Respiratory distress syndrome, adult Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
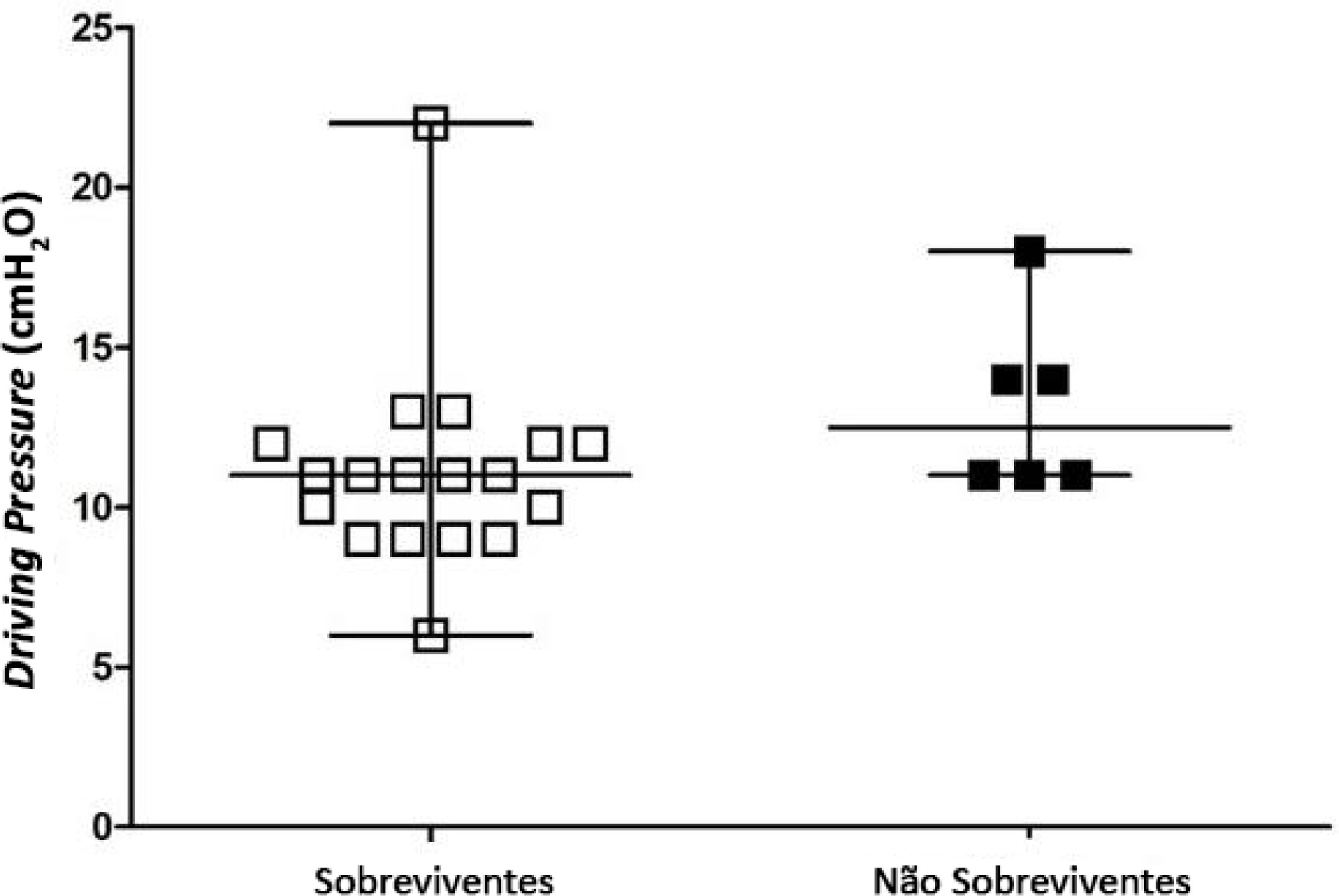
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2021;33(2):261-265
DOI 10.5935/0103-507X.20210033
To identify the possible association between driving pressure and mechanical power values and oxygenation index on the first day of mechanical ventilation with the mortality of trauma patients without a diagnosis of acute respiratory distress syndrome.
Patients under pressure-controlled or volume-controlled ventilation were included, with data collection 24 hours after orotracheal intubation. Patient follow-up was performed for 30 days to obtain the clinical outcome. The patients were admitted to two intensive care units of the Hospital de Pronto Socorro de Porto Alegre from June to September 2019.
A total of 24 patients were evaluated. Driving pressure, mechanical power and oxygenation index were similar among patients who survived and those who died, with no statistically significant difference between groups.
