Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2010;22(4):333-338
DOI 10.1590/S0103-507X2010000400004
OBJECTIVES: To describe the clinical features and outcomes of patients admitted with influenza A (H1N1) infection in two private hospitals' intensive care units in São Paulo, Brazil, during the 2009 pandemics. METHODS: A retrospective cohort study was conducted to evaluate demographic data, initial clinical presentation, prognostic scores [Simplified Acute Physiology Score (SAPS) 3 and Sequential Organ Failure Assessment (SOFA)], comorbidities, outcomes and treatment of patients with confirmed pandemic influenza diagnosis from July to September 2009. RESULTS: 22 patients were admitted. Median age was 30 (25-43.5) years. Median SAPS 3 and SOFA were 42 (37-49) and 2 (1-3.5), respectively. Comorbidities were common (45.4%), especially obesity (22.7%). Two (9.1%) patients were pregnant. Five (22.7%) patients required invasive mechanical ventilation, with high positive end expiratory pressures (median of 16 cmH2O, interquartile range 10-25cmH2O). There was a 50% incidence of non-invasive ventilation failure. Most (77.2%) of patients were treated with oseltamivir. Hospital mortality was 4.5%. Initial SAPS 3, SOFA and PaO2/FiO2 ratio were associated with mechanical ventilation requirement (p<0.01). CONCLUSIONS: Pandemic influenza infection mainly affected young and obese patients. In this study, patients were less severe than those previously described, what explains our low mortality and mechanical ventilation needs. However, high positive end expiratory pressures were required for mechanically ventilated patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):333-338
DOI 10.1590/S0103-507X2010000400004
OBJECTIVES: To describe the clinical features and outcomes of patients admitted with influenza A (H1N1) infection in two private hospitals' intensive care units in São Paulo, Brazil, during the 2009 pandemics. METHODS: A retrospective cohort study was conducted to evaluate demographic data, initial clinical presentation, prognostic scores [Simplified Acute Physiology Score (SAPS) 3 and Sequential Organ Failure Assessment (SOFA)], comorbidities, outcomes and treatment of patients with confirmed pandemic influenza diagnosis from July to September 2009. RESULTS: 22 patients were admitted. Median age was 30 (25-43.5) years. Median SAPS 3 and SOFA were 42 (37-49) and 2 (1-3.5), respectively. Comorbidities were common (45.4%), especially obesity (22.7%). Two (9.1%) patients were pregnant. Five (22.7%) patients required invasive mechanical ventilation, with high positive end expiratory pressures (median of 16 cmH2O, interquartile range 10-25cmH2O). There was a 50% incidence of non-invasive ventilation failure. Most (77.2%) of patients were treated with oseltamivir. Hospital mortality was 4.5%. Initial SAPS 3, SOFA and PaO2/FiO2 ratio were associated with mechanical ventilation requirement (p<0.01). CONCLUSIONS: Pandemic influenza infection mainly affected young and obese patients. In this study, patients were less severe than those previously described, what explains our low mortality and mechanical ventilation needs. However, high positive end expiratory pressures were required for mechanically ventilated patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):339-345
DOI 10.1590/S0103-507X2010000400005
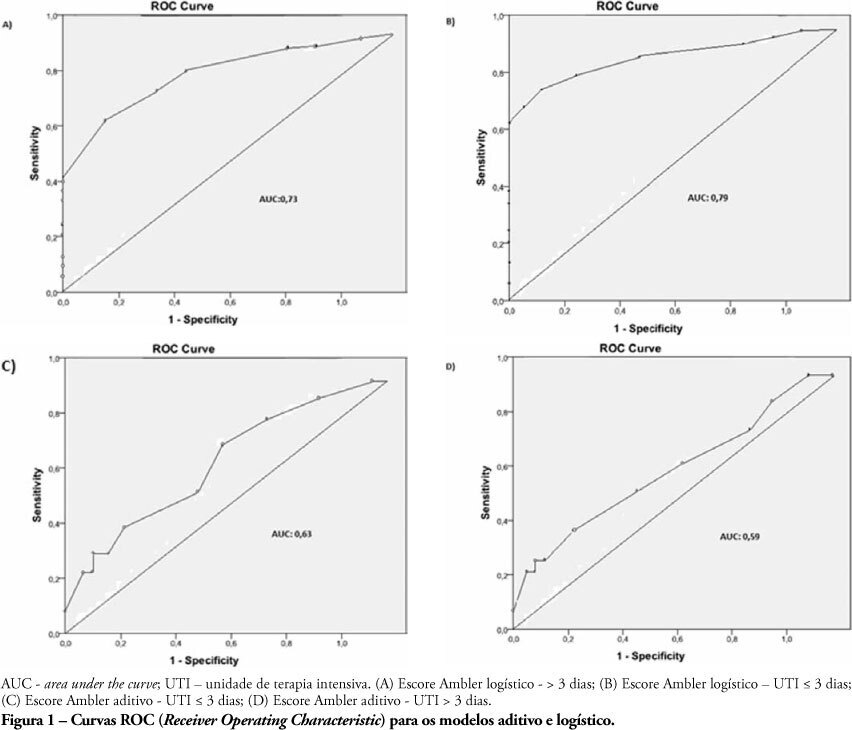
