Você pesquisou por y - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2013;25(2):106-114
DOI 10.5935/0103-507X.20130021
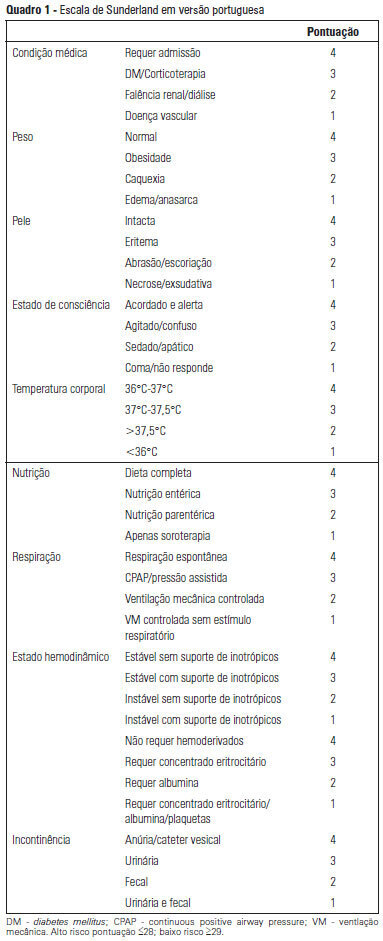
OBJECTIVE: To Translate into Portuguese and evaluate the measuring properties of the Sunderland Scale and the Cubbin & Jackson Revised Scale, which are instruments for evaluating the risk of developing pressure ulcers during intensive care. METHODS: This study included the process of translation and adaptation of the scales to the Portuguese language, as well as the validation of these tools. To assess the reliability, Cronbach alpha values of 0.702 to 0.708 were identified for the Sunderland Scale and the Cubbin & Jackson Revised Scale, respectively. The validation criteria (predictive) were performed comparatively with the Braden Scale (gold standard), and the main measurements evaluated were sensitivity, specificity, positive predictive value, negative predictive value, and area under the curve, which were calculated based on cutoff points. RESULTS: The Sunderland Scale exhibited 60% sensitivity, 86.7% specificity, 47.4% positive predictive value, 91.5% negative predictive value, and 0.86 for the area under the curve. The Cubbin & Jackson Revised Scale exhibited 73.3% sensitivity, 86.7% specificity, 52.4% positive predictive value, 94.2% negative predictive value, and 0.91 for the area under the curve. The Braden scale exhibited 100% sensitivity, 5.3% specificity, 17.4% positive predictive value, 100% negative predictive value, and 0.72 for the area under the curve. CONCLUSIONS: Both tools demonstrated reliability and validity for this sample. The Cubbin & Jackson Revised Scale yielded better predictive values for the development of pressure ulcers during intensive care.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):106-114
DOI 10.5935/0103-507X.20130021
OBJECTIVE: To Translate into Portuguese and evaluate the measuring properties of the Sunderland Scale and the Cubbin & Jackson Revised Scale, which are instruments for evaluating the risk of developing pressure ulcers during intensive care. METHODS: This study included the process of translation and adaptation of the scales to the Portuguese language, as well as the validation of these tools. To assess the reliability, Cronbach alpha values of 0.702 to 0.708 were identified for the Sunderland Scale and the Cubbin & Jackson Revised Scale, respectively. The validation criteria (predictive) were performed comparatively with the Braden Scale (gold standard), and the main measurements evaluated were sensitivity, specificity, positive predictive value, negative predictive value, and area under the curve, which were calculated based on cutoff points. RESULTS: The Sunderland Scale exhibited 60% sensitivity, 86.7% specificity, 47.4% positive predictive value, 91.5% negative predictive value, and 0.86 for the area under the curve. The Cubbin & Jackson Revised Scale exhibited 73.3% sensitivity, 86.7% specificity, 52.4% positive predictive value, 94.2% negative predictive value, and 0.91 for the area under the curve. The Braden scale exhibited 100% sensitivity, 5.3% specificity, 17.4% positive predictive value, 100% negative predictive value, and 0.72 for the area under the curve. CONCLUSIONS: Both tools demonstrated reliability and validity for this sample. The Cubbin & Jackson Revised Scale yielded better predictive values for the development of pressure ulcers during intensive care.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):115-122
DOI 10.5935/0103-507X.20130022
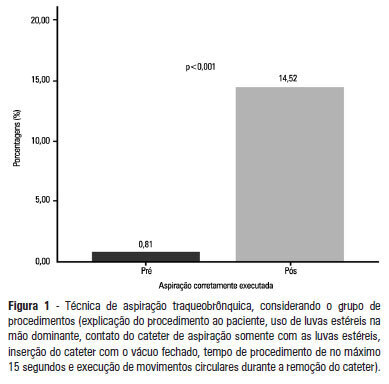