Driving pressure, mechanical power and oxygenation index values obtained on the first day of mechanical ventilation were not associated with mortality of trauma patients without acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):354-362
DOI 10.5935/0103-507X.20200063
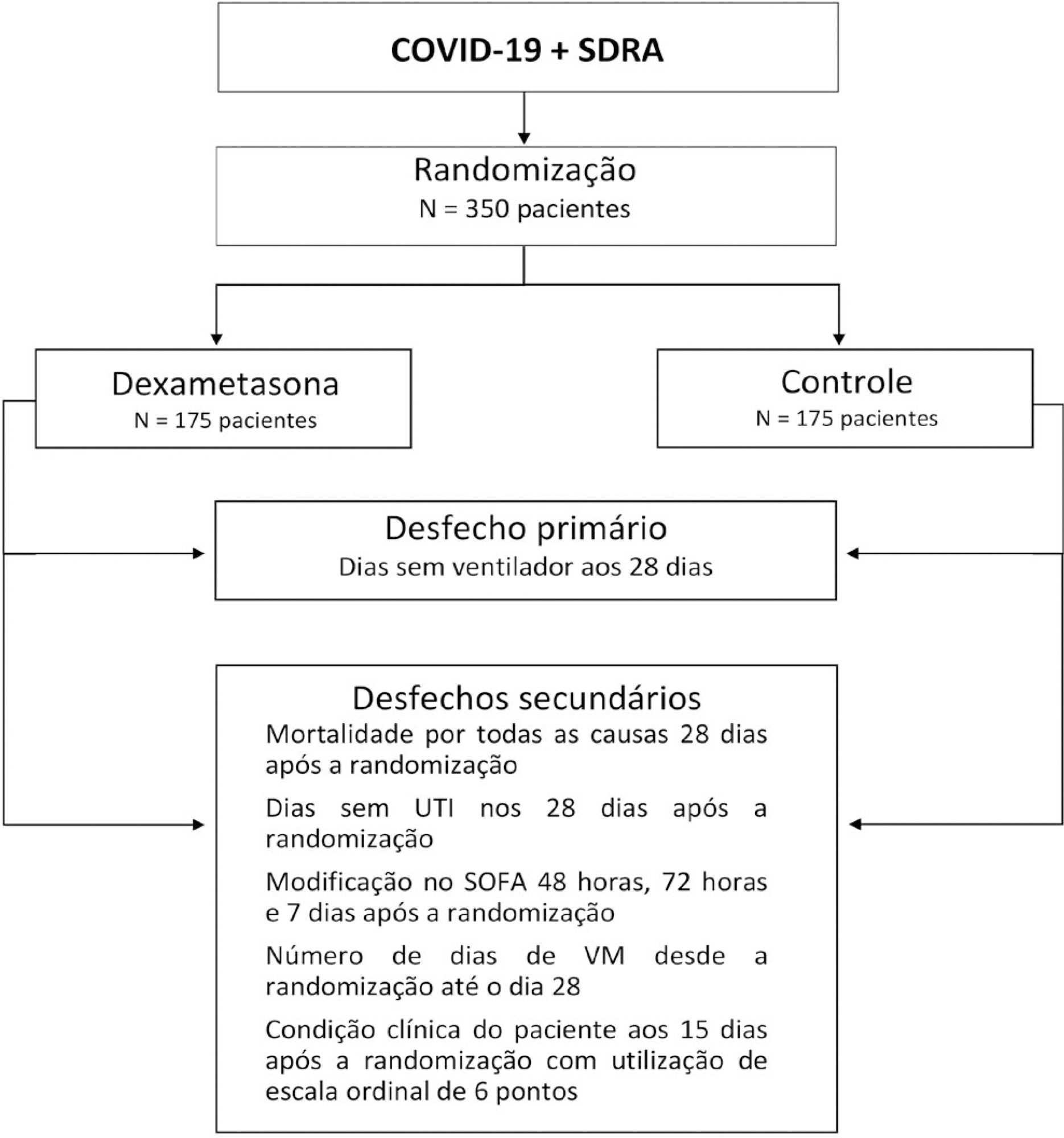
The infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spreads worldwide and is considered a pandemic. The most common manifestation of SARS-CoV-2 infection (coronavirus disease 2019 - COVID-19) is viral pneumonia with varying degrees of respiratory compromise and up to 40% of hospitalized patients might develop acute respiratory distress syndrome. Several clinical trials evaluated the role of corticosteroids in non-COVID-19 acute respiratory distress syndrome with conflicting results. We designed a trial to evaluate the effectiveness of early intravenous dexamethasone administration on the number of days alive and free of mechanical ventilation within 28 days after randomization in adult patients with moderate or severe acute respiratory distress syndrome due to confirmed or probable COVID-19.
