Case Reports Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
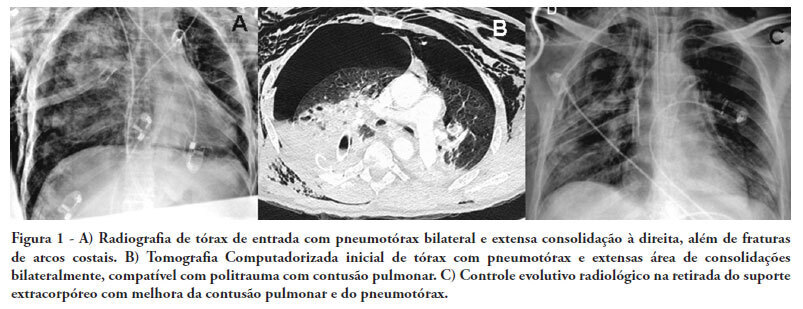
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2011;23(3):374-379
DOI 10.1590/S0103-507X2011000300017
There are few reports in the literature regarding the use of venoarterial extracorporeal membrane oxygenation (ECMO) for double-dysfunction from both heart and lung contusions in polytrauma patients. This article reports a 48-year-old patient admitted after a traffic accident. He rapidly progressed to shock with low cardiac output due to myocardial contusion and refractory hypoxemia due to pulmonary contusion, an unstable chest wall and bilateral pneumothorax. ECMO was an effective rescue procedure in this dramatic situation and was successfully discontinued on the fourth day after the trauma. The patient also developed an extensive brain infarction and eventually died on the seventh day after admission
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):310-314
DOI 10.1590/S0103-507X2010000300015
Systemic complications are frequent in subarachnoid hemorrhage patients. Among these complications, electrocardiographic abnormalities simulating ischemic cardiomyopathy may occur, possibly associated with myocardial dysfunction. This manuscript aims to report a case of subarachnoid hemorrhage associated with myocardial dysfunction and cardiogenic shock. A 45 years old woman was admitted with subarachnoid hemorrhage and coma, showing Glasgow scale = 7, Hunt-Hess = 5 and Fischer computed tomography classification = 3. On the second day, the patient underwent anterior cerebral communicant artery aneurysm embolization. The clinical evaluation revealed diffuse pulmonary infiltration, dyspnea and hypotension. Additional tests showed electrocardiographic lateral wall repolarization changes and elevated creatine kinase-MB fraction (36U/L). The cardiac index was 2.03 L/minute/m², Vascular systemic resistance was 3728 dynes.sec/cm². The non-responsiveness to volume demonstrated a cardiogenic shock pattern. The ventricular ejection fraction was 39%. The coronariography was normal, showing no obstructive lesions. Six days later the patient was removed from respiratory support and after eight days the dobutamine infusion was discontinued. The ejection fraction recovered up to 65%. Serial transcranial Doppler evaluations did not show vascular spasm. After ten days the patient was discharged from the intensive care unit. Patients with subarachnoid hemorrhage may be complicated with ventricular dysfunction and cardiogenic shock, increasing the cerebral ischemia risk. Diagnosis optimization and hemodynamic stabilization are essential to minimize the risk of cerebral vasospasm and ischemia.