OBJECTIVE: To evaluate the effectiveness of an educational intervention on healthcare professionals' adherence to the technical recommendations for tracheobronchial aspiration in intensive care unit patients. METHODS: A quasi-experimental study was performed to evaluate intensive care unit professionals' adherence to the tracheobronchial aspiration technical recommendations in intensive care unit patients both before and after a theoretical and practical educational intervention. Comparisons were performed using the chi-square test, and the significance level was set to p<0.05. RESULTS: A total of 124 procedures, pre- and post-intervention, were observed. Increased adherence was observed in the following actions: the use of personal protective equipment (p=0.01); precaution when opening the catheter package (p<0.001); the use of a sterile glove on the dominant hand to remove the catheter (p=0.003); the contact of the sterile glove with the catheter only (p<0.001); the execution of circular movements during the catheter removal (p<0.001); wrapping the catheter in the sterile glove at the end of the procedure (p=0.003); the use of distilled water, opened at the start of the procedure, to wash the connection latex (p=0.002); the disposal of the leftover distilled water at the end of the procedure (p<0.001); and the performance of the aspiration technique procedures (p<0.001). CONCLUSION: There was a low adherence by health professionals to the preventive measures against hospital infection, indicating the need to implement educational strategies. The educational intervention used was shown to be effective in increasing adherence to the technical recommendations for tracheobronchial aspiration.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):115-122
DOI 10.5935/0103-507X.20130022
OBJECTIVE: To evaluate the effectiveness of an educational intervention on healthcare professionals' adherence to the technical recommendations for tracheobronchial aspiration in intensive care unit patients. METHODS: A quasi-experimental study was performed to evaluate intensive care unit professionals' adherence to the tracheobronchial aspiration technical recommendations in intensive care unit patients both before and after a theoretical and practical educational intervention. Comparisons were performed using the chi-square test, and the significance level was set to p<0.05. RESULTS: A total of 124 procedures, pre- and post-intervention, were observed. Increased adherence was observed in the following actions: the use of personal protective equipment (p=0.01); precaution when opening the catheter package (p<0.001); the use of a sterile glove on the dominant hand to remove the catheter (p=0.003); the contact of the sterile glove with the catheter only (p<0.001); the execution of circular movements during the catheter removal (p<0.001); wrapping the catheter in the sterile glove at the end of the procedure (p=0.003); the use of distilled water, opened at the start of the procedure, to wash the connection latex (p=0.002); the disposal of the leftover distilled water at the end of the procedure (p<0.001); and the performance of the aspiration technique procedures (p<0.001). CONCLUSION: There was a low adherence by health professionals to the preventive measures against hospital infection, indicating the need to implement educational strategies. The educational intervention used was shown to be effective in increasing adherence to the technical recommendations for tracheobronchial aspiration.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):123-129
DOI 10.5935/0103-507X.20130023
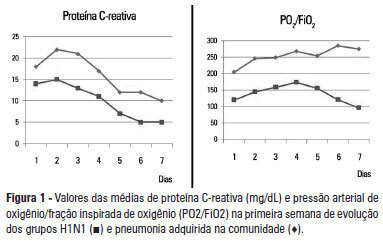
OBJECTIVE: To analyze the clinical, laboratory and evolution data of patients with severe influenza A H1N1 pneumonia and compare the data with that of patients with severe community-acquired bacterial pneumonia. METHODS: Cohort and retrospective study. All patients admitted to the intensive care unit between May 2009 and December 2010 with a diagnosis of severe pneumonia caused by the influenza A H1N1 virus were included in the study. Thirty patients with severe community-acquired pneumonia admitted within the same period were used as a control group. Severe community-acquired pneumonia