This is a pragmatic, prospective, randomized, stratified, multicenter, open-label, controlled trial including 350 patients with early-onset (less than 48 hours before randomization) moderate or severe acute respiratory distress syndrome, defined by the Berlin criteria, due to COVID-19. Eligible patients will be randomly allocated to either standard treatment plus dexamethasone (Intervention Group) or standard treatment without dexamethasone (Control Group). Patients in the intervention group will receive dexamethasone 20mg intravenous once daily for 5 days, followed by dexamethasone 10mg IV once daily for additional 5 days or until intensive care unit discharge, whichever occurs first. The primary outcome is ventilator-free days within 28 days after randomization, defined as days alive and free from invasive mechanical ventilation. Secondary outcomes are all-cause mortality rates at day 28, evaluation of the clinical status at day 15 assessed with a 6-level ordinal scale, mechanical ventilation duration from randomization to day 28, Sequential Organ Failure Assessment Score evaluation at 48 hours, 72 hours and 7 days and intensive care unit -free days within 28.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):354-362
DOI 10.5935/0103-507X.20200063
The infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spreads worldwide and is considered a pandemic. The most common manifestation of SARS-CoV-2 infection (coronavirus disease 2019 - COVID-19) is viral pneumonia with varying degrees of respiratory compromise and up to 40% of hospitalized patients might develop acute respiratory distress syndrome. Several clinical trials evaluated the role of corticosteroids in non-COVID-19 acute respiratory distress syndrome with conflicting results. We designed a trial to evaluate the effectiveness of early intravenous dexamethasone administration on the number of days alive and free of mechanical ventilation within 28 days after randomization in adult patients with moderate or severe acute respiratory distress syndrome due to confirmed or probable COVID-19.
This is a pragmatic, prospective, randomized, stratified, multicenter, open-label, controlled trial including 350 patients with early-onset (less than 48 hours before randomization) moderate or severe acute respiratory distress syndrome, defined by the Berlin criteria, due to COVID-19. Eligible patients will be randomly allocated to either standard treatment plus dexamethasone (Intervention Group) or standard treatment without dexamethasone (Control Group). Patients in the intervention group will receive dexamethasone 20mg intravenous once daily for 5 days, followed by dexamethasone 10mg IV once daily for additional 5 days or until intensive care unit discharge, whichever occurs first. The primary outcome is ventilator-free days within 28 days after randomization, defined as days alive and free from invasive mechanical ventilation. Secondary outcomes are all-cause mortality rates at day 28, evaluation of the clinical status at day 15 assessed with a 6-level ordinal scale, mechanical ventilation duration from randomization to day 28, Sequential Organ Failure Assessment Score evaluation at 48 hours, 72 hours and 7 days and intensive care unit -free days within 28.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
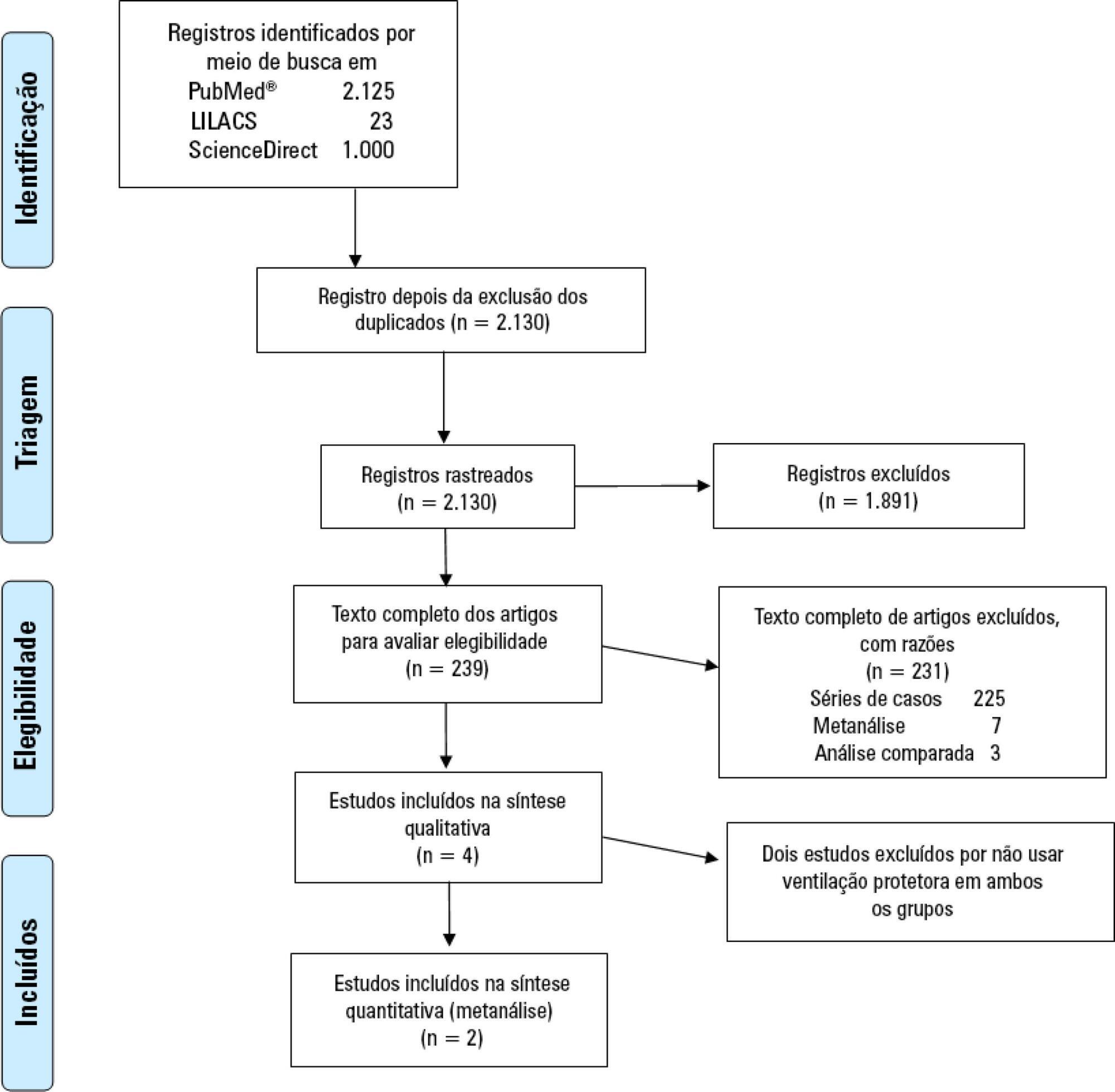
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% - 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 - 0.95 and RR: 0.68; 95%CI 0.55 - 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 - 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th - P75th: 12.49 - 17.18) and P50th 29.80 (P25th - P75th: 26.04 - 33.56] days, respectively.