OBJECTIVES: The length of stay after prolonged cardiac surgery has been associated with poor immediate outcomes and increased costs. This study aimed to evaluate the predictive power of the Ambler Score to anticipate the length of stay in the intensive care unit. METHODS: This was a retrospective cohort study based on data collected from 110 patients undergoing valve replacement surgery alone or in combination with other procedures. Additive and logistic Ambler Scores were obtained and their predictive performances calculated using the Receiver Operating Characteristic curve. The normal length stay in the intensive care unit was assumed to be <3 days and prolonged >3 days. The areas under the receiver operating curves for both the additive and logistic models were compared using the Hanley-MacNeil test. RESULTS: The mean intensive care unit length of stay was 4.2 days. Sixty-three patients were male. The logistic model showed areas under the receiver operating characteristic curve of 0.73 and 0.79 for hospitalization > 3 days and < 3 days, respectively, showing good discriminative power. For the additive model, the areas were 0.63 and 0.59 for hospitalization > 3 days and < 3 days, respectively, a poor discriminative power. CONCLUSIONS: In our database, prolonged length of stay in the intensive care unit was positively correlated with the logistic Ambler score. The performance of the logistic Ambler Score had good discriminative power for correlation with the intensive care unit length of stay.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):339-345
DOI 10.1590/S0103-507X2010000400005
OBJECTIVES: The length of stay after prolonged cardiac surgery has been associated with poor immediate outcomes and increased costs. This study aimed to evaluate the predictive power of the Ambler Score to anticipate the length of stay in the intensive care unit. METHODS: This was a retrospective cohort study based on data collected from 110 patients undergoing valve replacement surgery alone or in combination with other procedures. Additive and logistic Ambler Scores were obtained and their predictive performances calculated using the Receiver Operating Characteristic curve. The normal length stay in the intensive care unit was assumed to be <3 days and prolonged >3 days. The areas under the receiver operating curves for both the additive and logistic models were compared using the Hanley-MacNeil test. RESULTS: The mean intensive care unit length of stay was 4.2 days. Sixty-three patients were male. The logistic model showed areas under the receiver operating characteristic curve of 0.73 and 0.79 for hospitalization > 3 days and < 3 days, respectively, showing good discriminative power. For the additive model, the areas were 0.63 and 0.59 for hospitalization > 3 days and < 3 days, respectively, a poor discriminative power. CONCLUSIONS: In our database, prolonged length of stay in the intensive care unit was positively correlated with the logistic Ambler score. The performance of the logistic Ambler Score had good discriminative power for correlation with the intensive care unit length of stay.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):346-350
DOI 10.1590/S0103-507X2010000400006
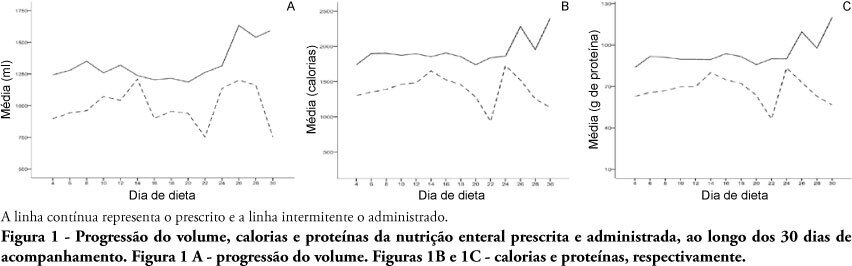
OBJECTIVES: Different conditions require that critically ill patients to receive lower than prescribed enteral nutrition volumes, energy and protein. This study objective was to evaluate the prescribed versus administered enteral nutrition difference in adults admitted to an intensive care unit. METHODS: In 2009, patients were followed for 30 days from the start of enteral nutrition to its discontinuation, or discharge from the intensive care unit. Parametric and nonparametric tests were used to evaluate prescribed versus administered differences. RESULTS: Eighty five patients were enrolled; mean age was 58.6±18.0 years and 40% were male. The patients remained in hospital for 29.5 days (IQ: 15.2 - 48.7) and were under enteral nutrition for 10 (IQ: 4.2 - 27.5) days. Lower than enteral nutrition prescribed