was defined as the presence of at least one major severity criteria (ventilator or vasopressor use) or two minor criteria. RESULTS: The data of 45 patients were evaluated. Of these patients, 15 were infected with H1N1. When compared to the group with community-acquired pneumonia, patients from the H1N1 group had significantly lower leukocyte counts on admission (6,728±4,070 versus 16,038±7,863; p<0.05) and lower C-reactive protein levels (Day 2: 15.1±8.1 versus 22.1±10.9 mg/dL; p<0.05). The PaO2/FiO2 ratio values were lower in the first week in patients with H1N1. Patients who did not survive the H1N1 severe pneumonia had significantly higher levels of C-reactive protein and higher serum creatinine levels compared with patients who survived. The mortality rate was significantly higher in the H1N1 group than in the control group (53% versus 20%; p=0.056, respectivelly). CONCLUSION: Differences in the leukocyte count, C-reactive protein concentrations and oxygenation profiles may contribute to the diagnosis and prognosis of patients with severe influenza A H1N1 virus-related pneumonia and community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):123-129
DOI 10.5935/0103-507X.20130023
OBJECTIVE: To analyze the clinical, laboratory and evolution data of patients with severe influenza A H1N1 pneumonia and compare the data with that of patients with severe community-acquired bacterial pneumonia. METHODS: Cohort and retrospective study. All patients admitted to the intensive care unit between May 2009 and December 2010 with a diagnosis of severe pneumonia caused by the influenza A H1N1 virus were included in the study. Thirty patients with severe community-acquired pneumonia admitted within the same period were used as a control group. Severe community-acquired pneumonia was defined as the presence of at least one major severity criteria (ventilator or vasopressor use) or two minor criteria. RESULTS: The data of 45 patients were evaluated. Of these patients, 15 were infected with H1N1. When compared to the group with community-acquired pneumonia, patients from the H1N1 group had significantly lower leukocyte counts on admission (6,728±4,070 versus 16,038±7,863; p<0.05) and lower C-reactive protein levels (Day 2: 15.1±8.1 versus 22.1±10.9 mg/dL; p<0.05). The PaO2/FiO2 ratio values were lower in the first week in patients with H1N1. Patients who did not survive the H1N1 severe pneumonia had significantly higher levels of C-reactive protein and higher serum creatinine levels compared with patients who survived. The mortality rate was significantly higher in the H1N1 group than in the control group (53% versus 20%; p=0.056, respectivelly). CONCLUSION: Differences in the leukocyte count, C-reactive protein concentrations and oxygenation profiles may contribute to the diagnosis and prognosis of patients with severe influenza A H1N1 virus-related pneumonia and community-acquired pneumonia.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
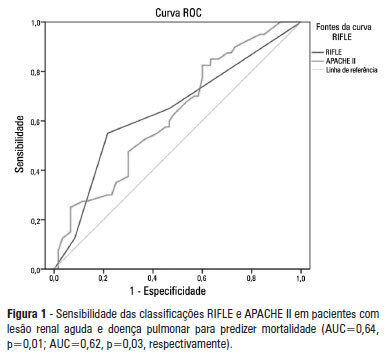
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):130-136
DOI 10.5935/0103-507X.20130024
OBJECTIVE: To examine the factors associated with acute kidney injury and outcome in patients with lung disease. METHODS: A prospective study was conducted with 100 consecutive patients admitted to a respiratory intensive care unit in Fortaleza (CE), Brazil. The risk factors for acute kidney injury and mortality were investigated in a group of patients with lung diseases. RESULTS: The mean age of the study population was 57 years, and 50% were male. The incidence of acute kidney injury was higher in patients with PaO2/FiO2<200 mmHg (54% versus 23.7%; p=0.02). Death was observed in 40 cases and the rate of mortality of the acute kidney injury group was higher (62.8% versus 27.6%; p=0.01). The independent factor that was found to be associated with acute kidney injury was PaO2/FiO2<200 mmHg (p=0.01), and the independent risk factors for death were PEEP at admission (OR: 3.6; 95%CI: 1.3-9.6; p=0.009) and need for hemodialysis (OR: 7.9; 95%CI: 2.2-28.3; p=0.001). CONCLUSION: There was a higher mortality rate in the acute kidney injury group. Increased mortality was associated with mechanical ventilation, high PEEP, urea and need for dialysis. Further studies must be performed to better establish the relationship between kidney and lung injury and its impact on patient outcome.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):137-147