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):548-554
DOI 10.5935/0103-507X.20190077
The evidence of improved survival with the use of extracorporeal membrane oxygenation (ECMO) in acute respiratory distress syndrome is still uncertain.
This systematic review and meta-analysis was registered in the PROSPERO database with the number CRD-42018098618. We performed a structured search of Medline, Lilacs, and ScienceDirect for randomized controlled trials evaluating the use of ECMO associated with (ultra)protective mechanical ventilation for severe acute respiratory failure in adult patients. We used the Cochrane risk of bias tool to evaluate the quality of the evidence. Our primary objective was to evaluate the effect of ECMO on the last reported mortality. Secondary outcomes were treatment failure, hospital length of stay and the need for renal replacement therapy in both groups.
Two randomized controlled studies were included in the meta-analysis, comprising 429 patients, of whom 214 were supported with ECMO. The most common reason for acute respiratory failure was pneumonia (60% - 65%). Respiratory ECMO support was associated with a reduction in last reported mortality and treatment failure with risk ratios (RR: 0.76; 95%CI 0.61 - 0.95 and RR: 0.68; 95%CI 0.55 - 0.85, respectively). Extracorporeal membrane oxygenation reduced the need for renal replacement therapy, with a RR of 0.88 (95%CI 0.77 - 0.99). Intensive care unit and hospital lengths of stay were longer in ECMO-supported patients, with an additional P50th 14.84 (P25th - P75th: 12.49 - 17.18) and P50th 29.80 (P25th - P75th: 26.04 - 33.56] days, respectively.
Respiratory ECMO support in severe acute respiratory distress syndrome patients is associated with a reduced mortality rate and a reduced need for renal replacement therapy but a substantial increase in the lengths of stay in the intensive care unit and hospital. Our results may help bedside decision-making regarding ECMO initiation in patients with severe respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):483-489
DOI 10.5935/0103-507X.20190071
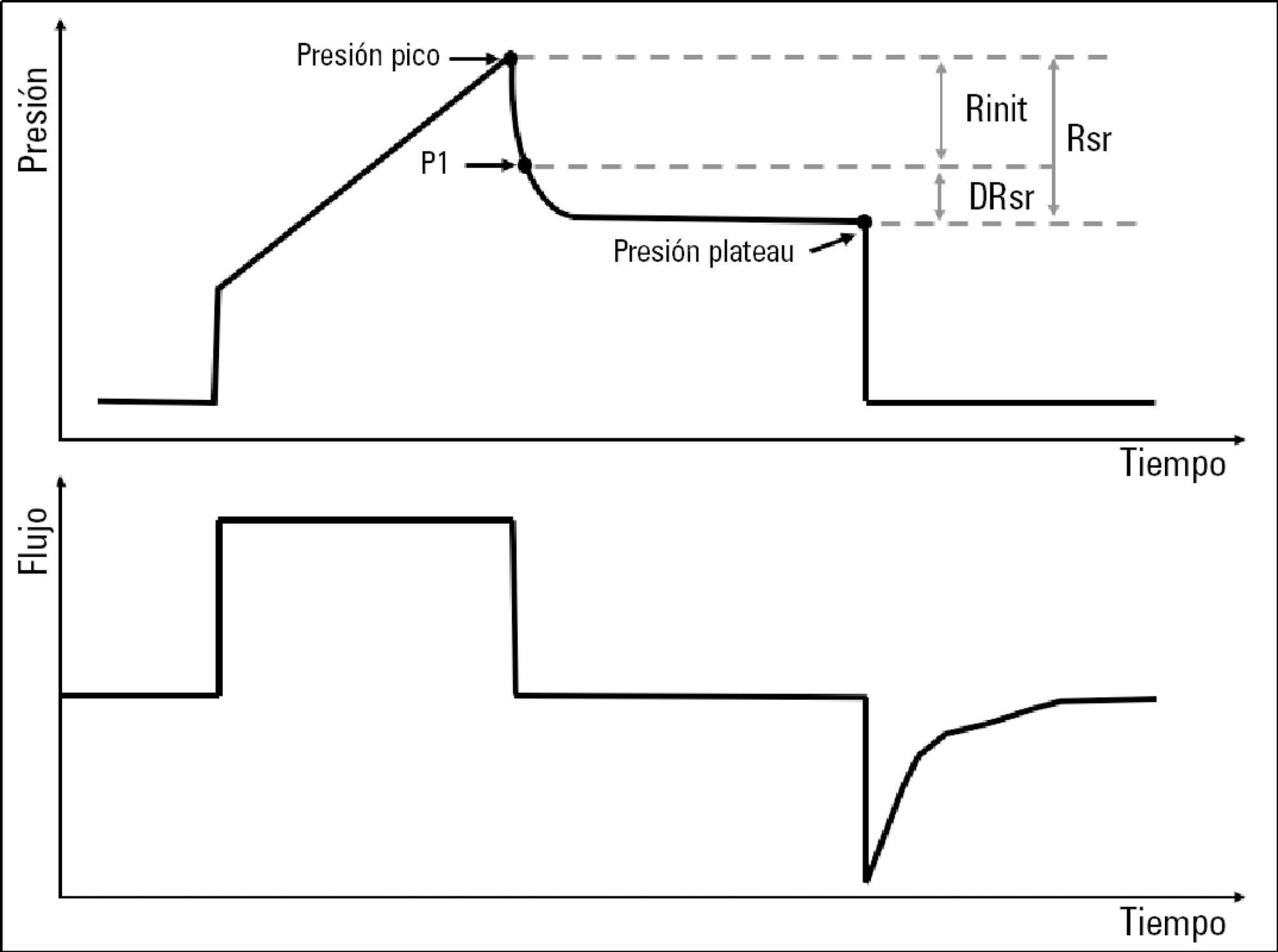
To describe the behavior of inspiratory resistance components when positive end-expiratory pressure (PEEP) increases in patients with acute respiratory distress syndrome under a protective ventilation strategy.
In volume-controlled mode, at 6mL/kg and constant flow, end-inspiratory occlusions were performed at 0, 5 10, 15 and 20cmH2O PEEP. Peak, initial and plateau pressure values were assessed, calculating the maximum, minimum and differential resistances. The results were compared by repeated measures analysis of variance (ANOVA) with post hoc Bonferroni correction, considering p < 0.05 significant.
