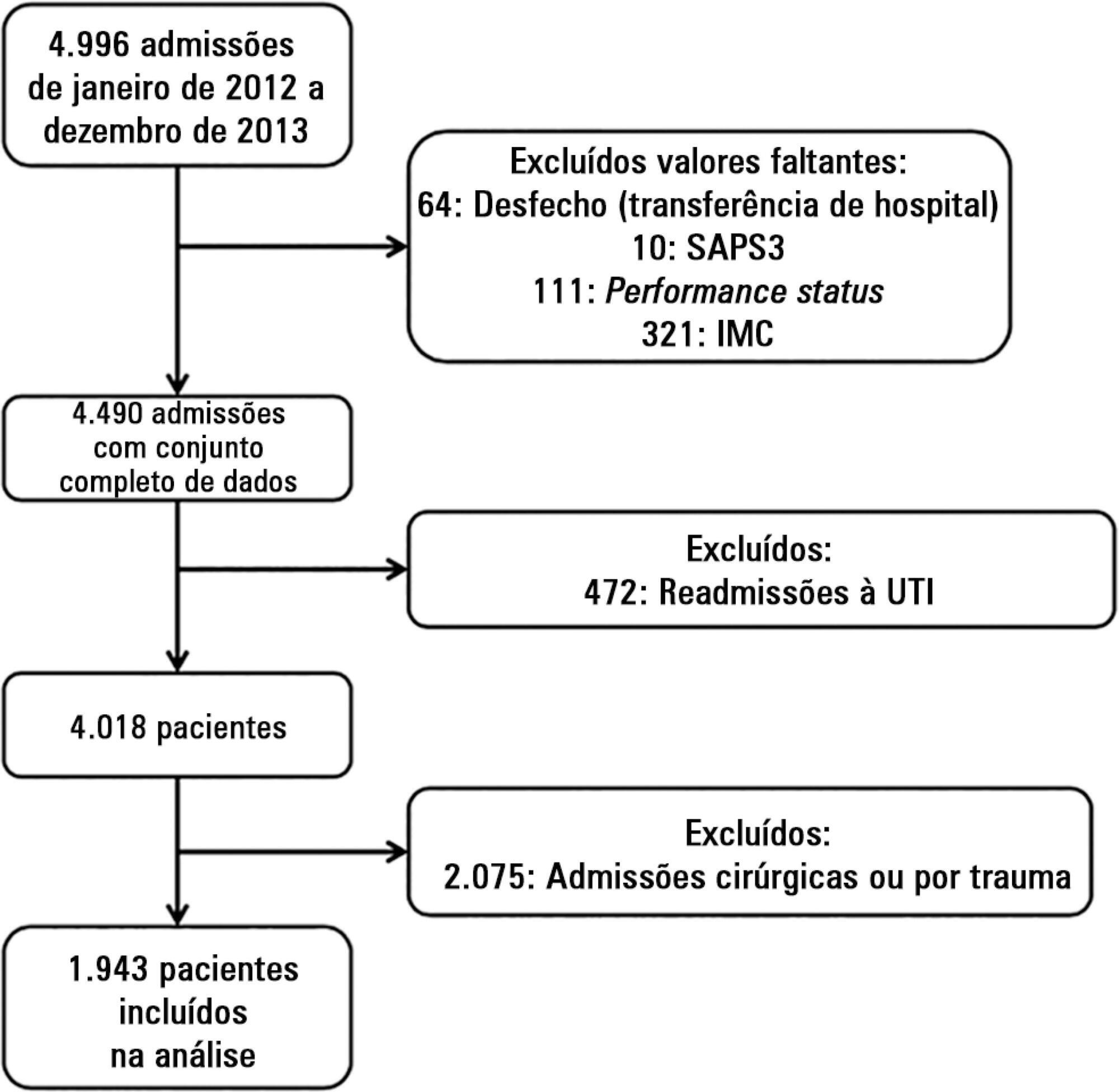
We performed a retrospective analysis on a two-year single-center database including 1943 patients. We evaluated the impact of body mass index on hospital mortality using a gradient-boosted model that also included comorbidities and was assessed by Charlson’s comorbidity index, performance status and illness severity, which was measured by the SAPS3 score. The SAPS3 score was adjusted to avoid including the same variable twice in the model. We also assessed the impact of body mass index on the length of stay in the hospital after intensive care unit admission using multiple linear regressions.