DOI 10.5935/0103-507X.20130025
Delirium occurs in up to 80% of patients admitted to intensive care units. Although under-diagnosed, delirium is associated with a significant increase in morbidity and mortality in critical patients. Here, we review the main risk factors, clinical manifestations and preventative and therapeutic approaches (pharmacological and non-pharmacological) for this illness.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):137-147
DOI 10.5935/0103-507X.20130025
Delirium occurs in up to 80% of patients admitted to intensive care units. Although under-diagnosed, delirium is associated with a significant increase in morbidity and mortality in critical patients. Here, we review the main risk factors, clinical manifestations and preventative and therapeutic approaches (pharmacological and non-pharmacological) for this illness.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):148-154
DOI 10.5935/0103-507X.20130026
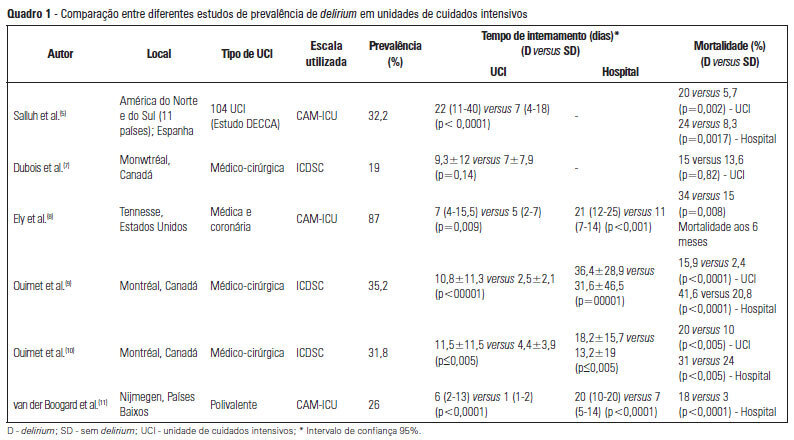
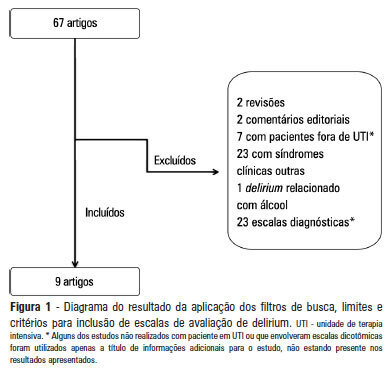
OBJECTIVE: To identify scales that can establish a quantitative assessment of delirium symptoms in critically ill patients through a systematic review. METHODS: Studies that evaluated delirium stratification scales in patients hospitalized in intensive care units were selected in a search performed in the MedLine database. Validation studies of these scales and their target patient populations were analyzed, and we identified the examiner and the signs and symptoms evaluated. In addition, the duration of the application and the sensitivity and specificity of each scale were assessed. RESULTS: Six scales were identified: the Delirium Detection Score, the Cognitive Test of Delirium, the Memorial Delirium Assessment Scale, the Intensive Care Delirium Screening Checklist, The Neelon and Champagne Confusion Scale and the Delirium Rating Scale-Revised-98. CONCLUSION: The scales identified allow the stratification and monitoring of critically ill patients with delirium. Among the six scales, the most studied and best suited for use in the intensive care units was the Intensive Care Delirium Screening
Abstract
Rev Bras Ter Intensiva. 2013;25(2):148-154
DOI 10.5935/0103-507X.20130026
OBJECTIVE: To identify scales that can establish a quantitative assessment of delirium symptoms in critically ill patients through a systematic review. METHODS: Studies that evaluated delirium stratification scales in patients hospitalized in intensive care units were selected in a search performed in the MedLine database. Validation studies of these scales and their target patient populations were analyzed, and we identified the examiner and the signs and symptoms evaluated. In addition, the duration of the application and the sensitivity and specificity of each scale were assessed. RESULTS: Six scales were identified: the Delirium Detection Score, the Cognitive Test of Delirium, the Memorial Delirium Assessment Scale, the Intensive Care Delirium Screening Checklist, The Neelon and Champagne Confusion Scale and the Delirium Rating Scale-Revised-98. CONCLUSION: The scales identified allow the stratification and monitoring of critically ill patients with delirium. Among the six scales, the most studied and best suited for use in the intensive care units was the Intensive Care Delirium Screening
Abstract
Rev Bras Ter Intensiva. 2013;25(2):155-161