The highest maximum resistance was observed at the lowest PEEP levels. The values for 10 and 15cmH2O PEEP significantly differed from those for 5 and 0cmH2O PEEP, whereas that for 20cmH2O PEEP only significantly differed from that for 0cmH2O PEEP (p < 0.05). The minimum resistance behaved similarly to the maximum resistance; the values for PEEP levels from 10cmH2O to 20cmH2O significantly differed from those for 0 and 5cmH2O PEEP (p < 0.05). Differential resistance showed the opposite variation to the maximum and minimum resistances. The only PEEP level that showed significant differences from 0 and 5cmH2O PEEP was 20cmH2O PEEP. Significant differences were also found between 15 and 5cmH2O PEEP (p < 0.05).
During protective ventilation in patients with acute respiratory distress syndrome, the maximum resistance of the respiratory system decreases with PEEP, reflecting the minimum resistance response, whereas differential resistance increases with PEEP.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):483-489
DOI 10.5935/0103-507X.20190071
To describe the behavior of inspiratory resistance components when positive end-expiratory pressure (PEEP) increases in patients with acute respiratory distress syndrome under a protective ventilation strategy.
In volume-controlled mode, at 6mL/kg and constant flow, end-inspiratory occlusions were performed at 0, 5 10, 15 and 20cmH2O PEEP. Peak, initial and plateau pressure values were assessed, calculating the maximum, minimum and differential resistances. The results were compared by repeated measures analysis of variance (ANOVA) with post hoc Bonferroni correction, considering p < 0.05 significant.
The highest maximum resistance was observed at the lowest PEEP levels. The values for 10 and 15cmH2O PEEP significantly differed from those for 5 and 0cmH2O PEEP, whereas that for 20cmH2O PEEP only significantly differed from that for 0cmH2O PEEP (p < 0.05). The minimum resistance behaved similarly to the maximum resistance; the values for PEEP levels from 10cmH2O to 20cmH2O significantly differed from those for 0 and 5cmH2O PEEP (p < 0.05). Differential resistance showed the opposite variation to the maximum and minimum resistances. The only PEEP level that showed significant differences from 0 and 5cmH2O PEEP was 20cmH2O PEEP. Significant differences were also found between 15 and 5cmH2O PEEP (p < 0.05).