volume (-428±243ml/day), energy (-665±412 Kcal/day) and protein (-30±19 g protein/day) was received. Individual patients' evaluation demonstrated that about 40% of the prescribed volume was not actually given. The main reasons for enteral nutrition interruptions were nausea and vomiting, abdominal distension, constipation and clinical complications (52%); diagnostic procedures (41.6%); and transition to oral feeding (5.6%). CONCLUSION: Patients admitted to intensive care unit receive less than the prescribed enteral nutrition. The routine care and gastrointestinal tract complications lead to enteral nutrition interruptions, contributing to less than prescribed calories administration.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):346-350
DOI 10.1590/S0103-507X2010000400006
OBJECTIVES: Different conditions require that critically ill patients to receive lower than prescribed enteral nutrition volumes, energy and protein. This study objective was to evaluate the prescribed versus administered enteral nutrition difference in adults admitted to an intensive care unit. METHODS: In 2009, patients were followed for 30 days from the start of enteral nutrition to its discontinuation, or discharge from the intensive care unit. Parametric and nonparametric tests were used to evaluate prescribed versus administered differences. RESULTS: Eighty five patients were enrolled; mean age was 58.6±18.0 years and 40% were male. The patients remained in hospital for 29.5 days (IQ: 15.2 - 48.7) and were under enteral nutrition for 10 (IQ: 4.2 - 27.5) days. Lower than enteral nutrition prescribed volume (-428±243ml/day), energy (-665±412 Kcal/day) and protein (-30±19 g protein/day) was received. Individual patients' evaluation demonstrated that about 40% of the prescribed volume was not actually given. The main reasons for enteral nutrition interruptions were nausea and vomiting, abdominal distension, constipation and clinical complications (52%); diagnostic procedures (41.6%); and transition to oral feeding (5.6%). CONCLUSION: Patients admitted to intensive care unit receive less than the prescribed enteral nutrition. The routine care and gastrointestinal tract complications lead to enteral nutrition interruptions, contributing to less than prescribed calories administration.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):351-357
DOI 10.1590/S0103-507X2010000400007
OBJECTIVE: To identify the relevant differences between portable blood glucose meter readings in different sampling accesses blood and laboratory analysis. METHODS: Quantitative validity study. Daily samples were collected from capillary blood, central venous access catheter and arterial catheter and the blood glucose values checked using portable blood glucose meter and laboratory analysis. The findings were analyzed with the Statistical Package for the Social Sciences - SPSS software. RESULTS: Central venous catheter samples blood glucose meter readings were found to have the best correlation with the laboratory analysis results, considered as the gold-standard. CONCLUSION: Hemodynamically unstable patients' capillary blood samples may provide false blood glucose results, and lead to inappropriate insulin solution management. Therefore, ideal blood glucose sampling is relevant to prevent insulin solution management errors.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):351-357
DOI 10.1590/S0103-507X2010000400007
