Child Archives - Critical Care Science (CCS)

Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(3):286-293
DOI 10.5935/0103-507X.20180051
This study aimed to study the incidence of stress hyperglycemia in critically ill children and to investigate the etiological basis of the hyperglycemia based on homeostasis model assessment.
This was a prospective cohort study in one of the pediatric intensive care units of Cairo University, including 60 critically ill children and 21 healthy controls. Serum blood glucose, insulin, and C-peptide levels were measured within 24 hours of admission. Homeostasis model assessment was used to assess β-cell function and insulin sensitivity.
Hyperglycemia was estimated in 70% of patients. Blood glucose values ≥ 180mg/dL were associated with a poor outcome. Blood glucose levels were positively correlated with Pediatric Risk for Mortality (PRISM III) score and number of organ dysfunctions (p = 0.019 and p = 0.022, respectively), while insulin levels were negatively correlated with number of organ dysfunctions (r = −0.33, p = 0.01). Homeostasis model assessment revealed that 26 (43.3%) of the critically ill patients had low β-cell function, and 18 (30%) had low insulin sensitivity. Combined pathology was detected in 2 (3.3%) patients only. Low β-cell function was significantly associated with the presence of multi-organ dysfunction; respiratory, cardiovascular, and hematological dysfunctions; and the presence of sepsis.
β-Cell dysfunction appeared to be prevalent in our cohort and was associated with multi-organ dysfunction.
Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(3):286-293
DOI 10.5935/0103-507X.20180051
This study aimed to study the incidence of stress hyperglycemia in critically ill children and to investigate the etiological basis of the hyperglycemia based on homeostasis model assessment.
This was a prospective cohort study in one of the pediatric intensive care units of Cairo University, including 60 critically ill children and 21 healthy controls. Serum blood glucose, insulin, and C-peptide levels were measured within 24 hours of admission. Homeostasis model assessment was used to assess β-cell function and insulin sensitivity.
Hyperglycemia was estimated in 70% of patients. Blood glucose values ≥ 180mg/dL were associated with a poor outcome. Blood glucose levels were positively correlated with Pediatric Risk for Mortality (PRISM III) score and number of organ dysfunctions (p = 0.019 and p = 0.022, respectively), while insulin levels were negatively correlated with number of organ dysfunctions (r = −0.33, p = 0.01). Homeostasis model assessment revealed that 26 (43.3%) of the critically ill patients had low β-cell function, and 18 (30%) had low insulin sensitivity. Combined pathology was detected in 2 (3.3%) patients only. Low β-cell function was significantly associated with the presence of multi-organ dysfunction; respiratory, cardiovascular, and hematological dysfunctions; and the presence of sepsis.
β-Cell dysfunction appeared to be prevalent in our cohort and was associated with multi-organ dysfunction.
Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
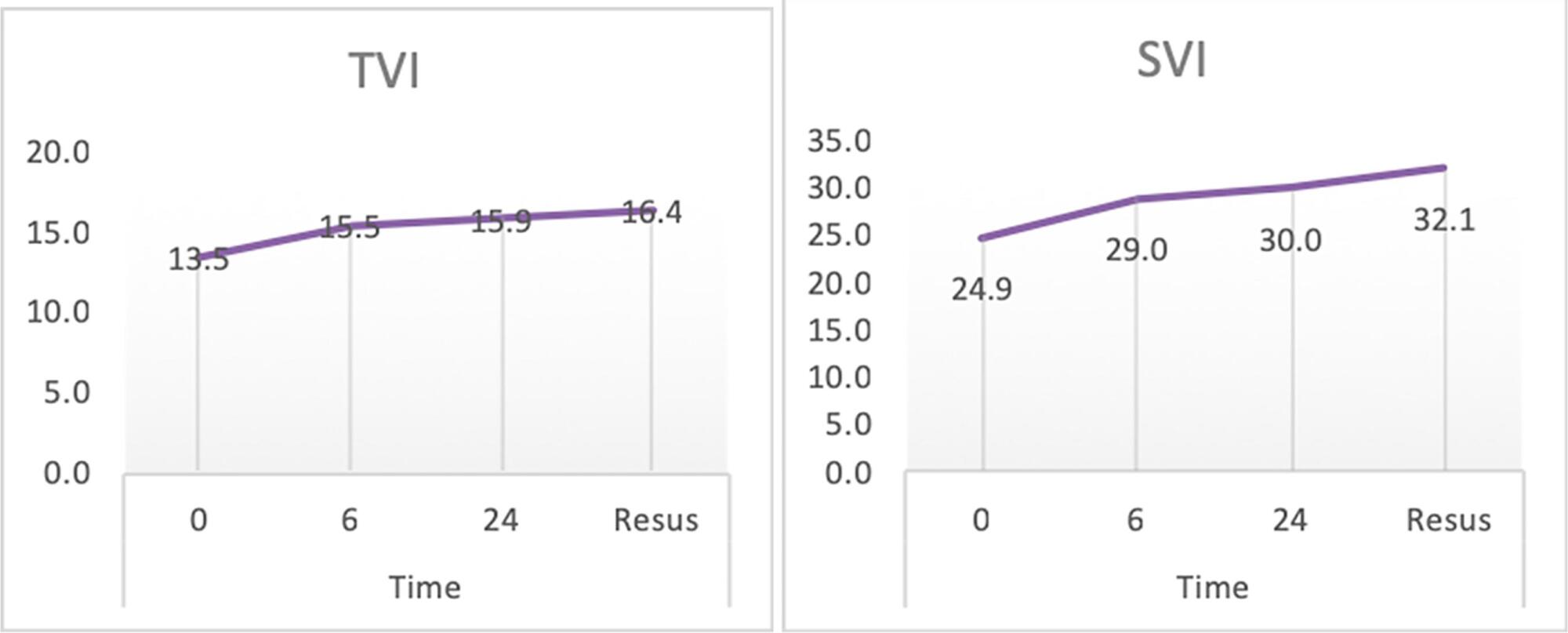
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(4):460-470
DOI 10.5935/0103-507X.20180067
Follow-up of cardiac index and systemic vascular resistance index by bedside echocardiography until resuscitation.