During protective ventilation in patients with acute respiratory distress syndrome, the maximum resistance of the respiratory system decreases with PEEP, reflecting the minimum resistance response, whereas differential resistance increases with PEEP.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Abstract
Rev Bras Ter Intensiva. 2019;31(4):555-560
DOI 10.5935/0103-507X.20190074
Patients with acute respiratory distress syndrome require ventilation strategies that have been shown to be important for reducing short-term mortality, such as protective ventilation and prone position ventilation. However, patients who survive have a prolonged stay in both the intensive care unit and the hospital, and they experience a reduction in overall satisfaction with life (independence, acceptance and positive outlook) as well as decreased mental health (including anxiety, depression and posttraumatic stress disorder symptoms), physical health (impaired physical state and activities of daily living; fatigue and muscle weakness), social health and the ability to participate in social activities (including relationships with friends and family, hobbies and social gatherings).
Abstract
Rev Bras Ter Intensiva. 2018;30(2):208-218
DOI 10.5935/0103-507X.20180038
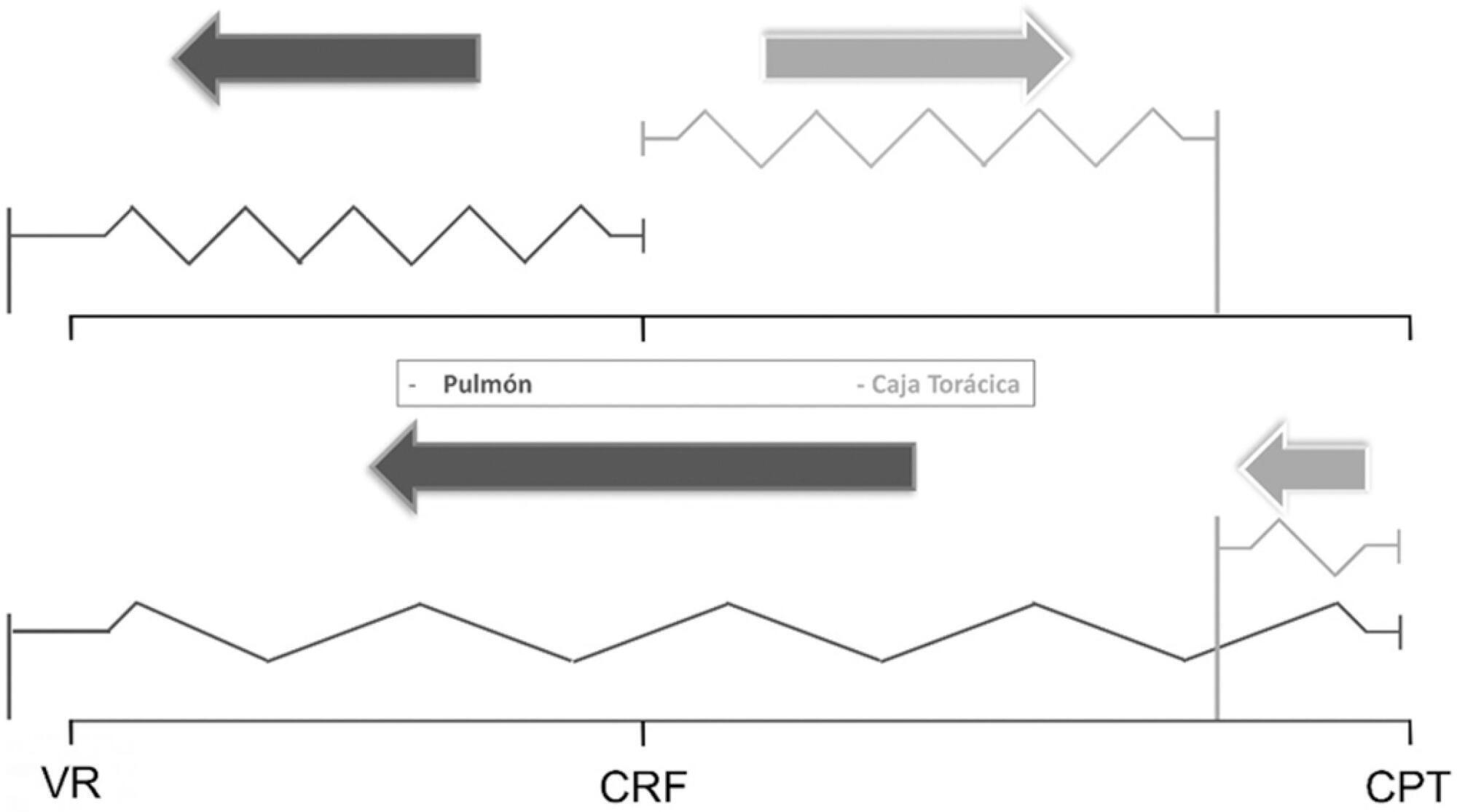
The respiratory system mechanics depend on the characteristics of the lung and chest wall and their interaction. In patients with acute respiratory distress syndrome under mechanical ventilation, the monitoring of airway plateau pressure is fundamental given its prognostic value and its capacity to assess pulmonary stress. However, its validity can be affected by changes in mechanical characteristics of the chest wall, and it provides no data to correctly titrate positive end-expiratory pressure by restoring lung volume. The chest wall effect on respiratory mechanics in acute respiratory distress syndrome has not been completely described, and it has likely been overestimated, which may lead to erroneous decision making. The load imposed by the chest wall is negligible when the respiratory system is insufflated with positive end-expiratory pressure. Under dynamic conditions, moving this structure demands a pressure change whose magnitude is related to its mechanical characteristics, and this load remains constant regardless of the volume from which it is insufflated. Thus, changes in airway pressure reflect changes in the lung mechanical conditions. Advanced monitoring could be reserved for patients with increased intra-abdominal pressure in whom a protective mechanical ventilation strategy cannot be implemented. The estimates of alveolar recruitment based on respiratory system mechanics could reflect differences in chest wall response to insufflation and not actual alveolar recruitment.