OBJECTIVE: To identify the relevant differences between portable blood glucose meter readings in different sampling accesses blood and laboratory analysis. METHODS: Quantitative validity study. Daily samples were collected from capillary blood, central venous access catheter and arterial catheter and the blood glucose values checked using portable blood glucose meter and laboratory analysis. The findings were analyzed with the Statistical Package for the Social Sciences - SPSS software. RESULTS: Central venous catheter samples blood glucose meter readings were found to have the best correlation with the laboratory analysis results, considered as the gold-standard. CONCLUSION: Hemodynamically unstable patients' capillary blood samples may provide false blood glucose results, and lead to inappropriate insulin solution management. Therefore, ideal blood glucose sampling is relevant to prevent insulin solution management errors.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
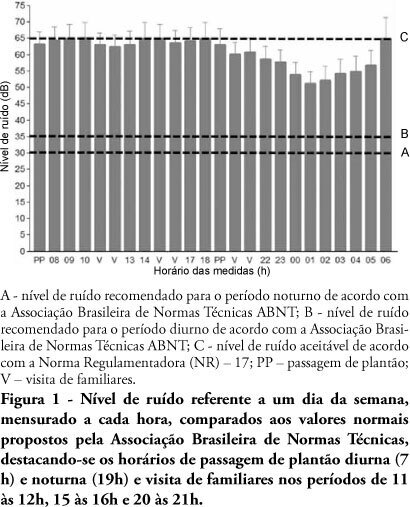
OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit's healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit's healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):300-304
DOI 10.1590/S0103-507X2010000300013
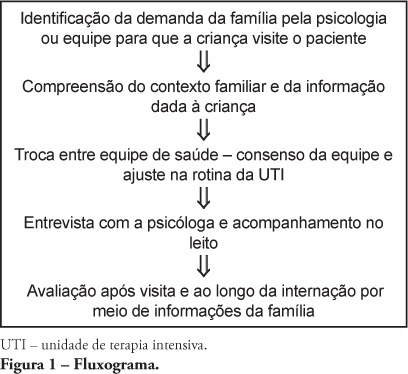
Most hospitals only allow children above 12 years-old to visit adult intensive care unit patients. However, younger children participating in the hospitalization process manifest, through their family members, their willingness to visit their hospitalized relatives. This raises different health care team members' opinions on how to manage their visits to the intensive care unit and prevent psychological harm. Aiming to expand and support this practice, a literature review was conducted, and the children's cognitive and emotional development phases related to understanding of death studied. From this, a routine for children's visits to adult intensive care unit is proposed.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):300-304
DOI 10.1590/S0103-507X2010000300013
Most hospitals only allow children above 12 years-old to visit adult intensive care unit patients. However, younger children participating in the hospitalization process manifest, through their family members, their willingness to visit their hospitalized relatives. This raises different health care team members' opinions on how to manage their visits to the intensive care unit and prevent psychological harm. Aiming to expand and support this practice, a literature review was conducted, and the children's cognitive and emotional development phases related to understanding of death studied. From this, a routine for children's visits to adult intensive care unit is proposed.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):264-269
DOI 10.1590/S0103-507X2010000300008
OBJECTIVES: In mechanically ventilated patients, humidifier devices are used to heat and moisturize the inspired gas. Heating and humidifying inspired gas may prevent complications associated with the respiratory mucosa dryness such as mucus plugging and endotracheal tube occlusion. Two devices have been commonly used to this, either heated humidifier or the heat moisture exchange filter. This study aimed to compare the effects of the heated humidifier and a model of heat moisture exchange filter on respiratory mechanics in mechanically ventilated neurological patients. METHODS: This was a randomized crossover trial, involving 31 neurological patients under mechanical ventilation randomly assigned to the humidification devices. Expired tidal volume, peak inspiratory flow, peak expiratory flow, static compliance, dynamic compliance and respiratory system resistance were evaluated. Statistical analysis used the Kolmogorov-Smirnov test and Student's t test for paired samples, in which P values < 0.05 were considered significant. RESULTS: The heat moisture exchanger filter decreased expired tidal volume, peak inspiratory flow, peak expiratory flow (p < 0.001) and dynamic compliance (p = 0.002), and increased respiratory system resistance (p < 0.001). CONCLUSION: In the studied population, the use of a heat moisture exchange filter model leaded to several changes on respiratory mechanics parameters.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):264-269