A set of hemodynamic parameters was obtained, including cardiac output, stroke volume, cardiac index, systemic vascular resistance index, velocity time integral, myocardial performance index, capillary refill time, and heart rate at 0 hours after fluid boluses before the start of inotropes, and followed up after 6 hours and 24 hours.
Included were 45 patients with community-acquired septic shock. Septic foci were gastroenteritis (24%), intestinal perforation requiring emergency surgery (24%), pneumonia (20%), central nervous system infection (22%) and soft tissue infection (8%). Klebsiella and Enterobacter were the most frequent isolates. We estimated the factors affecting the cardiac index: high central venous pressure at zero time (r = 0.33, p = 0.024) and persistently high heart rate at hour 6 (r = 0.33, p = 0.03). The systemic vascular resistance index was high in most patients at 0 and 24 hours and at the time of resuscitation and inversely affected the cardiac index as well as affecting the velocity time integral (r = -0.416, -0.61, 0.55 and -0.295). Prolonged capillary refill time was a clinical predictor of the low velocity time integral at 24 hours (r = -0.4). The mortality was 27%. Lower systemic vascular resistance index and higher cardiac output were observed in nonsurviving patients.
There was a persistently high systemic vascular resistance index in cold shock patients that influenced the stroke volume index, cardiac index, and velocity time integral. The use of echocardiograms for hemodynamic measurements is important in pediatric septic shock patients to adjust dilators, and vasopressor doses and achieve resuscitation targets in a timely manner.
Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(2):226-232
DOI 10.5935/0103-507X.20180039
In an ethical dilemma, there is always an option that can be identified as the best one to be chosen. When it is impossible to adopt such option, the situation can lead professionals to experience moral distress. This review aims to define the issue of moral distress and propose coping strategies. Systematic searches in the MEDLINE/PubMed and SciELO databases were conducted using the keywords "moral distress" and "moral suffering" in articles published between 2000 and 2017. This review was non-exhaustive and contextual, with a focus on definitions, etiologies and methods of resolution for moral distress. In the daily practice of intensive care, moral distress was commonly related to the prolongation of patients' suffering and feelings of helplessness, as well as difficulties in communication among team members. Coping strategies for moral distress included organizational, personal and administrative actions. Actions such as workload management, mutual support among professionals and the development of techniques to cultivate open communication, reflection and questioning within the multidisciplinary team were identified. In clinical practice, health professionals need to be recognized as moral agents, and the development of moral courage was considered helpful to overcome ethical dilemmas and interprofessional conflicts. Both in pediatric and adult intensive care, professionals are challenged by questions about their practice, and they may experience moral distress. This suffering can be minimized and solved by understanding that the focus is always on the patient and acting with moral courage and good communication in an environment of mutual respect.
Abstract
Revista Brasileira de Terapia Intensiva. 2018;30(2):226-232
DOI 10.5935/0103-507X.20180039
In an ethical dilemma, there is always an option that can be identified as the best one to be chosen. When it is impossible to adopt such option, the situation can lead professionals to experience moral distress. This review aims to define the issue of moral distress and propose coping strategies. Systematic searches in the MEDLINE/PubMed and SciELO databases were conducted using the keywords "moral distress" and "moral suffering" in articles published between 2000 and 2017. This review was non-exhaustive and contextual, with a focus on definitions, etiologies and methods of resolution for moral distress. In the daily practice of intensive care, moral distress was commonly related to the prolongation of patients' suffering and feelings of helplessness, as well as difficulties in communication among team members. Coping strategies for moral distress included organizational, personal and administrative actions. Actions such as workload management, mutual support among professionals and the development of techniques to cultivate open communication, reflection and questioning within the multidisciplinary team were identified. In clinical practice, health professionals need to be recognized as moral agents, and the development of moral courage was considered helpful to overcome ethical dilemmas and interprofessional conflicts. Both in pediatric and adult intensive care, professionals are challenged by questions about their practice, and they may experience moral distress. This suffering can be minimized and solved by understanding that the focus is always on the patient and acting with moral courage and good communication in an environment of mutual respect.
