
You searched for:"Gilberto Friedman"
We found (29) results for your search.-
Original Article
Adequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
Abstract
Original ArticleAdequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
DOI 10.5935/0103-507X.20190004
Views0ABSTRACT
Objective:
To correlate short-term (duration of mechanical ventilation and length of intensive care unit stay) and long-term (functional capacity) clinical outcomes of patients who reached nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization in the intensive care unit.
Methods:
This was a prospective observational pilot study conducted in an 18-bed intensive care unit. A total of 100 mechanically ventilated patients receiving exclusive enteral nutritional support and receiving intensive care for more than 72 hours were included. Patients who never received enteral nutrition, those with spinal cord trauma, pregnant women, organ donors and cases of family refusal were excluded. The variables studied were nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization, length of intensive care unit stay, duration of mechanical ventilation and the ability to perform activities of daily living after 12 months, assessed via telephone contact using the Lawton Activities of Daily Living Scale.
Results:
The mean duration of mechanical ventilation was 18 ± 9 days, and the mean intensive care unit length of stay was 19 ± 8 days. Only 45% of the patients received more than 70% of the target nutrition in 72 hours. There was no association between nutritional adequacy and short-term (duration of mechanical ventilation, length of stay in the intensive care unit and mortality) or long-term (functional capacity and mortality) clinical outcomes.
Conclusion:
Critically ill patients receiving caloric intake ≥ 70% in the first 72 hours of hospitalization did not present better outcomes in the short term or after 1 year.
Keywords:Activities of daily livingCritical careCritical illnessEnergy requiremententeral nutritionIntensive care unitsNutritional supportRespiration, artificialSee moreViews0

Abstract
Original ArticleAdequacy of enteral nutritional support in intensive care units does not affect the short- and long-term prognosis of mechanically ventilated patients: a pilot study
Rev Bras Ter Intensiva. 2019;31(1):34-38
DOI 10.5935/0103-507X.20190004
Views0ABSTRACT
Objective:
To correlate short-term (duration of mechanical ventilation and length of intensive care unit stay) and long-term (functional capacity) clinical outcomes of patients who reached nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization in the intensive care unit.
Methods:
This was a prospective observational pilot study conducted in an 18-bed intensive care unit. A total of 100 mechanically ventilated patients receiving exclusive enteral nutritional support and receiving intensive care for more than 72 hours were included. Patients who never received enteral nutrition, those with spinal cord trauma, pregnant women, organ donors and cases of family refusal were excluded. The variables studied were nutritional adequacy ≥ 70% of predicted in the first 72 hours of hospitalization, length of intensive care unit stay, duration of mechanical ventilation and the ability to perform activities of daily living after 12 months, assessed via telephone contact using the Lawton Activities of Daily Living Scale.
Results:
The mean duration of mechanical ventilation was 18 ± 9 days, and the mean intensive care unit length of stay was 19 ± 8 days. Only 45% of the patients received more than 70% of the target nutrition in 72 hours. There was no association between nutritional adequacy and short-term (duration of mechanical ventilation, length of stay in the intensive care unit and mortality) or long-term (functional capacity and mortality) clinical outcomes.
Conclusion:
Critically ill patients receiving caloric intake ≥ 70% in the first 72 hours of hospitalization did not present better outcomes in the short term or after 1 year.
Keywords:Activities of daily livingCritical careCritical illnessEnergy requiremententeral nutritionIntensive care unitsNutritional supportRespiration, artificialSee more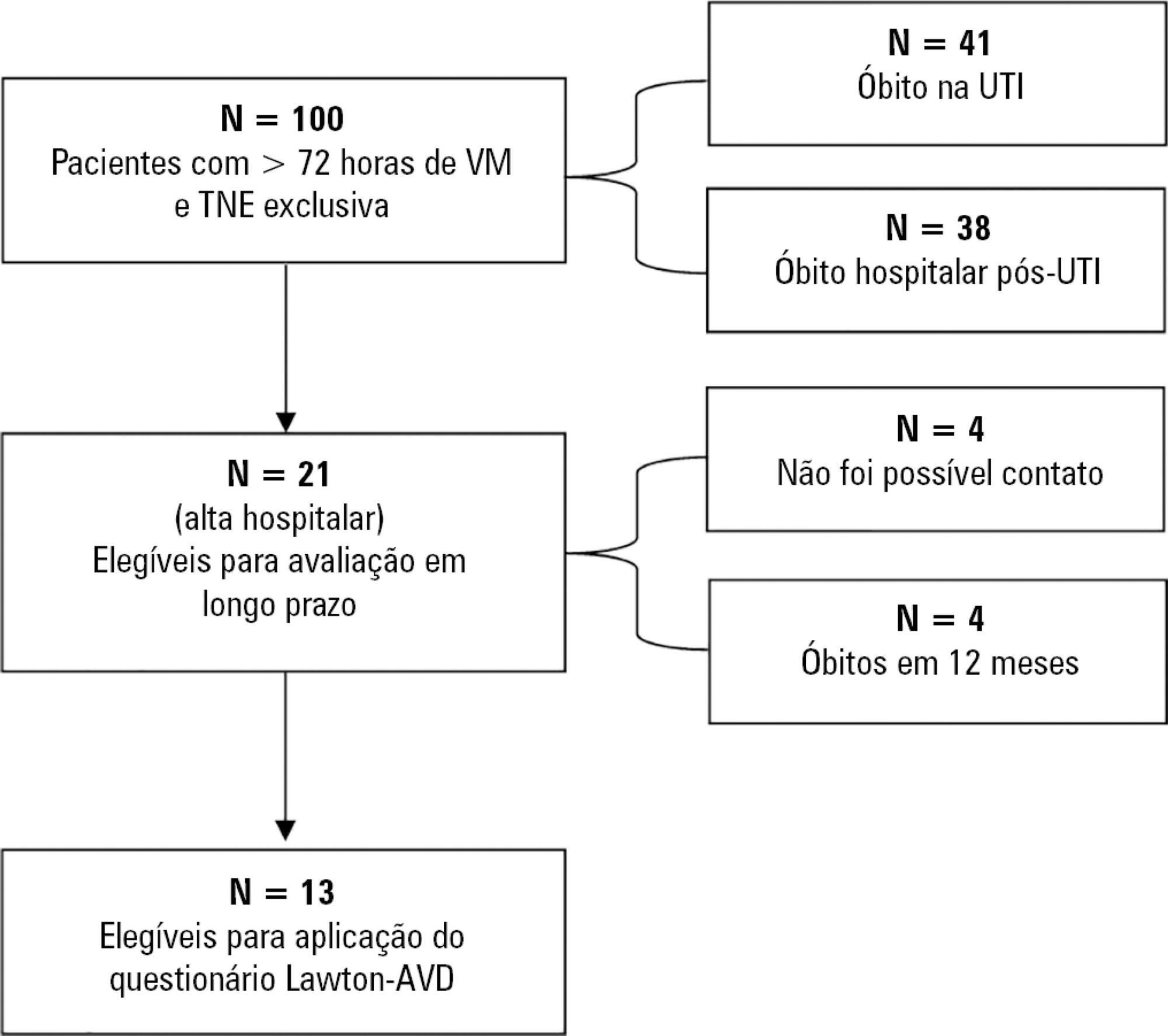
-
Original Article
Statistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
Abstract
Original ArticleStatistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
DOI 10.5935/0103-507X.20180041
Views0See moreABSTRACT
Background:
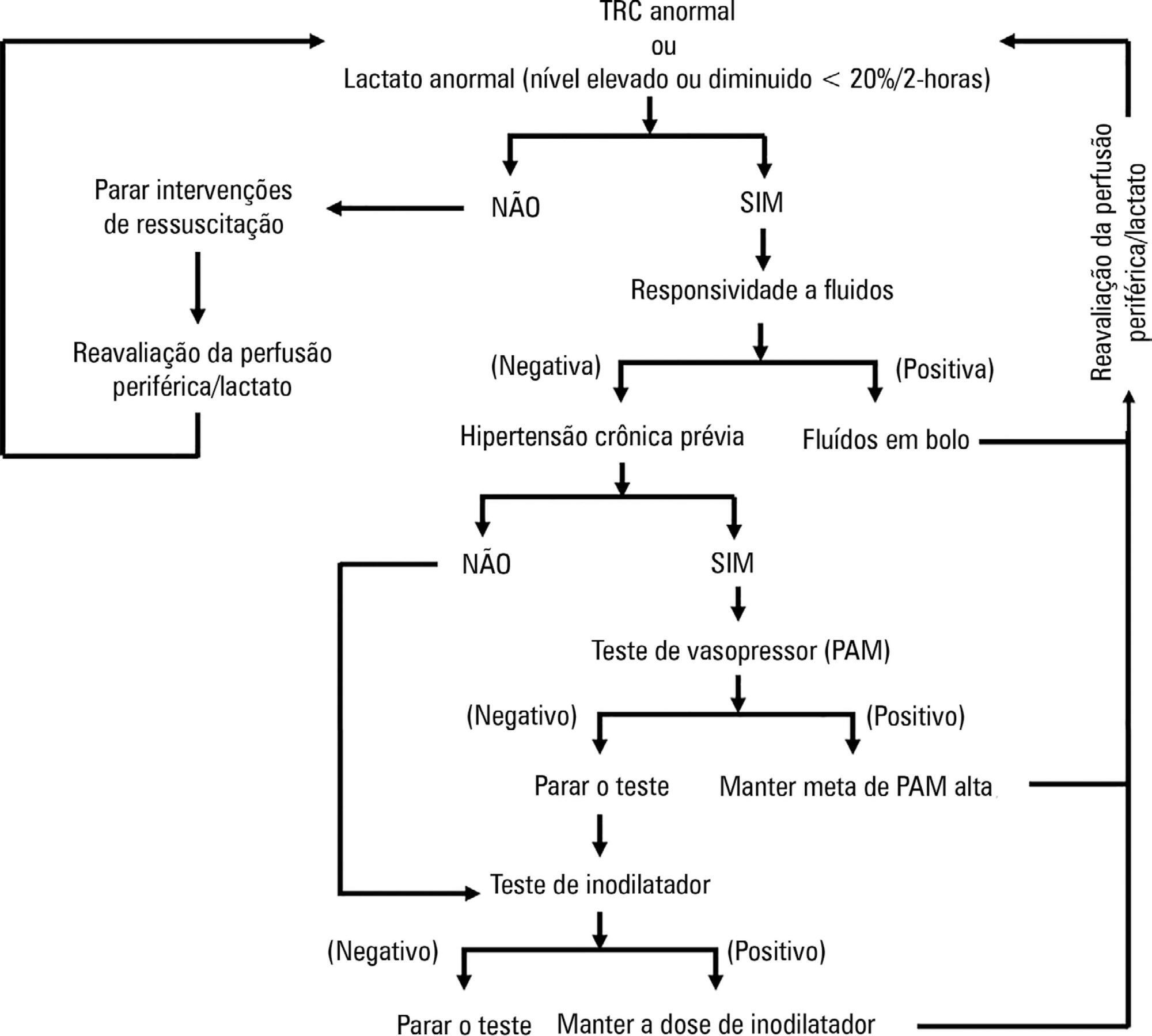
ANDROMEDA-SHOCK is an international, multicenter, randomized controlled trial comparing peripheral perfusion-targeted resuscitation to lactate-targeted resuscitation in patients with septic shock in order to test the hypothesis that resuscitation targeting peripheral perfusion will be associated with lower morbidity and mortality.
Objective:
To report the statistical analysis plan for the ANDROMEDA-SHOCK trial.
Methods:
We describe the trial design, primary and secondary objectives, patients, methods of randomization, interventions, outcomes, and sample size. We describe our planned statistical analysis for the primary, secondary and tertiary outcomes. We also describe the subgroup and sensitivity analyses. Finally, we provide details for presenting our results, including mock tables showing baseline characteristics, the evolution of hemodynamic and perfusion variables, and the effects of treatments on outcomes.
Conclusion:
According to the best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and initiating the analyses. We anticipate that this procedure will prevent analysis bias and enhance the utility of the reported results.
Views0Abstract
Original ArticleStatistical analysis plan for early goal-directed therapy using a physiological holistic view – the ANDROMEDA-SHOCK: a randomized controlled trial
