
-
Correspondence
To: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
- Josef Finsterer
 ,
, - Carla Alexandra Scorza ,
- Antonio-Carlos Guimarães Almeida ,
- Fulvio Alexandre Scorza
Abstract
CorrespondenceTo: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240131en
DOI 10.62675/2965-2774.20240131-en
- Josef Finsterer ,
- Carla Alexandra Scorza ,
- Antonio-Carlos Guimarães Almeida ,
- Fulvio Alexandre Scorza
Views5To the Editor We read an interesting prospective, single-center, observational cohort study on the relationship between the cross-sectional diameter of the rectus femoris muscle, the degree of diaphragmatic excursion, and the outcome of weaning 81 critically ill patients by Vieira et al.() Successfully weaning critically ill patients from mechanical ventilation has been found to be […]See moreViews5

Abstract
CorrespondenceTo: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240131en
DOI 10.62675/2965-2774.20240131-en
- Josef Finsterer ,
- Carla Alexandra Scorza ,
- Antonio-Carlos Guimarães Almeida ,
- Fulvio Alexandre Scorza
Views5To the Editor We read an interesting prospective, single-center, observational cohort study on the relationship between the cross-sectional diameter of the rectus femoris muscle, the degree of diaphragmatic excursion, and the outcome of weaning 81 critically ill patients by Vieira et al.() Successfully weaning critically ill patients from mechanical ventilation has been found to be […]See more - Josef Finsterer
-
Research Letter
Generalizing the application of machine learning predictive models across different populations: does a model to predict the use of renal replacement therapy in critically ill COVID-19 patients apply to general intensive care unit patients?
- Allan Rodrigo Murrieta França ,
- Julia Nunes Cantarino,
- Jorge Ibrain Figueira Salluh ,
- Leonardo dos Santos Lourenço Bastos
Abstract
Research LetterGeneralizing the application of machine learning predictive models across different populations: does a model to predict the use of renal replacement therapy in critically ill COVID-19 patients apply to general intensive care unit patients?
Crit Care Sci. 2024;36:e20240285en
DOI 10.62675/2965-2774.20240285-pt
- Allan Rodrigo Murrieta França ,
- Julia Nunes Cantarino,
- Jorge Ibrain Figueira Salluh ,
- Leonardo dos Santos Lourenço Bastos
Views38TO THE EDITOR The widespread use of machine learning has created the possibility of generating robust prediction models for individual patients; however, caution is needed in their use for heterogeneous critically ill populations.() Recent literature has demonstrated major advances in the field of acute kidney injury prediction and the need for renal replacement therapy (RRT).() […]See moreViews38Abstract
Research LetterGeneralizing the application of machine learning predictive models across different populations: does a model to predict the use of renal replacement therapy in critically ill COVID-19 patients apply to general intensive care unit patients?
Crit Care Sci. 2024;36:e20240285en
DOI 10.62675/2965-2774.20240285-pt
- Allan Rodrigo Murrieta França ,
- Julia Nunes Cantarino,
- Jorge Ibrain Figueira Salluh ,
- Leonardo dos Santos Lourenço Bastos
Views38TO THE EDITOR The widespread use of machine learning has created the possibility of generating robust prediction models for individual patients; however, caution is needed in their use for heterogeneous critically ill populations.() Recent literature has demonstrated major advances in the field of acute kidney injury prediction and the need for renal replacement therapy (RRT).() […]See more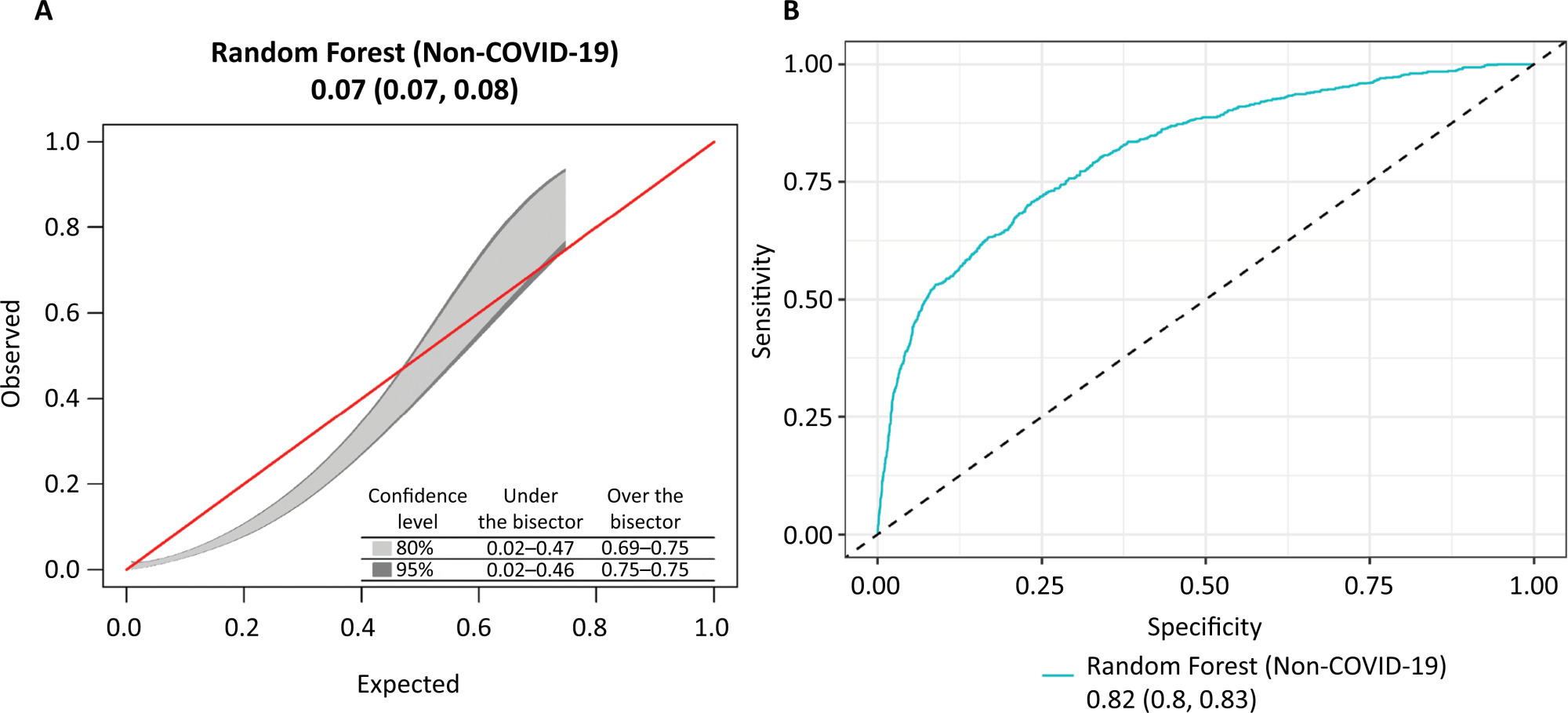
- Allan Rodrigo Murrieta França
-
Viewpoint
Revolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Crit Care Sci. 2024;36:e20240023en
Abstract
ViewpointRevolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Crit Care Sci. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Views7Frailty represents a condition of vulnerability leading to inadequate recovery following a stressful event, such as an acute illness or injury. This inadequate recovery results from cumulative, multisystem physiological depletion over a lifetime.() The frailty state implies that the available functional reserve is insufficient for complete recovery, often leading to a maladaptive response disproportionate to […]See moreViews7Abstract
ViewpointRevolutionizing care: unleashing the power of comprehensive geriatric assessment in tailoring treatment for frail postintensive care patients
Crit Care Sci. 2024;36:e20240023en
DOI 10.62675/2965-2774.20240023-en
Views7Frailty represents a condition of vulnerability leading to inadequate recovery following a stressful event, such as an acute illness or injury. This inadequate recovery results from cumulative, multisystem physiological depletion over a lifetime.() The frailty state implies that the available functional reserve is insufficient for complete recovery, often leading to a maladaptive response disproportionate to […]See more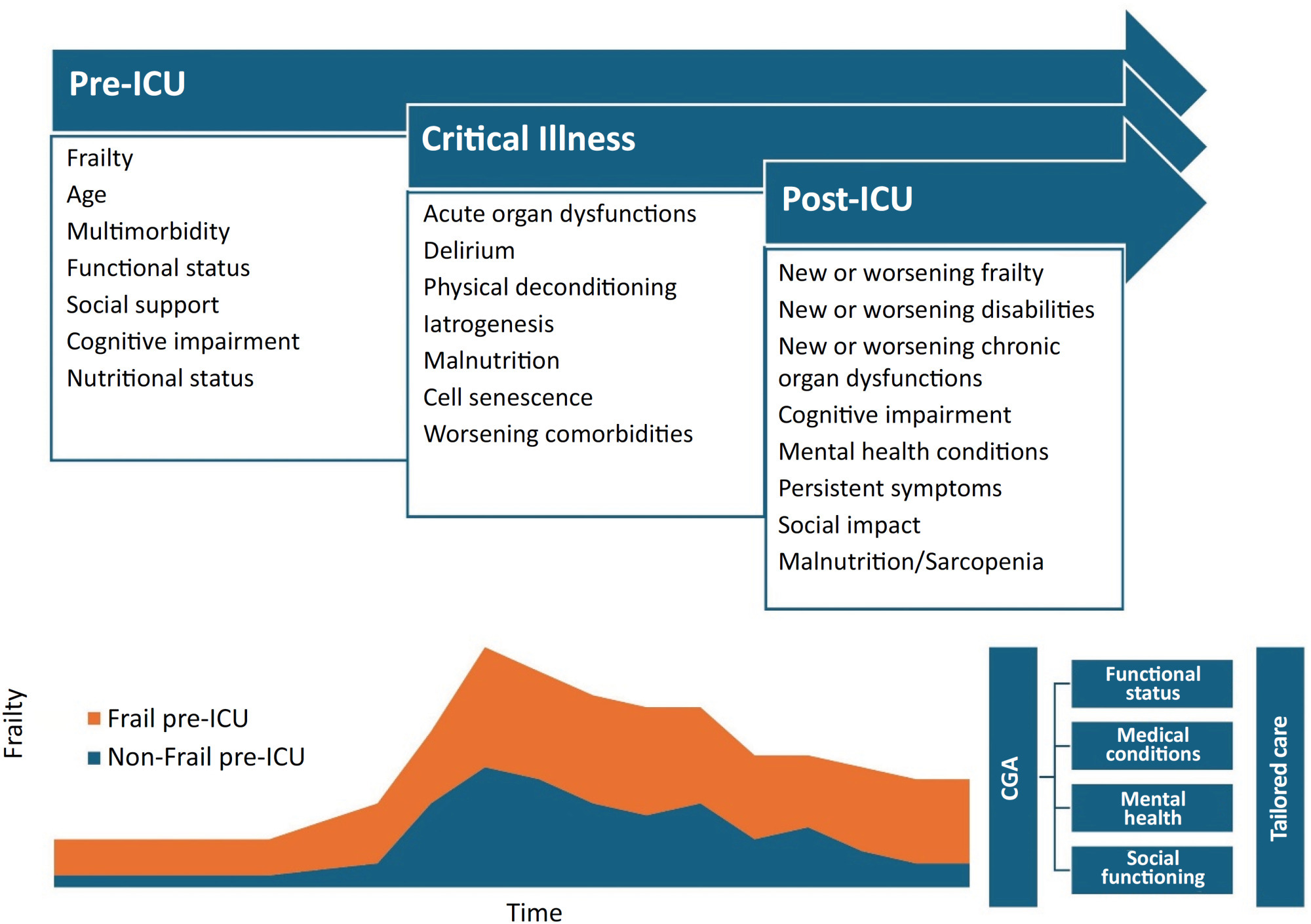
-
Original Article
Efficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover , [ … ],
- Vighnesh Ashok
Abstract
Original ArticleEfficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
Crit Care Sci. 2024;36:e20240144en
DOI 10.62675/2965-2774.20240144-pt
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover ,
- Sunaakshi Puri ,
- Vighnesh Ashok
Views551See moreABSTRACT
Objective:
To determine whether enteral melatonin decreases the incidence of delirium in critically ill adults.
