monitoring Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2021;33(3):461-468
DOI 10.5935/0103-507X.20210061
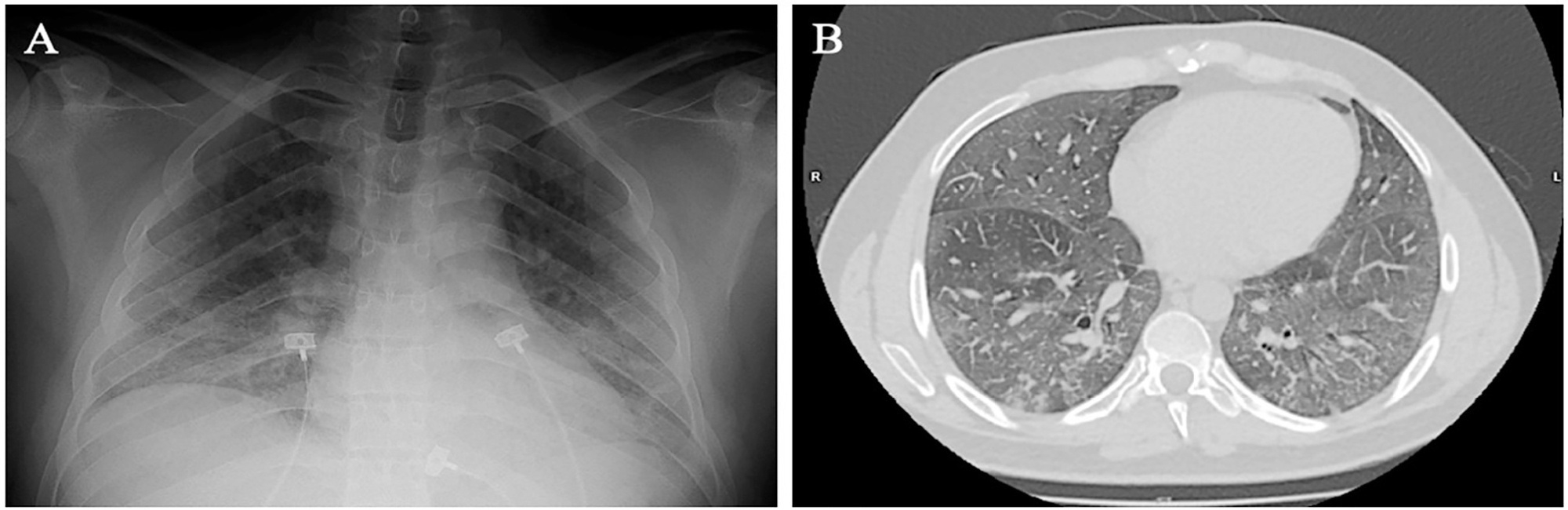
Spontaneous breathing can be deleterious in patients with previously injured lungs, especially in acute respiratory distress syndrome. Moreover, the failure to assume spontaneous breathing during mechanical ventilation and the need to switch back to controlled mechanical ventilation are associated with higher mortality. There is a gap of knowledge regarding which parameters might be useful to predict the risk of patient self-inflicted lung injury and to detect the inability to assume spontaneous breathing. We report a case of patient self-inflicted lung injury, the corresponding basic and advanced monitoring of the respiratory system mechanics and physiological and clinical results related to spontaneous breathing. The patient was a 33-year-old Caucasian man with a medical history of AIDS who developed acute respiratory distress syndrome and needed invasive mechanical ventilation after noninvasive ventilatory support failure. During the controlled ventilation periods, a protective ventilation strategy was adopted, and the patient showed clear clinical and radiographic improvement. However, during each spontaneous breathing period under pressure support ventilation, despite adequate initial parameters and a strictly adjusted ventilatory setting and monitoring, the patient developed progressive hypoxemia and worsening of respiratory system mechanics with a clearly correlated radiographic deterioration (patient self-inflicted lung injury). After failing three spontaneous breathing assumption trials, he died on day 29 due to refractory hypoxemia. Conventional basic and advanced monitoring variables in this case were not sufficient to identify the aptitude to breathe spontaneously or to predict the risk and development of patient self-inflicted lung injury during partial support ventilation.