Rev Bras Ter Intensiva. 2018;30(3):253-263
DOI 10.5935/0103-507X.20180041
Views0See moreABSTRACT
Background:
ANDROMEDA-SHOCK is an international, multicenter, randomized controlled trial comparing peripheral perfusion-targeted resuscitation to lactate-targeted resuscitation in patients with septic shock in order to test the hypothesis that resuscitation targeting peripheral perfusion will be associated with lower morbidity and mortality.
Objective:
To report the statistical analysis plan for the ANDROMEDA-SHOCK trial.
Methods:
We describe the trial design, primary and secondary objectives, patients, methods of randomization, interventions, outcomes, and sample size. We describe our planned statistical analysis for the primary, secondary and tertiary outcomes. We also describe the subgroup and sensitivity analyses. Finally, we provide details for presenting our results, including mock tables showing baseline characteristics, the evolution of hemodynamic and perfusion variables, and the effects of treatments on outcomes.
Conclusion:
According to the best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and initiating the analyses. We anticipate that this procedure will prevent analysis bias and enhance the utility of the reported results.
-
Original Articles
Clinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
Abstract
Original ArticlesClinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
Views0ABSTRACT
Objective:
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
Methods:
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher’s exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
Results:
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Conclusion:
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Keywords:Early ambulationMuscle weaknessPatient care teamPhysical therapy modalitiesRespiration, artificialSee moreViews0Abstract
Original ArticlesClinical attitudes and perceived barriers to early mobilization of critically ill patients in adult intensive care units
Rev Bras Ter Intensiva. 2018;30(2):187-194
DOI 10.5935/0103-507X.20180037
Views0ABSTRACT
Objective:
To investigate the knowledge of multi-professional staff members about the early mobilization of critically ill adult patients and identify attitudes and perceived barriers to its application.
Methods:
A cross-sectional study was conducted during the second semester of 2016 with physicians, nursing professionals and physical therapists from six intensive care units at two teaching hospitals. Questions were answered on a 5-point Likert scale and analyzed as proportions of professionals who agreed or disagreed with statements. The chi-square and Fisher’s exact tests were used to investigate differences in the responses according to educational/training level, previous experience with early mobilization and years of experience in intensive care units.