Methods:
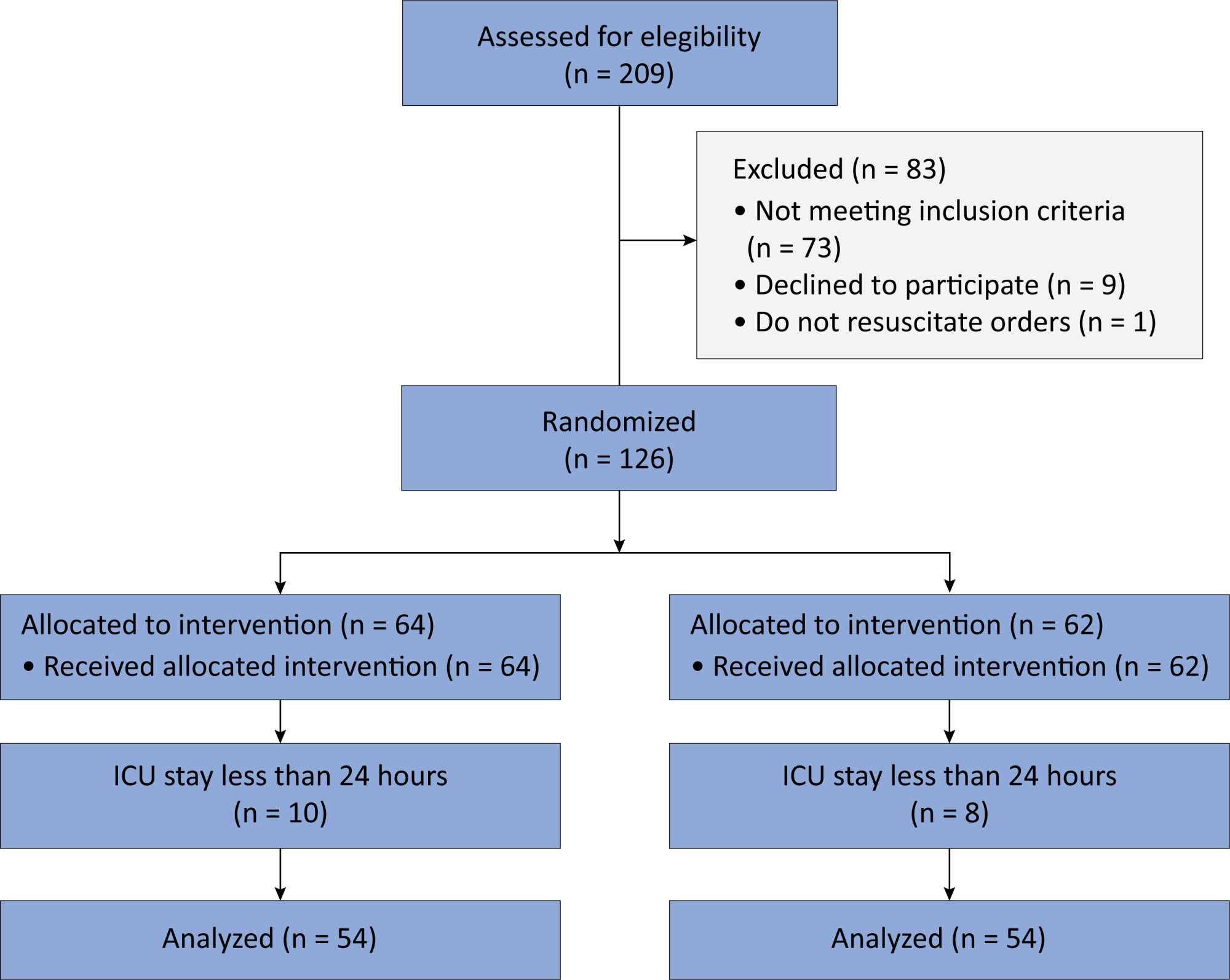
In this randomized controlled trial, adults were admitted to the intensive care unit and received either usual standard care alone (Control Group) or in combination with 3mg of enteral melatonin once a day at 9 PM (Melatonin Group). Concealment of allocation was done by serially numbered opaque sealed envelopes. The intensivist assessing delirium and the investigator performing the data analysis were blinded to the group allocation. The primary outcome was the incidence of delirium within 24 hours of the intensive care unit stay. The secondary outcomes were the incidence of delirium on Days 3 and 7, intensive care unit mortality, length of intensive care unit stay, duration of mechanical ventilation and Glasgow outcome score (at discharge).
Results:
We included 108 patients in the final analysis, with 54 patients in each group. At 24 hours of intensive care unit stay, there was no difference in the incidence of delirium between Melatonin and Control Groups (29.6 versus 46.2%; RR = 0.6; 95%CI 0.38 – 1.05; p = 0.11). No secondary outcome showed a statistically significant difference.
Conclusion:
Enteral melatonin 3mg is not more effective at decreasing the incidence of delirium than standard care is in critically ill adults.
Views551Abstract
Original ArticleEfficacy of melatonin in decreasing the incidence of delirium in critically ill adults: a randomized controlled trial
Crit Care Sci. 2024;36:e20240144en
DOI 10.62675/2965-2774.20240144-pt
- Anjishnujit Bandyopadhyay ,
- Lakshmi Narayana Yaddanapudi ,
- Vikas Saini ,
- Neeru Sahni ,
- Sandeep Grover ,
- Sunaakshi Puri ,
- Vighnesh Ashok
Views551See moreABSTRACT
Objective:
To determine whether enteral melatonin decreases the incidence of delirium in critically ill adults.
Methods:
In this randomized controlled trial, adults were admitted to the intensive care unit and received either usual standard care alone (Control Group) or in combination with 3mg of enteral melatonin once a day at 9 PM (Melatonin Group). Concealment of allocation was done by serially numbered opaque sealed envelopes. The intensivist assessing delirium and the investigator performing the data analysis were blinded to the group allocation. The primary outcome was the incidence of delirium within 24 hours of the intensive care unit stay. The secondary outcomes were the incidence of delirium on Days 3 and 7, intensive care unit mortality, length of intensive care unit stay, duration of mechanical ventilation and Glasgow outcome score (at discharge).
Results:
We included 108 patients in the final analysis, with 54 patients in each group. At 24 hours of intensive care unit stay, there was no difference in the incidence of delirium between Melatonin and Control Groups (29.6 versus 46.2%; RR = 0.6; 95%CI 0.38 – 1.05; p = 0.11). No secondary outcome showed a statistically significant difference.
Conclusion:
Enteral melatonin 3mg is not more effective at decreasing the incidence of delirium than standard care is in critically ill adults.