Abstract
Rev Bras Ter Intensiva. 2021;33(3):461-468
DOI 10.5935/0103-507X.20210061
Spontaneous breathing can be deleterious in patients with previously injured lungs, especially in acute respiratory distress syndrome. Moreover, the failure to assume spontaneous breathing during mechanical ventilation and the need to switch back to controlled mechanical ventilation are associated with higher mortality. There is a gap of knowledge regarding which parameters might be useful to predict the risk of patient self-inflicted lung injury and to detect the inability to assume spontaneous breathing. We report a case of patient self-inflicted lung injury, the corresponding basic and advanced monitoring of the respiratory system mechanics and physiological and clinical results related to spontaneous breathing. The patient was a 33-year-old Caucasian man with a medical history of AIDS who developed acute respiratory distress syndrome and needed invasive mechanical ventilation after noninvasive ventilatory support failure. During the controlled ventilation periods, a protective ventilation strategy was adopted, and the patient showed clear clinical and radiographic improvement. However, during each spontaneous breathing period under pressure support ventilation, despite adequate initial parameters and a strictly adjusted ventilatory setting and monitoring, the patient developed progressive hypoxemia and worsening of respiratory system mechanics with a clearly correlated radiographic deterioration (patient self-inflicted lung injury). After failing three spontaneous breathing assumption trials, he died on day 29 due to refractory hypoxemia. Conventional basic and advanced monitoring variables in this case were not sufficient to identify the aptitude to breathe spontaneously or to predict the risk and development of patient self-inflicted lung injury during partial support ventilation.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):143-147
DOI 10.5935/0103-507X.20140021
To evaluate the behavior of fractional excretion of potassium in the course of acute kidney injury in critically ill patients.
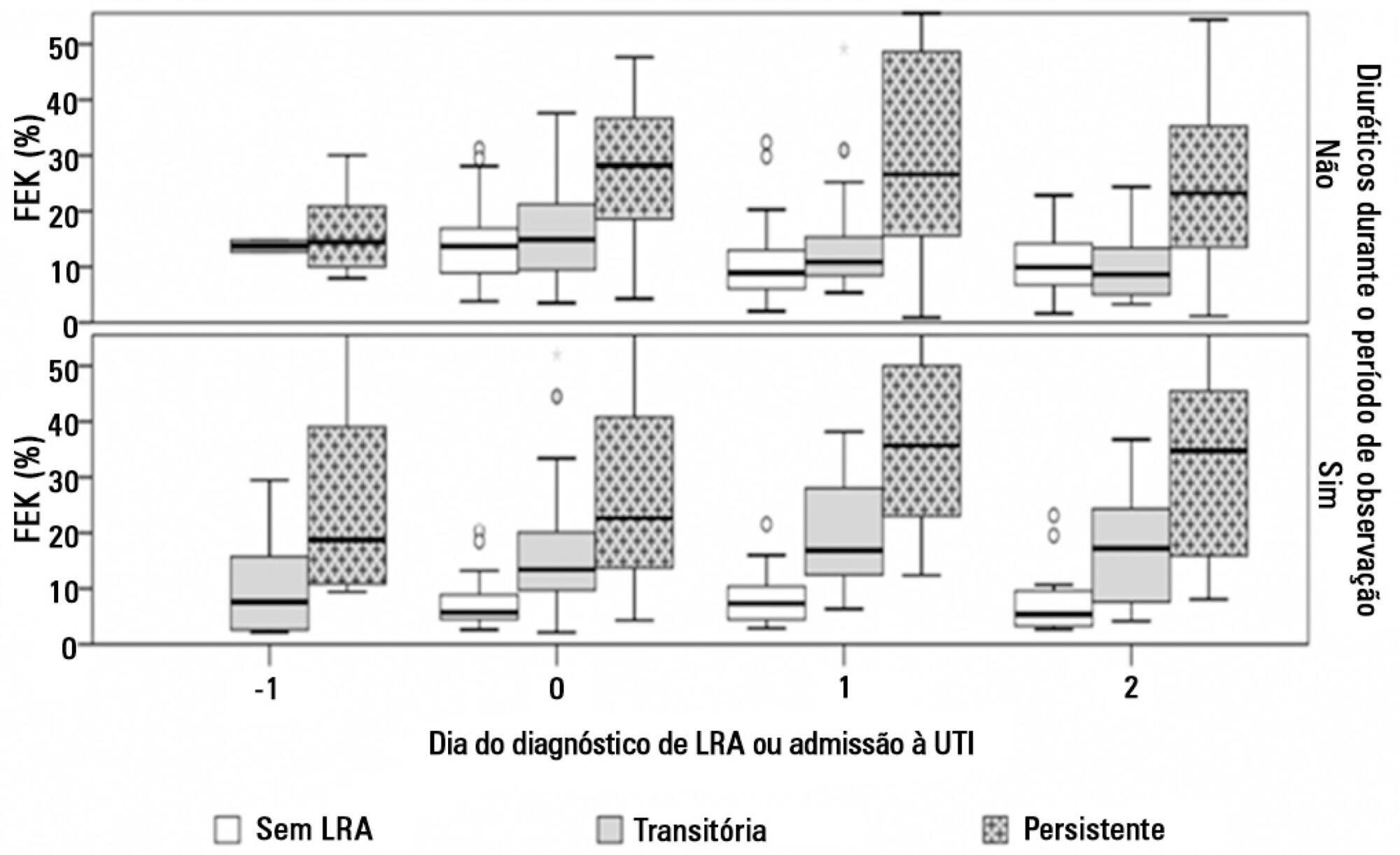
As part of a larger study in which we have evaluated blood and urinary parameters in the course of acute kidney injury, 168 patients were included. Blood and urine samples were collected daily until the removal of the urinary catheter or the initiation of renal replacement therapy. We describe the evolution of fractional excretion of potassium based on whether acute kidney injury was diagnosed, its duration (transient or persistent) and its severity (creatinine-based Acute Kidney Injury Network - AKIN stage). The diagnostic performance of fractional excretion of potassium in predicting the duration of acute kidney injury and the need for renal replacement therapy on the day of acute kidney injury diagnosis was also evaluated.