Abstract
Rev Bras Ter Intensiva. 2018;30(2):208-218
DOI 10.5935/0103-507X.20180038
The respiratory system mechanics depend on the characteristics of the lung and chest wall and their interaction. In patients with acute respiratory distress syndrome under mechanical ventilation, the monitoring of airway plateau pressure is fundamental given its prognostic value and its capacity to assess pulmonary stress. However, its validity can be affected by changes in mechanical characteristics of the chest wall, and it provides no data to correctly titrate positive end-expiratory pressure by restoring lung volume. The chest wall effect on respiratory mechanics in acute respiratory distress syndrome has not been completely described, and it has likely been overestimated, which may lead to erroneous decision making. The load imposed by the chest wall is negligible when the respiratory system is insufflated with positive end-expiratory pressure. Under dynamic conditions, moving this structure demands a pressure change whose magnitude is related to its mechanical characteristics, and this load remains constant regardless of the volume from which it is insufflated. Thus, changes in airway pressure reflect changes in the lung mechanical conditions. Advanced monitoring could be reserved for patients with increased intra-abdominal pressure in whom a protective mechanical ventilation strategy cannot be implemented. The estimates of alveolar recruitment based on respiratory system mechanics could reflect differences in chest wall response to insufflation and not actual alveolar recruitment.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):105-110
DOI 10.5935/0103-507X.20170015
Acute respiratory distress syndrome is characterized by diffuse inflammatory lung injury and is classified as mild, moderate, and severe. Clinically, hypoxemia, bilateral opacities in lung images, and decreased pulmonary compliance are observed. Sepsis is one of the most prevalent causes of this condition (30 - 50%). Among the direct causes of acute respiratory distress syndrome, chlorine inhalation is an uncommon cause, generating mucosal and airway irritation in most cases. We present a case of severe acute respiratory distress syndrome after accidental inhalation of chlorine in a swimming pool, with noninvasive ventilation used as a treatment with good response in this case. We classified severe acute respiratory distress syndrome based on an oxygen partial pressure/oxygen inspired fraction ratio <100, although the Berlin classification is limited in considering patients with severe hypoxemia managed exclusively with noninvasive ventilation. The failure rate of noninvasive ventilation in cases of acute respiratory distress syndrome is approximately 52% and is associated with higher mortality. The possible complications of using noninvasive positive-pressure mechanical ventilation in cases of acute respiratory distress syndrome include delays in orotracheal intubation, which is performed in cases of poor clinical condition and with high support pressure levels, and deep inspiratory efforts, generating high tidal volumes and excessive transpulmonary pressures, which contribute to ventilation-related lung injury. Despite these complications, some studies have shown a decrease in the rates of orotracheal intubation in patients with acute respiratory distress syndrome with low severity scores, hemodynamic stability, and the absence of other organ dysfunctions.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):105-110
DOI 10.5935/0103-507X.20170015
Acute respiratory distress syndrome is characterized by diffuse inflammatory lung injury and is classified as mild, moderate, and severe. Clinically, hypoxemia, bilateral opacities in lung images, and decreased pulmonary compliance are observed. Sepsis is one of the most prevalent causes of this condition (30 - 50%). Among the direct causes of acute respiratory distress syndrome, chlorine inhalation is an uncommon cause, generating mucosal and airway irritation in most cases. We present a case of severe acute respiratory distress syndrome after accidental inhalation of chlorine in a swimming pool, with noninvasive ventilation used as a treatment with good response in this case. We classified severe acute respiratory distress syndrome based on an oxygen partial pressure/oxygen inspired fraction ratio <100, although the Berlin classification is limited in considering patients with severe hypoxemia managed exclusively with noninvasive ventilation. The failure rate of noninvasive ventilation in cases of acute respiratory distress syndrome is approximately 52% and is associated with higher mortality. The possible complications of using noninvasive positive-pressure mechanical ventilation in cases of acute respiratory distress syndrome include delays in orotracheal intubation, which is performed in cases of poor clinical condition and with high support pressure levels, and deep inspiratory efforts, generating high tidal volumes and excessive transpulmonary pressures, which contribute to ventilation-related lung injury. Despite these complications, some studies have shown a decrease in the rates of orotracheal intubation in patients with acute respiratory distress syndrome with low severity scores, hemodynamic stability, and the absence of other organ dysfunctions.

