Case Report Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(3):474-478
DOI 10.5935/0103-507X.20200078
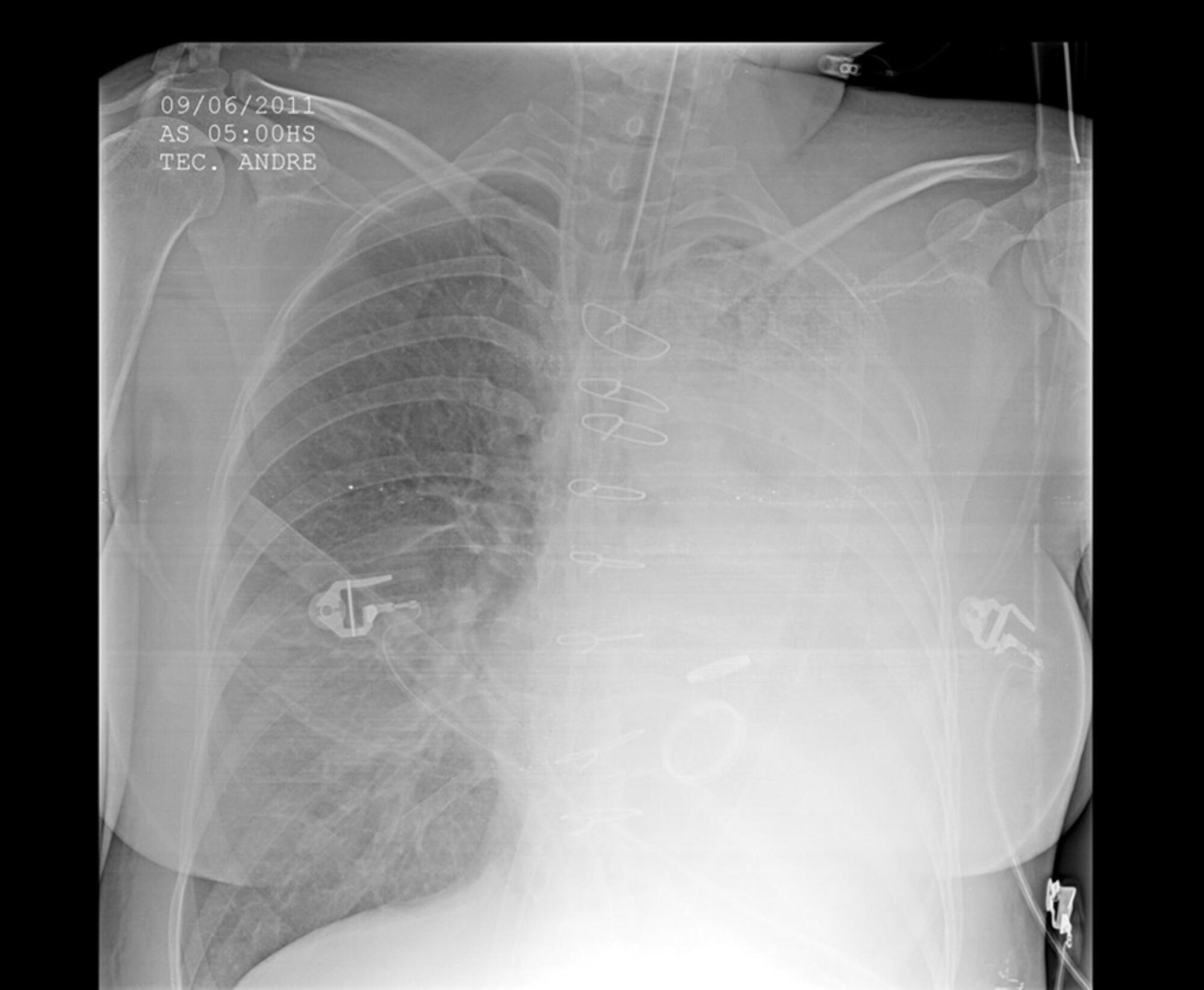
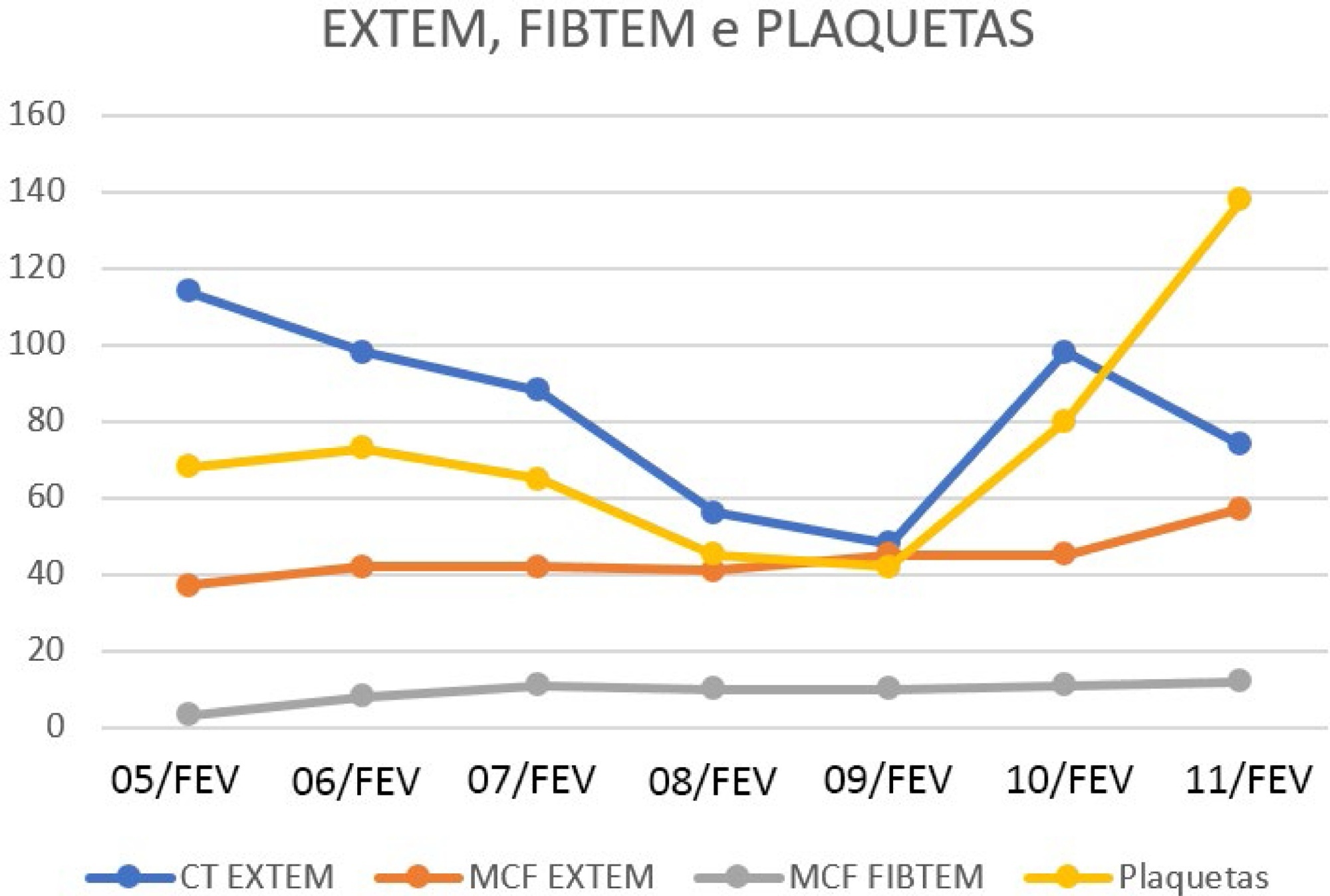
This case report a severe case of yellow fever complicated by liver failure and disseminated intravascular coagulation. Thromboelastometry was capable of identifying clotting disorders and guiding hemostatic therapy. We report the case of a 23-year-old male admitted to the Intensive Care Unit with sudden onset of fever, generalized muscle pain associated with liver failure, and disseminated intravascular coagulation. The results of conventional laboratory tests showed thrombocytopenia, whereas thromboelastometry suggested coagulopathy with slight hypofibrinogenemia, clotting factor consumption, and, consequently, an increased risk of bleeding. Unlike conventional laboratory tests, thromboelastometry identified the specific coagulation disorder and thereby guided hemostatic therapy. Both fibrinogen concentrates and vitamin K were administered, and no blood component transfusion was required, even in the presence of thrombocytopenia. Administration of hemostatic drugs, including fibrinogen concentrate and vitamin K, improved thromboelastometric parameters, correcting the complex coagulation disorder. Blood component transfusion was not performed, and there was no bleeding.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):474-478
DOI 10.5935/0103-507X.20200078
