Original Articles Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
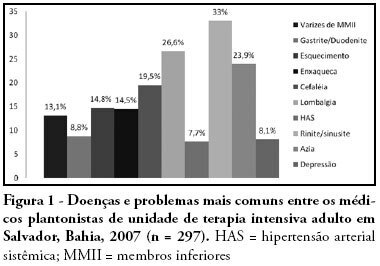
OBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia - Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):235-240
DOI 10.1590/S0103-507X2008000300005
OBJECTIVES: Burnout syndrome is a response to prolonged occupational stress that involves three main dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The aim of this study was to describe socio-demographic characteristics of intensive care unit physicians and evaluate factors associated to the presence of Burnout syndrome in this population. METHODS: A cross-sectional study was performed to evaluate physicians who have worked in intensive care units from the city of Salvador (Bahia - Brazil) with a minimum weekly workload of 12-hour. An anonymous self-reported questionnaire was used and it was divided into two parts: socio-demographic characteristics and evaluation of Burnout syndrome through Maslach Burnout Inventory. RESULTS: We studied 297 physicians and most of them were male (70%). The mean age and time of graduation were, respectively, 34.2 and 9 years. High levels of emotional exhaustion, depersonalization, and reduced personal accomplishment were found in respectively, 47.5%, 24.6% and 28.3%. The prevalence of Burnout syndrome, considered as high level in at least one dimension, was of 63.3%. This prevalence was statistically lower in physicians specialized on intensive care, those with more than nine years of graduation and those who intend to continue working in intensive care units for more than 10 years. The prevalence was higher in the doctors with more than 24-hours of uninterrupted intensive care work per week. CONCLUSIONS: Burnout syndrome was common among intensive care physicians and it was more frequent in the youngest doctors, with higher workload and without specialization on intensive care.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
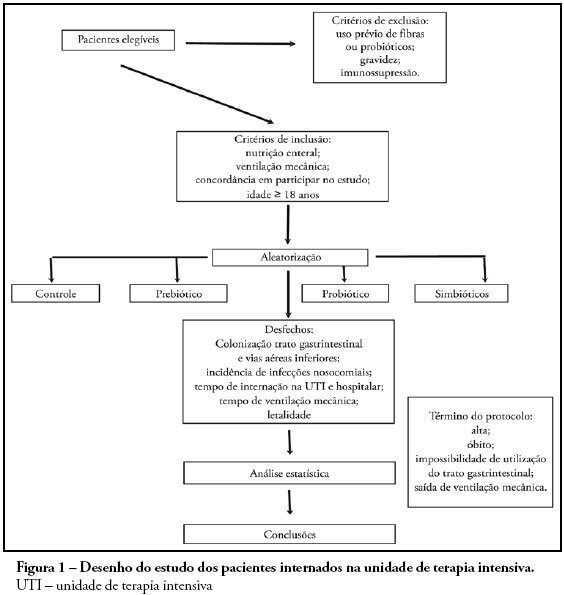
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):241-248
DOI 10.1590/S0103-507X2008000300006
OBJECTIVES: Sepsis is the main cause of death in the intensive care unit. New preventive measures for nosocomial infections have been researched, such as pre, pro and symbiotic usage, due to its immunoregulatory properties. The objective was to evaluate the effect of administration of pre, pro and symbiotic on gastrointestinal and inferior airway colonization and on nosocomial infections, particularly ventilator-associated pneumonia. METHODS: Patients who were admitted to the intensive care unit at Hospital Universitário Clementino Fraga Filho between November 2004 and September 2006 and mechanically ventilated were randomized in one of four groups: control (n = 16), prebiotic (n = 10), probiotic (n = 12) or symbiotic (n = 11). Treatment was administered for fourteen days. Outcomes measured were: a) Colonization of the gastrointestinal tract and trachea; b) incidence of nosocomial infections, particularly ventilator associated pneumonia; c) duration of mechanical ventilation, length of stay in the intensive care unit, duration of hospitalization, mortality rates, and d) development of organ dysfunction. RESULTS: Forty-nine patients were evaluated. intensive care unit's mortality was 34% and in-hospital mortality was 53%, APACHE II median was 20 (13 -25). The groups were matched at admission. There was no difference between the groups in relation to the incidence of ventilator associated pneumonia or nosocomial infection. There was a non-significant increase in the proportion of enterobacteria in the trachea at the seventh day in the pre and probiotic groups compared to control. There was a non-significant decrease in the number of bacteria found in the stomach in the pre, pro and symbiotic group at day 7. No significant difference, in regards to the remaining measured parameters, could be found. CONCLUSIONS: Probiotic therapy was not efficient in the prevention of nosocomial infection but there was a tendency to reduction in tracheal colonization by non-fermenting bacteria.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
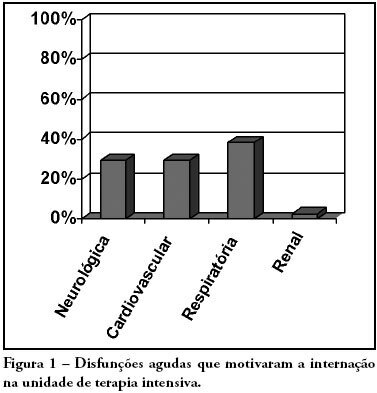
OBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):249-253
DOI 10.1590/S0103-507X2008000300007