Abstract
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
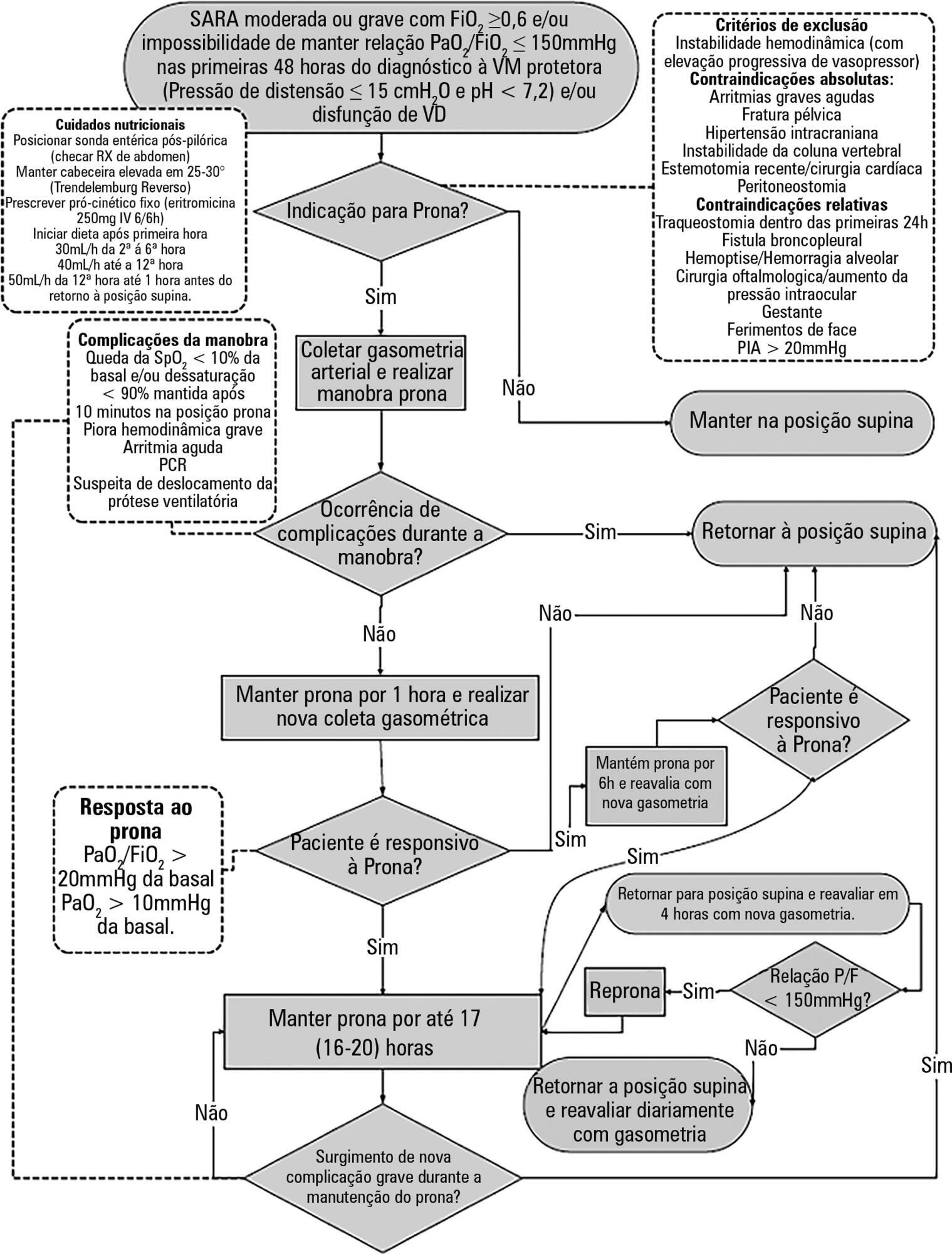
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team's understanding of the tool's importance to patient safety and training in its use are necessary for its success.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):131-141
DOI 10.5935/0103-507X.20170023
To construct and implement an instrument (checklist) to improve safety when performing the prone maneuver.
This was an applied, qualitative and descriptive study. The instrument was developed based on a broad review of the literature pertaining to the construction of a care protocol using the main electronic databases (MEDLINE, LILACS and Cochrane).
We describe the construction of a patient safety tool with numerous modifications and adaptations based on the observations of the multidisciplinary team regarding its use in daily practice.
The use of the checklist when performing the prone maneuver increased the safety and reliability of the procedure. The team's understanding of the tool's importance to patient safety and training in its use are necessary for its success.