Results:
The questionnaire was answered by 98 out of 514 professionals (response rate: 19%). The acknowledged benefits of early mobilization were maintenance of muscle strength (53%) and shortened length of mechanical ventilation (83%). Favorable attitudes toward early mobilization included recognition that its benefits for patients under mechanical ventilation exceed the risks for both patients and staff, that early mobilization should be routinely performed via nursing and physical therapy protocols, and readiness to change the parameters of mechanical ventilation and reduce sedation to facilitate the early mobilization of patients. The main barriers mentioned were the unavailability of professionals and time to mobilize patients, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Conclusion:
The participants were aware of the benefits of early mobilization and manifested attitudes favorable to its application. However, the actual performance of early mobilization was perceived as a challenge, mainly due to the lack of professionals and time, excessive sedation, delirium, risk of musculoskeletal self-injury and excessive stress at work.
Keywords:Early ambulationMuscle weaknessPatient care teamPhysical therapy modalitiesRespiration, artificialSee more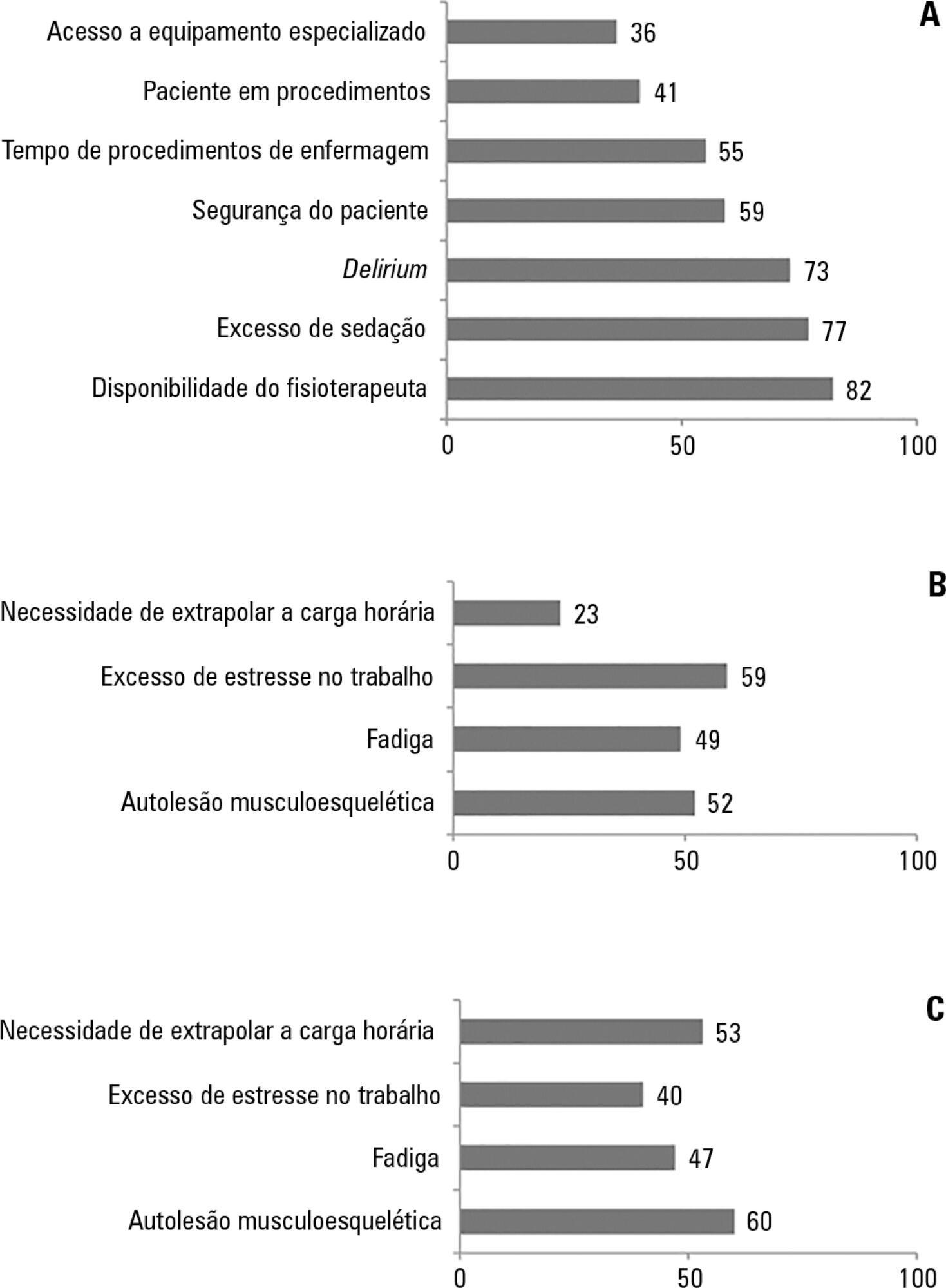
-
Review Articles
Variable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
Abstract
Review ArticlesVariable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
Views0ABSTRACT
Objective:
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Methods:
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms “variable ventilation” OR “noisy ventilation” OR “biologically variable ventilation”.