Fractional excretion of potassium was significantly higher in persistent acute kidney injury compared to transient acute kidney injury on the day of acute kidney injury diagnosis (24.8 vs. 13.8%, p<0.001). Both groups had the median fractional excretion of potassium increasing in the two days preceding the acute kidney injury diagnosis. Patients without acute kidney injury had stable low fractional excretion of potassium values. The fractional excretion of potassium was fairly accurate in predicting persistent acute kidney injury (area under the curve: 0.712; 95% confidence interval: 0.614-0.811; p<0.001) on the day of acute kidney injury diagnosis. The area under the curve was 0.663 (95% confidence interval: 0.523-0.803; p=0.03) for renal replacement therapy. The fractional excretion of potassium increased with maximum AKIN stage reached, in both transient and persistent acute kidney injury.
Sequential fractional excretion of potassium assessment appears to be useful in critically ill patients at risk for acute kidney injury.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):143-147
DOI 10.5935/0103-507X.20140021
To evaluate the behavior of fractional excretion of potassium in the course of acute kidney injury in critically ill patients.
As part of a larger study in which we have evaluated blood and urinary parameters in the course of acute kidney injury, 168 patients were included. Blood and urine samples were collected daily until the removal of the urinary catheter or the initiation of renal replacement therapy. We describe the evolution of fractional excretion of potassium based on whether acute kidney injury was diagnosed, its duration (transient or persistent) and its severity (creatinine-based Acute Kidney Injury Network - AKIN stage). The diagnostic performance of fractional excretion of potassium in predicting the duration of acute kidney injury and the need for renal replacement therapy on the day of acute kidney injury diagnosis was also evaluated.
Fractional excretion of potassium was significantly higher in persistent acute kidney injury compared to transient acute kidney injury on the day of acute kidney injury diagnosis (24.8 vs. 13.8%, p<0.001). Both groups had the median fractional excretion of potassium increasing in the two days preceding the acute kidney injury diagnosis. Patients without acute kidney injury had stable low fractional excretion of potassium values. The fractional excretion of potassium was fairly accurate in predicting persistent acute kidney injury (area under the curve: 0.712; 95% confidence interval: 0.614-0.811; p<0.001) on the day of acute kidney injury diagnosis. The area under the curve was 0.663 (95% confidence interval: 0.523-0.803; p=0.03) for renal replacement therapy. The fractional excretion of potassium increased with maximum AKIN stage reached, in both transient and persistent acute kidney injury.
Sequential fractional excretion of potassium assessment appears to be useful in critically ill patients at risk for acute kidney injury.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):341-351
DOI 10.1590/S0103-507X2011000300013
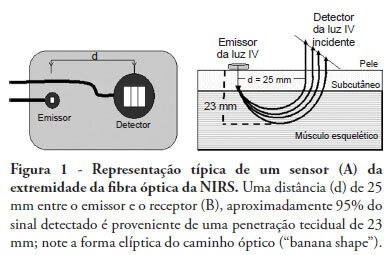
Near infrared spectroscopy (NIRS) is a non-invasive technique that allows determination of tissue oxygenation based on spectro-photometric quantitation of oxy- and deoxyhemoglobin within a tissue. This technique has gained acceptance as a tool to monitor peripheral tissue perfusion in critically ill patient. NIRS principle is based on the use of near-infrared electromagnetic waves for qualitative and quantitative assessments of molecular factors related to tissue oxygenation. Although this technique can be apllied in any tissue, it is primarily used for monitoring peripheral oxygenation in the muscle. Parameters that are determined using NIRS can be either directly calculated or can be derived from physiological interventions, such as arterial and venous occlusions methods. Information regarding muscle oxygen saturation, muscle oxygen consumption and regional blood flow can therefore be obtained. Clinical applications of NIRS include peripheral oxygenation monitoring during resuscitation of trauma and septic shock as well as the assessment of regional microcirculatory disorders. This review provides a brief discussion of NIRS basic principles and main clinical uses of this technique, with a specific focus on studies that assess the usefulness of NIRS in intensive care and emergency patients.