- Anjishnujit Bandyopadhyay
-
Viewpoint
“While the wolf is away”: the echo of globalization delaying family decisions in intensive care
Crit Care Sci. 2024;36:e20240008en
Abstract
Viewpoint“While the wolf is away”: the echo of globalization delaying family decisions in intensive care
Crit Care Sci. 2024;36:e20240008en
DOI 10.62675/2965-2774.20240008-en
Views9Globalization is a complex process that is defined as the “shrinking” of our world through advances in technology and industry; specifically, individuals, peoples, and nations that are very distant from each other are now in contact and may share at least some aspects of a “global” culture.() Globalization is multifaceted by nature, affecting society economically, […]See moreViews9Abstract
Viewpoint“While the wolf is away”: the echo of globalization delaying family decisions in intensive care
Crit Care Sci. 2024;36:e20240008en
DOI 10.62675/2965-2774.20240008-en
Views9Globalization is a complex process that is defined as the “shrinking” of our world through advances in technology and industry; specifically, individuals, peoples, and nations that are very distant from each other are now in contact and may share at least some aspects of a “global” culture.() Globalization is multifaceted by nature, affecting society economically, […]See more -
Original Article
A comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada , [ … ],
- Carlos Roberto Ribeiro de Carvalho
Abstract
Original ArticleA comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
Crit Care Sci. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada ,
- Patrícia Rocha Alves Ferreira ,
- Karina Ramiceli Soares da Silva ,
- Natália Tiemi Simokomaki Souza ,
- Carlos Toufen Junior ,
- Luciana Dias Chiavegato ,
- Marcelo Britto Passos Amato ,
- Maria Ignez Zanetti Feltrim ,
- Carlos Roberto Ribeiro de Carvalho
Views60See moreABSTRACT
Objective:
To examine the physical function and respiratory muscle strength of patients – who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
Methods:
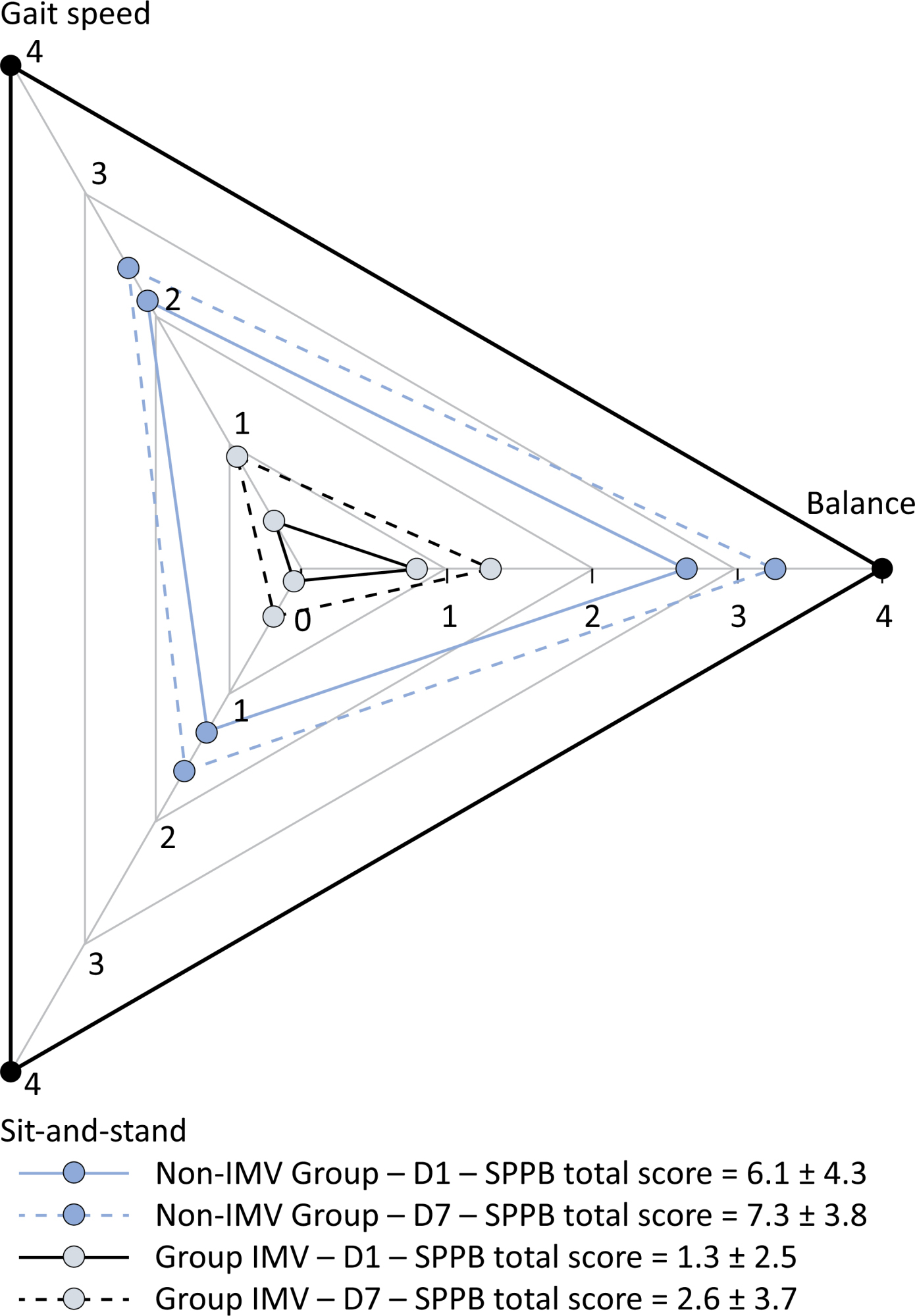
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Results:
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 – 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Conclusion:
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
Views60Abstract
Original ArticleA comprehensive physical functional assessment of survivors of critical care unit stay due to COVID-19
Crit Care Sci. 2024;36:e20240284en
DOI 10.62675/2965-2774.20240284-en
- Marcia Souza Volpe ,
- Ana Carolina Cardoso dos Santos ,
- Sílvia Gaspar ,
- Jade Lara de Melo ,
- Gabriela Harada ,
- Patrícia Rocha Alves Ferreira ,
- Karina Ramiceli Soares da Silva ,
- Natália Tiemi Simokomaki Souza ,
- Carlos Toufen Junior ,
- Luciana Dias Chiavegato ,
- Marcelo Britto Passos Amato ,
- Maria Ignez Zanetti Feltrim ,
- Carlos Roberto Ribeiro de Carvalho
Views60See moreABSTRACT
Objective:
To examine the physical function and respiratory muscle strength of patients – who recovered from critical COVID-19 – after intensive care unit discharge to the ward on Days one (D1) and seven (D7), and to investigate variables associated with functional impairment.
Methods:
This was a prospective cohort study of adult patients with COVID-19 who needed invasive mechanical ventilation, non-invasive ventilation or high-flow nasal cannula and were discharged from the intensive care unit to the ward. Participants were submitted to Medical Research Council sum-score, handgrip strength, maximal inspiratory pressure, maximal expiratory pressure, and short physical performance battery tests. Participants were grouped into two groups according to their need for invasive ventilation: the Invasive Mechanical Ventilation Group (IMV Group) and the Non-Invasive Mechanical Ventilation Group (Non-IMV Group).
Results:
Patients in the IMV Group (n = 31) were younger and had higher Sequential Organ Failure Assessment scores than those in the Non-IMV Group (n = 33). The short physical performance battery scores (range 0 – 12) on D1 and D7 were 6.1 ± 4.3 and 7.3 ± 3.8, respectively for the Non-Invasive Mechanical Ventilation Group, and 1.3 ± 2.5 and 2.6 ± 3.7, respectively for the IMV Group. The prevalence of intensive care unit-acquired weakness on D7 was 13% for the Non-IMV Group and 72% for the IMV Group. The maximal inspiratory pressure, maximal expiratory pressure, and handgrip strength increased on D7 in both groups, but the maximal expiratory pressure and handgrip strength were still weak. Only maximal inspiratory pressure was recovered (i.e., > 80% of the predicted value) in the Non-IMV Group. Female sex, and the need and duration of invasive mechanical were independently and negatively associated with the short physical performance battery score and handgrip strength.
Conclusion:
Patients who recovered from critical COVID-19 and who received invasive mechanical ventilation presented greater disability than those who were not invasively ventilated. However, they both showed marginal functional improvement during early recovery, regardless of the need for invasive mechanical ventilation. This might highlight the severity of disability caused by SARS-CoV-2.
- Marcia Souza Volpe
-
Original Article
Driving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota , [ … ],
- Bruno Valle Pinheiro
Abstract
Original ArticleDriving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
Crit Care Sci. 2024;36:e20240208en
DOI 10.62675/2965-2774.20240208-en
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota ,
- Giovani Bernardo Costa ,
- Fernando Antonio Basile Colugnati ,
- Bruno Valle Pinheiro
Views27ABSTRACT
Objective:
To evaluate the association between driving pressure and tidal volume based on predicted body weight and mortality in a cohort of patients with acute respiratory distress syndrome caused by COVID-19.
Methods:
This was a prospective, observational study that included patients with acute respiratory distress syndrome due to COVID-19 admitted to two intensive care units. We performed multivariable analyses to determine whether driving pressure and tidal volume/kg predicted body weight on the first day of mechanical ventilation, as independent variables, are associated with hospital mortality.
Results:
We included 231 patients. The mean age was 64 (53 – 74) years, and the mean Simplified Acute and Physiology Score 3 score was 45 (39 – 54). The hospital mortality rate was 51.9%. Driving pressure was independently associated with hospital mortality (odds ratio 1.21, 95%CI 1.04 – 1.41 for each cm H2O increase in driving pressure, p = 0.01). Based on a double stratification analysis, we found that for the same level of tidal volume/kg predicted body weight, the risk of hospital death increased with increasing driving pressure. However, changes in tidal volume/kg predicted body weight were not associated with mortality when they did not lead to an increase in driving pressure.