Results:
A low value (< 20kg/m2) was associated with a sharp increase in hospital mortality. Mortality tended to subsequently decrease as body mass index increased, but the impact of a high body mass index in defining mortality was low. Mortality increased as the burden of comorbidities increased and as the performance status decreased. Body mass index interacted with the impact of SAPS3 on patient outcome, but there was no significant interaction between body mass index, performance status and comorbidities. There was no apparent association between body mass index and the length of stay at the hospital after intensive care unit admission.
Conclusion:
Body mass index does appear to influence the shortterm outcomes of critically ill medical patients, who are generally underweight. This association was independent of comorbidities and performance status.
Views0Abstract
Original ArticlesA gradient-boosted model analysis of the impact of body mass index on the short-term outcomes of critically ill medical patients
Rev Bras Ter Intensiva. 2015;27(2):141-148
DOI 10.5935/0103-507X.20150025
Views0See moreABSTRACT
Objective:
To evaluate the impact of body mass index on the short-term prognosis of non-surgical critically ill patients while controlling for performance status and comorbidities.
Methods:
We performed a retrospective analysis on a two-year single-center database including 1943 patients. We evaluated the impact of body mass index on hospital mortality using a gradient-boosted model that also included comorbidities and was assessed by Charlson’s comorbidity index, performance status and illness severity, which was measured by the SAPS3 score. The SAPS3 score was adjusted to avoid including the same variable twice in the model. We also assessed the impact of body mass index on the length of stay in the hospital after intensive care unit admission using multiple linear regressions.
Results:
A low value (< 20kg/m2) was associated with a sharp increase in hospital mortality. Mortality tended to subsequently decrease as body mass index increased, but the impact of a high body mass index in defining mortality was low. Mortality increased as the burden of comorbidities increased and as the performance status decreased. Body mass index interacted with the impact of SAPS3 on patient outcome, but there was no significant interaction between body mass index, performance status and comorbidities. There was no apparent association between body mass index and the length of stay at the hospital after intensive care unit admission.
Conclusion:
Body mass index does appear to influence the shortterm outcomes of critically ill medical patients, who are generally underweight. This association was independent of comorbidities and performance status.
-
Original Articles
Pharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
