-
Editorial
Already a long way… and a longer way ahead: our future challenges
Rev Bras Ter Intensiva. 2013;25(3):181-183
Abstract
EditorialAlready a long way… and a longer way ahead: our future challenges
Rev Bras Ter Intensiva. 2013;25(3):181-183
DOI 10.5935/0103-507X.20130031
Views0Our journal, Revista Brasileira de Terapia Intensiva – RBTI, is now indexed in PubMed/MedLine. This achievement represents a critical step for the Brazilian-Portuguese-Latin American intensive care community. Certainly a well-deserved recognition of our quality and efforts in this crusade. We do expect an increase in our submissions, coming not only from Brazil and Portugal but […]See moreViews0

Abstract
EditorialAlready a long way… and a longer way ahead: our future challenges
Rev Bras Ter Intensiva. 2013;25(3):181-183
DOI 10.5935/0103-507X.20130031
Views0Our journal, Revista Brasileira de Terapia Intensiva – RBTI, is now indexed in PubMed/MedLine. This achievement represents a critical step for the Brazilian-Portuguese-Latin American intensive care community. Certainly a well-deserved recognition of our quality and efforts in this crusade.We do expect an increase in our submissions, coming not only from Brazil and Portugal but also […]See more -
Editorial
Urine assessment in the critically ill: a matter of both quantity and quality
Rev Bras Ter Intensiva. 2013;25(3):184-185
Abstract
EditorialUrine assessment in the critically ill: a matter of both quantity and quality
Rev Bras Ter Intensiva. 2013;25(3):184-185
DOI 10.5935/0103-507X.20130032
Views0In this issue of Revista Brasileira de Terapia Intensiva, Masevicius et al.( ) reported on the behavior of the plasma chloride concentration ([Cl–]plasma) of 148 consecutive postoperative patients in the first 24 hours after their intensive care unit (ICU) admission. The authors’ major finding was that, at the end of the first day in the […]See moreViews0Abstract
EditorialUrine assessment in the critically ill: a matter of both quantity and quality
Rev Bras Ter Intensiva. 2013;25(3):184-185
DOI 10.5935/0103-507X.20130032
Views0In this issue of Revista Brasileira de Terapia Intensiva, Masevicius et al.( ) reported on the behavior of the plasma chloride concentration ([Cl–]plasma) of 148 consecutive postoperative patients in the first 24 hours after their intensive care unit (ICU) admission. The authors’ major finding was that, at the end of the first day in the […]See more -
Editorial
Implementing sedation protocols: closing the evidence-practice gap
Rev Bras Ter Intensiva. 2013;25(3):186-187
Abstract
EditorialImplementing sedation protocols: closing the evidence-practice gap
Rev Bras Ter Intensiva. 2013;25(3):186-187
DOI 10.5935/0103-507X.20130033
Views0Sedation and analgesia are frequently used in the critical care unit. Pain has already been described as the “fifth vital sign,” and most people describe experiencing pain as a source of great stress during an intensive care unit (ICU) stay.( , ) Sedation can be used to ease discomfort, to facilitate adaptation to mechanical ventilation, […]See moreViews0Abstract
EditorialImplementing sedation protocols: closing the evidence-practice gap
Rev Bras Ter Intensiva. 2013;25(3):186-187
DOI 10.5935/0103-507X.20130033
Views0Sedation and analgesia are frequently used in the critical care unit. Pain has already been described as the “fifth vital sign,” and most people describe experiencing pain as a source of great stress during an intensive care unit (ICU) stay.( , ) Sedation can be used to ease discomfort, to facilitate adaptation to mechanical ventilation, […]See more -
Original Articles
The implementation of an analgesia-based sedation protocol reduced deep sedation and proved to be safe and feasible in patients on mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):188-196
Abstract
Original ArticlesThe implementation of an analgesia-based sedation protocol reduced deep sedation and proved to be safe and feasible in patients on mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Views0INTRODUCTION:
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
METHODS:
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
RESULTS:
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
CONCLUSIONS:
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Keywords:analgesiaClinical protocolsDeep sedationIntensive care unitsPatient safetyRespiration, artificialSee moreViews0Abstract
Original ArticlesThe implementation of an analgesia-based sedation protocol reduced deep sedation and proved to be safe and feasible in patients on mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):188-196
DOI 10.5935/0103-507X.20130034
Views0INTRODUCTION:
Deep sedation in critically ill patients is associated with a longer duration of mechanical ventilation and a prolonged length of stay in the intensive care unit. Several protocols have been used to improve these outcomes. We implement and evaluate an analgesia-based, goal-directed, nurse-driven sedation protocol used to treat critically ill patients who receive mechanical ventilation.
METHODS:
We performed a prospective, two-phase (before-after), non-randomized multicenter study that involved 13 intensive care units in Chile. After an observational phase (observational group, n=155), we designed, implemented and evaluated an analgesia-based, goal-directed, nurse-driven sedation protocol (intervention group, n=132) to treat patients who required mechanical ventilation for more than 48 hours. The primary outcome was to achieve ventilator-free days by day 28.
RESULTS:
The proportion of patients in deep sedation or in a coma decreased from 55.2% to 44.0% in the interventional group. Agitation did not change between the periods and remained approximately 7%. Ventilator-free days to day 28, length of stay in the intensive care unit and mortality were similar in both groups. At one year, post-traumatic stress disorder symptoms in survivors were similar in both groups.
CONCLUSIONS:
We designed and implemented an analgesia-based, goal-directed, nurse-driven sedation protocol in Chile. Although there was no improvement in major outcomes, we observed that the present protocol was safe and feasible and that it resulted in decreased periods of deep sedation without increasing agitation.