Conclusion:
In patients with acute respiratory distress syndrome caused by COVID-19, exposure to higher driving pressure, as opposed to higher tidal volume/kg predicted body weight, is associated with greater mortality. These results suggest that driving pressure might be a primary target for lung-protective mechanical ventilation in these patients.
Keywords:acute respiratory distress syndromeCoronavirus infectionsCOVID-19Intensive care unitsMortalityRespiration, artificialTidal VolumeSee moreViews27Abstract
Original ArticleDriving pressure, as opposed to tidal volume based on predicted body weight, is associated with mortality: results from a prospective cohort of COVID-19 acute respiratory distress syndrome patients
Crit Care Sci. 2024;36:e20240208en
DOI 10.62675/2965-2774.20240208-en
- Erich Vidal Carvalho ,
- Maycon Moura Reboredo ,
- Edimar Pedrosa Gomes ,
- Pedro Nascimento Martins ,
- Gabriel Paz Souza Mota ,
- Giovani Bernardo Costa ,
- Fernando Antonio Basile Colugnati ,
- Bruno Valle Pinheiro
Views27ABSTRACT
Objective:
To evaluate the association between driving pressure and tidal volume based on predicted body weight and mortality in a cohort of patients with acute respiratory distress syndrome caused by COVID-19.
Methods:
This was a prospective, observational study that included patients with acute respiratory distress syndrome due to COVID-19 admitted to two intensive care units. We performed multivariable analyses to determine whether driving pressure and tidal volume/kg predicted body weight on the first day of mechanical ventilation, as independent variables, are associated with hospital mortality.
Results:
We included 231 patients. The mean age was 64 (53 – 74) years, and the mean Simplified Acute and Physiology Score 3 score was 45 (39 – 54). The hospital mortality rate was 51.9%. Driving pressure was independently associated with hospital mortality (odds ratio 1.21, 95%CI 1.04 – 1.41 for each cm H2O increase in driving pressure, p = 0.01). Based on a double stratification analysis, we found that for the same level of tidal volume/kg predicted body weight, the risk of hospital death increased with increasing driving pressure. However, changes in tidal volume/kg predicted body weight were not associated with mortality when they did not lead to an increase in driving pressure.
Conclusion:
In patients with acute respiratory distress syndrome caused by COVID-19, exposure to higher driving pressure, as opposed to higher tidal volume/kg predicted body weight, is associated with greater mortality. These results suggest that driving pressure might be a primary target for lung-protective mechanical ventilation in these patients.
Keywords:acute respiratory distress syndromeCoronavirus infectionsCOVID-19Intensive care unitsMortalityRespiration, artificialTidal VolumeSee more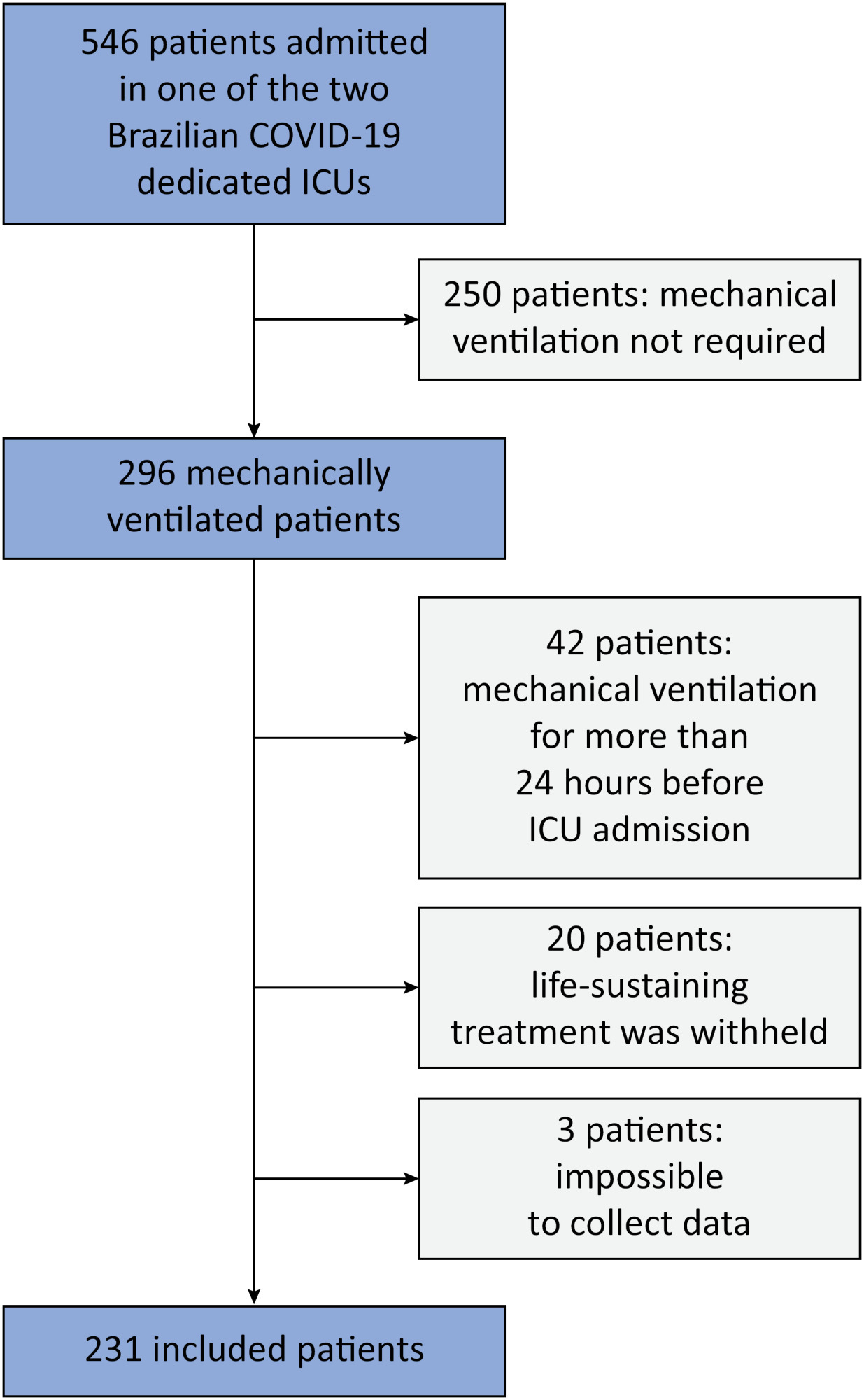
- Erich Vidal Carvalho
-
Editorial
Challenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See moreViews25Abstract
EditorialChallenges and limitations of using ventilator-free days as an outcome in critical care trials
Crit Care Sci. 2024;36:e20240088en
DOI 10.62675/2965-2774.20240088-en
Views25The use of ventilator-free days (VFDs) as an outcome measure is increasingly popular in critical care research.(-) This composite outcome simultaneously reflects patient survival and the time not spent on mechanical ventilation (MV) within a specified timeframe, which usually extends from randomization up to Day 28. For patients who do not survive this period, VFDs […]See more -
Original Article
Goal-directed therapy guided by the FloTrac sensor in major surgery: a systematic review and meta-analysis
- Márcia Regina Dias Alves ,
- Saulo Fernandes Saturnino ,
- Ana Beatriz Zen ,
- Dayane Gabriele Silveira de Albuquerque ,
- Henrique Diegoli
Abstract
Original ArticleGoal-directed therapy guided by the FloTrac sensor in major surgery: a systematic review and meta-analysis
Crit Care Sci. 2024;36:e20240196en
DOI 10.62675/2965-2774.20240196-en
- Márcia Regina Dias Alves ,
- Saulo Fernandes Saturnino ,
- Ana Beatriz Zen ,
- Dayane Gabriele Silveira de Albuquerque ,
- Henrique Diegoli
Views77ABSTRACT
Objective
To provide insights into the potential benefits of goal-directed therapy guided by FloTrac in reducing postoperative complications and improving outcomes.
Methods
We performed a systematic review and meta-analysis of randomized controlled trials to evaluate goal-directed therapy guided by FloTrac in major surgery, comparing goal-directed therapy with usual care or invasive monitoring in cardiac and noncardiac surgery subgroups. The quality of the articles and evidence were evaluated with a risk of bias tool and GRADE.
Results
We included 29 randomized controlled trials with 3,468 patients. Goal-directed therapy significantly reduced the duration of hospital stay (mean difference -1.43 days; 95%CI 2.07 to -0.79; I2 81%), intensive care unit stay (mean difference -0.77 days; 95%CI -1.18 to -0.36; I2 93%), and mechanical ventilation (mean difference -2.48 hours, 95%CI -4.10 to -0.86, I2 63%). There was no statistically significant difference in mortality, myocardial infarction, acute kidney injury or hypotension, but goal-directed therapy significantly reduced the risk of heart failure or pulmonary edema (RR 0.46; 95%CI 0.23 – 0.92; I2 0%).
Conclusion
Goal-directed therapy guided by the FloTrac sensor improved clinical outcomes and shortened the length of stay in the hospital and intensive care unit in patients undergoing major surgery. Further research can validate these results using specific protocols and better understand the potential benefits of FloTrac beyond these outcomes.