DOI 10.1590/S0103-507X2010000300008
OBJECTIVES: In mechanically ventilated patients, humidifier devices are used to heat and moisturize the inspired gas. Heating and humidifying inspired gas may prevent complications associated with the respiratory mucosa dryness such as mucus plugging and endotracheal tube occlusion. Two devices have been commonly used to this, either heated humidifier or the heat moisture exchange filter. This study aimed to compare the effects of the heated humidifier and a model of heat moisture exchange filter on respiratory mechanics in mechanically ventilated neurological patients. METHODS: This was a randomized crossover trial, involving 31 neurological patients under mechanical ventilation randomly assigned to the humidification devices. Expired tidal volume, peak inspiratory flow, peak expiratory flow, static compliance, dynamic compliance and respiratory system resistance were evaluated. Statistical analysis used the Kolmogorov-Smirnov test and Student's t test for paired samples, in which P values < 0.05 were considered significant. RESULTS: The heat moisture exchanger filter decreased expired tidal volume, peak inspiratory flow, peak expiratory flow (p < 0.001) and dynamic compliance (p = 0.002), and increased respiratory system resistance (p < 0.001). CONCLUSION: In the studied population, the use of a heat moisture exchange filter model leaded to several changes on respiratory mechanics parameters.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):274-279
DOI 10.1590/S0103-507X2010000300010
Delirium is an acute confusional state associated with increased mortality in the intensive care unit and long-term impaired functional recovery. Despite its elevated incidence and major impact in the outcomes of critically ill patients, delirium remains under-diagnosed. Presently, there are validated instruments to diagnose and monitor delirium, allowing the detection of early organ dysfunction and treatment initiation. Beyond patient's non-modifiable risk factors, there are modifiable clinical and environmental aspects that should be accessed to reduce the occurrence and severity of delirium. As recent studies demonstrate that interventions aiming to reduce sedative exposure and to improve patients' orientation associated with early mobility have proved to reduce delirium, a low incidence of delirium should be targeted and considered as a measure of quality of care in the intensive care unit (ICU).
Abstract
Rev Bras Ter Intensiva. 2010;22(3):274-279
DOI 10.1590/S0103-507X2010000300010
Delirium is an acute confusional state associated with increased mortality in the intensive care unit and long-term impaired functional recovery. Despite its elevated incidence and major impact in the outcomes of critically ill patients, delirium remains under-diagnosed. Presently, there are validated instruments to diagnose and monitor delirium, allowing the detection of early organ dysfunction and treatment initiation. Beyond patient's non-modifiable risk factors, there are modifiable clinical and environmental aspects that should be accessed to reduce the occurrence and severity of delirium. As recent studies demonstrate that interventions aiming to reduce sedative exposure and to improve patients' orientation associated with early mobility have proved to reduce delirium, a low incidence of delirium should be targeted and considered as a measure of quality of care in the intensive care unit (ICU).