Keywords:analgesiaClinical protocolsDeep sedationIntensive care unitsPatient safetyRespiration, artificialSee more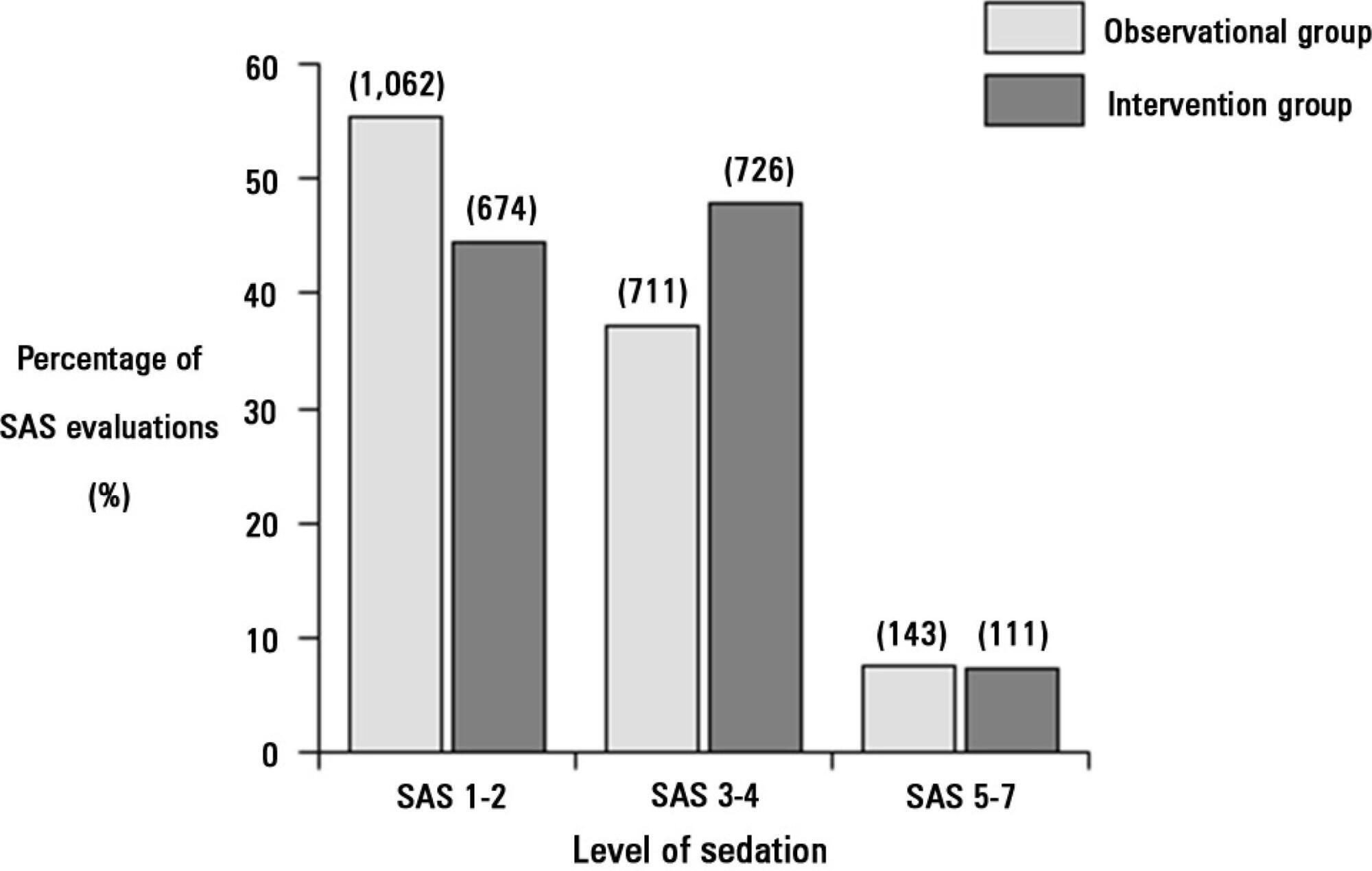
-
Original Articles
Urinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
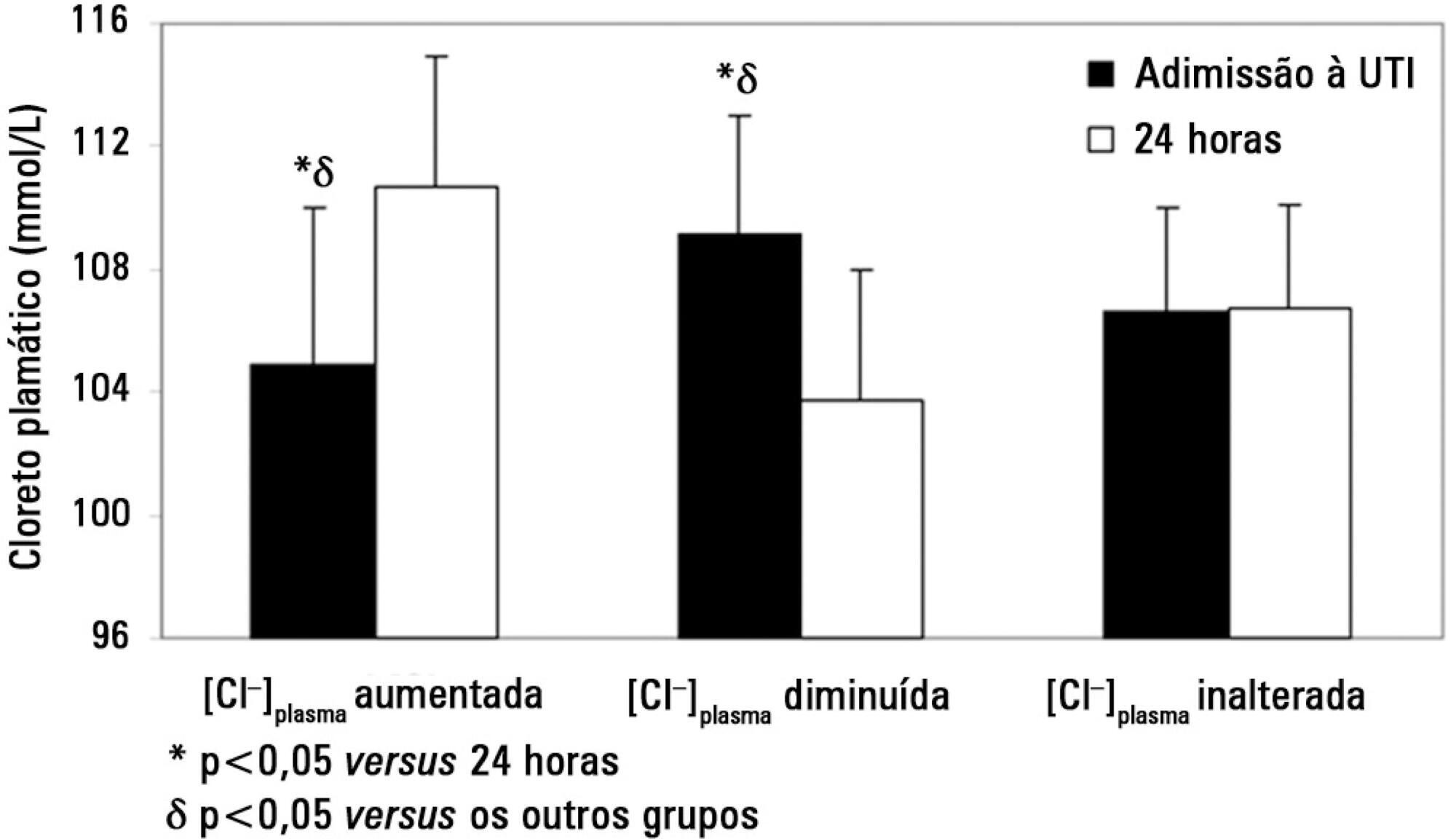
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
Views1Abstract
Original ArticlesUrinary strong ion difference is a major determinant of plasma chloride concentration changes in postoperative patients
Rev Bras Ter Intensiva. 2013;25(3):197-204
DOI 10.5935/0103-507X.20130035
Views1See moreOBJECTIVE:
To show that alterations in the plasma chloride concentration ([Cl–]plasma) during the postoperative period are largely dependent on the urinary strong ion difference ([SID]urine=[Na+]urine+[K+]urine-[Cl-]urine) and not on differences in fluid therapy.
METHODS:
Measurements were performed at intensive care unit admission and 24 hours later in a total of 148 postoperative patients. Patients were assigned into one of three groups according to the change in [Cl–]plasma at the 24 hours time point: increased [Cl–]plasma (n=39), decreased [Cl–]plasma (n=56) or unchanged [Cl–]plasma (n=53).
RESULTS:
On admission, the increased [Cl–]plasma group had a lower [Cl–]plasma (105±5 versus 109±4 and 106±3mmol/L, p<0.05), a higher plasma anion gap concentration ([AG]plasma) and a higher strong ion gap concentration ([SIG]). After 24 hours, the increased [Cl–]plasma group showed a higher [Cl–]plasma (111±4 versus 104±4 and 107±3mmol/L, p<0.05) and lower [AG]plasma and [SIG]. The volume and [SID] of administered fluids were similar between groups except that the [SID]urine was higher (38±37 versus 18±22 and 23±18mmol/L, p<0.05) in the increased [Cl–]plasma group at the 24 hours time point. A multiple linear regression analysis showed that the [Cl–]plasma on admission and [SID]urine were independent predictors of the variation in [Cl–]plasma 24 hours later.
CONCLUSIONS:
Changes in [Cl–]plasma during the first postoperative day were largely related to [SID]urine and [Cl–]plasma on admission and not to the characteristics of the infused fluids. Therefore, decreasing [SID]urine could be a major mechanism for preventing the development of salineinduced hyperchloremia.