Keywords:Goalsheart failureIntensive care unitsLength of stayMonitoring, intraoperativeTreatment outcomeSee moreViews77Abstract
Original ArticleGoal-directed therapy guided by the FloTrac sensor in major surgery: a systematic review and meta-analysis
Crit Care Sci. 2024;36:e20240196en
DOI 10.62675/2965-2774.20240196-en
- Márcia Regina Dias Alves ,
- Saulo Fernandes Saturnino ,
- Ana Beatriz Zen ,
- Dayane Gabriele Silveira de Albuquerque ,
- Henrique Diegoli
Views77ABSTRACT
Objective
To provide insights into the potential benefits of goal-directed therapy guided by FloTrac in reducing postoperative complications and improving outcomes.
Methods
We performed a systematic review and meta-analysis of randomized controlled trials to evaluate goal-directed therapy guided by FloTrac in major surgery, comparing goal-directed therapy with usual care or invasive monitoring in cardiac and noncardiac surgery subgroups. The quality of the articles and evidence were evaluated with a risk of bias tool and GRADE.
Results
We included 29 randomized controlled trials with 3,468 patients. Goal-directed therapy significantly reduced the duration of hospital stay (mean difference -1.43 days; 95%CI 2.07 to -0.79; I2 81%), intensive care unit stay (mean difference -0.77 days; 95%CI -1.18 to -0.36; I2 93%), and mechanical ventilation (mean difference -2.48 hours, 95%CI -4.10 to -0.86, I2 63%). There was no statistically significant difference in mortality, myocardial infarction, acute kidney injury or hypotension, but goal-directed therapy significantly reduced the risk of heart failure or pulmonary edema (RR 0.46; 95%CI 0.23 – 0.92; I2 0%).
Conclusion
Goal-directed therapy guided by the FloTrac sensor improved clinical outcomes and shortened the length of stay in the hospital and intensive care unit in patients undergoing major surgery. Further research can validate these results using specific protocols and better understand the potential benefits of FloTrac beyond these outcomes.
Keywords:Goalsheart failureIntensive care unitsLength of stayMonitoring, intraoperativeTreatment outcomeSee more - Márcia Regina Dias Alves
-
Original Article
Conscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda , [ … ],
- María del Carmen Cuadra-Campos
Abstract
Original ArticleConscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
Crit Care Sci. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda ,
- María del Carmen Cuadra-Campos
Views241See moreABSTRACT
Objective:
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
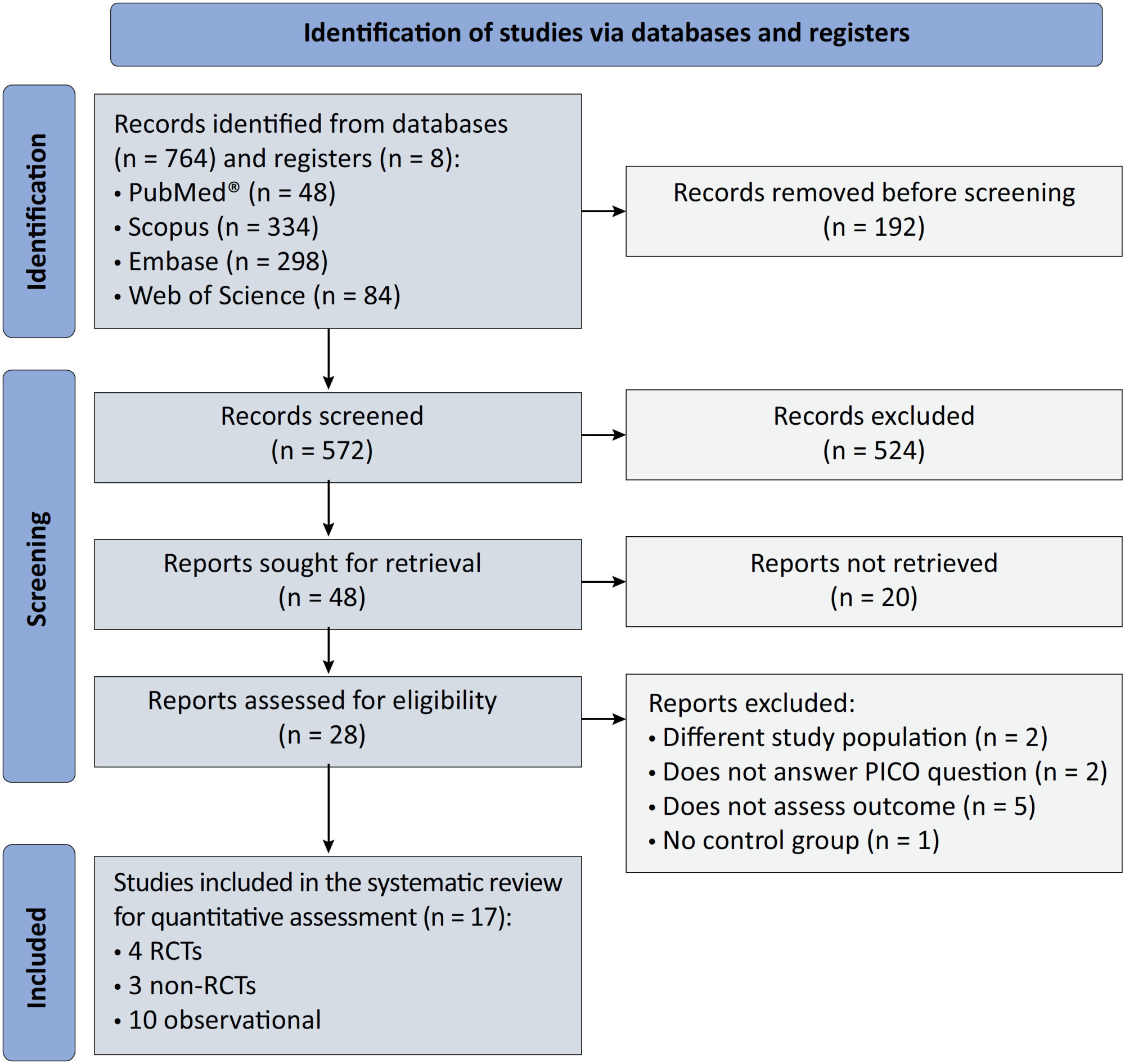
Methods:
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
Results:
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 – 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 – 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 – 0.72 and OR 0.38; 95%CI 0.24 – 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
Conclusion:
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
Views241Abstract
Original ArticleConscious prone positioning in nonintubated COVID-19 patients with acute respiratory distress syndrome: systematic review and meta-analysis
Crit Care Sci. 2024;36:e20240176en
DOI 10.62675/2965-2774.20240176-en
- Gustavo Adolfo Vásquez-Tirado ,
- Edinson Dante Meregildo-Rodríguez ,
- Martha Genara Asmat-Rubio ,
- María José Salazar-Castillo ,
- Claudia Vanessa Quispe-Castañeda ,
- María del Carmen Cuadra-Campos
Views241See moreABSTRACT
Objective:
To systematically review the effect of the prone position on endotracheal intubation and mortality in nonintubated COVID-19 patients with acute respiratory distress syndrome.
Methods:
We registered the protocol (CRD42021286711) and searched for four databases and gray literature from inception to December 31, 2022. We included observational studies and clinical trials. There was no limit by date or the language of publication. We excluded case reports, case series, studies not available in full text, and those studies that included children < 18-years-old.
Results:
We included ten observational studies, eight clinical trials, 3,969 patients, 1,120 endotracheal intubation events, and 843 deaths. All of the studies had a low risk of bias (Newcastle-Ottawa Scale and Risk of Bias 2 tools). We found that the conscious prone position decreased the odds of endotracheal intubation by 44% (OR 0.56; 95%CI 0.40 – 0.78) and mortality by 43% (OR 0.57; 95%CI 0.39 – 0.84) in nonintubated COVID-19 patients with acute respiratory distress syndrome. This protective effect on endotracheal intubation and mortality was more robust in those who spent > 8 hours/day in the conscious prone position (OR 0.43; 95%CI 0.26 – 0.72 and OR 0.38; 95%CI 0.24 – 0.60, respectively). The certainty of the evidence according to the GRADE criteria was moderate.
Conclusion:
The conscious prone position decreased the odds of endotracheal intubation and mortality, especially when patients spent over 8 hours/day in the conscious prone position and treatment in the intensive care unit. However, our results should be cautiously interpreted due to limitations in evaluating randomized clinical trials, nonrandomized clinical trials and observational studies. However, despite systematic reviews with meta-analyses of randomized clinical trials, we must keep in mind that these studies remain heterogeneous from a clinical and methodological point of view.
- Gustavo Adolfo Vásquez-Tirado
-
Correspondence
Reply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho , [ … ],
- Bruna Ziegler
Abstract
CorrespondenceReply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240012en
DOI 10.62675/2965-2774.20240012-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views24Dear editor, We appreciate the interesting and thoughtful critique provided by Finsterer et al. in the letter to the editor regarding our article titled “Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit”.() We would like to address the raised concerns and provide additional clarification […]See moreViews24Abstract
CorrespondenceReply to: Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit
Crit Care Sci. 2024;36:e20240012en
DOI 10.62675/2965-2774.20240012-en
- Fernando Nataniel Vieira ,
- Raquel Bortoluzzi Bertazzo ,
- Gabriela Carvalho Nascimento ,
- Mariluce Anderle ,
- Ana Cláudia Coelho ,
- Fabiana de Oliveira Chaise,
- Jaqueline da Silva Fink ,
- Wagner Luis Nedel ,
- Bruna Ziegler
Views24Dear editor, We appreciate the interesting and thoughtful critique provided by Finsterer et al. in the letter to the editor regarding our article titled “Association between rectus femoris cross-sectional area and diaphragmatic excursion with weaning of tracheostomized patients in the intensive care unit”.() We would like to address the raised concerns and provide additional clarification […]See more - Fernando Nataniel Vieira
-
Viewpoint
Why the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-pt
Views239The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See moreViews239Abstract
ViewpointWhy the Sequential Organ Failure Assessment score needs updating?
