Case Report Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.
Abstract
Rev Bras Ter Intensiva. 2018;30(1):116-120
DOI 10.5935/0103-507X.20180002
Extracorporeal membrane oxygenation has been used to treat refractory hypoxemia in numerous clinical scenarios. The fundamental principles for the management of massive hemoptysis patients include protecting the airway and healthy lung, locating the source of bleeding and controlling the hemorrhage. We report the case of a patient with acute respiratory failure associated with massive hemoptysis secondary to lung laceration during cardiac surgery. The use of extracorporeal membrane oxygenation allowed patient survival. However, due to the great difficulty in managing pulmonary clots after hemoptysis, it was necessary to use an unusual therapy involving endobronchial infusion of a thrombolytic agent as described in rare cases in the literature.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):394-397
DOI 10.5935/0103-507X.20180056
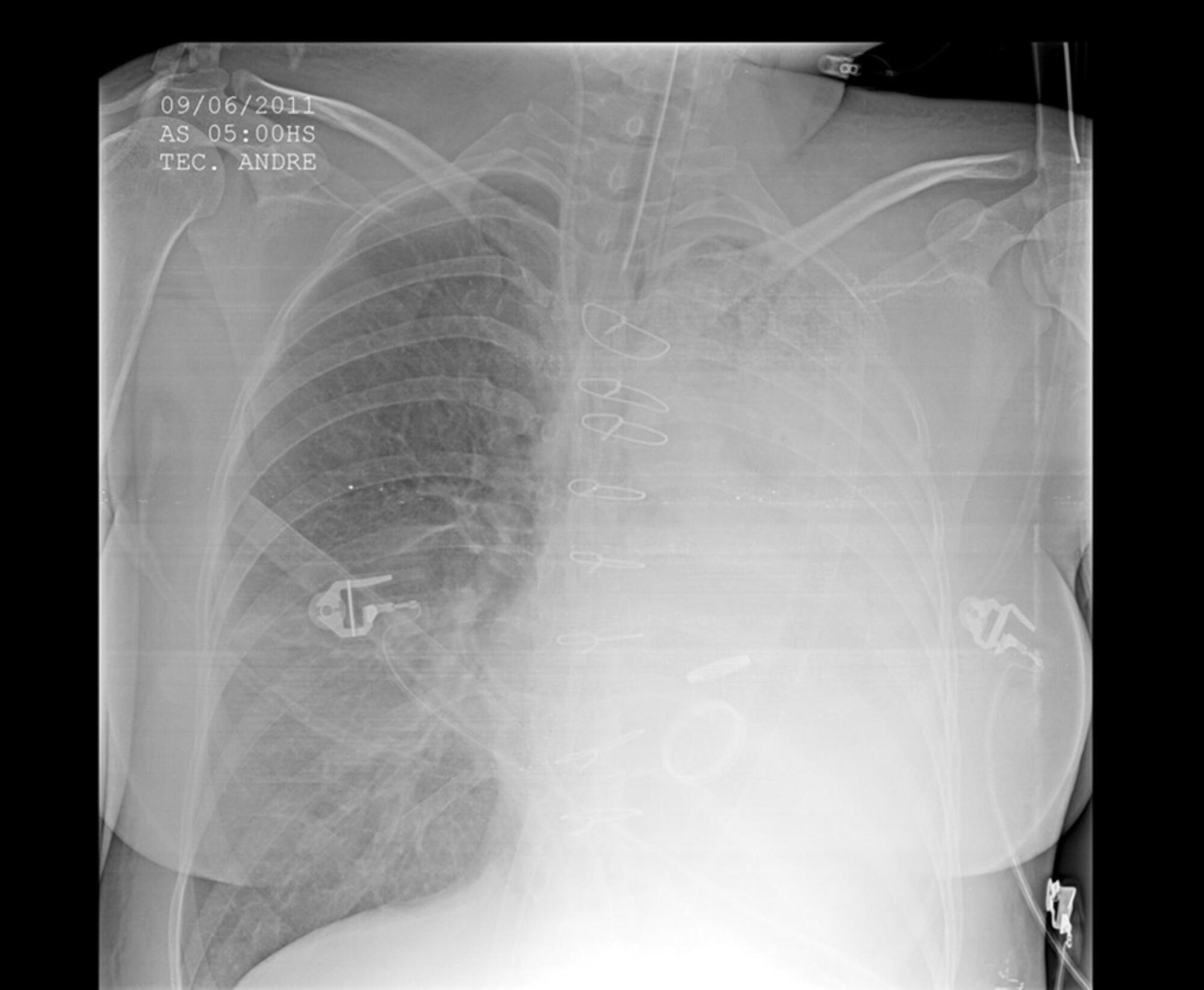
Platelet transfusion is a common practice to prevent spontaneous bleeding or bleeding due to invasive procedures. Transfusion of allogeneic blood components is associated with increased mortality and a worse clinical outcome. The clot strength is assessed by thromboelastometry and determined by the interaction between platelets and fibrinogen. The compensatory effect of high levels of fibrinogen on clot strength in patients with thrombocytopenia has been demonstrated in different clinical settings including sepsis. We report the case of a patient with severe thrombocytopenia whose thromboelastometry showed clot strength that was compensated for by the increase in plasma fibrinogen levels as an acute phase reactant of septic patients. Here, we report a case of a 62-year-old female diagnosed with bone marrow aplasia admitted in the intensive care unit with septic shock and severe thrombocytopenia. During the first 24 hours in the intensive care unit, she presented acute respiratory insufficiency and circulatory shock. The use of invasive mechanical ventilation and norepinephrine was required. Her chest X-ray showed bilateral lung injury. Thus, bronchoscopy with bronchoalveolar lavage was requested. Thromboelastometry was performed and resulted in