-
Original Articles
Anion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
Abstract
Original ArticlesAnion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
DOI 10.5935/0103-507X.20130036
Views1OBJECTIVE:
Corrected anion gap and strong ion gap are commonly used to estimate unmeasured anions. We evaluated the performance of the anion gap corrected for albumin, phosphate and lactate in predicting strong ion gap in a mixed population of critically ill patients. We hypothesized that anion gap corrected for albumin, phosphate and lactate would be a good predictor of strong ion gap, independent of the presence of metabolic acidosis. In addition, we evaluated the impact of strong ion gap at admission on hospital mortality.
METHODS:
We included 84 critically ill patients. Correlation and agreement between the anion gap corrected for albumin, phosphate and lactate and strong ion gap was evaluated by the Pearson correlation test, linear regression, a Bland-Altman plot and calculating interclass correlation coefficient. Two subgroup analyses were performed: one in patients with base-excess <-2mEq/L (low BE group - lBE) and the other in patients with base-excess >-2mEq/L (high BE group – hBE). A logistic regression was performed to evaluate the association between admission strong ion gap levels and hospital mortality.
RESULTS:
There was a very strong correlation and a good agreement between anion gap corrected for albumin, phosphate and lactate and strong ion gap in the general population (r2=0.94; bias 1.40; limits of agreement -0.75 to 3.57). Correlation was also high in the lBE group (r2=0.94) and in the hBE group (r2=0.92). High levels of strong ion gap were present in 66% of the whole population and 42% of the cases in the hBE group. Strong ion gap was not associated with hospital mortality by logistic regression.
CONCLUSION:
Anion gap corrected for albumin, phosphate and lactate and strong ion gap have an excellent correlation. Unmeasured anions are frequently elevated in critically ill patients with normal base-excess. However, there was no association between unmeasured anions and hospital mortality.
Keywords:Acid-base equilibrium/ physiologyBlood chemical analysisCritical illnessLactate/bloodPhosphate/ bloodPrognosisSerum albumin/bloodSee moreViews1Abstract
Original ArticlesAnion gap corrected for albumin, phosphate and lactate is a good predictor of strong ion gap in critically ill patients: a nested cohort study
Rev Bras Ter Intensiva. 2013;25(3):205-211
DOI 10.5935/0103-507X.20130036
Views1OBJECTIVE:
Corrected anion gap and strong ion gap are commonly used to estimate unmeasured anions. We evaluated the performance of the anion gap corrected for albumin, phosphate and lactate in predicting strong ion gap in a mixed population of critically ill patients. We hypothesized that anion gap corrected for albumin, phosphate and lactate would be a good predictor of strong ion gap, independent of the presence of metabolic acidosis. In addition, we evaluated the impact of strong ion gap at admission on hospital mortality.
METHODS:
We included 84 critically ill patients. Correlation and agreement between the anion gap corrected for albumin, phosphate and lactate and strong ion gap was evaluated by the Pearson correlation test, linear regression, a Bland-Altman plot and calculating interclass correlation coefficient. Two subgroup analyses were performed: one in patients with base-excess <-2mEq/L (low BE group - lBE) and the other in patients with base-excess >-2mEq/L (high BE group – hBE). A logistic regression was performed to evaluate the association between admission strong ion gap levels and hospital mortality.
RESULTS:
There was a very strong correlation and a good agreement between anion gap corrected for albumin, phosphate and lactate and strong ion gap in the general population (r2=0.94; bias 1.40; limits of agreement -0.75 to 3.57). Correlation was also high in the lBE group (r2=0.94) and in the hBE group (r2=0.92). High levels of strong ion gap were present in 66% of the whole population and 42% of the cases in the hBE group. Strong ion gap was not associated with hospital mortality by logistic regression.
CONCLUSION:
Anion gap corrected for albumin, phosphate and lactate and strong ion gap have an excellent correlation. Unmeasured anions are frequently elevated in critically ill patients with normal base-excess. However, there was no association between unmeasured anions and hospital mortality.
Keywords:Acid-base equilibrium/ physiologyBlood chemical analysisCritical illnessLactate/bloodPhosphate/ bloodPrognosisSerum albumin/bloodSee more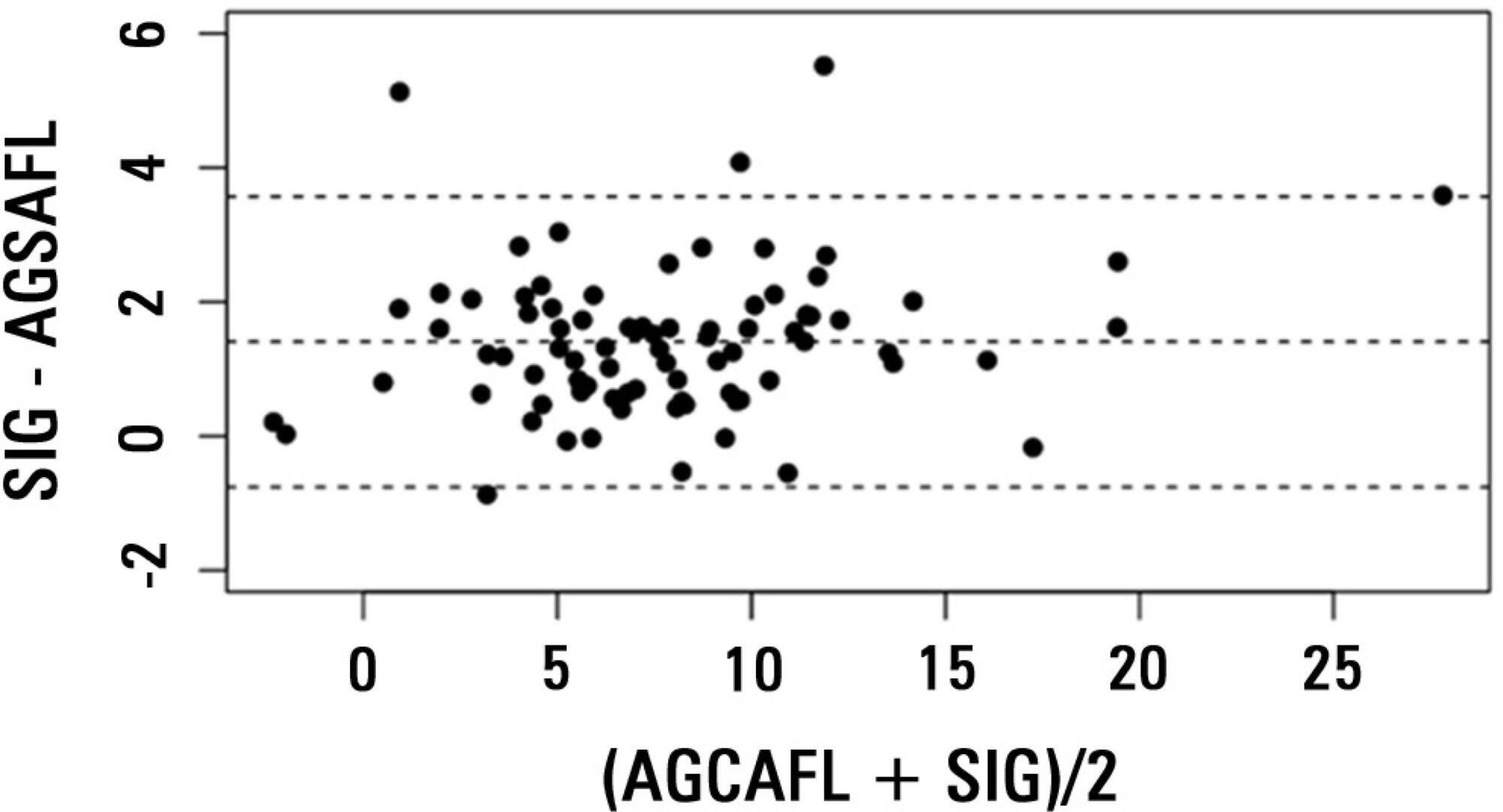
-
Original Articles
Association between the rapid shallow breathing index and extubation success in patients with traumatic brain injury
Rev Bras Ter Intensiva. 2013;25(3):212-217
Abstract
Original ArticlesAssociation between the rapid shallow breathing index and extubation success in patients with traumatic brain injury
Rev Bras Ter Intensiva. 2013;25(3):212-217
DOI 10.5935/0103-507X.20130037
Views0See moreOBJECTIVE:
To investigate the association between the rapid shallow breathing index and successful extubation in patients with traumatic brain injury.