OBJECTIVES: Due to the high incidence in our service, we did object on this study describe the features and outcome of patients with systemic lupus erythematosus (SLE) admitted to the intensive care unit of Walter Cantídio University Hospital METHODS: Patients were restrospectively characterized according to demography parameters, time of diagnosis of SLE, organ dysfunction and laboratorial parameters at admission, supportive therapies during their stay, length of stay in the hospital before admission, length of stay in the unit, readmission to the unit and outcome. We also evaluated Systemic Lupus Erythematosus Disease Activity (SLEDAI) score, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, expected mortality and standardized mortality ratio. RESULTS: From November 2003 to October 2006, 1,052 patients were admitted to the intensive care unit. Fifty patients had SLE and were included in this retrospective study. Of the 50 patients with SLE admitted to the ICU, 88.2% were female. The mean age was 30.3 ± 12.8 years. The median time of diagnosis of SLE was 67 months. The most common organ dysfunctions were renal (70.6%), cardiovascular (61.8%), respiratory (55.9%) and neurological (55.9%). The main reasons for admission to the ICU were respiratory (38.2%), cardiologic (29.4%) and neurological (29.4%) dysfunctions. Among the intensive care therapies, 44.1% of the patients needed blood products, 41.2% vasopressor agents and 35.3% mechanical ventilation, 23.5% dialysis. The mean SLEDAI score was 15.0 ± 12.2. The mean APACHE II score was 19.3 ± 6.8, with a predicted mortality rate of 37.6%. The actual mortality rate in ICU was 29.4%, with 8.8% before 48 hours. The standardized mortality ratio was 0.78. Patients with APACHE II > 18, with more than 3 acute organ involvements, leukopenia (< 4000 cells/mm3) and gastrointestinal or metabolic involvement had higher mortality in the intensive care unit. CONCLUSION: Although the severity of patients at admission to the ICU, demonstrated by APACHE II and the acute dysfunctions, the outcomes of analysed patients sugest susceptibility to the therapy.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):160-164
DOI 10.1590/S0103-507X2008000200008
BACKGROUND AND OBJECTIVES: Nosocomial catheter related bloodstream infections (CR-BSI) increase morbidity and mortality in critically ill patients. Central venous catheters (CVC) coated with rifampin and minocycline (RM) decrease rates of colonization and CR-BSI. However, recent trials challenged the clinical impact of such catheters. We designed this trial to compare rates of colonization and CR-BSI in RM catheters and controls in a cohort of critically ill patients in Brazil. METHODS: Prospective, controlled trial conducted in one medico-surgical ICU. Patients were assigned to receive a control or RM CVC. After removal, tips were cultured in association with blood cultures. Rates of colonization and CR-BSI were recorded. RESULTS: Among 120 catheters inserted, 100 could be evaluated, 49 in the uncoated and 51 in the coated group. Clinical characteristics of patients were similar in the two groups. Two cases of CR-BSI (3.9%) occurred in patients who received RM catheters compared with 5 (10.2%) in the uncoated group (p = 0.26). Six RM catheters (11.8%) were colonized compared with 14 (28.6%) control catheters (p = 0.036). Kaplan-Meier analysis showed no significant differences in the risk of colonization or CR-BSI. Rates of CR-BSI were 4.7 per 1000 catheter-days in the RM coated group compared to 11.4 per 1000 catheter days in the uncoated group (p = 0.45). CONCLUSIONS: In this pilot study, we showed lower rates of colonization in RM coated when compared with uncoated catheters. Incidence and rates of CR-BSI were similar in the two groups.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):160-164
DOI 10.1590/S0103-507X2008000200008
BACKGROUND AND OBJECTIVES: Nosocomial catheter related bloodstream infections (CR-BSI) increase morbidity and mortality in critically ill patients. Central venous catheters (CVC) coated with rifampin and minocycline (RM) decrease rates of colonization and CR-BSI. However, recent trials challenged the clinical impact of such catheters. We designed this trial to compare rates of colonization and CR-BSI in RM catheters and controls in a cohort of critically ill patients in Brazil. METHODS: Prospective, controlled trial conducted in one medico-surgical ICU. Patients were assigned to receive a control or RM CVC. After removal, tips were cultured in association with blood cultures. Rates of colonization and CR-BSI were recorded. RESULTS: Among 120 catheters inserted, 100 could be evaluated, 49 in the uncoated and 51 in the coated group. Clinical characteristics of patients were similar in the two groups. Two cases of CR-BSI (3.9%) occurred in patients who received RM catheters compared with 5 (10.2%) in the uncoated group (p = 0.26). Six RM catheters (11.8%) were colonized compared with 14 (28.6%) control catheters (p = 0.036). Kaplan-Meier analysis showed no significant differences in the risk of colonization or CR-BSI. Rates of CR-BSI were 4.7 per 1000 catheter-days in the RM coated group compared to 11.4 per 1000 catheter days in the uncoated group (p = 0.45). CONCLUSIONS: In this pilot study, we showed lower rates of colonization in RM coated when compared with uncoated catheters. Incidence and rates of CR-BSI were similar in the two groups.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
BACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists' knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient's family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):144-148
DOI 10.1590/S0103-507X2008000200005
BACKGROUND AND OBJECTIVES: Failure or delay to diagnose brain death leads to needless occupation of a hospital bed, emotional and financial losses, and unavailability of organs for transplants. The intensive care physician plays an essential role in this diagnosis. This study intended to evaluate intensivists' knowledge concerning brain death. METHODS: Cross-sectional study in 15 intensive care units (ICU) in eight hospitals in the city of Porto Alegre, Brazil. RESULTS: Two hundred forty-six intensivists were interviewed in a consecutive sample between April and December 2005. The prevalence of lack of knowledge regarding the concept was of 17%. Twenty per cent of the interviewees ignored the legal need for complementary confirmatory tests for their diagnosis. Forty-seven per cent considered themselves as having the highest level of assurance to explain the concept to a patient's family members. Twenty-nine per cent erroneously determined the legal time of death for brain dead patients. Pediatric intensivists had less knowledge about the concept, when compared to intensivists for adults (p < 0.001). CONCLUSIONS: Current knowledge of brain death is insufficient in Brazil, among the health care professionals who most often find patients in this situation. Education on the subject is needed to avoid unnecessary expenses, reduce family suffering and increase the offer of organs for transplant.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
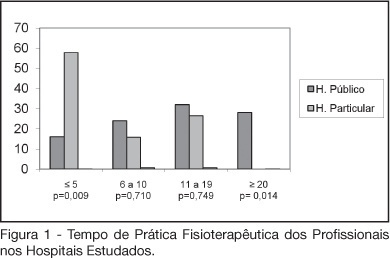
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):149-153
DOI 10.1590/S0103-507X2008000200006
BACKGROUND AND OBJECTIVES: The number of patients requiring prolonged time on mechanical ventilation is increasing considerably in the intensive care unit (ICU). The objective of this study was to characterize the variability of methods and criteria used by physiotherapists to obtain weaning parameters in hospitals of Fortaleza. METHODS: After approval by the UNIFOR Ethics Committee, survey questionnaires were distributed among physiotherapists working in the ICU of three public and three private hospitals. Forty-four physiotherapists answered thirty-two multiple choice questions anonymously. RESULTS: The main results concerned parameters commonly evaluated by physiotherapists. A significant difference between hospitals was found regarding the rapid shallow breathing index and maximum inspiratory pressure, which are more often used in private hospitals, with a percentage of 100% and 89.5%, respectively. Concerning the ventilatory mode for obtaining the weaning parameters for mechanical ventilation; the T-tube was the most used, not only in the public (56%) but also in the private hospitals (57.9%). CONCLUSIONS: Variability in the methods and criteria used to obtain weaning parameters by the physiotherapists was found in public and private hospitals in Fortaleza. Results from this survey stress the need to develop new scientific studies to standardize the techniques used for weaning.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
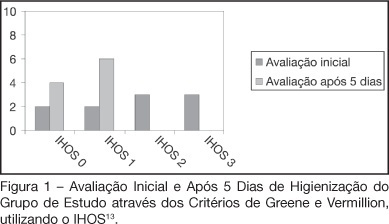
BACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):154-159
DOI 10.1590/S0103-507X2008000200007
BACKGROUND AND OBJECTIVES: Patients admitted to an intensive care unit (ICU), in most cases do not have a proper oral hygiene. This deficient condition of oral hygiene in critical patients often triggers periodontitis, gingivitis and other systemic and oral complications. This research aimed to evaluate the efficiency of the antimicrobial action of a solution with bioactive enzymatic system for oral hygiene, in totally care-dependent patients admitted to ICU. METHODS: A prospective, double blind pilot study was conducted with 20 patients admitted to an ICU, divided into 2 groups with the same technique of oral hygiene, protocols but using different solutions: the study group (n = 10) using an oral solution with enzymatic system and the control group (n = 10) using an oral solution based on cetylpyridinium. RESULTS: Results of microbiological cultures collected in the study group and control group, before and after the use of enzymatic solution, showed no significant difference between groups (p = 0.41). In clinical evaluation of the Simplified Oral Hygiene Index (SOHI) statistical significance was found by the Fisher Exact test (p = 0.01) when comparing the study group and control group. The value of statistical significance was set at 5%, or p < 0.05. CONCLUSIONS: The use of oral rinse with the lactoperoxidase enzyme was effective in the clinical evaluation of the oral hygiene of patients totally care-dependent in the hospital. This study stresses the importance of developing more research on the oral care of these patients.