a normal coagulable profile. Despite severe thrombocytopenia (1,000/mm3), fibrinogen levels were increased (1,050mg/dL) due to septic shock. Bronchoscopy was performed without any active or further bleeding. Here, we report the use of thromboelastometry in the diagnosis of coagulation disorders, preventing unnecessary prophylactic platelet transfusion.
Abstract
Rev Bras Ter Intensiva. 2018;30(3):394-397
DOI 10.5935/0103-507X.20180056
Platelet transfusion is a common practice to prevent spontaneous bleeding or bleeding due to invasive procedures. Transfusion of allogeneic blood components is associated with increased mortality and a worse clinical outcome. The clot strength is assessed by thromboelastometry and determined by the interaction between platelets and fibrinogen. The compensatory effect of high levels of fibrinogen on clot strength in patients with thrombocytopenia has been demonstrated in different clinical settings including sepsis. We report the case of a patient with severe thrombocytopenia whose thromboelastometry showed clot strength that was compensated for by the increase in plasma fibrinogen levels as an acute phase reactant of septic patients. Here, we report a case of a 62-year-old female diagnosed with bone marrow aplasia admitted in the intensive care unit with septic shock and severe thrombocytopenia. During the first 24 hours in the intensive care unit, she presented acute respiratory insufficiency and circulatory shock. The use of invasive mechanical ventilation and norepinephrine was required. Her chest X-ray showed bilateral lung injury. Thus, bronchoscopy with bronchoalveolar lavage was requested. Thromboelastometry was performed and resulted in a normal coagulable profile. Despite severe thrombocytopenia (1,000/mm3), fibrinogen levels were increased (1,050mg/dL) due to septic shock. Bronchoscopy was performed without any active or further bleeding. Here, we report the use of thromboelastometry in the diagnosis of coagulation disorders, preventing unnecessary prophylactic platelet transfusion.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):253-258
DOI 10.5935/0103-507X.20170035
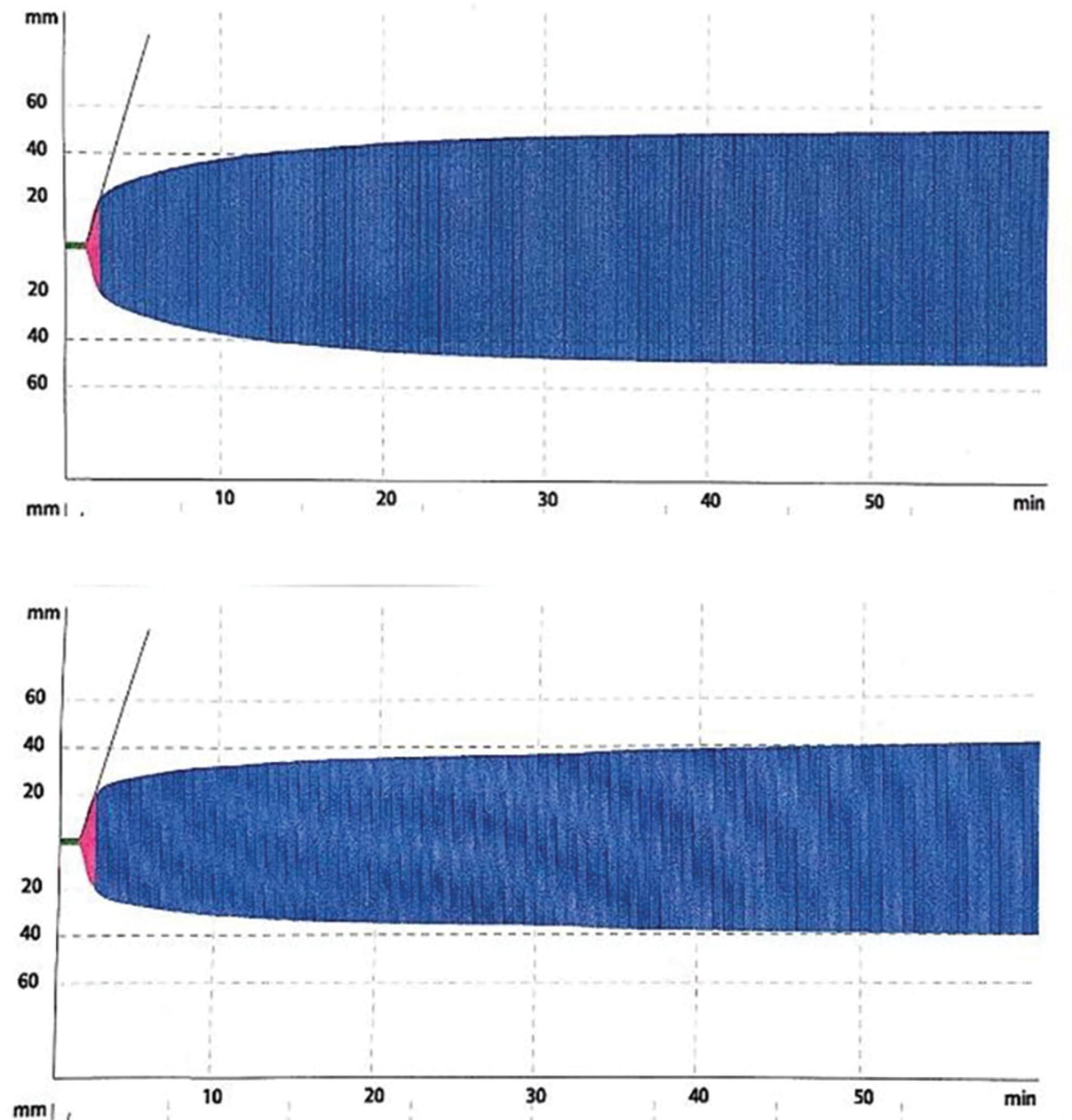
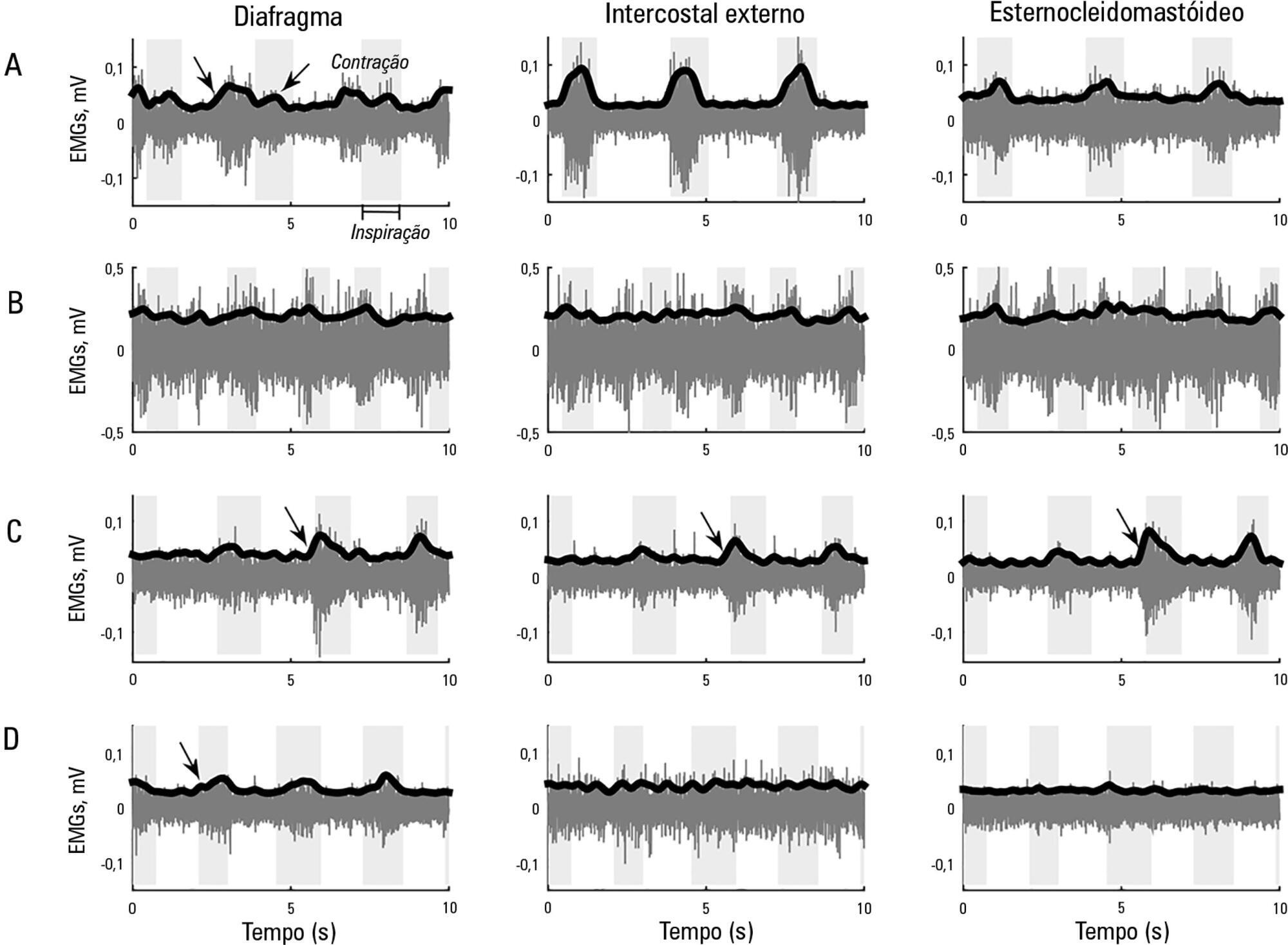