Abstract
Original ArticlesPharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
DOI 10.5935/0103-507X.20150026
Views0See moreABSTRACT
Objective:
To analyze the clinical activities performed and the accepted pharmacist recommendations made by a pharmacist as a part of his/her daily routine in an adult clinical intensive care unit over a period of three years.
Methods:
A cross-sectional, descriptive, and exploratory study was conducted at a tertiary university hospital from June 2010 to May 2013, in which pharmacist recommendations were categorized and analyzed.
Results:
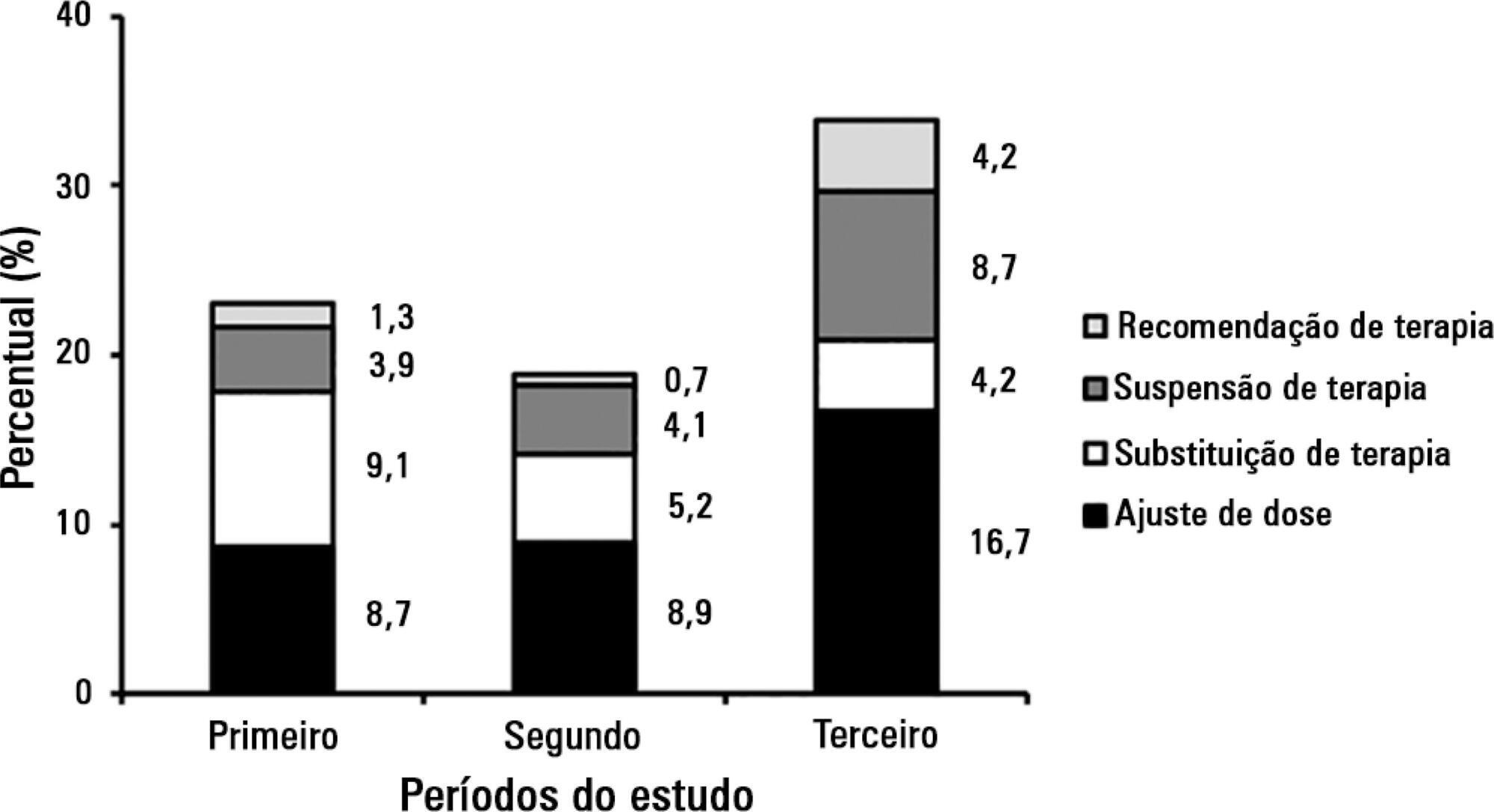
A total of 834 pharmacist recommendations (278 per year, on average) were analyzed and distributed across 21 categories. The recommendations were mainly made to physicians (n = 699; 83.8%) and concerned management of dilutions (n = 120; 14.4%), dose adjustment (n = 100; 12.0%), and adverse drug reactions (n = 91; 10.9%). A comparison per period demonstrated an increase in pharmacist recommendations with larger clinical content and a reduction of recommendations related to logistic aspects, such as drug supply, over time. The recommendations concerned 948 medications, particularly including systemic anti-infectious agents.
Conclusion:
The role that the pharmacist played in the intensive care unit of the institution where the study was performed evolved, shifting from reactive actions related to logistic aspects to effective clinical participation with the multi-professional staff (proactive actions).
Views0Abstract
Original ArticlesPharmacist recommendations in an intensive care unit: three-year clinical activities
Rev Bras Ter Intensiva. 2015;27(2):149-154
DOI 10.5935/0103-507X.20150026
Views0See moreABSTRACT
Objective:
To analyze the clinical activities performed and the accepted pharmacist recommendations made by a pharmacist as a part of his/her daily routine in an adult clinical intensive care unit over a period of three years.
Methods:
A cross-sectional, descriptive, and exploratory study was conducted at a tertiary university hospital from June 2010 to May 2013, in which pharmacist recommendations were categorized and analyzed.
Results:
A total of 834 pharmacist recommendations (278 per year, on average) were analyzed and distributed across 21 categories. The recommendations were mainly made to physicians (n = 699; 83.8%) and concerned management of dilutions (n = 120; 14.4%), dose adjustment (n = 100; 12.0%), and adverse drug reactions (n = 91; 10.9%). A comparison per period demonstrated an increase in pharmacist recommendations with larger clinical content and a reduction of recommendations related to logistic aspects, such as drug supply, over time. The recommendations concerned 948 medications, particularly including systemic anti-infectious agents.