Abstract
Rev Bras Ter Intensiva. 2010;22(3):305-309
DOI 10.1590/S0103-507X2010000300014
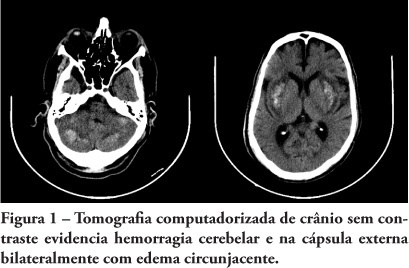
Hypernatremia is a common electrolyte disorder in people with impaired thirst control mechanism or access to water, and may lead from minimal disorders until coma. Among the hypernatremia morbidities, central nervous system hemorrhage is uncommon and poorly studied. We report a case involving a patient admitted to the intensive care unit with reduced consciousness level, hypernatremia and head computed tomography scan showing bilateral parenchyma hemorrhage. A literature review of hypernatremia hemorrhagic encephalopathy was conducted.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):305-309
DOI 10.1590/S0103-507X2010000300014
Hypernatremia is a common electrolyte disorder in people with impaired thirst control mechanism or access to water, and may lead from minimal disorders until coma. Among the hypernatremia morbidities, central nervous system hemorrhage is uncommon and poorly studied. We report a case involving a patient admitted to the intensive care unit with reduced consciousness level, hypernatremia and head computed tomography scan showing bilateral parenchyma hemorrhage. A literature review of hypernatremia hemorrhagic encephalopathy was conducted.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):104-108
DOI 10.1590/S0103-507X2009000100015
Treatment of pulmonary contusion when adequately established is very simple in most cases. Pathophysiological changes occur as a result of the effects produced by loss of chest wall integrity, accumulation of fluid in the pleural cavity, obstruction of the airways and lung dysfunction. The alveolar recruitment maneuver is the reopening of collapsed lung areas by increasing inspiratory pressure in the airway. The primary objective of this case report was to evaluate the effectiveness of the alveolar recruitment maneuver in a patient with pulmonary contusion. A 33 year old male patient, with a clinical condition of bilateral chest trauma and traumatic brain injury, evolved with reduction of the level of consciousness, acute respiratory failure, hypovolemic shock and hemoptysis. The patient underwent thoracentesis, bilateral thoracic drainage and was also submitted to invasive mechanical ventilation. After 48 hours of invasive mechanical ventilation, in accordance with protective strategy an alveolar recruitment maneuver mode, pressure-controlled ventilation, pressure controlled 10 cmH2O, respiratory rate 10 rpm, inspiratory time 3.0, positive end-expiratory pressure 30 cmH2O and FI0(2) 100%, for two minutes. After the alveolar recruitment maneuver, the patient presented clinical pulmonary improvement, but there was a variation of 185 to 322 of Pa0(2)/FiO2 (arterial partial pressure of oxygen/ fraction of inspired oxygen). He was discharged from the intensive care unit 22 days after admission. The alveolar recruitment maneuver in this patient showed significant results in the treatment of pulmonary contusion, improving blood oxygenation, preventing alveolar collapse and reversing atelectasis.

Abstract
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
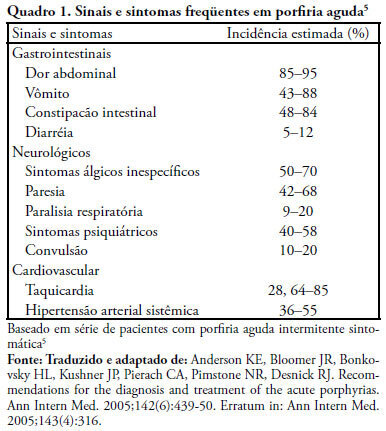
Acute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2008;20(4):429-434
DOI 10.1590/S0103-507X2008000400017
Acute intermittent porphyria is an unusual pathology with potentially severe consequences when not early detected. Among the possible causes of porphyric crises decrease of caloric intake has been described. A case of acute intermittent porphyria in the late postoperative period of a bariatric surgery performed for treatment of obesity is reported. A review of the diagnostic aspects and management of this pathology in the intensive care unit follows. A 31 year old woman was admitted in the intensive care unit three weeks after a bariatric surgery, with decreased level of consciousness and respiratory distress. The patient evolved with psychomotor agitation, mental confusion, abdominal pain and proximal tetraparesis. Diagnosis investigation disclosed severe hyponatremia (92mEq/L), hypomagnesemia, hypophosfatemia and hypocalcemia and cloudy urine without hematuria. Acute porphyria was suspected and the urine test detected high delta amino-levulinic acid and porphobilinogen. Treatment consisted of a correction of electrolyte disturbances and high carbohydrate intake. Hematin and heme arginate were not used, due to the difficulty to acquire the medication. After 8 months the patient progressed with full recovery of muscle strength and a clinical improvement. Acute intermittent porphyria has signs and symptoms common to several clinical, neurological, psychiatric and gastroenterological pathologies, which complicate diagnosis. Therefore, acute intermittent porphyria should be included in the differential diagnosis of neurological, psychiatric and gastroenterological alterations when results of all other exams are normal. Attention must be given to patients undergoing surgery mainly bariatric that, in addition to procedure stress, substantially limit the total caloric intake, potentially triggering crises. Review of literature did not disclose any report of acute intermittent porphyria crisis induced by bariatric surgery.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):313-317
DOI 10.1590/S0103-507X2008000300015
Anesthetic management of patients with severe chronic obstructive pulmonary disease is extensively discussed, due to the high rates of complications in this subtype of patients submitted to medium and high complexity surgical procedures. The objective of this study is to report use of noninvasive positive pressure mechanical ventilation - bilevel positive airway pressure - and spinal anesthesia in a patient with severe chronic obstructive pulmonary disease during total hip arthroplasty. An 81 year old, male patient with severe chronic obstructive pulmonary disease (GOLD 4) was submitted to total hip arthroplasty due to a femoral bone fracture under spinal anestesia and noninvasive positive pressure mechanical ventilation-bilevel positive airway pressure with expiratory pressure of 7 cmH2O, inspiratory pressure of 15 cmH2O and O2 flow of 3 L/min. During the procedure, the patient had one episode of bronchospasm that was promptly reverted pharmacologically with no complications in the postoperative period. The combination of less invasive anesthetic and ventilation techniques is easy to apply and may be useful in the perioperative management of patients with high anesthetic morbidity. Interaction between clinical, surgical and anesthetic teams for these cases is very important to reduce the mortality associated with extensive procedures in severe patients.