This study aimed to explore the usefulness of measuring respiratory muscle activity in mechanically ventilated patients suffering from acute organophosphate poisoning, with a view towards providing complementary information to determine the best time to suspend ventilatory support. Surface electromyography in respiratory muscles (diaphragm, external intercostal and sternocleidomastoid muscles) was recorded in a young man affected by self-poisoning with an unknown amount of parathion to determine the muscle activity level during several weaning attempts from mechanical ventilation. The energy distribution of each surface electromyography signal frequency, the synchronization between machine and patient and between muscles, acetylcholinesterase enzyme activity, and work of breathing and rapid shallow breathing indices were calculated in each weaning attempt. The work of breathing and rapid shallow breathing indices were not correlated with the failure/success of the weaning attempt. The diaphragm gradually increased its engagement with ventilation, achieving a maximal response that correlated with successful weaning and maximal acetylcholinesterase enzyme activity; in contrast, the activity of accessory respiratory muscles showed an opposite trend.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):253-258
DOI 10.5935/0103-507X.20170035
This study aimed to explore the usefulness of measuring respiratory muscle activity in mechanically ventilated patients suffering from acute organophosphate poisoning, with a view towards providing complementary information to determine the best time to suspend ventilatory support. Surface electromyography in respiratory muscles (diaphragm, external intercostal and sternocleidomastoid muscles) was recorded in a young man affected by self-poisoning with an unknown amount of parathion to determine the muscle activity level during several weaning attempts from mechanical ventilation. The energy distribution of each surface electromyography signal frequency, the synchronization between machine and patient and between muscles, acetylcholinesterase enzyme activity, and work of breathing and rapid shallow breathing indices were calculated in each weaning attempt. The work of breathing and rapid shallow breathing indices were not correlated with the failure/success of the weaning attempt. The diaphragm gradually increased its engagement with ventilation, achieving a maximal response that correlated with successful weaning and maximal acetylcholinesterase enzyme activity; in contrast, the activity of accessory respiratory muscles showed an opposite trend.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):195-198