Crit Care Sci. 2024;36:e20240296en
DOI 10.62675/2965-2774.20240296-pt
Views239The Sequential Organ Failure Assessment (SOFA) score was developed almost 30 years ago. It rapidly became one of the most widely used scoring systems in intensive care, both for clinical practice and research,(,) and remains one of the most cited scores in our speciality. Since its original description, there have been substantial changes in clinical […]See more -
Delirium and sleep quality in the intensive care unit: the role of melatonin
Crit Care Sci. 2024;36:e20240083en
Abstract
Delirium and sleep quality in the intensive care unit: the role of melatonin
Crit Care Sci. 2024;36:e20240083en
DOI 10.62675/2965-2774.20240083-en
Views62CORRELATION BETWEEN DELIRIUM AND SLEEP DISORDERS Patients in intensive care units (ICUs) frequently face challenges related to delirium and sleep disturbances.() Despite extensive research in recent years, delirium remains a complex condition with uncertain pathophysiology, and its occurrence is associated with worse outcomes as well as longer durations cognitive and functional impairment.(,) Although no study […]See moreViews62Abstract
Delirium and sleep quality in the intensive care unit: the role of melatonin
Crit Care Sci. 2024;36:e20240083en
DOI 10.62675/2965-2774.20240083-en
Views62CORRELATION BETWEEN DELIRIUM AND SLEEP DISORDERS Patients in intensive care units (ICUs) frequently face challenges related to delirium and sleep disturbances.() Despite extensive research in recent years, delirium remains a complex condition with uncertain pathophysiology, and its occurrence is associated with worse outcomes as well as longer durations cognitive and functional impairment.(,) Although no study […]See more -
Original Article
Association of biomarkers with successful ventilatory weaning in COVID-19 patients: an observational study
Crit Care Sci. 2024;36:e20240158en
Abstract
Original ArticleAssociation of biomarkers with successful ventilatory weaning in COVID-19 patients: an observational study
Crit Care Sci. 2024;36:e20240158en
DOI 10.62675/2965-2774.20240158-en
Views52ABSTRACT
Objective:
To evaluate the association of biomarkers with successful ventilatory weaning in COVID-19 patients.
Methods:
An observational, retrospective, and single-center study was conducted between March 2020 and April 2021. C-reactive protein, total lymphocytes, and the neutrophil/lymphocyte ratio were evaluated during attrition and extubation, and the variation in these biomarker values was measured. The primary outcome was successful extubation. ROC curves were drawn to find the best cutoff points for the biomarkers based on sensitivity and specificity. Statistical analysis was performed using logistic regression.
Results:
Of the 2,377 patients admitted to the intensive care unit, 458 were included in the analysis, 356 in the Successful Weaning Group and 102 in the Failure Group. The cutoff points found from the ROC curves were −62.4% for C-reactive protein, +45.7% for total lymphocytes, and −32.9% for neutrophil/lymphocyte ratio. These points were significantly associated with greater extubation success. In the multivariate analysis, only C-reactive protein variation remained statistically significant (OR 2.6; 95%CI 1.51 – 4.5; p < 0.001).
Conclusion:
In this study, a decrease in C-reactive protein levels was associated with successful extubation in COVID-19 patients. Total lymphocytes and the neutrophil/lymphocyte ratio did not maintain the association after multivariate analysis. However, a decrease in C-reactive protein levels should not be used as a sole variable to identify COVID-19 patients suitable for weaning; as in our study, the area under the ROC curve demonstrated poor accuracy in discriminating extubation outcomes, with low sensitivity and specificity.
Keywords:Airway extubationartificialBiomarkersCoronavirus infectionsCOVID-19Intensive care unitsintratrachealIntubationRespirationVentilator weaningSee moreViews52Abstract
Original ArticleAssociation of biomarkers with successful ventilatory weaning in COVID-19 patients: an observational study
Crit Care Sci. 2024;36:e20240158en
DOI 10.62675/2965-2774.20240158-en
Views52ABSTRACT
Objective:
To evaluate the association of biomarkers with successful ventilatory weaning in COVID-19 patients.
Methods:
An observational, retrospective, and single-center study was conducted between March 2020 and April 2021. C-reactive protein, total lymphocytes, and the neutrophil/lymphocyte ratio were evaluated during attrition and extubation, and the variation in these biomarker values was measured. The primary outcome was successful extubation. ROC curves were drawn to find the best cutoff points for the biomarkers based on sensitivity and specificity. Statistical analysis was performed using logistic regression.
Results:
Of the 2,377 patients admitted to the intensive care unit, 458 were included in the analysis, 356 in the Successful Weaning Group and 102 in the Failure Group. The cutoff points found from the ROC curves were −62.4% for C-reactive protein, +45.7% for total lymphocytes, and −32.9% for neutrophil/lymphocyte ratio. These points were significantly associated with greater extubation success. In the multivariate analysis, only C-reactive protein variation remained statistically significant (OR 2.6; 95%CI 1.51 – 4.5; p < 0.001).
Conclusion:
In this study, a decrease in C-reactive protein levels was associated with successful extubation in COVID-19 patients. Total lymphocytes and the neutrophil/lymphocyte ratio did not maintain the association after multivariate analysis. However, a decrease in C-reactive protein levels should not be used as a sole variable to identify COVID-19 patients suitable for weaning; as in our study, the area under the ROC curve demonstrated poor accuracy in discriminating extubation outcomes, with low sensitivity and specificity.
Keywords:Airway extubationartificialBiomarkersCoronavirus infectionsCOVID-19Intensive care unitsintratrachealIntubationRespirationVentilator weaningSee more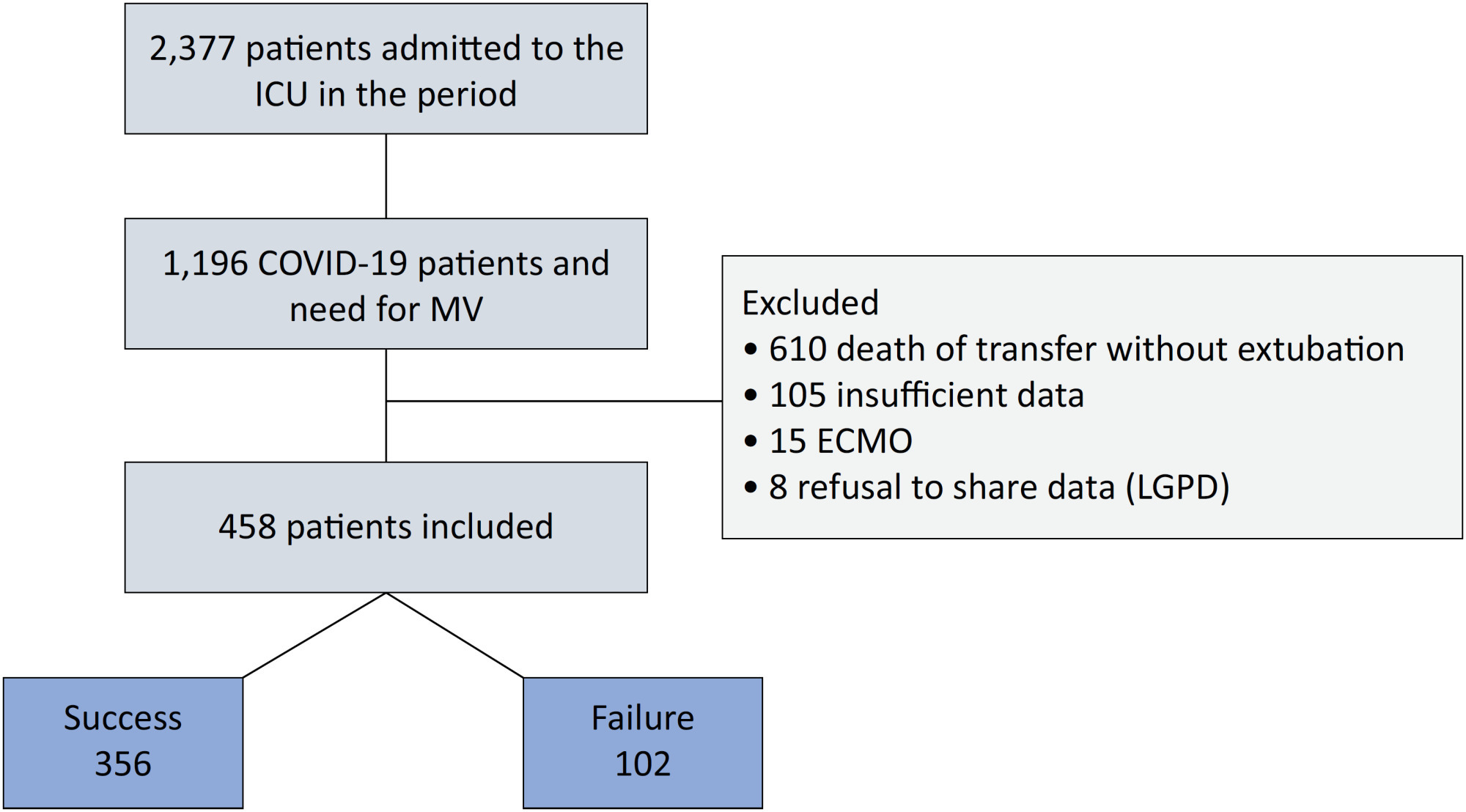
-
Clinical Report
Prospective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini , [ … ],
- Fernando Godinho Zampieri
Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views76ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee moreViews76Abstract
Clinical ReportProspective, randomized, controlled trial assessing the effects of a driving pressure–limiting strategy for patients with acute respiratory distress syndrome due to community-acquired pneumonia (STAMINA trial): protocol and statistical analysis plan
Crit Care Sci. 2024;36:e20240210en
DOI 10.62675/2965-2774.20240210-en
- ,
- Israel Silva Maia ,
- Fernando Azevedo Medrado Jr ,
- Lucas Tramujas ,
- Bruno Martins Tomazini ,
- Júlia Souza Oliveira,
- Erica Regina Ribeiro Sady ,
- Letícia Galvão Barbante,
- Marina Lazzari Nicola ,
- Rodrigo Magalhães Gurgel,
- Lucas Petri Damiani ,
- Karina Leal Negrelli,
- Tamiris Abait Miranda,
- Eliana Santucci ,
- Nanci Valeis ,
- Ligia Nasi Laranjeira,
- Glauco Adrieno Westphal ,
- Ruthy Perotto Fernandes,
- Cássio Luis Zandonai ,
- Mariangela Pimentel Pincelli ,
- Rodrigo Cruvinel Figueiredo,
- Cíntia Loss Sartori Bustamante,
- Luiz Fernando Norbin,
- Emerson Boschi ,
- Rafael Lessa,
- Marcelo Pereira Romano ,
- Mieko Cláudia Miura ,
- Meton Soares de Alencar Filho ,
- Vicente Cés de Souza Dantas ,
- Priscilla Alves Barreto,
- Mauro Esteves Hernandes ,
- Cintia Magalhães Carvalho Grion ,
- Alexandre Sanches Laranjeira,
- Ana Luiza Mezzaroba ,
- Marina Bahl ,
- Ana Carolina Starke ,
- Rodrigo Santos Biondi ,
- Felipe Dal-Pizzol ,
- Eliana Bernadete Caser,
- Marlus Muri Thompson,
- Andrea Allegrini Padial,
- Viviane Cordeiro Veiga ,
- Rodrigo Thot Leite,
- Gustavo Araújo,
- Mário Guimarães,
- Priscilla de Aquino Martins ,
- Fábio Holanda Lacerda ,
- Conrado Roberto Hoffmann Filho ,
- Livia Melro ,
- Eduardo Pacheco,
- Gustavo Adolfo Ospina-Táscon ,
- Juliana Carvalho Ferreira ,
- Fabricio Jocundo Calado Freires ,
- Flávia Ribeiro Machado ,
- Alexandre Biasi Cavalcanti ,
- Fernando Godinho Zampieri
Views76ABSTRACT
Background:
Driving pressure has been suggested to be the main driver of ventilator-induced lung injury and mortality in observational studies of acute respiratory distress syndrome. Whether a driving pressure-limiting strategy can improve clinical outcomes is unclear.
Objective:
To describe the protocol and statistical analysis plan that will be used to test whether a driving pressure-limiting strategy including positive end-expiratory pressure titration according to the best respiratory compliance and reduction in tidal volume is superior to a standard strategy involving the use of the ARDSNet low-positive end-expiratory pressure table in terms of increasing the number of ventilator-free days in patients with acute respiratory distress syndrome due to community-acquired pneumonia.
Methods:
The ventilator STrAtegy for coMmunIty acquired pNeumoniA (STAMINA) study is a randomized, multicenter, open-label trial that compares a driving pressure-limiting strategy to the ARDSnet low-positive end-expiratory pressure table in patients with moderate-to-severe acute respiratory distress syndrome due to community-acquired pneumonia admitted to intensive care units. We expect to recruit 500 patients from 20 Brazilian and 2 Colombian intensive care units. They will be randomized to a driving pressure-limiting strategy group or to a standard strategy using the ARDSNet low-positive end-expiratory pressure table. In the driving pressure-limiting strategy group, positive end-expiratory pressure will be titrated according to the best respiratory system compliance.
Outcomes:
The primary outcome is the number of ventilator-free days within 28 days. The secondary outcomes are in-hospital and intensive care unit mortality and the need for rescue therapies such as extracorporeal life support, recruitment maneuvers and inhaled nitric oxide.
Conclusion:
STAMINA is designed to provide evidence on whether a driving pressure-limiting strategy is superior to the ARDSNet low-positive end-expiratory pressure table strategy for increasing the number of ventilator-free days within 28 days in patients with moderate-to-severe acute respiratory distress syndrome. Here, we describe the rationale, design and status of the trial.
Keywords:Extracorporeal membrane oxygenationPneumoniaPositive pressure respirationRespiration, artificialRespiratory distress syndromeVentilator-induced lung injurySee more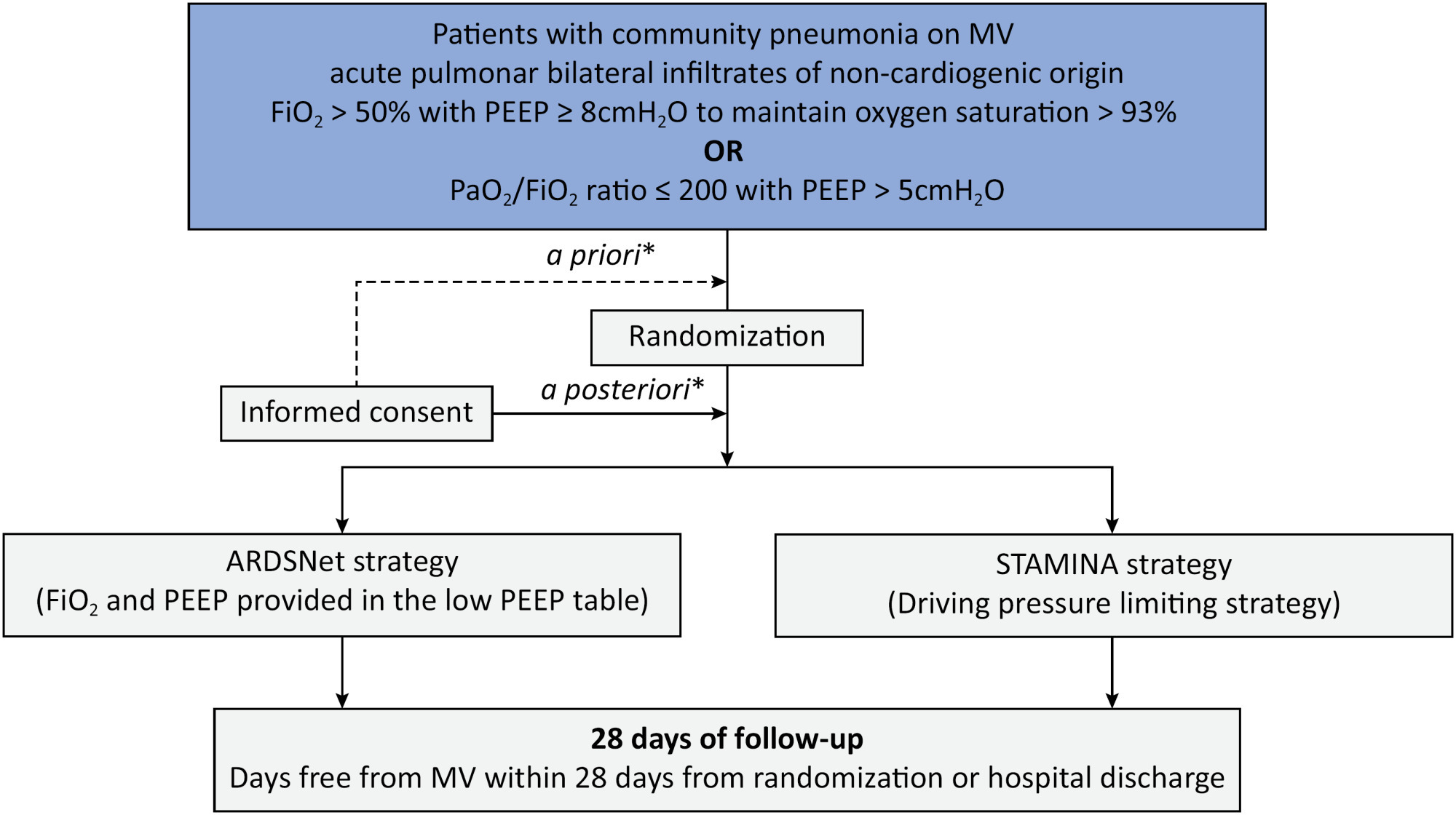
-
Research Letter
COVID-19 underpinning the inverse equity hypothesis between public and private health care in Brazil
Crit Care Sci. 2024;36:e20240294en
Abstract
Research LetterCOVID-19 underpinning the inverse equity hypothesis between public and private health care in Brazil
Crit Care Sci. 2024;36:e20240294en
DOI 10.62675/2965-2774.20240294-pt
Views37Since 1990, the Brazilian public health care system, known as the Unified Health System (SUS – Sistema Único de Saúde), has provided free health care services to all individuals throughout the country. However, approximately 24.9% of the Brazilian population has the financial means to afford private health care alternatives.() Equity, a fundamental principle of SUS, […]See moreViews37Abstract
Research LetterCOVID-19 underpinning the inverse equity hypothesis between public and private health care in Brazil
Crit Care Sci. 2024;36:e20240294en
DOI 10.62675/2965-2774.20240294-pt
Views37Since 1990, the Brazilian public health care system, known as the Unified Health System (SUS – Sistema Único de Saúde), has provided free health care services to all individuals throughout the country. However, approximately 24.9% of the Brazilian population has the financial means to afford private health care alternatives.() Equity, a fundamental principle of SUS, […]See more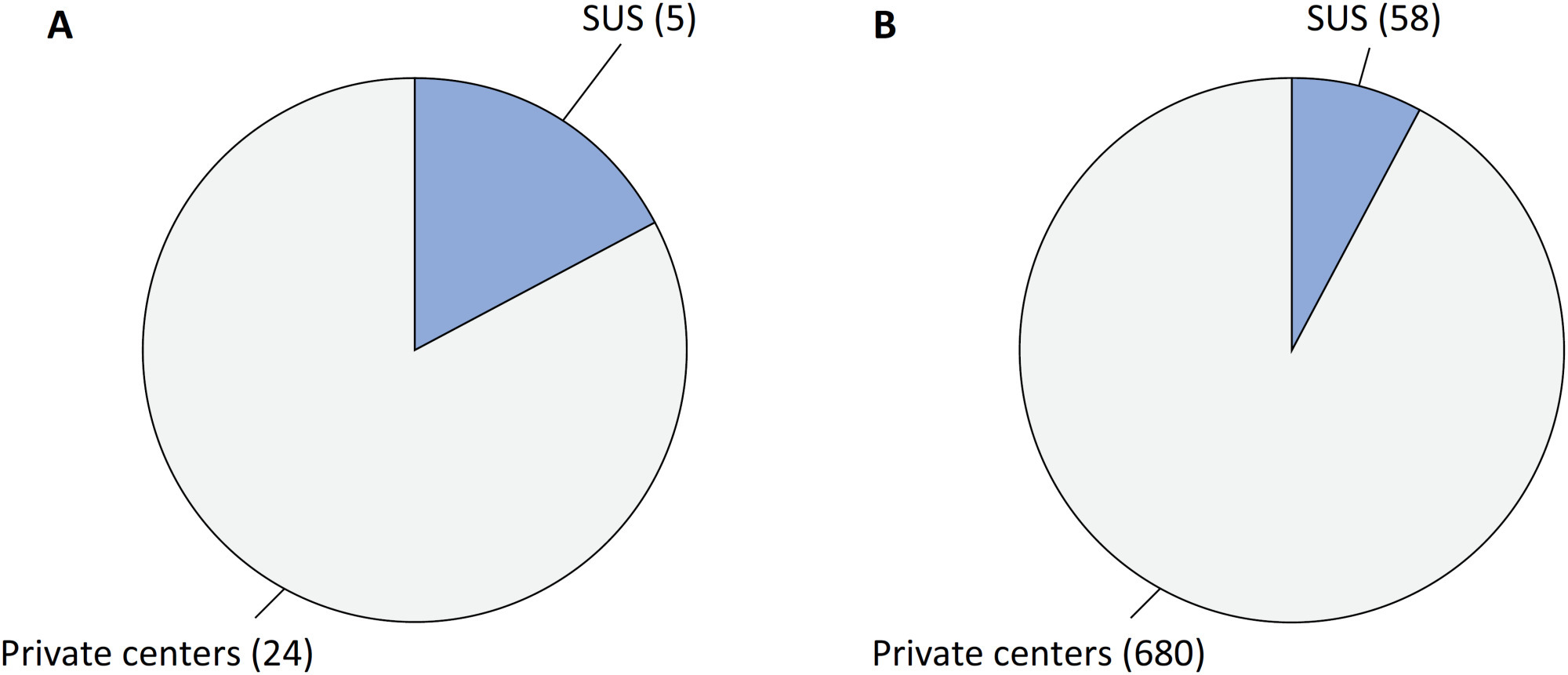
-
Original Article
Alternative approaches to analyzing ventilator-free days, mortality and duration of ventilation in critical care research
Crit Care Sci. 2024;36:e20240246en
Abstract
Original ArticleAlternative approaches to analyzing ventilator-free days, mortality and duration of ventilation in critical care research
Crit Care Sci. 2024;36:e20240246en
DOI 10.62675/2965-2774.20240246-en
Views10See moreABSTRACT
Objective:
To discuss the strengths and limitations of ventilator-free days and to provide a comprehensive discussion of the different analytic methods for analyzing and interpreting this outcome.