DOI 10.5935/0103-507X.20130027
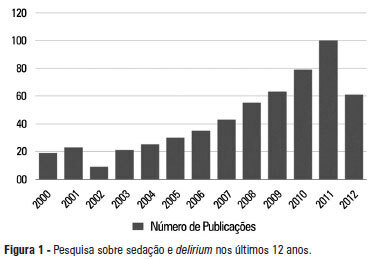
A significant number of landmark studies have been published in the last decade that increase the current knowledge on sedation for critically ill patients. Therefore, many practices that were considered standard of care are now outdated. Oversedation has been shown to be hazardous, and light sedation and no-sedation protocols are associated with better patient outcomes. Delirium is increasingly recognized as a major form of acute brain dysfunction that is associated with higher mortality, longer duration of mechanical ventilation and longer lengths of stay in the intensive care unit and hospital. Despite all the available evidence, translating research into bedside care is a daunting task. International surveys have shown that practices such as sedation interruption and titration are performed only in the minority of cases. Implementing best practices is a major challenge that must also be addressed in the new guidelines. In this review, we summarize the findings of sedation and delirium research over the last years. We also discuss the gap between evidence and clinical practice and highlight ways to implement best practices at the bedside.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):155-161
DOI 10.5935/0103-507X.20130027
A significant number of landmark studies have been published in the last decade that increase the current knowledge on sedation for critically ill patients. Therefore, many practices that were considered standard of care are now outdated. Oversedation has been shown to be hazardous, and light sedation and no-sedation protocols are associated with better patient outcomes. Delirium is increasingly recognized as a major form of acute brain dysfunction that is associated with higher mortality, longer duration of mechanical ventilation and longer lengths of stay in the intensive care unit and hospital. Despite all the available evidence, translating research into bedside care is a daunting task. International surveys have shown that practices such as sedation interruption and titration are performed only in the minority of cases. Implementing best practices is a major challenge that must also be addressed in the new guidelines. In this review, we summarize the findings of sedation and delirium research over the last years. We also discuss the gap between evidence and clinical practice and highlight ways to implement best practices at the bedside.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
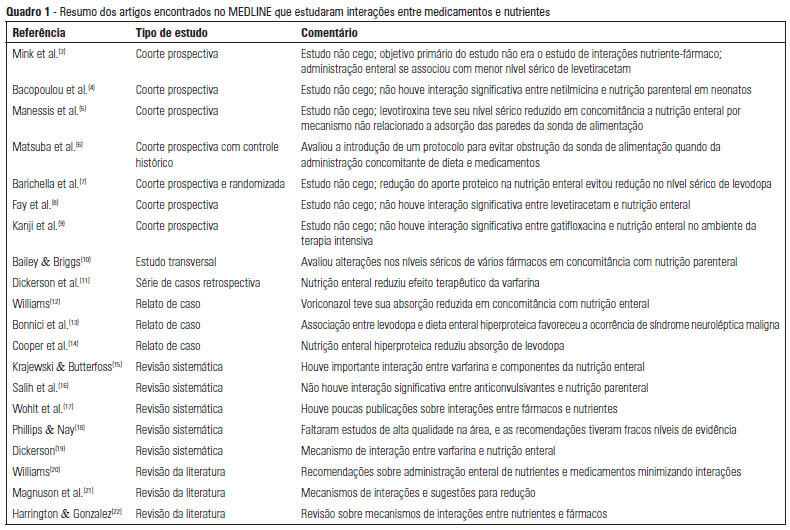
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.
Abstract
Rev Bras Ter Intensiva. 2013;25(2):162-167
DOI 10.5935/0103-507X.20130028
OBJECTIVE: To describe the interactions between drugs and nutrients and their frequency in the intensive care unit and to assess the professional team's awareness regarding this subject. METHODS: The keywords "drug interactions" and "nutrition therapy" were searched in the PubMed (specifically MeSH) electronic database. The studies were systematically reviewed for descriptions of the types of interactions between drugs and nutrients, including their frequency and consequences. RESULTS: Sixty-seven articles were found. Among these, 20 articles were appropriate for the methodology adopted and accomplished the objectives of the study. Of these 20 articles, 14 articles described interactions between drugs and enteral nutrition, three described interactions between drugs and parenteral nutrition, and three described the importance and care required to avoid such interactions. CONCLUSIONS: The literature about drug and nutrient interactions is limited and suggests the inability of health care teams to recognize the potential for these interactions. Possibly, the elaboration of a protocol to evaluate drug-nutrient interactions will increase the safety and efficacy of therapeutics.