DOI 10.5935/0103-507X.20160033
Ralstonia pickettii is a low-virulence gram-negative bacillus that may be associated with infections related to health care and may cause bacteremia. Ralstonia pickettii bacteremia is uncommon but is related to the contamination of medical products, mainly in immunodepressed patients. We present two cases of patients on chronic hemodialysis with Ralstonia pickettii bacteremia linked to contamination of the dialysis water. Similar cases have been published with links to intravenous fluid administration, medication ampules, and the use of extracorporeal oxygenation membranes, among other factors. The detection of Ralstonia pickettii bacteremia should provoke suspicion and a search for contaminated medical products, fluids, and/or medications.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):195-198
DOI 10.5935/0103-507X.20160033
Ralstonia pickettii is a low-virulence gram-negative bacillus that may be associated with infections related to health care and may cause bacteremia. Ralstonia pickettii bacteremia is uncommon but is related to the contamination of medical products, mainly in immunodepressed patients. We present two cases of patients on chronic hemodialysis with Ralstonia pickettii bacteremia linked to contamination of the dialysis water. Similar cases have been published with links to intravenous fluid administration, medication ampules, and the use of extracorporeal oxygenation membranes, among other factors. The detection of Ralstonia pickettii bacteremia should provoke suspicion and a search for contaminated medical products, fluids, and/or medications.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
Abstract
Rev Bras Ter Intensiva. 2016;28(2):190-194
DOI 10.5935/0103-507X.20160032