METHODS:
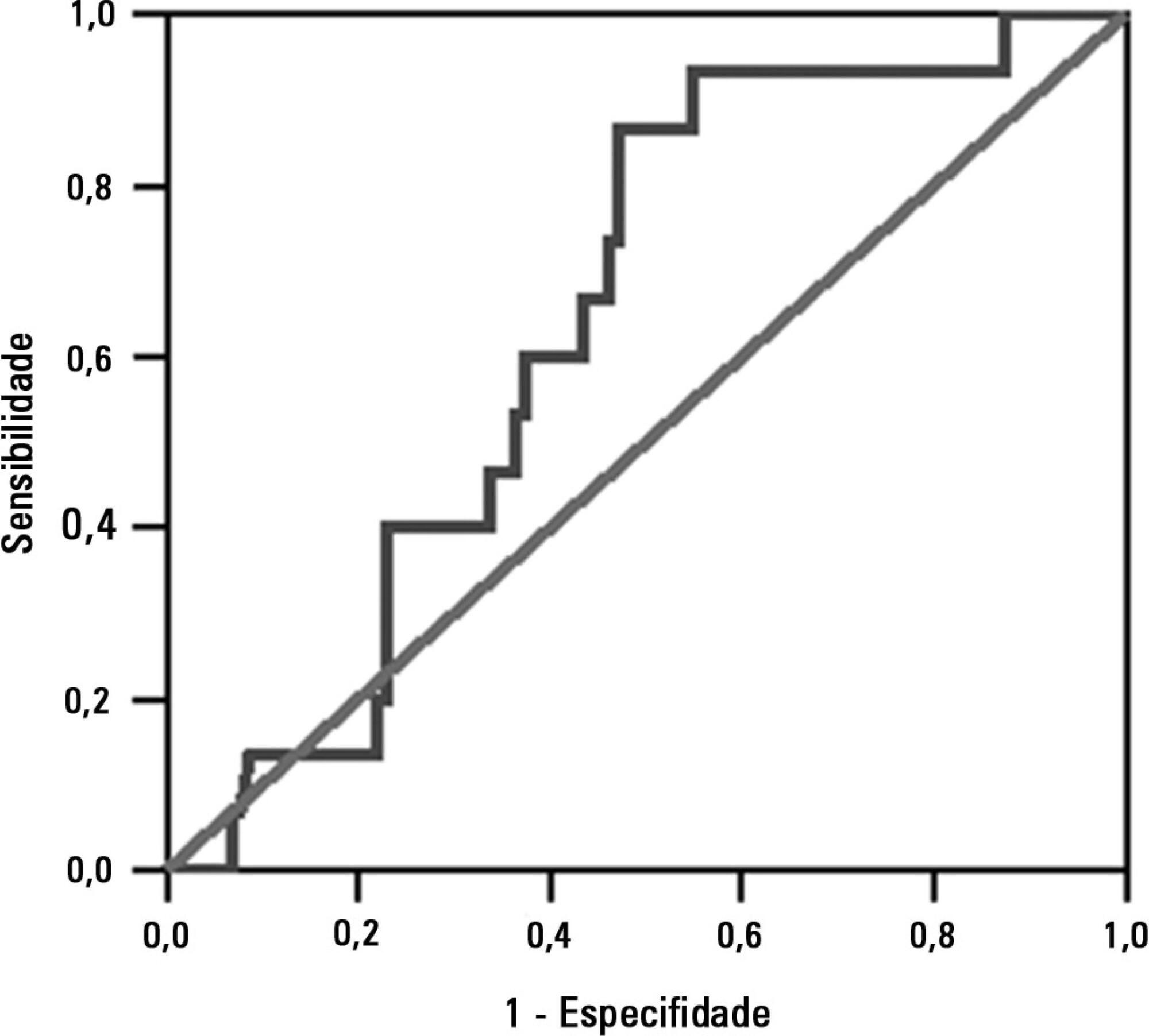
This study was a prospective study conducted in patients with traumatic brain injury of both genders who underwent mechanical ventilation for at least two days and who passed a spontaneous breathing trial. The minute volume and respiratory rate were measured using a ventilometer, and the data were used to calculate the rapid shallow breathing index (respiratory rate/tidal volume). The dependent variable was the extubation outcome: reintubation after up to 48 hours (extubation failure) or not (extubation success). The independent variable was the rapid shallow breathing index measured after a successful spontaneous breathing trial.
RESULTS:
The sample comprised 119 individuals, including 111 (93.3%) males. The average age of the sample was 35.0±12.9 years old. The average duration of mechanical ventilation was 8.1±3.6 days. A total of 104 (87.4%) participants achieved successful extubation. No association was found between the rapid shallow breathing index and extubation success.
CONCLUSION:
The rapid shallow breathing index was not associated with successful extubation in patients with traumatic brain injury.
Views0Abstract
Original ArticlesAssociation between the rapid shallow breathing index and extubation success in patients with traumatic brain injury
Rev Bras Ter Intensiva. 2013;25(3):212-217
DOI 10.5935/0103-507X.20130037
Views0See moreOBJECTIVE:
To investigate the association between the rapid shallow breathing index and successful extubation in patients with traumatic brain injury.
METHODS:
This study was a prospective study conducted in patients with traumatic brain injury of both genders who underwent mechanical ventilation for at least two days and who passed a spontaneous breathing trial. The minute volume and respiratory rate were measured using a ventilometer, and the data were used to calculate the rapid shallow breathing index (respiratory rate/tidal volume). The dependent variable was the extubation outcome: reintubation after up to 48 hours (extubation failure) or not (extubation success). The independent variable was the rapid shallow breathing index measured after a successful spontaneous breathing trial.
RESULTS:
The sample comprised 119 individuals, including 111 (93.3%) males. The average age of the sample was 35.0±12.9 years old. The average duration of mechanical ventilation was 8.1±3.6 days. A total of 104 (87.4%) participants achieved successful extubation. No association was found between the rapid shallow breathing index and extubation success.
CONCLUSION:
The rapid shallow breathing index was not associated with successful extubation in patients with traumatic brain injury.