Abstract
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
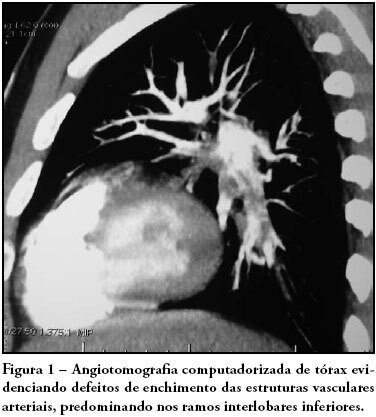
Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):318-320
DOI 10.1590/S0103-507X2008000300016
Pulmonary thromboembolism is a major cause of morbidity and mortality of patients undergoing neurosurgical procedures. The purpose of this study was to present a case of intra-arterial pulmonary thrombolysis in recent neurosurgery postoperative period. Male patient, undergoing neurosurgery, presented as a complication on the seventh day of postoperative massive pulmonary embolism with hemodynamic instability and intraarterial pulmonary thrombolysis with alteplase was indicated. Evolution was satisfactory without bleeding complications and patient was discharged. Pulmonary thromboembolism is a high morbidity and mortality condition at neurosurgical postoperative period and thrombolysis should be an alternative therapy in cases refractory to clinical treatment.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):205-209
DOI 10.1590/S0103-507X2008000200015
BACKGROUND AND OBJECTIVES: Palliative care is based on prevention and relief of suffering, identifying, assessing and treating pain and other physical, psychological, social and spiritual problems. Sudden dyspnea is frequently observed in terminal oncologic patients. In these cases, noninvasive ventilation can be an adequate option to control dyspnea promoting comfort and allowing patient interaction with their relatives. The aim of this article was to present the benefits of noninvasive ventilation in the palliative care setting. CASE REPORT: The case of a 29 year old patient, admitted in intensive care unit (ICU), after cesarean section delivery, for clinical treatment of acute respiratory failure is reported. Chest X-ray showed pulmonary mass in the right lung. After clinical and image investigation, metastatic thoracic sarcoma was diagnosed and palliative cares were introduced. The ICU interdisciplinary team chose to use noninvasive ventilation (modality CPAP + PSV) to relieve dyspnea and discomfort, as well as to allow interaction with her baby and family. CONCLUSIONS: Palliative care with noninvasive ventilation contributed to increase comfort of the patient by controlling dyspnea.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):205-209
DOI 10.1590/S0103-507X2008000200015
BACKGROUND AND OBJECTIVES: Palliative care is based on prevention and relief of suffering, identifying, assessing and treating pain and other physical, psychological, social and spiritual problems. Sudden dyspnea is frequently observed in terminal oncologic patients. In these cases, noninvasive ventilation can be an adequate option to control dyspnea promoting comfort and allowing patient interaction with their relatives. The aim of this article was to present the benefits of noninvasive ventilation in the palliative care setting. CASE REPORT: The case of a 29 year old patient, admitted in intensive care unit (ICU), after cesarean section delivery, for clinical treatment of acute respiratory failure is reported. Chest X-ray showed pulmonary mass in the right lung. After clinical and image investigation, metastatic thoracic sarcoma was diagnosed and palliative cares were introduced. The ICU interdisciplinary team chose to use noninvasive ventilation (modality CPAP + PSV) to relieve dyspnea and discomfort, as well as to allow interaction with her baby and family. CONCLUSIONS: Palliative care with noninvasive ventilation contributed to increase comfort of the patient by controlling dyspnea.