This case report a severe case of yellow fever complicated by liver failure and disseminated intravascular coagulation. Thromboelastometry was capable of identifying clotting disorders and guiding hemostatic therapy. We report the case of a 23-year-old male admitted to the Intensive Care Unit with sudden onset of fever, generalized muscle pain associated with liver failure, and disseminated intravascular coagulation. The results of conventional laboratory tests showed thrombocytopenia, whereas thromboelastometry suggested coagulopathy with slight hypofibrinogenemia, clotting factor consumption, and, consequently, an increased risk of bleeding. Unlike conventional laboratory tests, thromboelastometry identified the specific coagulation disorder and thereby guided hemostatic therapy. Both fibrinogen concentrates and vitamin K were administered, and no blood component transfusion was required, even in the presence of thrombocytopenia. Administration of hemostatic drugs, including fibrinogen concentrate and vitamin K, improved thromboelastometric parameters, correcting the complex coagulation disorder. Blood component transfusion was not performed, and there was no bleeding.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
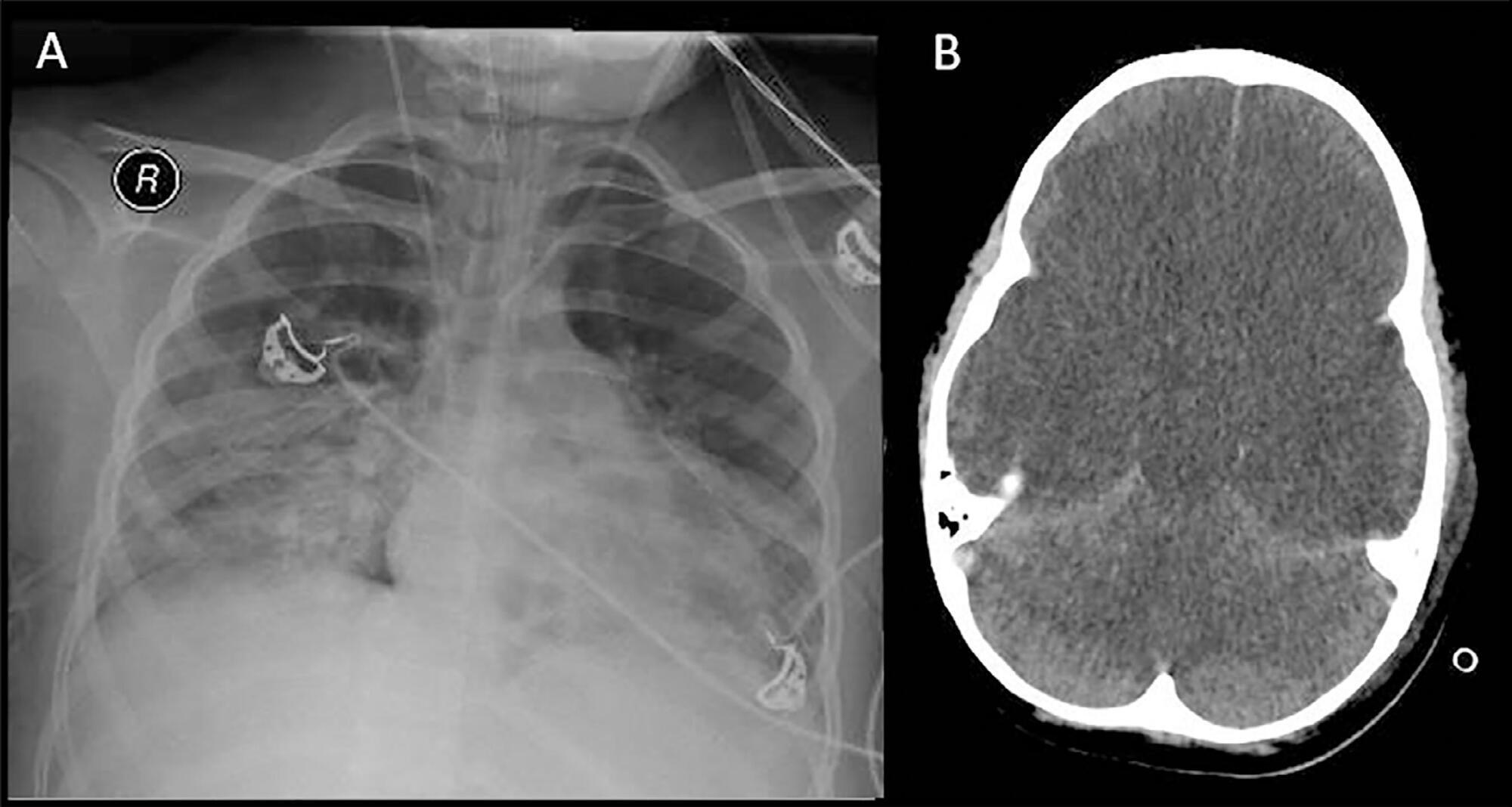
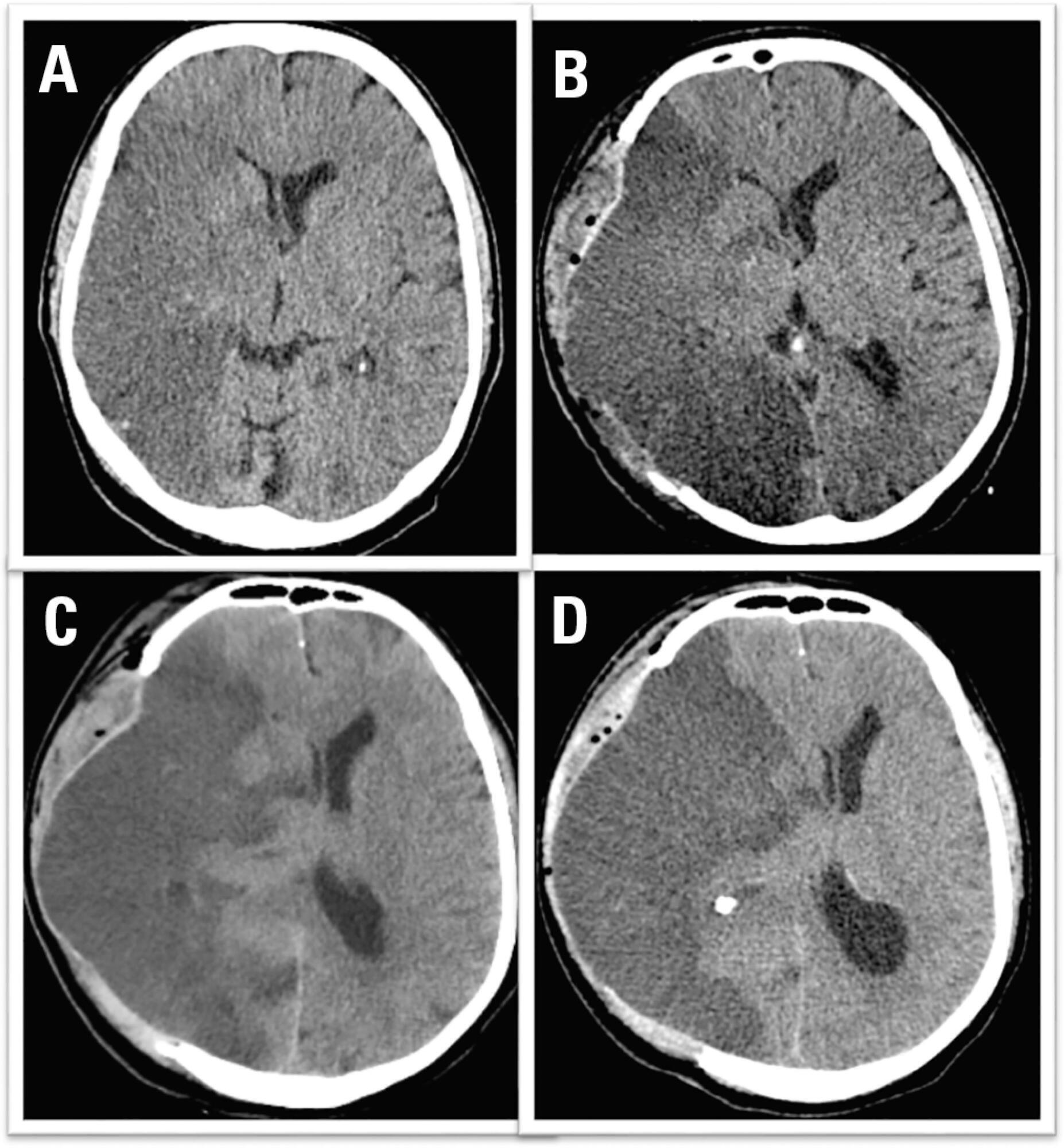
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):319-325
DOI 10.5935/0103-507X.20200032
The apnea test, which involves disconnection from the mechanical ventilator, presents risks during the determination of brain death, especially in hypoxemic patients. We describe the performance of the apnea test without disconnection from the mechanical ventilator in two patients. The