Hantavirus cardiopulmonary syndrome has a high mortality rate, and early connection to extracorporeal membrane oxygenation has been suggested to improve outcomes. We report the case of a patient with demonstrated Hantavirus cardiopulmonary syndrome and refractory shock who fulfilled the criteria for extracorporeal membrane oxygenation and responded successfully to high volume continuous hemofiltration. The implementation of high volume continuous hemofiltration along with protective ventilation reversed the shock within a few hours and may have prompted recovery. In patients with Hantavirus cardiopulmonary syndrome, a short course of high volume continuous hemofiltration may help differentiate patients who can be treated with conventional intensive care unit management from those who will require more complex therapies, such as extracorporeal membrane oxygenation.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):77-81
DOI 10.5935/0103-507X.20150013
Rhabdomyolysis is characterized by the destruction of skeletal muscle tissue, and its main causes are trauma, toxic substances and electrolyte disturbances. Among the latter is hyponatremia-induced rhabdomyolysis, a rare condition that occurs mainly in patients with psychogenic polydipsia. Psycogenic polydipsia mostly affects patients with schizophrenia, coursing with hyponatremia in almost 25% of the cases. It is also in this context that rhabdomyolysis secondary to hyponatremia occurs most often. In this article, the case of a 49-year-old male with a history of schizophrenia, medicated with clozapine, and brought to the emergency room in a state of coma and seizures is described. Severe hypoosmolar hyponatremia with cerebral edema was found on a computed tomography examination, and a subsequent diagnosis of hyponatremia secondary to psychogenic polydipsia was made. Hyponatremia correction therapy was started, and the patient was admitted to the intensive care unit. After the hyponatremia correction, the patient presented with analytical worsening, showing marked rhabdomyolysis with a creatine phosphokinase level of 44.058UI/L on day 3 of hospitalization. The condition showed a subsequent progressive improvement with therapy, with no occurrence of kidney damage. This case stresses the need for monitoring rhabdomyolysis markers in severe hyponatremia, illustrating the condition of rhabdomyolysis secondary to hyponatremia induced by psychogenic polydipsia, which should be considered in patients undergoing treatment with neuroleptics.
Abstract
Rev Bras Ter Intensiva. 2015;27(1):77-81
DOI 10.5935/0103-507X.20150013
Rhabdomyolysis is characterized by the destruction of skeletal muscle tissue, and its main causes are trauma, toxic substances and electrolyte disturbances. Among the latter is hyponatremia-induced rhabdomyolysis, a rare condition that occurs mainly in patients with psychogenic polydipsia. Psycogenic polydipsia mostly affects patients with schizophrenia, coursing with hyponatremia in almost 25% of the cases. It is also in this context that rhabdomyolysis secondary to hyponatremia occurs most often. In this article, the case of a 49-year-old male with a history of schizophrenia, medicated with clozapine, and brought to the emergency room in a state of coma and seizures is described. Severe hypoosmolar hyponatremia with cerebral edema was found on a computed tomography examination, and a subsequent diagnosis of hyponatremia secondary to psychogenic polydipsia was made. Hyponatremia correction therapy was started, and the patient was admitted to the intensive care unit. After the hyponatremia correction, the patient presented with analytical worsening, showing marked rhabdomyolysis with a creatine phosphokinase level of 44.058UI/L on day 3 of hospitalization. The condition showed a subsequent progressive improvement with therapy, with no occurrence of kidney damage. This case stresses the need for monitoring rhabdomyolysis markers in severe hyponatremia, illustrating the condition of rhabdomyolysis secondary to hyponatremia induced by psychogenic polydipsia, which should be considered in patients undergoing treatment with neuroleptics.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
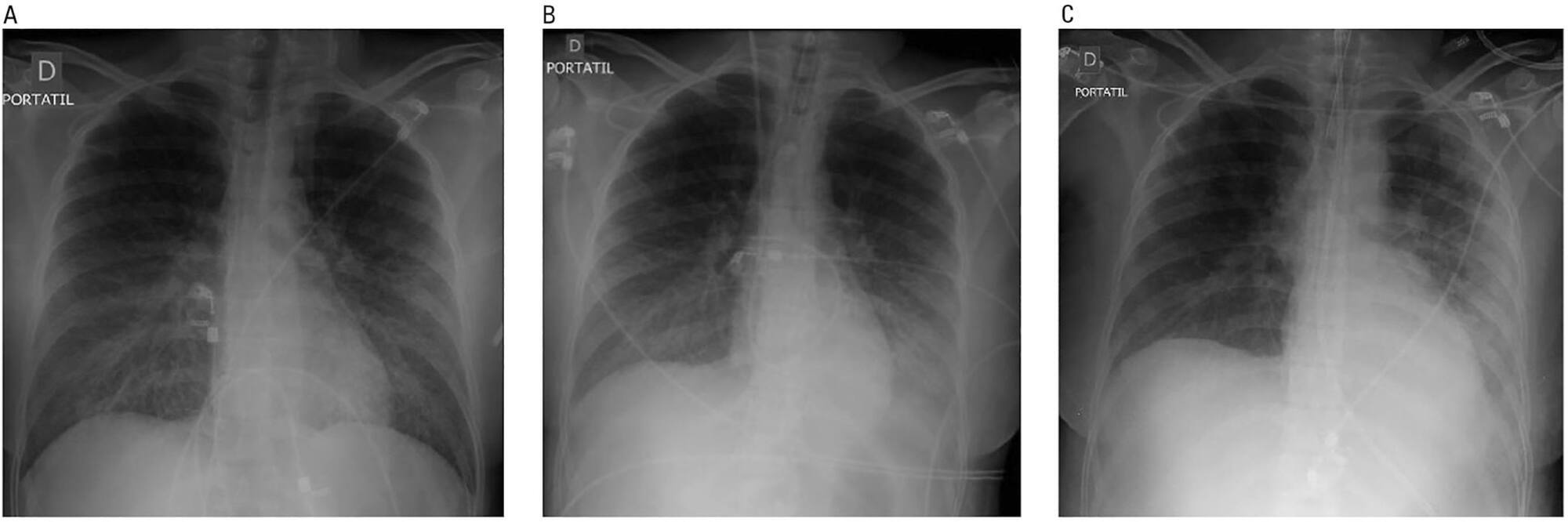
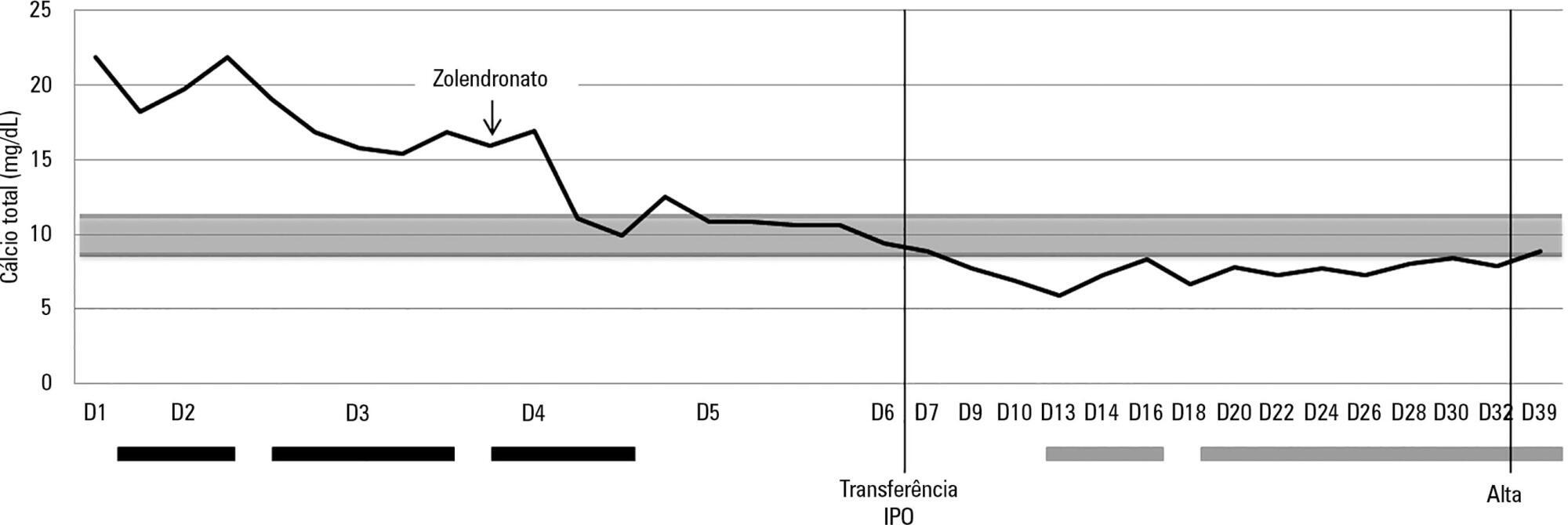
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):402-405
DOI 10.5935/0103-507X.20150067
Hypercalcemia is a rare metabolic disorder in children and is potentially fatal. It has a wide differential diagnosis, including cancer. Here, we report the case of a previously healthy 3-year-old who was admitted to the emergency room with fatigue, hyporeactivity, fever and limping gait that had evolved over 5 days and that was progressively worsening. On examination the patient was unconscious (Glasgow coma score: 8). Laboratory tests indicated severe hypercalcemia (total calcium 21.39mg/dL, ionized calcium 2.93mmol/L) and microcytic anemia. Hyperhydration was initiated, and the child was transferred to the pediatric intensive care unit. Continuous venovenous hemodiafiltration with calcium-free solution was instituted, which brought progressive normalization of serum calcium and an improved state of consciousness. Zoledronate was administered, and metabolic and infectious causes and poisoning were excluded. The bone marrow smear revealed a diagnosis of acute lymphoblastic leukemia. Hypercalcemia associated with malignancy in children is rare and occurs as a form of cancer presentation or recurrence. Continuous venovenous hemodiafiltration should be considered in situations where there is imminent risk to life.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
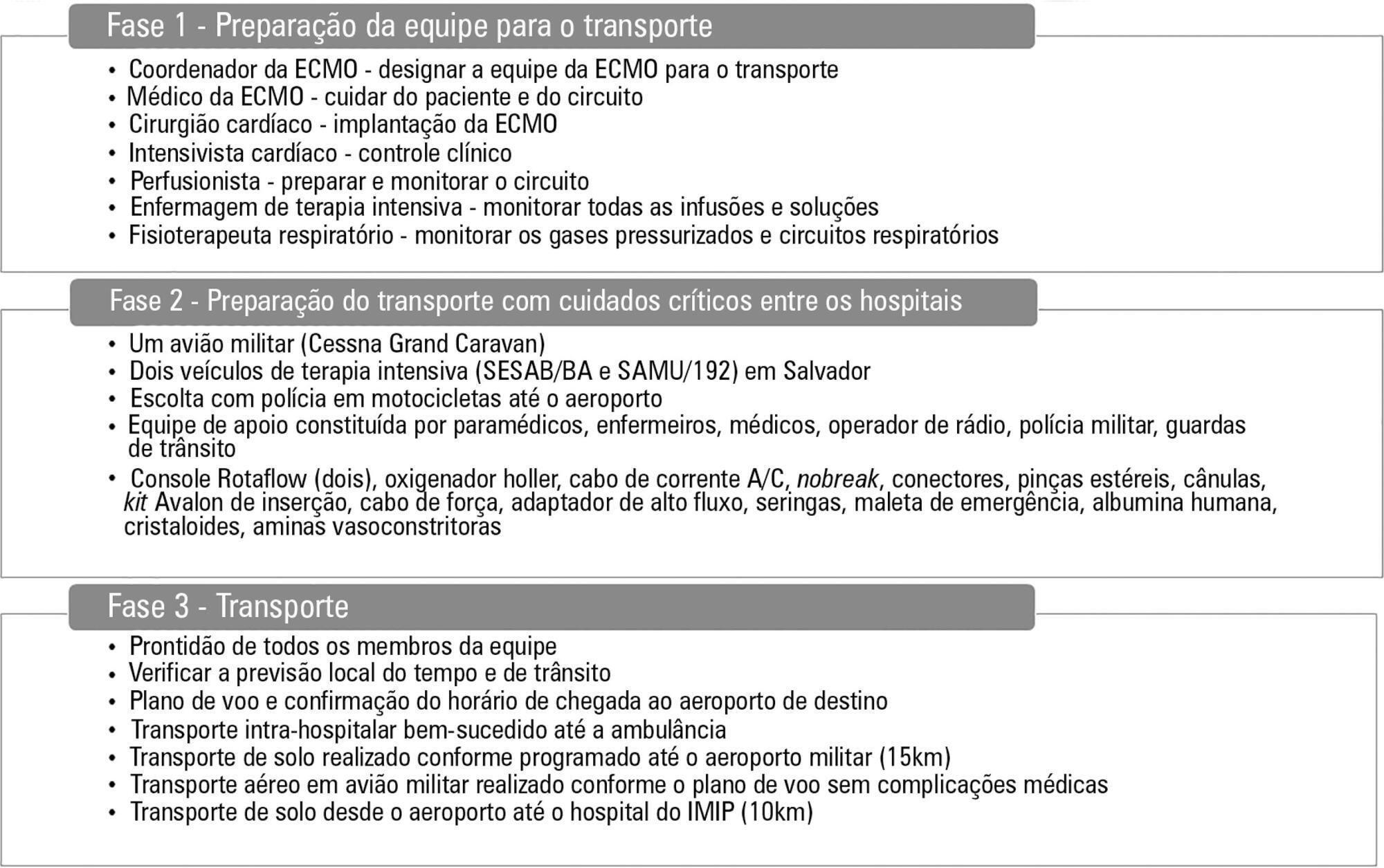
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.
Abstract
Rev Bras Ter Intensiva. 2015;27(4):397-401
DOI 10.5935/0103-507X.20150066
A 17-year-old Brazilian male presented with progressive dyspnea for 15 days, worsening in the last 24 hours, and was admitted in respiratory failure and cardiogenic shock, with multiple organ dysfunctions. Echocardiography showed a left ventricle ejection fraction of 11%, severe diffuse hypokinesia, and a systolic pulmonary artery pressure of 50mmHg, resulting in the need for hemodynamic support with dobutamine (20mcg/kg/min) and noradrenaline (1.7mcg/kg/min). After 48 hours with no clinical or hemodynamic improvement, an extracorporeal membrane oxygenation was implanted. The patient presented with hemodynamic, systemic perfusion and renal and liver function improvements; however, his cardiac function did not recover after 72 hours, and he was transfer to another hospital. Air transport was conducted from Salvador to Recife in Brazil. A heart transplant was performed with rapid recovery of both liver and kidney functions, as well as good graft function. Histopathology of the explanted heart showed chronic active myocarditis and amastigotes of Trypanosoma cruzi. The estimated global prevalence of T. cruzi infections declined from 18 million in 1991, when the first regional control initiative began, to 5.7 million in 2010. Myocarditis is an inflammatory disease due to infectious or non-infectious conditions. Clinical manifestation is variable, ranging from subclinical presentation to refractory heart failure and cardiogenic shock. Several reports suggest that the use of extracorporeal membrane oxygenation in patients presenting with severe refractory myocarditis is a potential bridging therapy to heart transplant when there is no spontaneous recovery of ventricular function. In a 6-month follow-up outpatient consult, the patient presented well and was asymptomatic.