Results:
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Conclusion:
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Keywords:acute respiratory distress syndromePulmonary gas exchange/methodsPulmonary ventilation/physiologyVentilation, artificial/methodsSee moreViews0Abstract
Review ArticlesVariable mechanical ventilation
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
Views0ABSTRACT
Objective:
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Methods:
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms “variable ventilation” OR “noisy ventilation” OR “biologically variable ventilation”.
Results:
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Conclusion:
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Keywords:acute respiratory distress syndromePulmonary gas exchange/methodsPulmonary ventilation/physiologyVentilation, artificial/methodsSee more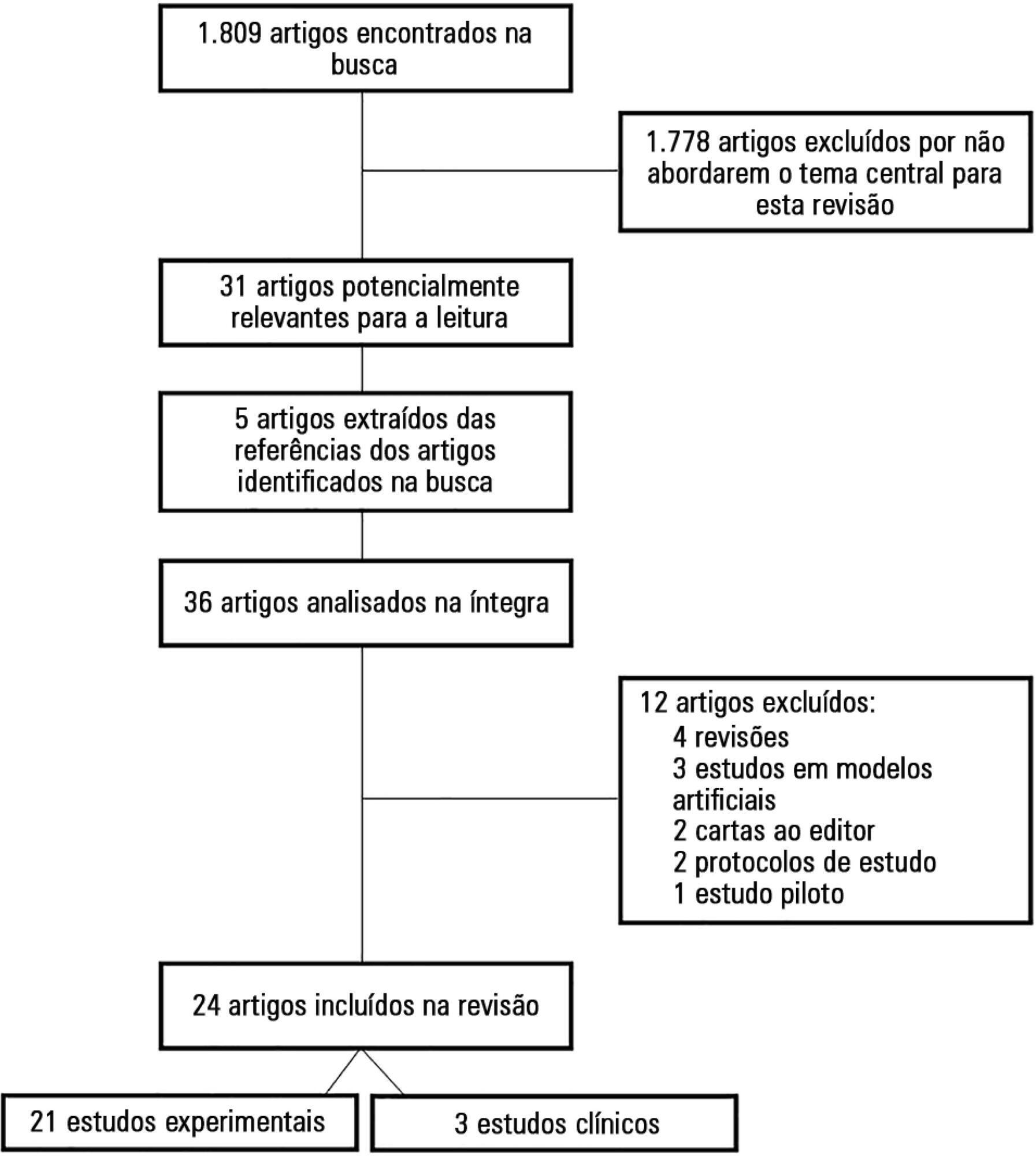
-
Brief Communication
High prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
Abstract
Brief CommunicationHigh prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
DOI 10.5935/0103-507X.20170017
Views0INTRODUCTIONBurnout syndrome involves emotional exhaustion (EE), depersonalization (DP) and reduced personal achievement (PA).(,) Burnout is associated with absenteeism, physical illnesses, emotional problems, poor work performance and negative attitudes() and may result in decreased quality of medical care.The most widely used burnout syndrome measurement tool is the Maslach Burnout Inventory (MBI).() Variations in burnout prevalence and […]See moreViews0Abstract