Conclusion:
The role that the pharmacist played in the intensive care unit of the institution where the study was performed evolved, shifting from reactive actions related to logistic aspects to effective clinical participation with the multi-professional staff (proactive actions).
-
Original Articles
Changes in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(2):155-160
Abstract
Original ArticlesChanges in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(2):155-160
DOI 10.5935/0103-507X.20150027
Views0See moreABSTRACT
Objective:
To evaluate the changes in ventilatory mechanics and hemodynamics that occur in patients dependent on mechanical ventilation who are subjected to a standard respiratory therapy protocol.
Methods:
This experimental and prospective study was performed in two intensive care units, in which patients dependent on mechanical ventilation for more than 48 hours were consecutively enrolled and subjected to an established respiratory physiotherapy protocol. Ventilatory variables (dynamic lung compliance, respiratory system resistance, tidal volume, peak inspiratory pressure, respiratory rate, and oxygen saturation) and hemodynamic variables (heart rate) were measured one hour before (T-1), immediately after (T0) and one hour after (T+1) applying the respiratory physiotherapy protocol.
Results:
During the period of data collection, 104 patients were included in the study. Regarding the ventilatory variables, an increase in dynamic lung compliance (T-1 = 52.3 ± 16.1mL/cmH2O versus T0 = 65.1 ± 19.1mL/cmH2O; p < 0.001), tidal volume (T-1 = 550 ± 134mL versus T0 = 698 ± 155mL; p < 0.001), and peripheral oxygen saturation (T-1 = 96.5 ± 2.29% versus T0 = 98.2 ± 1.62%; p < 0.001) were observed, in addition to a reduction of respiratory system resistance (T-1 = 14.2 ± 4.63cmH2O/L/s versus T0 = 11.0 ± 3.43cmH2O/L/s; p < 0.001), after applying the respiratory physiotherapy protocol. All changes were present in the assessment performed one hour (T+1) after the application of the respiratory physiotherapy protocol. Regarding the hemodynamic variables, an immediate increase in the heart rate after application of the protocol was observed, but that increase was not maintained (T-1 = 88.9 ± 18.7 bpm versus T0 = 93.7 ± 19.2bpm versus T+1 = 88.5 ± 17.1bpm; p < 0.001).
Conclusion:
Respiratory therapy leads to immediate changes in the lung mechanics and hemodynamics of mechanical ventilation-dependent patients, and ventilatory changes are likely to remain for at least one hour.
Views0Abstract
Original ArticlesChanges in respiratory mechanics during respiratory physiotherapy in mechanically ventilated patients
Rev Bras Ter Intensiva. 2015;27(2):155-160
DOI 10.5935/0103-507X.20150027
Views0See moreABSTRACT
Objective:
To evaluate the changes in ventilatory mechanics and hemodynamics that occur in patients dependent on mechanical ventilation who are subjected to a standard respiratory therapy protocol.
Methods:
This experimental and prospective study was performed in two intensive care units, in which patients dependent on mechanical ventilation for more than 48 hours were consecutively enrolled and subjected to an established respiratory physiotherapy protocol. Ventilatory variables (dynamic lung compliance, respiratory system resistance, tidal volume, peak inspiratory pressure, respiratory rate, and oxygen saturation) and hemodynamic variables (heart rate) were measured one hour before (T-1), immediately after (T0) and one hour after (T+1) applying the respiratory physiotherapy protocol.
Results:
During the period of data collection, 104 patients were included in the study. Regarding the ventilatory variables, an increase in dynamic lung compliance (T-1 = 52.3 ± 16.1mL/cmH2O versus T0 = 65.1 ± 19.1mL/cmH2O; p < 0.001), tidal volume (T-1 = 550 ± 134mL versus T0 = 698 ± 155mL; p < 0.001), and peripheral oxygen saturation (T-1 = 96.5 ± 2.29% versus T0 = 98.2 ± 1.62%; p < 0.001) were observed, in addition to a reduction of respiratory system resistance (T-1 = 14.2 ± 4.63cmH2O/L/s versus T0 = 11.0 ± 3.43cmH2O/L/s; p < 0.001), after applying the respiratory physiotherapy protocol. All changes were present in the assessment performed one hour (T+1) after the application of the respiratory physiotherapy protocol. Regarding the hemodynamic variables, an immediate increase in the heart rate after application of the protocol was observed, but that increase was not maintained (T-1 = 88.9 ± 18.7 bpm versus T0 = 93.7 ± 19.2bpm versus T+1 = 88.5 ± 17.1bpm; p < 0.001).
Conclusion:
Respiratory therapy leads to immediate changes in the lung mechanics and hemodynamics of mechanical ventilation-dependent patients, and ventilatory changes are likely to remain for at least one hour.
-
Original Articles
Functional evolution of critically ill patients undergoing an early rehabilitation protocol
Rev Bras Ter Intensiva. 2015;27(2):161-169
Abstract
Original ArticlesFunctional evolution of critically ill patients undergoing an early rehabilitation protocol
Rev Bras Ter Intensiva. 2015;27(2):161-169
DOI 10.5935/0103-507X.20150028
Views0See moreABSTRACT
Objective:
Evaluation of the functional outcomes of patients undergoing an early rehabilitation protocol for critically ill patients from admission to discharge from the intensive care unit.
Methods:
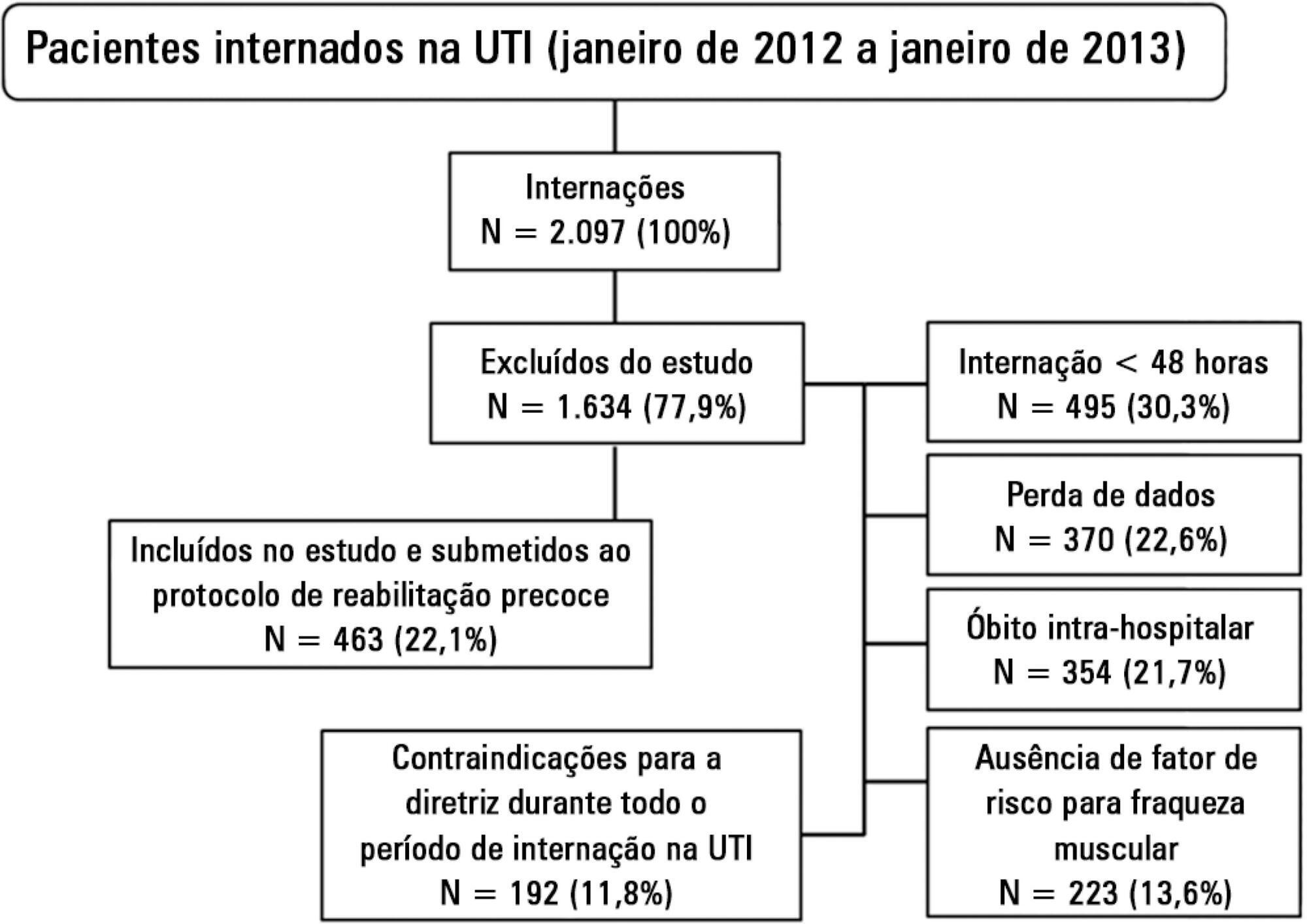
A retrospective cross-sectional study was conducted that included 463 adult patients with clinical and/or surgical diagnosis undergoing an early rehabilitation protocol. The overall muscle strength was evaluated at admission to the intensive care unit using the Medical Research Council scale. Patients were allocated to one of four intervention plans according to the Medical Research Council score, the suitability of the plan’s parameters, and the increasing scale of the plan expressing improved functional status. Uncooperative patients were allocated to intervention plans based on their functional status. The overall muscle strength and/or functional status were reevaluated upon discharge from the intensive care unit by comparison between the Intervention Plans upon admission (Planinitial) and discharge (Planfinal). Patients were classified into three groups according to the improvement of their functional status or not: responsive 1 (Planfinal > Planinitial), responsive 2 (Planfinal = Planinitial) and unresponsive (Planfinal < Planinitial).
Results:
In total, 432 (93.3%) of 463 patients undergoing the protocol responded positively to the intervention strategy, showing maintenance and/or improvement of the initial functional status. Clinical patients classified as unresponsive were older (74.3 ± 15.1 years of age; p = 0.03) and had longer lengths of intensive care unit (11.6 ± 14.2 days; p = 0.047) and hospital (34.5 ± 34.1 days; p = 0.002) stays.