-
Original Articles
Functional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
Abstract
Original ArticlesFunctional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
Views1See moreOBJECTIVE:
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
METHODS:
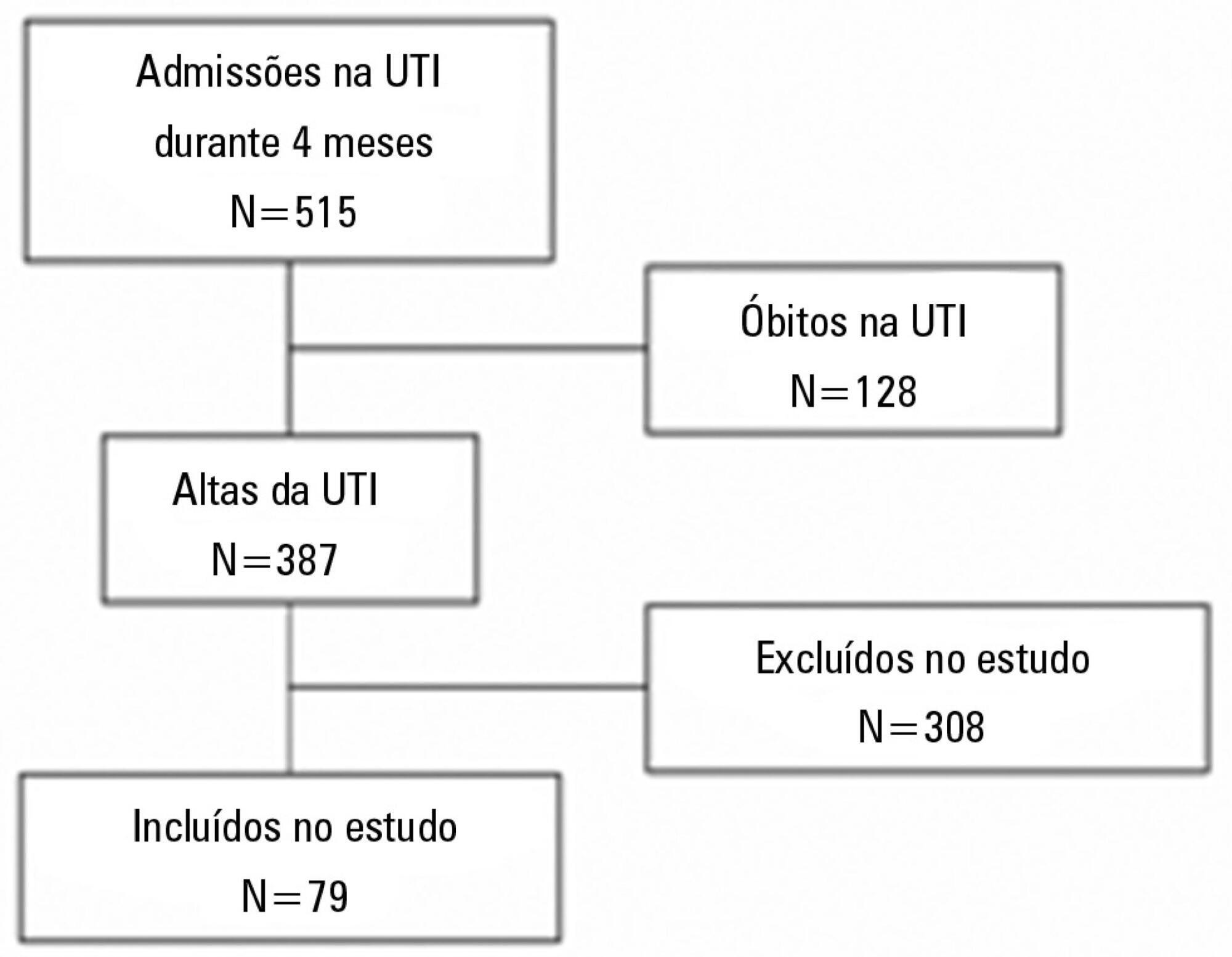
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
RESULTS:
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
CONCLUSIONS:
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
Views1Abstract
Original ArticlesFunctional and psychological features immediately after discharge from an Intensive Care Unit: prospective cohort study
Rev Bras Ter Intensiva. 2013;25(3):218-224
DOI 10.5935/0103-507X.20130038
Views1See moreOBJECTIVE:
To assess the functional and psychological features of patients immediately after discharge from the intensive care unit.
METHODS:
Prospective cohort study. Questionnaires and scales assessing the degree of dependence and functional capacity (modified Barthel and Karnofsky scales) and psychological problems (Hospital Anxiety and Depression Scale), in addition to the Epworth Sleepiness Scale, were administered during interviews conducted over the first week after intensive care unit discharge, to all survivors who had been admitted to this service from August to November 2012 and had remained longer than 72 hours.
RESULTS:
The degree of dependence as measured by the modified Barthel scale increased after intensive care unit discharge compared with the data before admission (57±30 versus 47±36; p<0.001) in all 79 participants. This impairment was homogeneous among all the categories in the modified Barthel scale (p<0.001) in the 64 participants who were independent or partially dependent (Karnofsky score ≥40) before admission. The impairment affected the categories of personal hygiene (p=0.01) and stair climbing (p=0.04) only in the 15 participants who were highly dependent (Karnofsky score <40) before admission. Assessment of the psychological changes identified mood disorders (anxiety and/or depression) in 31% of the sample, whereas sleep disorders occurred in 43.3%.
CONCLUSIONS:
Patients who remained in an intensive care unit for 72 hours or longer exhibited a reduced functional capacity and an increased degree of dependence during the first week after intensive care unit discharge. In addition, the incidence of depressive symptoms, anxiety, and sleep disorders was high among that population.
-
Original Articles
Nursing workload in public and private intensive care units
Rev Bras Ter Intensiva. 2013;25(3):225-232
Abstract
Original ArticlesNursing workload in public and private intensive care units
Rev Bras Ter Intensiva. 2013;25(3):225-232
DOI 10.5935/0103-507X.20130039
Views1OBJECTIVE:
This study sought to compare patients at public and private intensive care units according to the nursing workload and interventions provided.
METHODS:
This retrospective, comparative cohort study included 600 patients admitted to 4 intensive care units in São Paulo. The nursing workload and interventions were assessed using the Nursing Activities Score during the first and last 24 hours of the patient’s stay at the intensive care unit. Pearson’s chi-square test, Fisher’s exact test, the Mann-Whitney test, and Student’s t test were used to compare the patient groups.
RESULTS:
The average Nursing Activities Score upon admission to the intensive care unit was 61.9, with a score of 52.8 upon discharge. Significant differences were found among the patients at public and private intensive care units relative to the average Nursing Activities Score upon admission, as well as for 12 out of 23 nursing interventions performed during the first 24 hours of stay at the intensive care units. The patients at the public intensive care units exhibited a higher average score and overall more frequent nursing interventions, with the exception of those involved in the “care of drains”, “mobilization and positioning”, and “intravenous hyperalimentation”. The groups also differed with regard to the evolution of the Nursing Activities Score among the total case series as well as the groups of survivors from the time of admission to discharge from the intensive care unit.
CONCLUSION:
Patients admitted to public and private intensive care units exhibit differences in their nursing care demands, which may help managers with nursing manpower planning.
Keywords:Hospitals, private/manpowerHospitals, public/manpowerIntensive care unitsNursing staff, hospitalWorkloadSee moreViews1Abstract
Original ArticlesNursing workload in public and private intensive care units
Rev Bras Ter Intensiva. 2013;25(3):225-232
DOI 10.5935/0103-507X.20130039
Views1OBJECTIVE:
This study sought to compare patients at public and private intensive care units according to the nursing workload and interventions provided.
METHODS:
This retrospective, comparative cohort study included 600 patients admitted to 4 intensive care units in São Paulo. The nursing workload and interventions were assessed using the Nursing Activities Score during the first and last 24 hours of the patient’s stay at the intensive care unit. Pearson’s chi-square test, Fisher’s exact test, the Mann-Whitney test, and Student’s t test were used to compare the patient groups.
RESULTS:
The average Nursing Activities Score upon admission to the intensive care unit was 61.9, with a score of 52.8 upon discharge. Significant differences were found among the patients at public and private intensive care units relative to the average Nursing Activities Score upon admission, as well as for 12 out of 23 nursing interventions performed during the first 24 hours of stay at the intensive care units. The patients at the public intensive care units exhibited a higher average score and overall more frequent nursing interventions, with the exception of those involved in the “care of drains”, “mobilization and positioning”, and “intravenous hyperalimentation”. The groups also differed with regard to the evolution of the Nursing Activities Score among the total case series as well as the groups of survivors from the time of admission to discharge from the intensive care unit.
CONCLUSION:
Patients admitted to public and private intensive care units exhibit differences in their nursing care demands, which may help managers with nursing manpower planning.
Keywords:Hospitals, private/manpowerHospitals, public/manpowerIntensive care unitsNursing staff, hospitalWorkloadSee more -
Original Articles
Correlation of the EuroSCORE with the onset of postoperative acute kidney injury in cardiac surgery
Rev Bras Ter Intensiva. 2013;25(3):233-238
Abstract
Original ArticlesCorrelation of the EuroSCORE with the onset of postoperative acute kidney injury in cardiac surgery
Rev Bras Ter Intensiva. 2013;25(3):233-238
DOI 10.5935/0103-507X.20130040
Views0OBJECTIVE:
The objective of this study was to assess the correlation between the European System for Cardiac Operative Risk Evaluation (EuroSCORE) score and the risk of developing acute kidney injury in cardiac surgery patients.