first case involved an 8-year-old boy admitted with severe hypoxemia due to pneumonia. He presented with cardiorespiratory arrest, followed by unresponsive coma due to hypoxic-ischemic encephalopathy. Two clinical exams revealed the absence of brainstem reflexes, and transcranial Doppler ultrasound revealed brain circulatory arrest. Three attempts were made to perform the apnea test, which were interrupted by hypoxemia; therefore, the apnea test was performed without disconnection from the mechanical ventilator, adjusting the continuous airway pressure to 10cmH2O and the inspired fraction of oxygen to 100%. The oxygen saturation was maintained at 100% for 10 minutes. Posttest blood gas analysis results were as follows: pH, 6.90; partial pressure of oxygen, 284.0mmHg; partial pressure of carbon dioxide, 94.0mmHg; and oxygen saturation, 100%. The second case involved a 43-year-old woman admitted with subarachnoid hemorrhage (Hunt-Hess V and Fisher IV). Two clinical exams revealed unresponsive coma and absence of all brainstem reflexes. Brain scintigraphy showed no radioisotope uptake into the brain parenchyma. The first attempt at the apnea test was stopped after 5 minutes due to hypothermia (34.9°C). After rewarming, the apnea test was repeated without disconnection from the mechanical ventilator, showing maintenance of the functional residual volume with electrical bioimpedance. Posttest blood gas analysis results were as follows: pH, 7.01; partial pressure of oxygen, 232.0mmHg; partial pressure of carbon dioxide, 66.9mmHg; and oxygen saturation, 99.0%. The apnea test without disconnection from the mechanical ventilator allowed the preservation of oxygenation in both cases. The use of continuous airway pressure during the apnea test seems to be a safe alternative in order to maintain alveolar recruitment and oxygenation during brain death determination.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):143-148
DOI 10.5935/0103-507X.20200020
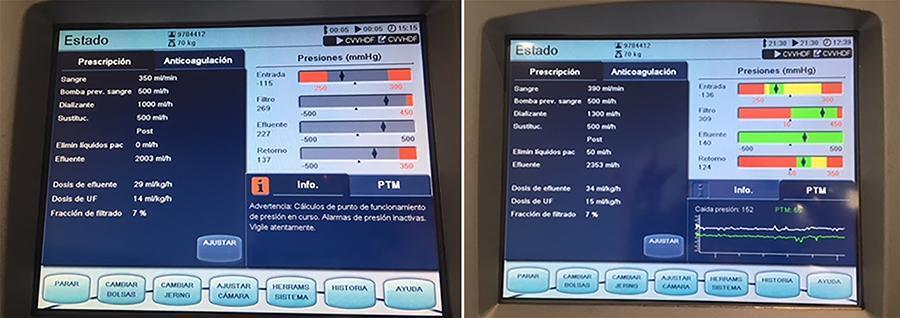
In recent years and due, in part, to technological advances, the use of extracorporeal carbon dioxide removal systems paired with the use of extracorporeal membrane oxygenation has resurfaced. However, studies are lacking that establish its indications and evidence to support its use. These systems efficiently eliminate carbon dioxide in patients with hypercapnic respiratory failure using small-bore cannula, usually double-lumen cannula with a small membrane lung surface area. Currently, we have several systems with different types of membranes and sizes. Pump-driven veno-venous systems generate fewer complications than do arteriovenous systems. Both require systemic anticoagulation. The “lung-kidney” support system, by combining a removal system with hemofiltration, simultaneously eliminates carbon dioxide and performs continuous extrarenal replacement. We describe our initial experience with a combined system for extracorporeal carbon dioxide removal-continuous extrarenal replacement in a lung transplant patients with hypercapnic respiratory failure, barotrauma and associated acute renal failure. The most important technical aspects, the effectiveness of the system for the elimination of carbon dioxide and a review of the literature are described.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):143-148
DOI 10.5935/0103-507X.20200020
In recent years and due, in part, to technological advances, the use of extracorporeal carbon dioxide removal systems paired with the use of extracorporeal membrane oxygenation has resurfaced. However, studies are lacking that establish its indications and evidence to support its use. These systems efficiently eliminate carbon dioxide in patients with hypercapnic respiratory failure using small-bore cannula, usually double-lumen cannula with a small membrane lung surface area. Currently, we have several systems with different types of membranes and sizes. Pump-driven veno-venous systems generate fewer complications than do arteriovenous systems. Both require systemic anticoagulation. The “lung-kidney” support system, by combining a removal system with hemofiltration, simultaneously eliminates carbon dioxide and performs continuous extrarenal replacement. We describe our initial experience with a combined system for extracorporeal carbon dioxide removal-continuous extrarenal replacement in a lung transplant patients with hypercapnic respiratory failure, barotrauma and associated acute renal failure. The most important technical aspects, the effectiveness of the system for the elimination of carbon dioxide and a review of the literature are described.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
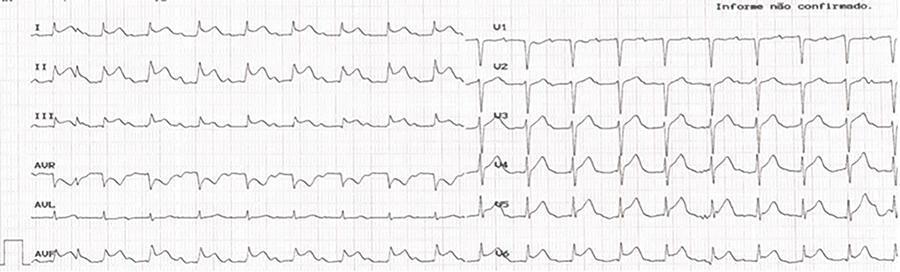
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):149-152
DOI 10.5935/0103-507X.20200021
Kounis syndrome, while an acute coronary syndrome, occurs in the context of a hypersensitivity reaction, allergies, or anaphylaxis and is subdivided into three types: coronary spasm in normal arteries, instability of plaques in atherosclerotic coronary arteries, and thrombosis of coronary stents. Herein, the case of a 73-year-old patient who, after administration of amoxicillin/clavulanic acid, went into cardiorespiratory arrest with evidence of ST-T segment elevation on electrocardiogram is reported. Coronarography revealed no obstructive lesions, and spontaneous resolution of electrocardiographic abnormalities was observed. A review of anamnesis with the family revealed a previous allergy to penicillin. The tryptase dosage was strongly positive. Kounis syndrome type 2 was diagnosed, and the clinical outcome was good.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):258-261
DOI 10.5935/0103-507X.20190040
Rituximab safety and efficacy in patients with renal impairment have not been established, nor have the effects of hemodialysis on serum rituximab level. There are only a few published case reports assessing serum rituximab level pre- and postdialysis. No data have been published regarding the usage of rituximab in patients with continuous renal replacement therapy. The authors present a case of a 59-year-old female patient who presented with paraneoplastic tetraparesis. She was admitted to the intensive care unit due to alveolar hemorrhage with respiratory failure and acute kidney injury requiring continuous renal replacement therapy. After a diagnostic workup, the diagnosis of lymphoplasmacytic lymphoma was established. Therapy with rituximab and cyclophosphamide was started. Rituximab levels were determined in serum and dialysate. No rituximab was found in the dialysate. The patient died after 2 months in the intensive care unit from nosocomial pneumonia due to multidrug-resistant Pseudomonas aeruginosa.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):262-265
DOI 10.5935/0103-507X.20190034
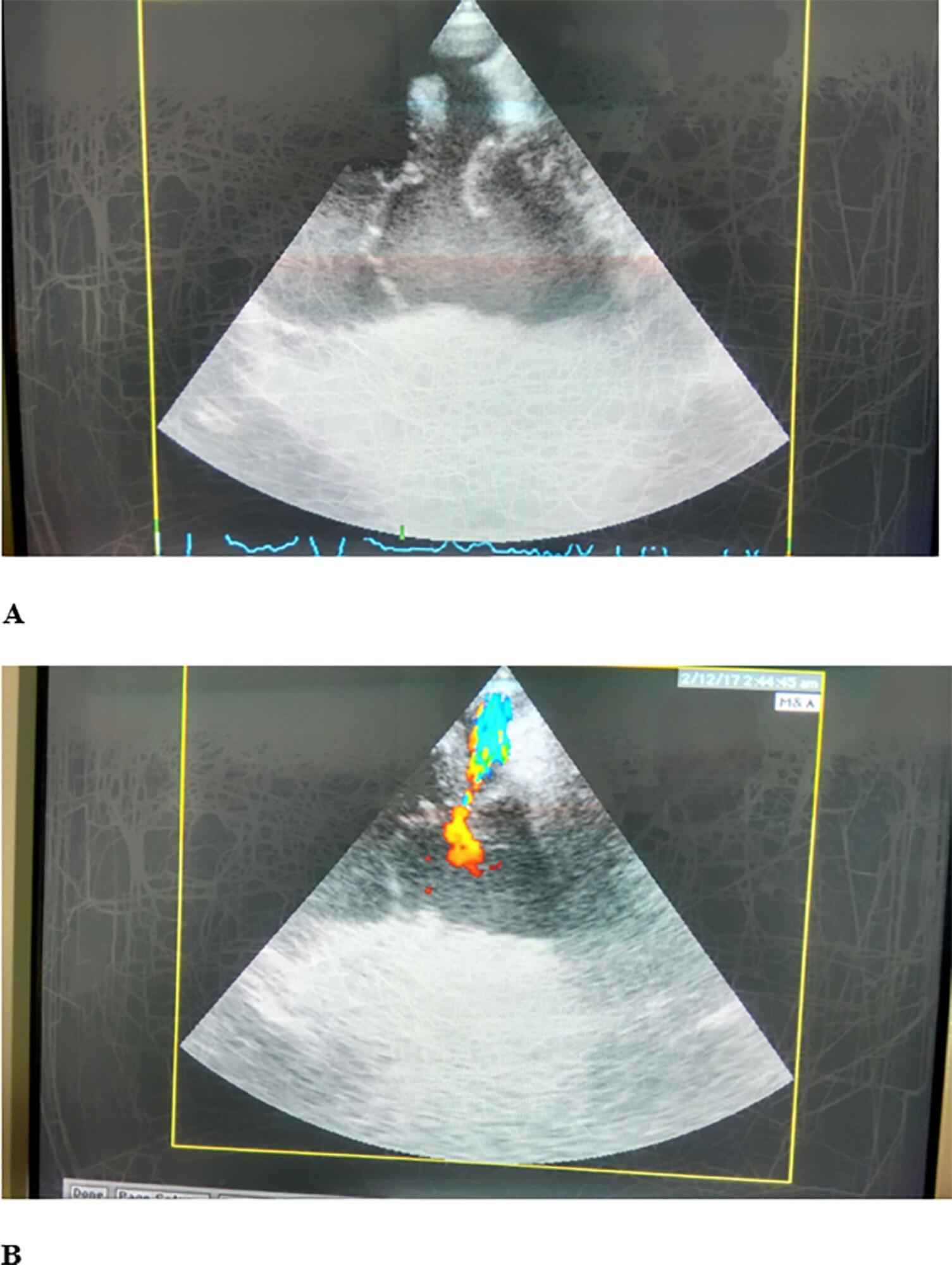
Cardiac trauma often occurs in motor vehicle accidents. A 50-year-old female driver was transported to our hospital with multiple trauma after a high-speed car accident. After admission to the intensive care unit, cardiac ultrasound examination revealed traumatic tricuspid valve papillary muscle rupture and patent foramen ovale, while Lancisi's sign was noted on physical examination. Surgical treatment was performed with valve annuloplasty and closure of the patent foramen ovale and a covert right atrial defect that was detected intraoperatively.
Abstract
Rev Bras Ter Intensiva. 2019;31(2):262-265
DOI 10.5935/0103-507X.20190034
Cardiac trauma often occurs in motor vehicle accidents. A 50-year-old female driver was transported to our hospital with multiple trauma after a high-speed car accident. After admission to the intensive care unit, cardiac ultrasound examination revealed traumatic tricuspid valve papillary muscle rupture and patent foramen ovale, while Lancisi's sign was noted on physical examination. Surgical treatment was performed with valve annuloplasty and closure of the patent foramen ovale and a covert right atrial defect that was detected intraoperatively.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Abstract
Rev Bras Ter Intensiva. 2019;31(1):106-110
DOI 10.5935/0103-507X.20190015
We report the case of a patient in whom brain death was suspected and associated with atelectasis and moderate to severe hypoxemia even though the patient was subjected to protective ventilation, a closed tracheal suction system, positive end-expiratory pressure, and recruitment maneuvers. Faced with the failure to obtain an adequate partial pressure of oxygen for the apnea test, we elected to place the patient in a prone position, use higher positive end-expiratory pressure, perform a new recruitment maneuver, and ventilate with a higher tidal volume (8mL/kg) without exceeding the plateau pressure of 30cmH2O. The apnea test was performed with the patient in a prone position, with continuous positive airway pressure coupled with a T-piece. The delay in diagnosis was 10 hours, and organ donation was not possible due to circulatory arrest. This report demonstrates the difficulties in obtaining higher levels of the partial pressure of oxygen for the apnea test. The delays in the diagnosis of brain death and in the organ donation process are discussed, as well as potential strategies to optimize the partial pressure of oxygen to perform the apnea test according to the current recommendations.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.