Abstract
Revista Brasileira de Terapia Intensiva. 2017;29(4):460-465
DOI 10.5935/0103-507X.20170066
To evaluate the functional status of pediatric patients after discharge from the pediatric intensive care unit using the Functional Status Scale and to compare the time of invasive mechanical ventilation, length of stay in the pediatric intensive care unit, and Pediatric Index of Mortality 2 results among individuals with different degrees of functional impairment.
A cross-sectional study was conducted on patients who were discharged from a pediatric intensive care unit. The functional evaluation by the Functional Status Scale was performed on the first day after discharge from the unit, and the Pediatric Index of Mortality 2 was used to predict the mortality rate at the time of admission to the pediatric intensive care unit.
The sample consisted of 50 individuals, 60% of which were male, with a median age of 19 [6 - 61] months. The overall score of the Functional Status Scale was 11.5 [7 - 15], and the highest scores were observed in the "motor function" 3 [1 - 4] and "feeding" 4 [1 - 4] domains. Compared to patients who were not readmitted to the pediatric intensive care unit, patients who were readmitted presented a worse overall score (p = 0.01), worse scores in the "motor function" (p = 0.01), "feeding" (p = 0.02), and "respiratory" (p = 0.036) domains, and a higher mortality rate according to the Pediatric Index of Mortality 2 (p = 0.025).
Evaluation of the functional status using the Functional Status Scale indicated moderate impairment in patients after discharge from the pediatric intensive care unit, mainly in the "motor function" and "feeding" domains; patients who were readmitted to the pediatric intensive care unit demonstrated worse overall functional, motor function, feeding and respiratory scores. Individuals with greater functional impairment had longer times of invasive mechanical ventilation and hospitalization in the pediatric intensive care unit.
Abstract
Revista Brasileira de Terapia Intensiva. 2017;29(4):460-465
DOI 10.5935/0103-507X.20170066
To evaluate the functional status of pediatric patients after discharge from the pediatric intensive care unit using the Functional Status Scale and to compare the time of invasive mechanical ventilation, length of stay in the pediatric intensive care unit, and Pediatric Index of Mortality 2 results among individuals with different degrees of functional impairment.
A cross-sectional study was conducted on patients who were discharged from a pediatric intensive care unit. The functional evaluation by the Functional Status Scale was performed on the first day after discharge from the unit, and the Pediatric Index of Mortality 2 was used to predict the mortality rate at the time of admission to the pediatric intensive care unit.
The sample consisted of 50 individuals, 60% of which were male, with a median age of 19 [6 - 61] months. The overall score of the Functional Status Scale was 11.5 [7 - 15], and the highest scores were observed in the "motor function" 3 [1 - 4] and "feeding" 4 [1 - 4] domains. Compared to patients who were not readmitted to the pediatric intensive care unit, patients who were readmitted presented a worse overall score (p = 0.01), worse scores in the "motor function" (p = 0.01), "feeding" (p = 0.02), and "respiratory" (p = 0.036) domains, and a higher mortality rate according to the Pediatric Index of Mortality 2 (p = 0.025).
Evaluation of the functional status using the Functional Status Scale indicated moderate impairment in patients after discharge from the pediatric intensive care unit, mainly in the "motor function" and "feeding" domains; patients who were readmitted to the pediatric intensive care unit demonstrated worse overall functional, motor function, feeding and respiratory scores. Individuals with greater functional impairment had longer times of invasive mechanical ventilation and hospitalization in the pediatric intensive care unit.
Abstract
Revista Brasileira de Terapia Intensiva. 2017;29(2):206-212
DOI 10.5935/0103-507X.20170029
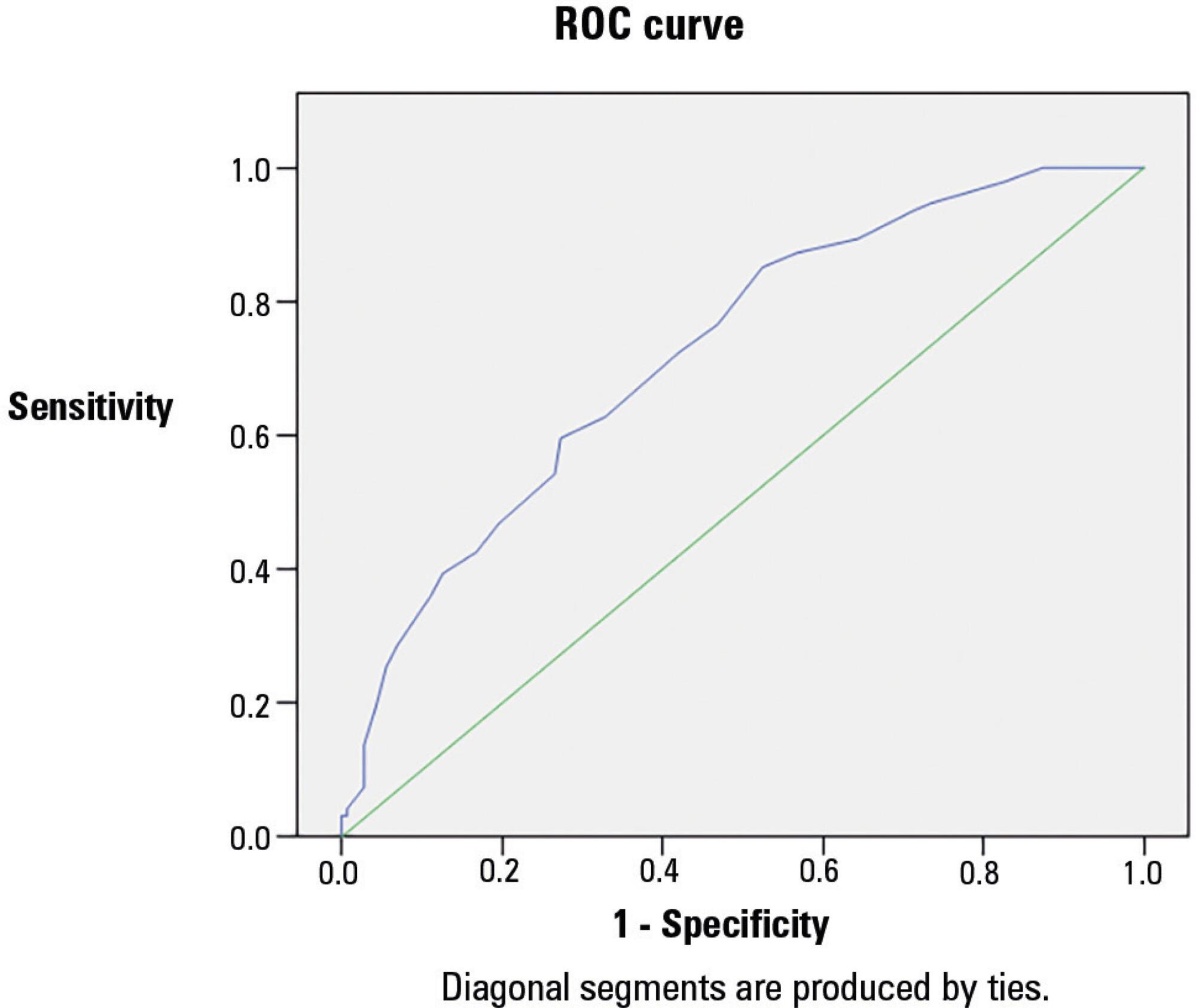
To assess the frequency of primary multiple organ failure and the role of sepsis as a causative agent in critically ill pediatric patients; and calculate and evaluate the accuracy of the Pediatric Risk of Mortality III (PRISM III) and Pediatric Logistic Organ Dysfunction (PELOD) scores to predict the outcomes of critically ill children.
Retrospective study, which evaluated data from patients admitted from January to December 2011 in the pediatric intensive care unit of the Children's Hospital of the University of Cairo.
Out of 237 patients in the study, 72% had multiple organ dysfunctions, and 45% had sepsis with multiple organ dysfunctions. The mortality rate in patients with multiple organ dysfunction was 73%. Independent risk factors for death were mechanical ventilation and neurological failure [OR: 36 and 3.3, respectively]. The PRISM III score was more accurate than the PELOD score in predicting death, with a Hosmer-Lemeshow X2 (Chi-square value) of 7.3 (df = 8, p = 0.5). The area under the curve was 0.723 for PRISM III and 0.78 for PELOD.
A multiple organ dysfunctions was associated with high mortality. Sepsis was the major cause. Pneumonia, diarrhea and central nervous system infections were the major causes of sepsis. PRISM III had a better calibration than the PELOD for prognosis of the patients, despite the high frequency of the multiple organ dysfunction syndrome.
Abstract
Revista Brasileira de Terapia Intensiva. 2017;29(2):206-212
DOI 10.5935/0103-507X.20170029
To assess the frequency of primary multiple organ failure and the role of sepsis as a causative agent in critically ill pediatric patients; and calculate and evaluate the accuracy of the Pediatric Risk of Mortality III (PRISM III) and Pediatric Logistic Organ Dysfunction (PELOD) scores to predict the outcomes of critically ill children.
Retrospective study, which evaluated data from patients admitted from January to December 2011 in the pediatric intensive care unit of the Children's Hospital of the University of Cairo.
Out of 237 patients in the study, 72% had multiple organ dysfunctions, and 45% had sepsis with multiple organ dysfunctions. The mortality rate in patients with multiple organ dysfunction was 73%. Independent risk factors for death were mechanical ventilation and neurological failure [OR: 36 and 3.3, respectively]. The PRISM III score was more accurate than the PELOD score in predicting death, with a Hosmer-Lemeshow X2 (Chi-square value) of 7.3 (df = 8, p = 0.5). The area under the curve was 0.723 for PRISM III and 0.78 for PELOD.
A multiple organ dysfunctions was associated with high mortality. Sepsis was the major cause. Pneumonia, diarrhea and central nervous system infections were the major causes of sepsis. PRISM III had a better calibration than the PELOD for prognosis of the patients, despite the high frequency of the multiple organ dysfunction syndrome.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(2):167-178
DOI 10.5935/0103-507X.20160020
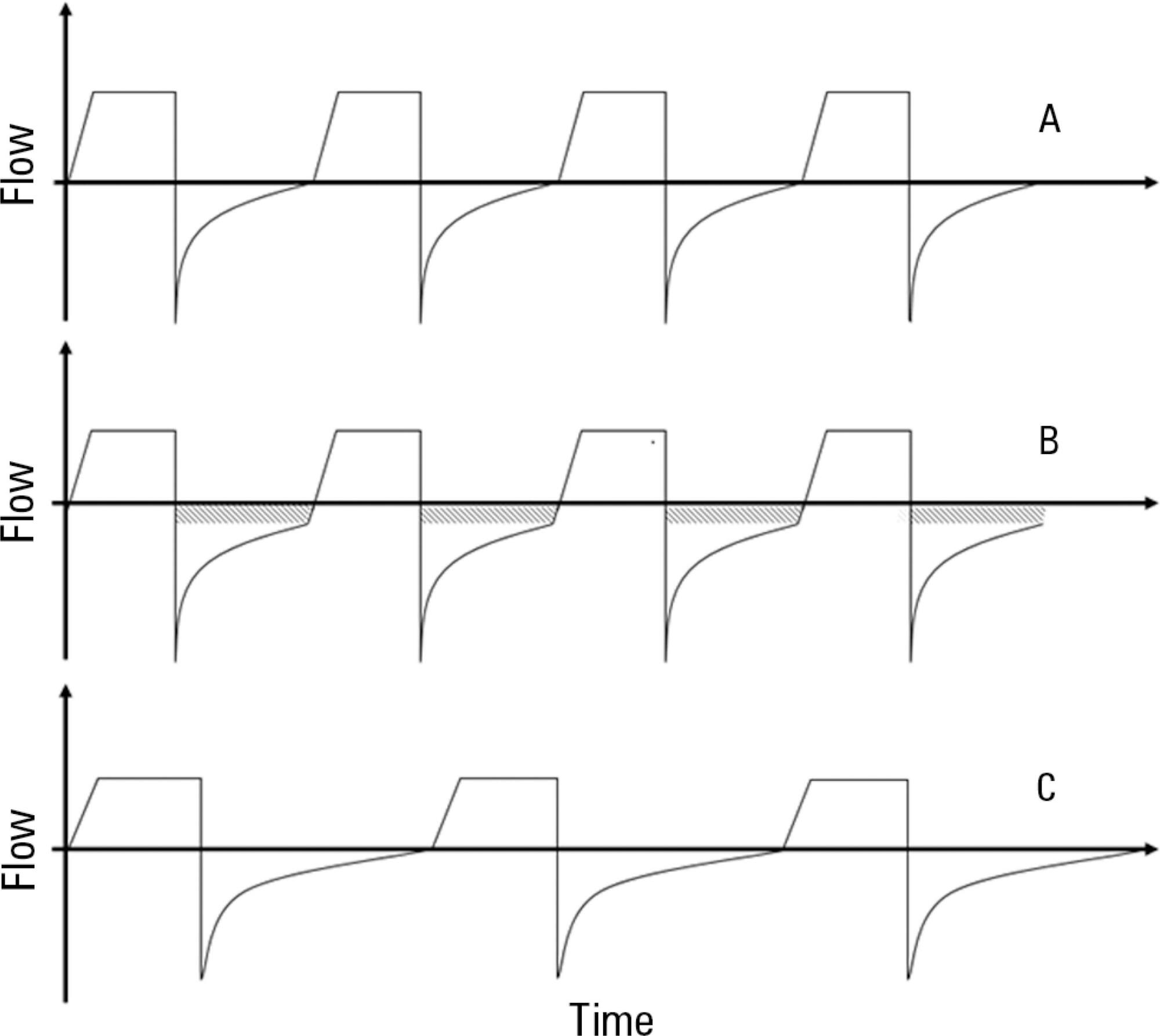
Asthma is the most common chronic illness in childhood. Although the vast majority of children with acute asthma exacerbations do not require critical care, some fail to respond to standard treatment and require escalation of support. Children with critical or near-fatal asthma require close monitoring for deterioration and may require aggressive treatment strategies. This review examines the available evidence supporting therapies for critical and near-fatal asthma and summarizes the contemporary clinical care of these children. Typical treatment includes parenteral corticosteroids and inhaled or intravenous beta-agonist drugs. For children with an inadequate response to standard therapy, inhaled ipratropium bromide, intravenous magnesium sulfate, methylxanthines, helium-oxygen mixtures, and non-invasive mechanical support can be used. Patients with progressive respiratory failure benefit from mechanical ventilation with a strategy that employs large tidal volumes and low ventilator rates to minimize dynamic hyperinflation, barotrauma, and hypotension. Sedatives, analgesics and a neuromuscular blocker are often necessary in the early phase of treatment to facilitate a state of controlled hypoventilation and permissive hypercapnia. Patients who fail to improve with mechanical ventilation may be considered for less common approaches, such as inhaled anesthetics, bronchoscopy, and extracorporeal life support. This contemporary approach has resulted in extremely low mortality rates, even in children requiring mechanical support.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(2):167-178
DOI 10.5935/0103-507X.20160020
Asthma is the most common chronic illness in childhood. Although the vast majority of children with acute asthma exacerbations do not require critical care, some fail to respond to standard treatment and require escalation of support. Children with critical or near-fatal asthma require close monitoring for deterioration and may require aggressive treatment strategies. This review examines the available evidence supporting therapies for critical and near-fatal asthma and summarizes the contemporary clinical care of these children. Typical treatment includes parenteral corticosteroids and inhaled or intravenous beta-agonist drugs. For children with an inadequate response to standard therapy, inhaled ipratropium bromide, intravenous magnesium sulfate, methylxanthines, helium-oxygen mixtures, and non-invasive mechanical support can be used. Patients with progressive respiratory failure benefit from mechanical ventilation with a strategy that employs large tidal volumes and low ventilator rates to minimize dynamic hyperinflation, barotrauma, and hypotension. Sedatives, analgesics and a neuromuscular blocker are often necessary in the early phase of treatment to facilitate a state of controlled hypoventilation and permissive hypercapnia. Patients who fail to improve with mechanical ventilation may be considered for less common approaches, such as inhaled anesthetics, bronchoscopy, and extracorporeal life support. This contemporary approach has resulted in extremely low mortality rates, even in children requiring mechanical support.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(4):436-443
DOI 10.5935/0103-507X.20160077
To evaluate the clinical course and respiratory parameters of mechanically ventilated children with cancer suffering from sepsis-related acute respiratory distress syndrome.
This 2-year prospective, longitudinal, observational cohort study enrolled 29 children and adolescents. Clinical data, measurements of blood gases and ventilation parameters were collected at four different time points. Fluctuations between measurements as well as differences in estimated means were analyzed by linear mixed models in which death within 28 days from the onset of acute respiratory distress syndrome was the primary endpoint.
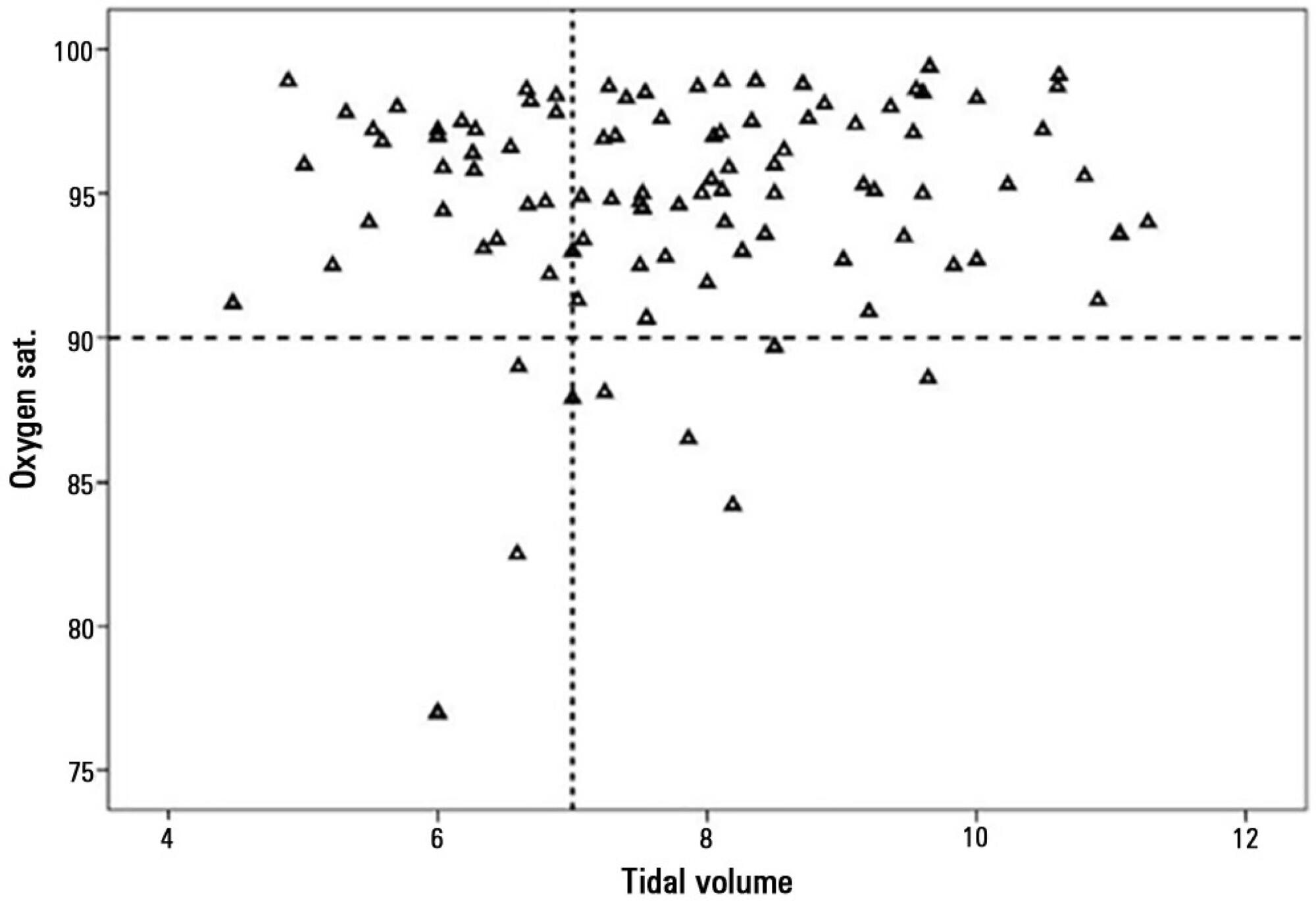
There were 17 deaths within 28 days of acute respiratory distress syndrome onset and another 7 between 29 - 60 days. Only 5 patients survived for more than 60 days. Nine (31%) patients died as a direct consequence of refractory hypoxemia, and the others died of multiple organ failure and catecholamine-refractory shock. In 66% of the measurements, the tidal volume required to obtain oxygen saturation equal to or above 90% was greater than 7mL/kg. The estimated means of dynamic compliance were low and were similar for survivors and non-survivors but with a negative slope between the first and final measurements, accompanied by a negative slope of the tidal volume for non-survivors. Non-survivors were significantly more hypoxemic, with PaO2/FiO2 ratios showing lower estimated means and a negative slope along the four measurements. Peak, expiratory and mean airway pressures showed positive slopes in the non-survivors, who also had more metabolic acidosis.
In most of our children with cancer, sepsis and acute respiratory distress syndrome progressed with deteriorating ventilation indexes and escalating organic dysfunction, making this triad nearly fatal in children.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(4):436-443
DOI 10.5935/0103-507X.20160077
To evaluate the clinical course and respiratory parameters of mechanically ventilated children with cancer suffering from sepsis-related acute respiratory distress syndrome.
This 2-year prospective, longitudinal, observational cohort study enrolled 29 children and adolescents. Clinical data, measurements of blood gases and ventilation parameters were collected at four different time points. Fluctuations between measurements as well as differences in estimated means were analyzed by linear mixed models in which death within 28 days from the onset of acute respiratory distress syndrome was the primary endpoint.
There were 17 deaths within 28 days of acute respiratory distress syndrome onset and another 7 between 29 - 60 days. Only 5 patients survived for more than 60 days. Nine (31%) patients died as a direct consequence of refractory hypoxemia, and the others died of multiple organ failure and catecholamine-refractory shock. In 66% of the measurements, the tidal volume required to obtain oxygen saturation equal to or above 90% was greater than 7mL/kg. The estimated means of dynamic compliance were low and were similar for survivors and non-survivors but with a negative slope between the first and final measurements, accompanied by a negative slope of the tidal volume for non-survivors. Non-survivors were significantly more hypoxemic, with PaO2/FiO2 ratios showing lower estimated means and a negative slope along the four measurements. Peak, expiratory and mean airway pressures showed positive slopes in the non-survivors, who also had more metabolic acidosis.
In most of our children with cancer, sepsis and acute respiratory distress syndrome progressed with deteriorating ventilation indexes and escalating organic dysfunction, making this triad nearly fatal in children.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(1):55-61
DOI 10.5935/0103-507X.20160003
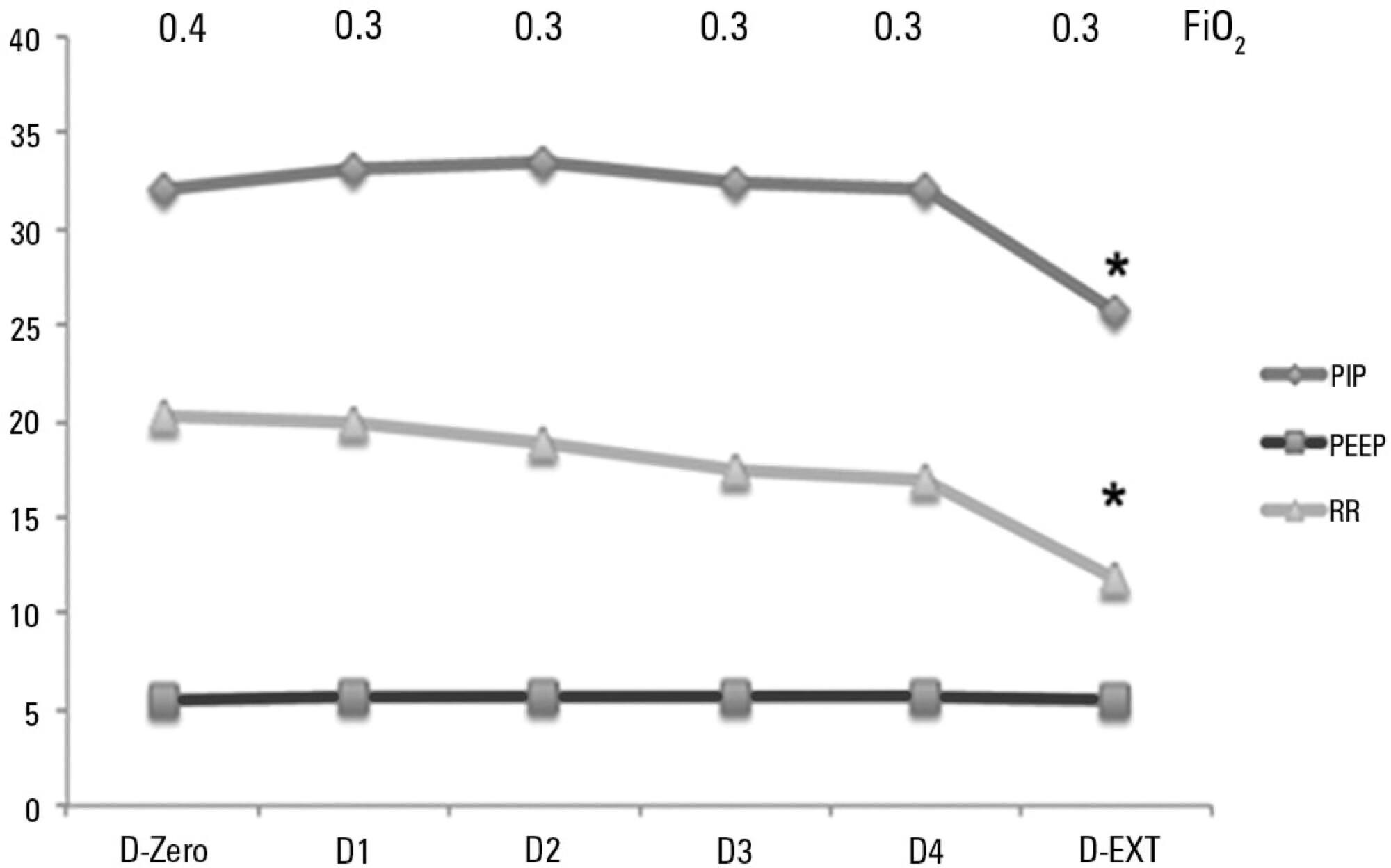
To analyze the characteristics of children with acute viral bronchiolitis subjected to mechanical ventilation for three consecutive years and to correlate their progression with mechanical ventilation parameters and fluid balance.
Longitudinal study of a series of infants (< one year old) subjected to mechanical ventilation for acute viral bronchitis from January 2012 to September 2014 in the pediatric intensive care unit. The children's clinical records were reviewed, and their anthropometric data, mechanical ventilation parameters, fluid balance, clinical progression, and major complications were recorded.
Sixty-six infants (3.0 ± 2.0 months old and with an average weight of 4.7 ± 1.4kg) were included, of whom 62% were boys; a virus was identified in 86%. The average duration of mechanical ventilation was 6.5 ± 2.9 days, and the average length of stay in the pediatric intensive care unit was 9.1 ± 3.5 days; the mortality rate was 1.5% (1/66). The peak inspiratory pressure remained at 30cmH2O during the first four days of mechanical ventilation and then decreased before extubation (25 cmH2O; p < 0.05). Pneumothorax occurred in 10% of the sample and extubation failure in 9%, which was due to upper airway obstruction in half of the cases. The cumulative fluid balance on mechanical ventilation day four was 402 ± 254mL, which corresponds to an increase of 9.0 ± 5.9% in body weight. Thirty-seven patients (56%) exhibited a weight gain of 10% or more, which was not significantly associated with the ventilation parameters on mechanical ventilation day four, extubation failure, duration of mechanical ventilation or length of stay in the pediatric intensive care unit.
The rate of mechanical ventilation for acute viral bronchiolitis remains constant, being associated with low mortality, few adverse effects, and positive cumulative fluid balance during the first days. Better fluid control might reduce the duration of mechanical ventilation.
Abstract
Revista Brasileira de Terapia Intensiva. 2016;28(1):55-61
DOI 10.5935/0103-507X.20160003
To analyze the characteristics of children with acute viral bronchiolitis subjected to mechanical ventilation for three consecutive years and to correlate their progression with mechanical ventilation parameters and fluid balance.
Longitudinal study of a series of infants (< one year old) subjected to mechanical ventilation for acute viral bronchitis from January 2012 to September 2014 in the pediatric intensive care unit. The children's clinical records were reviewed, and their anthropometric data, mechanical ventilation parameters, fluid balance, clinical progression, and major complications were recorded.
Sixty-six infants (3.0 ± 2.0 months old and with an average weight of 4.7 ± 1.4kg) were included, of whom 62% were boys; a virus was identified in 86%. The average duration of mechanical ventilation was 6.5 ± 2.9 days, and the average length of stay in the pediatric intensive care unit was 9.1 ± 3.5 days; the mortality rate was 1.5% (1/66). The peak inspiratory pressure remained at 30cmH2O during the first four days of mechanical ventilation and then decreased before extubation (25 cmH2O; p < 0.05). Pneumothorax occurred in 10% of the sample and extubation failure in 9%, which was due to upper airway obstruction in half of the cases. The cumulative fluid balance on mechanical ventilation day four was 402 ± 254mL, which corresponds to an increase of 9.0 ± 5.9% in body weight. Thirty-seven patients (56%) exhibited a weight gain of 10% or more, which was not significantly associated with the ventilation parameters on mechanical ventilation day four, extubation failure, duration of mechanical ventilation or length of stay in the pediatric intensive care unit.
The rate of mechanical ventilation for acute viral bronchiolitis remains constant, being associated with low mortality, few adverse effects, and positive cumulative fluid balance during the first days. Better fluid control might reduce the duration of mechanical ventilation.