METHODS:
This retrospective study was conducted at a tertiary hospital on consecutive cardiac surgery patients (e.g., valvular, ischemic and congenital heart diseases) between October 2010 and July 2011.
RESULTS:
One hundred patients were assessed. Among the 100 patients, six were excluded, including five because of prior kidney disease or dialysis therapy and one because of incomplete medical records. The primary surgical indications were myocardial revascularization in 55 patients (58.5% of cases) and valve replacement in 28 patients (29.8%). According to the EuroSCORE, 55 patients were classified as high risk (58.5%), 27 patients as medium risk (28.7%) and 12 patients as low risk (12.8%). In the postoperative period, patients were classified with the Risk, Injury, Failure, Loss and End-stage kidney disease (RIFLE) score. Among the 31 patients (33%) who displayed an increase in serum creatinine, 18 patients (19.1%) were classified as RIFLE “R” (risk), seven patients (7.4%) were classified as RIFLE “I” (injury) and six patients (6.5%) were classified as RIFLE “F” (failure). Among the patients who were considered to be high risk according to the EuroSCORE criteria, 24 patients (43.6%) showed acute kidney injury. Among the patients who were classified as medium or low risk, acute kidney injury occurred in 18.5 and 16.6% of the cases, respectively. The correlations between risk stratification (low, medium and high) and the EuroSCORE and postoperative RIFLE scores were statistically significant (p=0.03).
CONCLUSION:
In the studied population, there was a statistically significant correlation between the EuroSCORE and the risk of developing acute kidney injury in the postoperative period after cardiac surgery.
Keywords:Acute kidney injuryPostoperative complicationsRenal dialysisRisk assessmentSeverity of illness indexThoracic surgerySee moreViews0Abstract
Original ArticlesCorrelation of the EuroSCORE with the onset of postoperative acute kidney injury in cardiac surgery
Rev Bras Ter Intensiva. 2013;25(3):233-238
DOI 10.5935/0103-507X.20130040
Views0OBJECTIVE:
The objective of this study was to assess the correlation between the European System for Cardiac Operative Risk Evaluation (EuroSCORE) score and the risk of developing acute kidney injury in cardiac surgery patients.
METHODS:
This retrospective study was conducted at a tertiary hospital on consecutive cardiac surgery patients (e.g., valvular, ischemic and congenital heart diseases) between October 2010 and July 2011.
RESULTS:
One hundred patients were assessed. Among the 100 patients, six were excluded, including five because of prior kidney disease or dialysis therapy and one because of incomplete medical records. The primary surgical indications were myocardial revascularization in 55 patients (58.5% of cases) and valve replacement in 28 patients (29.8%). According to the EuroSCORE, 55 patients were classified as high risk (58.5%), 27 patients as medium risk (28.7%) and 12 patients as low risk (12.8%). In the postoperative period, patients were classified with the Risk, Injury, Failure, Loss and End-stage kidney disease (RIFLE) score. Among the 31 patients (33%) who displayed an increase in serum creatinine, 18 patients (19.1%) were classified as RIFLE “R” (risk), seven patients (7.4%) were classified as RIFLE “I” (injury) and six patients (6.5%) were classified as RIFLE “F” (failure). Among the patients who were considered to be high risk according to the EuroSCORE criteria, 24 patients (43.6%) showed acute kidney injury. Among the patients who were classified as medium or low risk, acute kidney injury occurred in 18.5 and 16.6% of the cases, respectively. The correlations between risk stratification (low, medium and high) and the EuroSCORE and postoperative RIFLE scores were statistically significant (p=0.03).
CONCLUSION:
In the studied population, there was a statistically significant correlation between the EuroSCORE and the risk of developing acute kidney injury in the postoperative period after cardiac surgery.
Keywords:Acute kidney injuryPostoperative complicationsRenal dialysisRisk assessmentSeverity of illness indexThoracic surgerySee more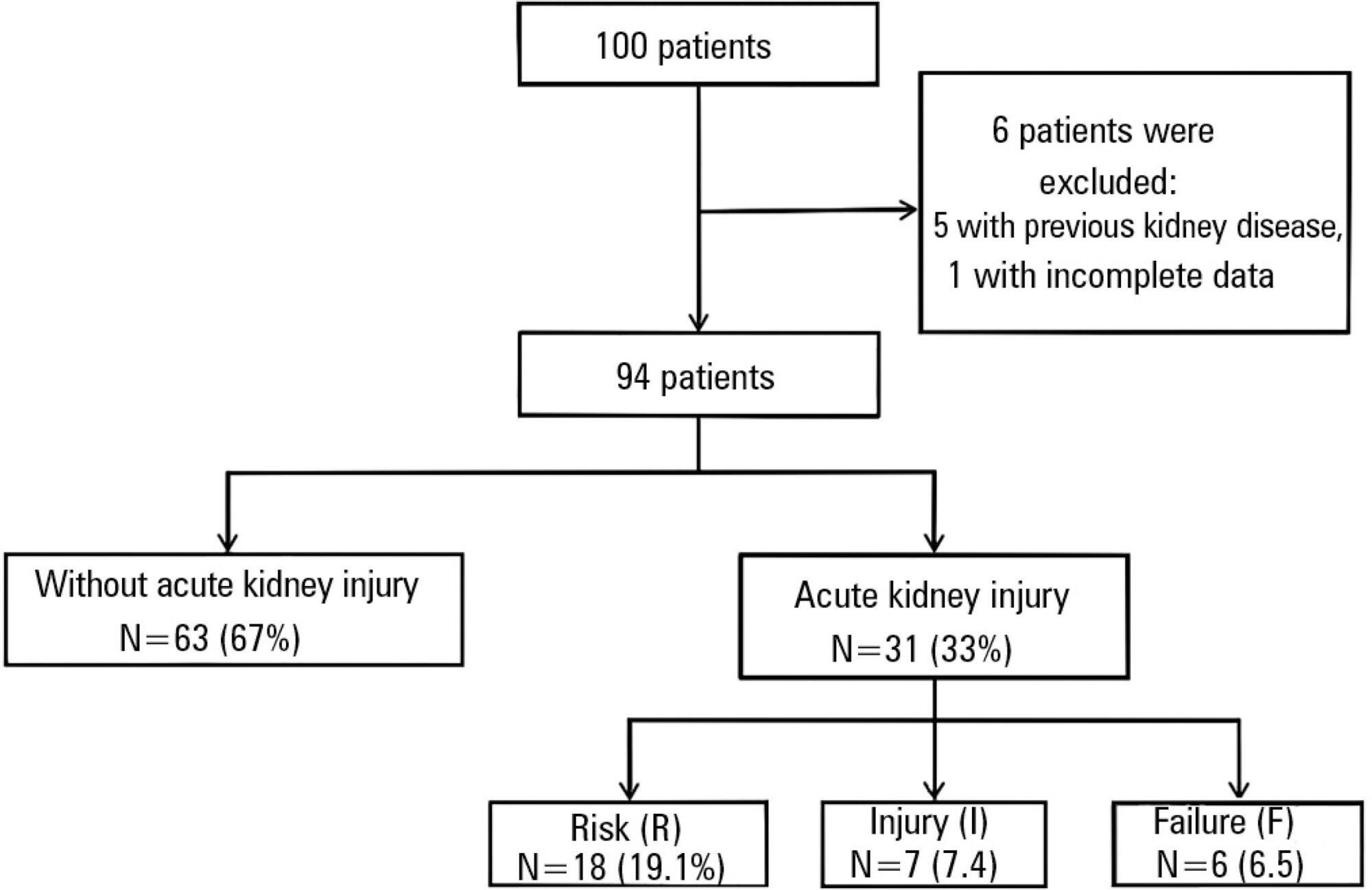
-
Original Articles
Healthcare associated infections caused by coagulase-negative Staphylococci in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2013;25(3):239-244
Abstract
Original ArticlesHealthcare associated infections caused by coagulase-negative Staphylococci in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2013;25(3):239-244
DOI 10.5935/0103-507X.20130041
Views0See moreOBJECTIVE:
This study sought to evaluate infections related to health care caused by coagulase-negative Staphylococci in a neonatal intensive care unit by assessing antimicrobial susceptibility profiles and potentially effective antibiotic regimens.