Conclusion:
The maintenance and/or improvement of the admission functional status were associated with shorter lengths of intensive care unit and hospital stays. The results suggest that the type of diagnosis, clinical or surgical, fails to define the positive response to an early rehabilitation protocol.
Views0Abstract
Original ArticlesFunctional evolution of critically ill patients undergoing an early rehabilitation protocol
Rev Bras Ter Intensiva. 2015;27(2):161-169
DOI 10.5935/0103-507X.20150028
Views0See moreABSTRACT
Objective:
Evaluation of the functional outcomes of patients undergoing an early rehabilitation protocol for critically ill patients from admission to discharge from the intensive care unit.
Methods:
A retrospective cross-sectional study was conducted that included 463 adult patients with clinical and/or surgical diagnosis undergoing an early rehabilitation protocol. The overall muscle strength was evaluated at admission to the intensive care unit using the Medical Research Council scale. Patients were allocated to one of four intervention plans according to the Medical Research Council score, the suitability of the plan’s parameters, and the increasing scale of the plan expressing improved functional status. Uncooperative patients were allocated to intervention plans based on their functional status. The overall muscle strength and/or functional status were reevaluated upon discharge from the intensive care unit by comparison between the Intervention Plans upon admission (Planinitial) and discharge (Planfinal). Patients were classified into three groups according to the improvement of their functional status or not: responsive 1 (Planfinal > Planinitial), responsive 2 (Planfinal = Planinitial) and unresponsive (Planfinal < Planinitial).
Results:
In total, 432 (93.3%) of 463 patients undergoing the protocol responded positively to the intervention strategy, showing maintenance and/or improvement of the initial functional status. Clinical patients classified as unresponsive were older (74.3 ± 15.1 years of age; p = 0.03) and had longer lengths of intensive care unit (11.6 ± 14.2 days; p = 0.047) and hospital (34.5 ± 34.1 days; p = 0.002) stays.
Conclusion:
The maintenance and/or improvement of the admission functional status were associated with shorter lengths of intensive care unit and hospital stays. The results suggest that the type of diagnosis, clinical or surgical, fails to define the positive response to an early rehabilitation protocol.
-
Original Articles
Baseline acetylcholinesterase activity and serotonin plasma levels are not associated with delirium in critically ill patients
Rev Bras Ter Intensiva. 2015;27(2):170-177
Abstract
Original ArticlesBaseline acetylcholinesterase activity and serotonin plasma levels are not associated with delirium in critically ill patients
Rev Bras Ter Intensiva. 2015;27(2):170-177
DOI 10.5935/0103-507X.20150029
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate whether plasma serotonin levels or acetylcholinesterase activities determined upon intensive care unit admission could predict the occurrence of acute brain dysfunction in intensive care unit patients.
Methods:
A prospective cohort study was conducted with a sample of 77 non-consecutive patients observed between May 2009 and September 2010. Delirium was determined using the Confusion Assessment Method for the Intensive Care Unit tool, and the acetylcholinesterase and serotonin measurements were determined from blood samples collected up to a maximum of 24 h after the admission of the patient to the intensive care unit.
Results:
In the present study, 38 (49.6%) patients developed delirium during their intensive care unit stays. Neither serum acetylcholinesterase activity nor serotonin level was independently associated with delirium. No significant correlations of acetylcholinesterase activity or serotonin level with delirium/coma-free days were observed, but in the patients who developed delirium, there was a strong negative correlation between the acetylcholinesterase level and the number of delirium/coma-free days, indicating that higher acetylcholinesterase levels are associated with fewer days alive without delirium or coma. No associations were found between the biomarkers and mortality.
Conclusions:
Neither serum acetylcholinesterase activity nor serotonin level was associated with delirium or acute brain dysfunction in critically ill patients. Sepsis did not modify these relationships.
Views0Abstract
Original ArticlesBaseline acetylcholinesterase activity and serotonin plasma levels are not associated with delirium in critically ill patients
Rev Bras Ter Intensiva. 2015;27(2):170-177
DOI 10.5935/0103-507X.20150029
Views0See moreABSTRACT
Objective:
The aim of this study was to investigate whether plasma serotonin levels or acetylcholinesterase activities determined upon intensive care unit admission could predict the occurrence of acute brain dysfunction in intensive care unit patients.
Methods:
A prospective cohort study was conducted with a sample of 77 non-consecutive patients observed between May 2009 and September 2010. Delirium was determined using the Confusion Assessment Method for the Intensive Care Unit tool, and the acetylcholinesterase and serotonin measurements were determined from blood samples collected up to a maximum of 24 h after the admission of the patient to the intensive care unit.
Results:
In the present study, 38 (49.6%) patients developed delirium during their intensive care unit stays. Neither serum acetylcholinesterase activity nor serotonin level was independently associated with delirium. No significant correlations of acetylcholinesterase activity or serotonin level with delirium/coma-free days were observed, but in the patients who developed delirium, there was a strong negative correlation between the acetylcholinesterase level and the number of delirium/coma-free days, indicating that higher acetylcholinesterase levels are associated with fewer days alive without delirium or coma. No associations were found between the biomarkers and mortality.
Conclusions:
Neither serum acetylcholinesterase activity nor serotonin level was associated with delirium or acute brain dysfunction in critically ill patients. Sepsis did not modify these relationships.
-
Original Articles
Blood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
Abstract
Original ArticlesBlood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
Views0ABSTRACT
Objective:
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Methods:
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
Results:
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = – 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Conclusion:
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee moreViews0Abstract
Original ArticlesBlood flow/pump rotation ratio as an artificial lung performance monitoring tool during extracorporeal respiratory support using centrifugal pumps
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
Views0ABSTRACT
Objective:
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Methods:
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
Results:
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = – 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Conclusion:
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Keywords:acute respiratory distress syndromeExtracorporeal membrane oxygenationMultiple organ failureRespiration, artificialSwineSee more
-
Case Report
Aortic and tricuspid endocarditis in hemodialysis patient with systemic and pulmonary embolism
Rev Bras Ter Intensiva. 2015;27(2):185-189
Abstract
Case ReportAortic and tricuspid endocarditis in hemodialysis patient with systemic and pulmonary embolism
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
Views0ABSTRACT
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Keywords:Aortic valveCase reportsEmbolismEndocarditis/etiologyRenal dialysisTomography, X-ray computedTricuspid valveSee moreViews0Abstract
Case ReportAortic and tricuspid endocarditis in hemodialysis patient with systemic and pulmonary embolism
Rev Bras Ter Intensiva. 2015;27(2):185-189
DOI 10.5935/0103-507X.20150031
Views0ABSTRACT
This is a case report of a 43-year-old Caucasian male with end-stage renal disease being treated with hemodialysis and infective endocarditis in the aortic and tricuspid valves. The clinical presentation was dominated by neurologic impairment with cerebral embolism and hemorrhagic components. A thoracoabdominal computerized tomography scan revealed septic pulmonary embolus. The patient underwent empirical antibiotherapy with ceftriaxone, gentamicin and vancomycin, and the therapy was changed to flucloxacilin and gentamicin after the isolation of S. aureus in blood cultures. The multidisciplinary team determined that the patient should undergo valve replacement after the stabilization of the intracranial hemorrhage; however, on the 8th day of hospitalization, the patient entered cardiac arrest due to a massive septic pulmonary embolism and died. Despite the risk of aggravation of the hemorrhagic cerebral lesion, early surgical intervention should be considered in high-risk patients.
Keywords:Aortic valveCase reportsEmbolismEndocarditis/etiologyRenal dialysisTomography, X-ray computedTricuspid valveSee more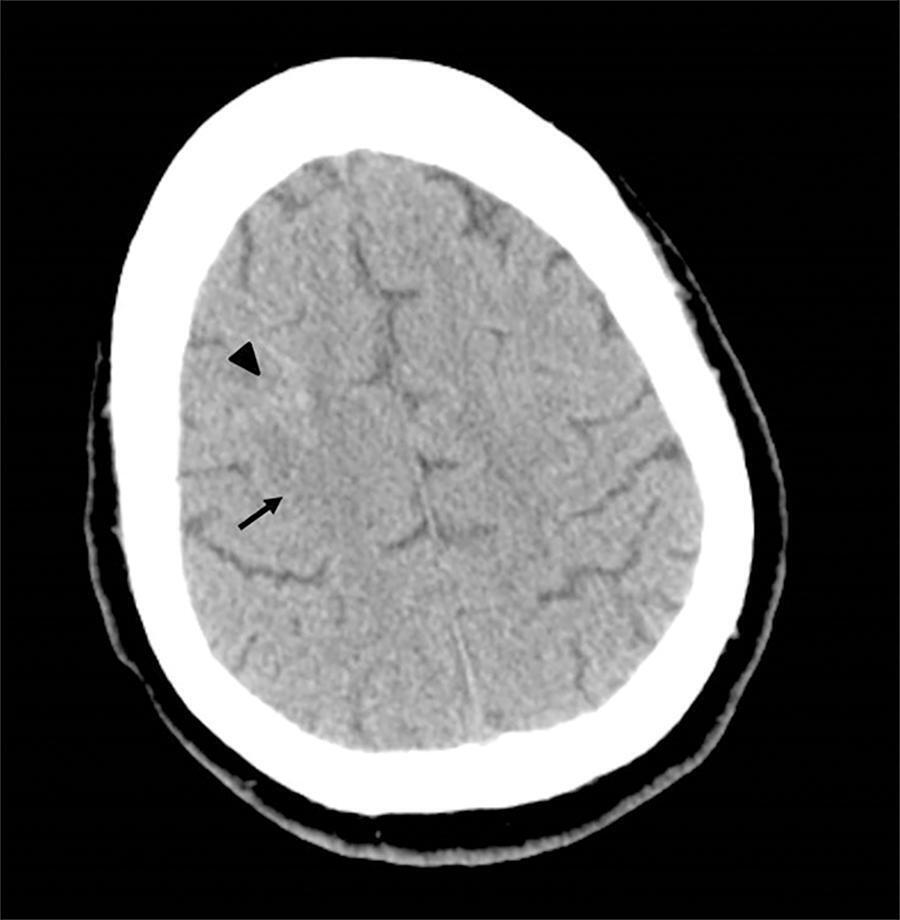
Volume Articles - Critical Care Science (CCS)