Methods:
Using simulations, the power of different analytical methods was assessed, namely: quantile (median) regression, cumulative logistic regression, generalized pairwise comparison, conditional approach and truncated approach. Overall, 3,000 simulations of a two-arm trial with n = 300 per arm were computed using a two-sided alternative hypothesis and a type I error rate of α = 0.05.
Results:
When considering power, median regression did not perform well in studies where the treatment effect was mainly driven by mortality. Median regression performed better in situations with a weak effect on mortality but a strong effect on duration, duration only, and moderate mortality and duration. Cumulative logistic regression was found to produce similar power to the Wilcoxon rank-sum test across all scenarios, being the best strategy for the scenarios of moderate mortality and duration, weak mortality and strong duration, and duration only.
Conclusion:
In this study, we describe the relative power of new methods for analyzing ventilator-free days in critical care research. Our data provide validation and guidance for the use of the cumulative logistic model, median regression, generalized pairwise comparisons, and the conditional and truncated approach in specific scenarios.
Views10Abstract
Original ArticleAlternative approaches to analyzing ventilator-free days, mortality and duration of ventilation in critical care research
Crit Care Sci. 2024;36:e20240246en
DOI 10.62675/2965-2774.20240246-en
Views10See moreABSTRACT
Objective:
To discuss the strengths and limitations of ventilator-free days and to provide a comprehensive discussion of the different analytic methods for analyzing and interpreting this outcome.
Methods:
Using simulations, the power of different analytical methods was assessed, namely: quantile (median) regression, cumulative logistic regression, generalized pairwise comparison, conditional approach and truncated approach. Overall, 3,000 simulations of a two-arm trial with n = 300 per arm were computed using a two-sided alternative hypothesis and a type I error rate of α = 0.05.
Results:
When considering power, median regression did not perform well in studies where the treatment effect was mainly driven by mortality. Median regression performed better in situations with a weak effect on mortality but a strong effect on duration, duration only, and moderate mortality and duration. Cumulative logistic regression was found to produce similar power to the Wilcoxon rank-sum test across all scenarios, being the best strategy for the scenarios of moderate mortality and duration, weak mortality and strong duration, and duration only.
Conclusion:
In this study, we describe the relative power of new methods for analyzing ventilator-free days in critical care research. Our data provide validation and guidance for the use of the cumulative logistic model, median regression, generalized pairwise comparisons, and the conditional and truncated approach in specific scenarios.
-
Clinical Report
Topical glyceryl trinitrate to increase radial artery diameter in neonates: study protocol for a randomized controlled trial
Crit Care Sci. 2024;36:e20240235en
Abstract
Clinical ReportTopical glyceryl trinitrate to increase radial artery diameter in neonates: study protocol for a randomized controlled trial
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Views21ABSTRACT
Background:
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
Methods/Design:
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children’s Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
Discussion:
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.
Keywords:Catheterization, peripheralInfantInfant, newbornIntensive care units, neonatalNitroglycerinRadial arterySee moreViews21Abstract
Clinical ReportTopical glyceryl trinitrate to increase radial artery diameter in neonates: study protocol for a randomized controlled trial
Crit Care Sci. 2024;36:e20240235en
DOI 10.62675/2965-2774.20240235-pt
Views21ABSTRACT
Background:
Newborn infants admitted to the neonatal intensive care unit require arterial cannulation for hemodynamic monitoring and blood sampling. Arterial access is achieved through catheterization of umbilical or peripheral arteries. Peripheral artery cannulation is performed in critically ill newborns, but artery localization and cannulation is often challenging and unsuccessful. Therefore, increasing the internal diameter and preventing vasospasm are important for successful peripheral artery cannulation in neonates. Topical glyceryl trinitrate has the potential to increase cannulation success by relaxing arterial smooth muscles and thus increasing the internal diameter. We aim to conduct a pilot randomized controlled trial to evaluate the efficacy and safety of topycal glyceryl trinitrate in increasing the diameter of the radial artery in neonates.
Methods/Design:
This study will be a single-center, observer-blind, randomized, placebo-controlled trial conducted in the neonatal intensive care unit of Perth Children’s Hospital, Western Australia. A total of 60 infants born at >34 weeks of gestation who are admitted for elective surgery or medical reasons and for whom a peripheral arterial line is needed for sampling or blood pressure monitoring will be recruited after informed parental consent is obtained. The primary outcome will be the change in radial arterial diameter from baseline to postintervention. Secondary outcomes will be the absolute and percentage change from baseline in the radial arterial diameter in both limbs and safety (hypotension and methemoglobinemia).
Discussion:
This will be the first randomized controlled trial evaluating the use of topical glyceryl trinitrate to facilitate peripheral artery cannulation in neonates. If our pilot randomized controlled trial confirms the benefits of glyceryl trinitrate patches, it will pave the way for large multicenter randomized controlled trials in this field.
Keywords:Catheterization, peripheralInfantInfant, newbornIntensive care units, neonatalNitroglycerinRadial arterySee more
2024, Volume 36