Brief CommunicationHigh prevalence of burnout syndrome among intensivists of the city of Porto Alegre
Rev Bras Ter Intensiva. 2017;29(1):115-120
DOI 10.5935/0103-507X.20170017
Views0INTRODUCTIONBurnout syndrome involves emotional exhaustion (EE), depersonalization (DP) and reduced personal achievement (PA).(,) Burnout is associated with absenteeism, physical illnesses, emotional problems, poor work performance and negative attitudes() and may result in decreased quality of medical care.The most widely used burnout syndrome measurement tool is the Maslach Burnout Inventory (MBI).() Variations in burnout prevalence and […]See more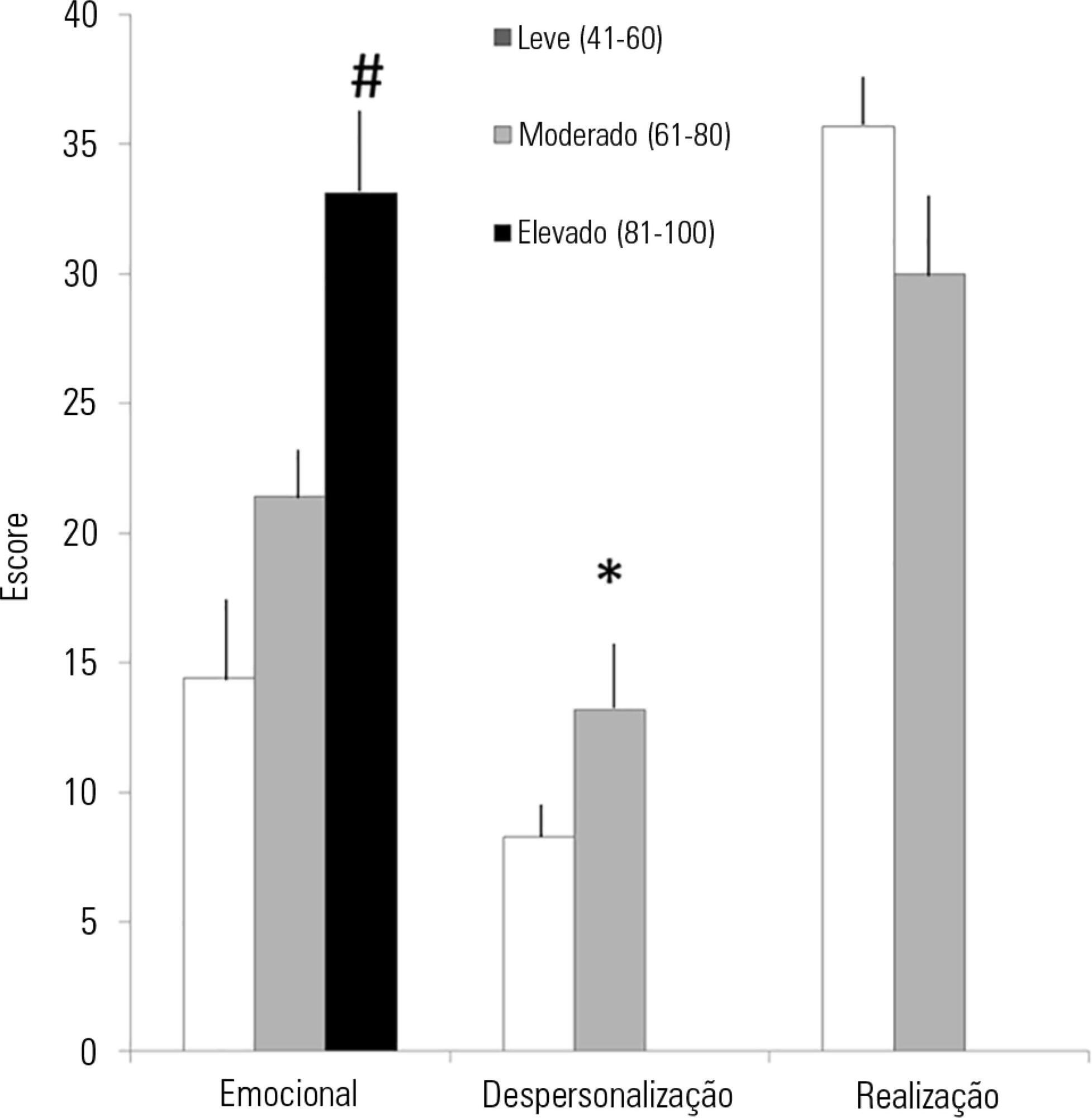
-
Original Articles
Right internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness
Rev Bras Ter Intensiva. 2015;27(3):205-211
Abstract
Original ArticlesRight internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness
Rev Bras Ter Intensiva. 2015;27(3):205-211
DOI 10.5935/0103-507X.20150042
Views0ABSTRACT
Objective:
To investigate whether the respiratory variation of the inferior vena cava diameter (∆DIVC) and right internal jugular vein diameter (∆DRIJ) are correlated in mechanically ventilated patients.