METHODS:
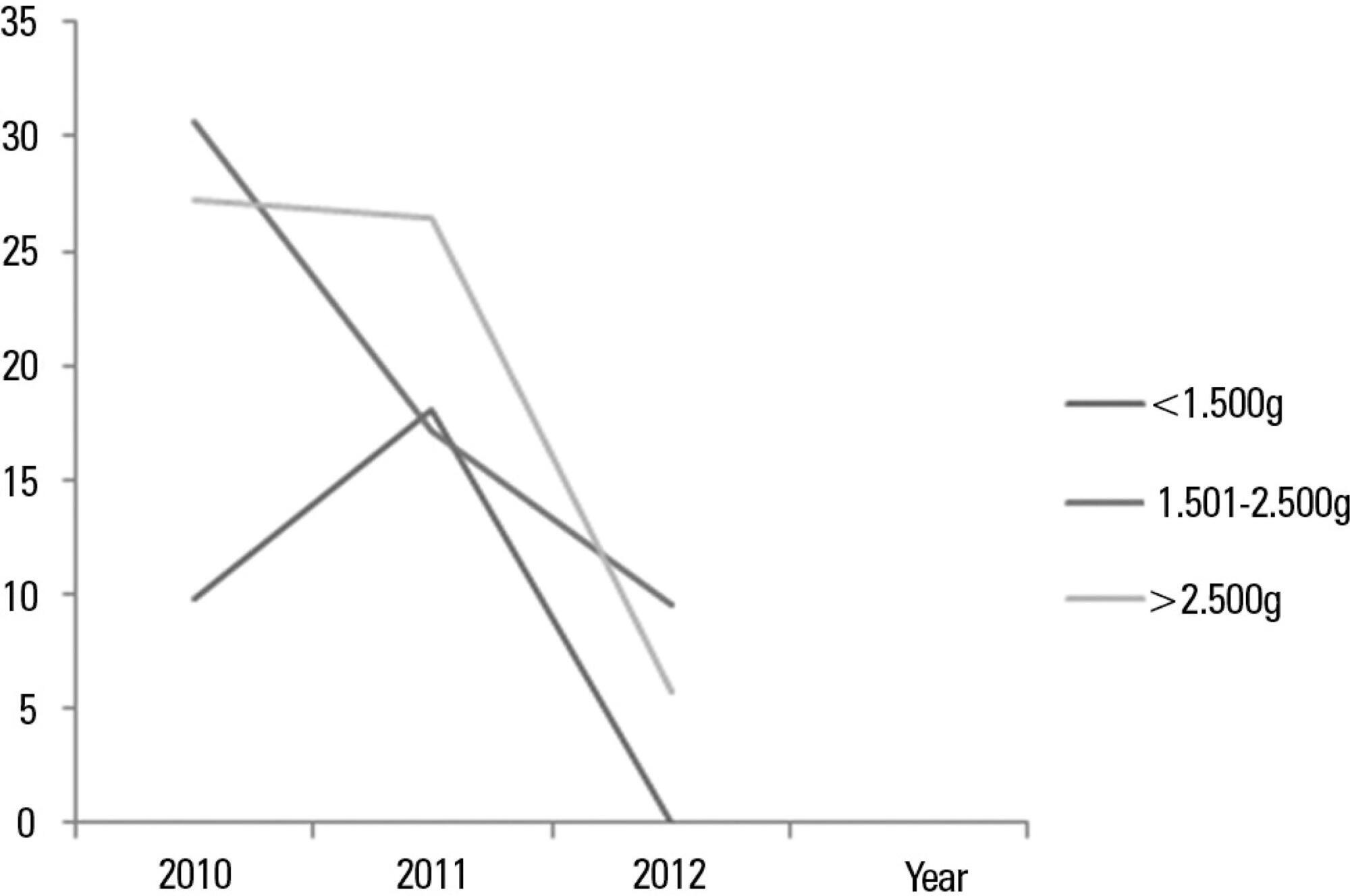
This was a retrospective descriptive study performed on a case series of healthcare-associated infections, and the antimicrobial susceptibility profiles were evaluated. Newborns from other hospitals who were admitted to a neonatal intensive care unit in Rio de Janeiro between January 1, 2010, and June 30, 2012, were studied.
RESULTS:
In total, 765 patients were admitted, totaling 3,051 patient-days, and the incidence density of general infection was 18.9 per 1,000 patient-days. The rate of central venous catheter use was 71.6%, and the positive culture rate for all sites and all infections related to health care were 68.4%. Coagulase-negative Staphylococci were identified in 11 (19.2%) of 57 health care-related infections, and infections with extended-spectrum beta-lactamase producing Klebsiella pneumoniae and Candida sp. constituted 5 cases each. Of the 11 cases of coagulase-negative Staphylococci, 10 (90.9%) were primary bloodstream infections. The sensitivity of the coagulase-negative Staphylococci isolates to vancomycin, clindamycin, ciprofloxacin, oxacillin and gentamycin was 100%, 81.8%, 72.7%, 27.2% and 22.2%, respectively. There were no deaths directly attributed to coagulase-negative Staphylococci infection.
CONCLUSION:
Coagulase-negative Staphylococci was the main agent identified in healthcare-associated infections, with low rates of infections related to central venous catheter. In hospitals with a high oxacillin resistance profile, similar to those included in this study, vancomycin may be used as an initial therapy, although clindamycin represents a viable alternative.
Views0Abstract
Original ArticlesHealthcare associated infections caused by coagulase-negative Staphylococci in a neonatal intensive care unit
Rev Bras Ter Intensiva. 2013;25(3):239-244
DOI 10.5935/0103-507X.20130041
Views0See moreOBJECTIVE:
This study sought to evaluate infections related to health care caused by coagulase-negative Staphylococci in a neonatal intensive care unit by assessing antimicrobial susceptibility profiles and potentially effective antibiotic regimens.
METHODS:
This was a retrospective descriptive study performed on a case series of healthcare-associated infections, and the antimicrobial susceptibility profiles were evaluated. Newborns from other hospitals who were admitted to a neonatal intensive care unit in Rio de Janeiro between January 1, 2010, and June 30, 2012, were studied.
RESULTS:
In total, 765 patients were admitted, totaling 3,051 patient-days, and the incidence density of general infection was 18.9 per 1,000 patient-days. The rate of central venous catheter use was 71.6%, and the positive culture rate for all sites and all infections related to health care were 68.4%. Coagulase-negative Staphylococci were identified in 11 (19.2%) of 57 health care-related infections, and infections with extended-spectrum beta-lactamase producing Klebsiella pneumoniae and Candida sp. constituted 5 cases each. Of the 11 cases of coagulase-negative Staphylococci, 10 (90.9%) were primary bloodstream infections. The sensitivity of the coagulase-negative Staphylococci isolates to vancomycin, clindamycin, ciprofloxacin, oxacillin and gentamycin was 100%, 81.8%, 72.7%, 27.2% and 22.2%, respectively. There were no deaths directly attributed to coagulase-negative Staphylococci infection.
CONCLUSION:
Coagulase-negative Staphylococci was the main agent identified in healthcare-associated infections, with low rates of infections related to central venous catheter. In hospitals with a high oxacillin resistance profile, similar to those included in this study, vancomycin may be used as an initial therapy, although clindamycin represents a viable alternative.
-
Original Articles
Early nasal injury resulting from the use of nasal prongs in preterm infants with very low birth weight: a pilot study
Rev Bras Ter Intensiva. 2013;25(3):245-250
Abstract
Original ArticlesEarly nasal injury resulting from the use of nasal prongs in preterm infants with very low birth weight: a pilot study
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
Views0See moreOBJECTIVE:
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
METHODS:
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
RESULTS:
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology – Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
CONCLUSION:
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
Views0Abstract
Original ArticlesEarly nasal injury resulting from the use of nasal prongs in preterm infants with very low birth weight: a pilot study
Rev Bras Ter Intensiva. 2013;25(3):245-250
DOI 10.5935/0103-507X.20130042
Views0See moreOBJECTIVE:
To analyze the incidence of early-onset nasal injury in infants with very low birth weight and indication for noninvasive ventilation via nasal prongs.
METHODS:
A prospective case series of infants with gestational age <37 weeks, weight <1.500 g and postnatal age <29 days. The patients were evaluated three times daily from the installation of nasal prongs to the 3rd day of use. The patients' clinical conditions and the device's characteristics and its application were analyzed. The initial analysis was descriptive, indicating the prevalence of nasal injury and factors associated with it. Categorical data were analyzed using the chi-squared test or Fisher's exact test, and numerical data were analyzed using the t-test or the Mann-Whitney test.
RESULTS:
Eighteen infants were included; 12 (with a gestational age of 29.8±3.1 weeks, birth weight of 1.070±194 g and a Score for Neonatal Acute Physiology – Perinatal Extension (SNAPPE) of 15.4±17.5) developed nasal injuries (injury group), and 6 (with a gestational age of 28.0±1.9 weeks, weight of 1.003±317 g and SNAPPE of 26.2±7.5) showed no nasal injury (uninjured group). The injury group subjects were more often male (75% versus 17%), and their injuries appeared after an average of 18 hours, predominantly during the night (75%).
CONCLUSION:
The incidence of nasal injury in preterm infants who experienced noninvasive ventilation via nasal prongs was high, and a study of associated factors may be planned based on this pilot.
-
Original Articles
Impact of renal replacement therapy on the respiratory function of patients under mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):251-257
Abstract
Original ArticlesImpact of renal replacement therapy on the respiratory function of patients under mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
Views0See moreOBJECTIVE:
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
METHODS:
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
RESULTS:
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
CONCLUSION:
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
Views0Abstract
Original ArticlesImpact of renal replacement therapy on the respiratory function of patients under mechanical ventilation
Rev Bras Ter Intensiva. 2013;25(3):251-257
DOI 10.5935/0103-507X.20130044
Views0See moreOBJECTIVE:
To assess the oxygenation behavior and ventilatory mechanics after hemodialysis in patients under ventilatory support.
METHODS:
The present study was performed in the general intensive care unit of a tertiary public hospital. Patients over 18 years of age under mechanical ventilation and in need of dialysis support were included. Each patient was submitted to 2 evaluations (pre- and post-dialysis) regarding the cardiovascular and ventilatory parameters, the ventilatory mechanics and a laboratory evaluation.
RESULTS:
Eighty patients with acute or chronic renal failure were included. The analysis of the ventilatory mechanics revealed a reduction in the plateau pressure and an increased static compliance after dialysis that was independent of a reduction in blood volume. The patients with acute renal failure also exhibited a reduction in peak pressure (p=0.024) and an increase in the dynamic compliance (p=0.026), whereas the patients with chronic renal failure exhibited an increase in the resistive pressure (p=0.046) and in the resistance of the respiratory system (p=0.044). The group of patients with no loss of blood volume after dialysis exhibited an increase in the resistive pressure (p=0.010) and in the resistance of the respiratory system (p=0.020), whereas the group with a loss of blood volume >2,000mL exhibited a reduction in the peak pressure (p=0.027). No changes in the partial pressure of oxygen in arterial blood (PaO2) or in the PaO2/the fraction of inspired oxygen (PaO2/FiO2) ratio were observed.
CONCLUSION:
Hemodialysis was able to alter the mechanics of the respiratory system and specifically reduced the plateau pressure and increased the static compliance independent of a reduction in blood volume.
-
Review Articles
Manual hyperinflation in airway clearance in pediatric patients: a systematic review
Rev Bras Ter Intensiva. 2013;25(3):258-262
Abstract
Review ArticlesManual hyperinflation in airway clearance in pediatric patients: a systematic review
Rev Bras Ter Intensiva. 2013;25(3):258-262
DOI 10.5935/0103-507X.20130043
Views0See moreOBJECTIVE:
To perform an assessment of the available literature on manual hyperinflation as a respiratory physical therapy technique used in pediatric patients, with the main outcome of achieving airway clearance.
METHODS:
We reviewed articles included in the Lilacs (Latin American and Caribbean Literature on Health Sciences/Literatura Latino Americana e do Caribe em Ciências da Saúde), Cochrane Library, Medline (via Virtual Health Library and PubMed), SciELO (Scientific Electronic Library), and PEDro (Physiotherapy Evidence Database) databases from 2002 to 2013 using the following search terms: “physiotherapy (techniques)”, “respiratory therapy”, “intensive care”, and “airway clearance”. The selected studies were classified according to the level of evidence and grades of recommendation (method of the Oxford Centre for Evidence-Based Medicine) by two examiners, while a third examiner repeated the search and analysis and checked the classification of the articles.
RESULTS:
Three articles were included for analysis, comprising 250 children (aged 0 to 16 years). The main diagnoses were acute respiratory failure, recovery following heart congenital disease and upper abdominal surgery, bone marrow transplantation, asthma, tracheal reconstruction, brain injury, airway injury, and heterogeneous lung diseases. The studies were classified as having a level of evidence 2C and grade of recommendation C.
CONCLUSIONS:
Manual hyperinflation appeared useful for airway clearance in the investigated population, although the evidence available in the literature remains insufficient. Therefore, controlled randomized studies are needed to establish the safety and efficacy of manual hyperinflation in pediatric patients. However, manual hyperinflation must be performed by trained physical therapists only.
Views0Abstract
Review ArticlesManual hyperinflation in airway clearance in pediatric patients: a systematic review
Rev Bras Ter Intensiva. 2013;25(3):258-262
DOI 10.5935/0103-507X.20130043
Views0See moreOBJECTIVE:
To perform an assessment of the available literature on manual hyperinflation as a respiratory physical therapy technique used in pediatric patients, with the main outcome of achieving airway clearance.
METHODS:
We reviewed articles included in the Lilacs (Latin American and Caribbean Literature on Health Sciences/Literatura Latino Americana e do Caribe em Ciências da Saúde), Cochrane Library, Medline (via Virtual Health Library and PubMed), SciELO (Scientific Electronic Library), and PEDro (Physiotherapy Evidence Database) databases from 2002 to 2013 using the following search terms: “physiotherapy (techniques)”, “respiratory therapy”, “intensive care”, and “airway clearance”. The selected studies were classified according to the level of evidence and grades of recommendation (method of the Oxford Centre for Evidence-Based Medicine) by two examiners, while a third examiner repeated the search and analysis and checked the classification of the articles.
RESULTS:
Three articles were included for analysis, comprising 250 children (aged 0 to 16 years). The main diagnoses were acute respiratory failure, recovery following heart congenital disease and upper abdominal surgery, bone marrow transplantation, asthma, tracheal reconstruction, brain injury, airway injury, and heterogeneous lung diseases. The studies were classified as having a level of evidence 2C and grade of recommendation C.
CONCLUSIONS:
Manual hyperinflation appeared useful for airway clearance in the investigated population, although the evidence available in the literature remains insufficient. Therefore, controlled randomized studies are needed to establish the safety and efficacy of manual hyperinflation in pediatric patients. However, manual hyperinflation must be performed by trained physical therapists only.
Volume Articles - Critical Care Science (CCS)