Abstract
Rev Bras Ter Intensiva. 2011;23(3):341-351
DOI 10.1590/S0103-507X2011000300013
Near infrared spectroscopy (NIRS) is a non-invasive technique that allows determination of tissue oxygenation based on spectro-photometric quantitation of oxy- and deoxyhemoglobin within a tissue. This technique has gained acceptance as a tool to monitor peripheral tissue perfusion in critically ill patient. NIRS principle is based on the use of near-infrared electromagnetic waves for qualitative and quantitative assessments of molecular factors related to tissue oxygenation. Although this technique can be apllied in any tissue, it is primarily used for monitoring peripheral oxygenation in the muscle. Parameters that are determined using NIRS can be either directly calculated or can be derived from physiological interventions, such as arterial and venous occlusions methods. Information regarding muscle oxygen saturation, muscle oxygen consumption and regional blood flow can therefore be obtained. Clinical applications of NIRS include peripheral oxygenation monitoring during resuscitation of trauma and septic shock as well as the assessment of regional microcirculatory disorders. This review provides a brief discussion of NIRS basic principles and main clinical uses of this technique, with a specific focus on studies that assess the usefulness of NIRS in intensive care and emergency patients.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
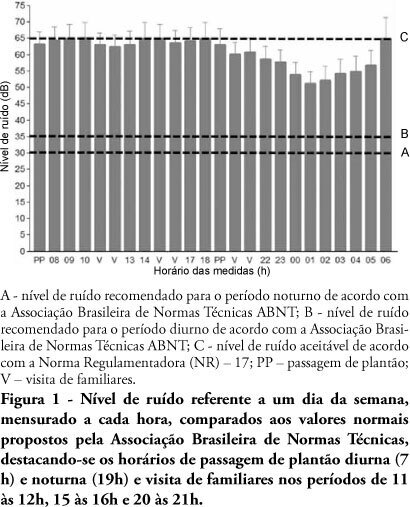
OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit's healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):369-374
DOI 10.1590/S0103-507X2010000400010
OBJECTIVE: The several multidisciplinary team personnel and device alarms make intensive care units noisy environments. This study aimed to measure the noise level of a medical-surgical intensive care unit in Recife, Brazil, and to assess the noise perception by the unit's healthcare professionals. METHODS: A decibel meter was used for continuous every five seconds one week noise levels recording. After this measurement, an interview shaped noise perception questionnaire was applied to the healthcare professionals, approaching the discomfort level and noise control possibilities. RESULTS: Mean 58.21 ± 5.93 dB noise was recorded. The morning noise level was higher than at night (60.85 ± 4.90 versus 55.60 ± 5.98, p <0.001), as well as work-days versus weekend (58. 77 ± 6.05 versus 56.83 ± 5.90, p <0.001). The evening staff shift change noise was louder than by daytime change (62.31 ± 4.70 versus 61.35 ± 5.08 dB; p < 0.001). Of the 73 questionnaire respondents, 97.3% believe that the intensive care unit has moderate or intense noise levels; 50.7% consider the noise harmful; and 98.6% believe that noise levels can be reduced. CONCLUSION: The measured noise levels were above the recommended. Preventive and educational programs approaching the importance of noise levels reduction should be encouraged in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):226-230
DOI 10.1590/S0103-507X2009000200017
Pulmonary artery catheter is frequently used to monitor patients during liver transplantation. Recently developed less invasive methods for estimating cardiac output and pulmonary capillary wedge pressure together with the failure of randomized studies to demonstrate reduced mortality in pulmonary artery catheter-monitored patients, has restricted its applicability. Pulmonary artery rupture by pulmonary artery catheter is a rare, but dangerous complication. The purpose of this report is to describe a pulmonary artery rupture caused by monitorization with a pulmonary artery catheter, reviewing the clinical approach and discussing hemodynamic monitoring with the pulmonary artery catheter during liver transplantation. A 56 year old female patient, with cirrhosis caused by hepatitis C virus (MELD score 26) presented with acute hepatic encephalopathy. She was medicated and received a liver transplantation with invasive monitoring with a pulmonary artery catheter. In the first 24 hours after surgery, the patient presented with hemodynamic instability, low hematocrit, and cardiorespiratory arrest. After cardiopulmonary resuscitation, hemopericardium was diagnosed by transthoracic echocardiography and even after pericardiocentesis the patient developed recurrent hemopericardium. Pulmonary angiography did not disclose large vessellesions. The pulmonary artery rupture diagnosis was only made after sternotomy and direct lesion observation. Complications from use of pulmonary artery catheter are infrequent, however, due to their clinical severity, can cause high morbidity and mortality. A decreased use of pulmonary artery catheter reduced the number of complications observed. New clinical studies comparing pulmonary artery catheter with non-invasive methods for pulmonary capillary wedge pressure measurement must be conducted in liver transplantation.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):226-230
DOI 10.1590/S0103-507X2009000200017
Pulmonary artery catheter is frequently used to monitor patients during liver transplantation. Recently developed less invasive methods for estimating cardiac output and pulmonary capillary wedge pressure together with the failure of randomized studies to demonstrate reduced mortality in pulmonary artery catheter-monitored patients, has restricted its applicability. Pulmonary artery rupture by pulmonary artery catheter is a rare, but dangerous complication. The purpose of this report is to describe a pulmonary artery rupture caused by monitorization with a pulmonary artery catheter, reviewing the clinical approach and discussing hemodynamic monitoring with the pulmonary artery catheter during liver transplantation. A 56 year old female patient, with cirrhosis caused by hepatitis C virus (MELD score 26) presented with acute hepatic encephalopathy. She was medicated and received a liver transplantation with invasive monitoring with a pulmonary artery catheter. In the first 24 hours after surgery, the patient presented with hemodynamic instability, low hematocrit, and cardiorespiratory arrest. After cardiopulmonary resuscitation, hemopericardium was diagnosed by transthoracic echocardiography and even after pericardiocentesis the patient developed recurrent hemopericardium. Pulmonary angiography did not disclose large vessellesions. The pulmonary artery rupture diagnosis was only made after sternotomy and direct lesion observation. Complications from use of pulmonary artery catheter are infrequent, however, due to their clinical severity, can cause high morbidity and mortality. A decreased use of pulmonary artery catheter reduced the number of complications observed. New clinical studies comparing pulmonary artery catheter with non-invasive methods for pulmonary capillary wedge pressure measurement must be conducted in liver transplantation.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):161-169
DOI 10.1590/S0103-507X2007000200004
BACKGROUND AND OBJECTIVES: In mechanical ventilation, invasive and noninvasive, the knowledge of respiratory mechanic physiology is indispensable to take decisions and into the efficient management of modern ventilators. Monitoring of pulmonary mechanic parameters is been recommended from all the review works and clinical research. The objective of this study was review concepts of pulmonary mechanic and the methods used to obtain measures in the bed side, preparing a rational sequence to obtain this data. METHODS: It was obtained bibliographic review through data bank LILACS, MedLine and PubMed, from the last ten years. RESULTS: This review approaches parameters of resistance, pulmonary compliance and intrinsic PEEP as primordial into comprehension of acute respiratory failure and mechanic ventilatory support, mainly in acute respiratory distress syndrome (ARDS) and in chronic obstructive pulmonary disease (COPD). CONCLUSIONS: Monitoring pulmonary mechanics in patients under mechanical ventilation in intensive care units gives relevant informations and should be implemented in a rational and systematic way.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):161-169
DOI 10.1590/S0103-507X2007000200004
BACKGROUND AND OBJECTIVES: In mechanical ventilation, invasive and noninvasive, the knowledge of respiratory mechanic physiology is indispensable to take decisions and into the efficient management of modern ventilators. Monitoring of pulmonary mechanic parameters is been recommended from all the review works and clinical research. The objective of this study was review concepts of pulmonary mechanic and the methods used to obtain measures in the bed side, preparing a rational sequence to obtain this data. METHODS: It was obtained bibliographic review through data bank LILACS, MedLine and PubMed, from the last ten years. RESULTS: This review approaches parameters of resistance, pulmonary compliance and intrinsic PEEP as primordial into comprehension of acute respiratory failure and mechanic ventilatory support, mainly in acute respiratory distress syndrome (ARDS) and in chronic obstructive pulmonary disease (COPD). CONCLUSIONS: Monitoring pulmonary mechanics in patients under mechanical ventilation in intensive care units gives relevant informations and should be implemented in a rational and systematic way.