Methods:
This study was a prospective clinical analysis in an intensive care unit at a university hospital. Thirty-nine mechanically ventilated patients with hemodynamic instability were included. ∆DIVC and ∆DRIJ were assessed by echography. Vein distensibility was calculated as the ratio of (A) Dmax – Dmin/Dmin and (B) Dmax – Dmin/ mean of Dmax – Dmin and expressed as a percentage.
Results:
∆DIVC and ∆DRIJ were correlated by both methods: (A) r = 0.34, p = 0.04 and (B) r = 0.51, p = 0.001. Using 18% for ∆DIVC, indicating fluid responsiveness by method (A), 16 patients were responders and 35 measurements showed agreement (weighted Kappa = 0.80). The area under the ROC curve was 0.951 (95%CI 0.830 – 0.993; cutoff = 18.92). Using 12% for ∆DIVC, indicating fluid responsiveness by method (B), 14 patients were responders and 32 measurements showed agreement (weighted Kappa = 0.65). The area under the ROC curve was 0.903 (95%CI 0.765 – 0.973; cut-off value = 11.86).
Conclusion:
The respiratory variation of the inferior vena cava and the right internal jugular veins are correlated and showed significant agreement. Evaluation of right internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness.
Keywords:Fluid therapyHemodynamicsJugular veins/ ultrasonographyRespiration, artificialVena cava, inferior/ ultrasonographySee moreViews0Abstract
Original ArticlesRight internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness
Rev Bras Ter Intensiva. 2015;27(3):205-211
DOI 10.5935/0103-507X.20150042
Views0ABSTRACT
Objective:
To investigate whether the respiratory variation of the inferior vena cava diameter (∆DIVC) and right internal jugular vein diameter (∆DRIJ) are correlated in mechanically ventilated patients.
Methods:
This study was a prospective clinical analysis in an intensive care unit at a university hospital. Thirty-nine mechanically ventilated patients with hemodynamic instability were included. ∆DIVC and ∆DRIJ were assessed by echography. Vein distensibility was calculated as the ratio of (A) Dmax – Dmin/Dmin and (B) Dmax – Dmin/ mean of Dmax – Dmin and expressed as a percentage.
Results:
∆DIVC and ∆DRIJ were correlated by both methods: (A) r = 0.34, p = 0.04 and (B) r = 0.51, p = 0.001. Using 18% for ∆DIVC, indicating fluid responsiveness by method (A), 16 patients were responders and 35 measurements showed agreement (weighted Kappa = 0.80). The area under the ROC curve was 0.951 (95%CI 0.830 – 0.993; cutoff = 18.92). Using 12% for ∆DIVC, indicating fluid responsiveness by method (B), 14 patients were responders and 32 measurements showed agreement (weighted Kappa = 0.65). The area under the ROC curve was 0.903 (95%CI 0.765 – 0.973; cut-off value = 11.86).
Conclusion:
The respiratory variation of the inferior vena cava and the right internal jugular veins are correlated and showed significant agreement. Evaluation of right internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness.
Keywords:Fluid therapyHemodynamicsJugular veins/ ultrasonographyRespiration, artificialVena cava, inferior/ ultrasonographySee more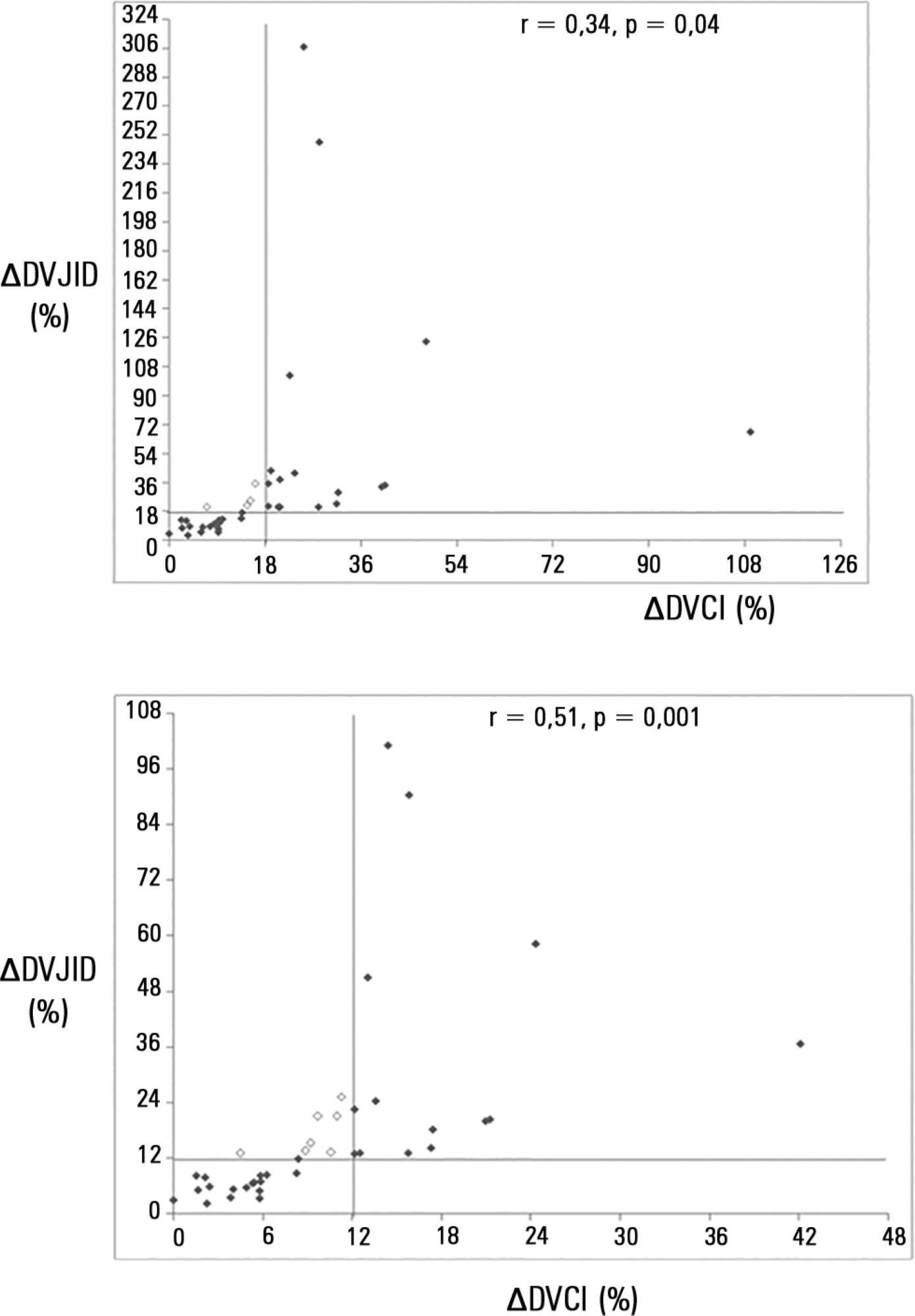
-
Original Articles – Clinical Research
Relative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
Abstract
Original Articles – Clinical ResearchRelative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
Views0OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Keywords:adrenal insufficiencyAdrenocorticotropic hormoneCritical illnessHydrocortisoneShock, septicSee moreViews0Abstract
Original Articles – Clinical ResearchRelative adrenal insufficiency as a predictor of disease severity and mortality in severe septic shock
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
Views0OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Keywords:adrenal insufficiencyAdrenocorticotropic hormoneCritical illnessHydrocortisoneShock, septicSee more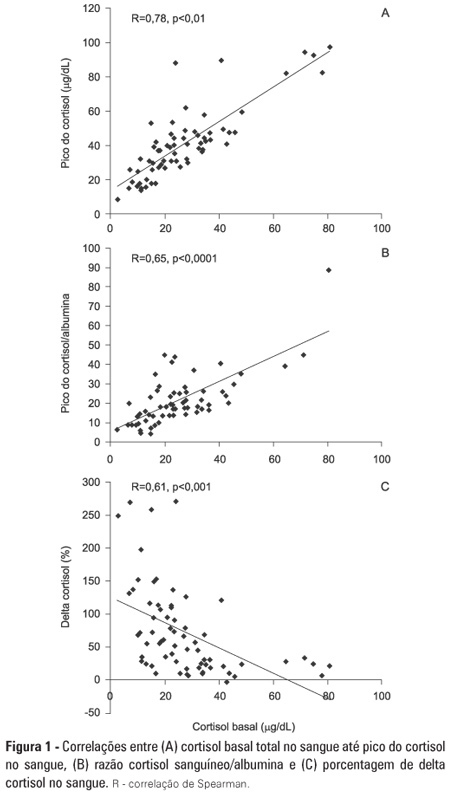
-
Special Articles
Guidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
Views0Abstract
Special ArticlesGuidelines for potential multiple organ donors (adult): part I. Overview and hemodynamic support
Rev Bras Ter Intensiva. 2011;23(3):255-268
DOI 10.1590/S0103-507X2011000300003
Views0See moreThere is a relative shortage of appropriate organs available for transplantation. The appropriate diagnosis of brain death, a suitable family approach and the maintenance of the deceased donor are fundamental in addressing this issue. The intensive care physician plays a key role in the maintenance of the deceased donor, thereby reducing losses and increasing the number of successful transplants
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis