acute respiratory distress syndrome Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2017;29(2):142-153
DOI 10.5935/0103-507X.20170024
The Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) is an international multicenter randomized pragmatic controlled trial with allocation concealment involving 120 intensive care units in Brazil, Argentina, Colombia, Italy, Poland, Portugal, Malaysia, Spain, and Uruguay. The primary objective of ART is to determine whether maximum stepwise alveolar recruitment associated with PEEP titration, adjusted according to the static compliance of the respiratory system (ART strategy), is able to increase 28-day survival in patients with acute respiratory distress syndrome compared to conventional treatment (ARDSNet strategy).
To describe the data management process and statistical analysis plan.
The statistical analysis plan was designed by the trial executive committee and reviewed and approved by the trial steering committee. We provide an overview of the trial design with a special focus on describing the primary (28-day survival) and secondary outcomes. We describe our data management process, data monitoring committee, interim analyses, and sample size calculation. We describe our planned statistical analyses for primary and secondary outcomes as well as pre-specified subgroup analyses. We also provide details for presenting results, including mock tables for baseline characteristics, adherence to the protocol and effect on clinical outcomes.
According to best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and beginning analyses. We anticipate that this document will prevent analysis bias and enhance the utility of the reported results.
ClinicalTrials.gov number, NCT01374022.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):142-153
DOI 10.5935/0103-507X.20170024
The Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) is an international multicenter randomized pragmatic controlled trial with allocation concealment involving 120 intensive care units in Brazil, Argentina, Colombia, Italy, Poland, Portugal, Malaysia, Spain, and Uruguay. The primary objective of ART is to determine whether maximum stepwise alveolar recruitment associated with PEEP titration, adjusted according to the static compliance of the respiratory system (ART strategy), is able to increase 28-day survival in patients with acute respiratory distress syndrome compared to conventional treatment (ARDSNet strategy).
To describe the data management process and statistical analysis plan.
The statistical analysis plan was designed by the trial executive committee and reviewed and approved by the trial steering committee. We provide an overview of the trial design with a special focus on describing the primary (28-day survival) and secondary outcomes. We describe our data management process, data monitoring committee, interim analyses, and sample size calculation. We describe our planned statistical analyses for primary and secondary outcomes as well as pre-specified subgroup analyses. We also provide details for presenting results, including mock tables for baseline characteristics, adherence to the protocol and effect on clinical outcomes.
According to best trial practice, we report our statistical analysis plan and data management plan prior to locking the database and beginning analyses. We anticipate that this document will prevent analysis bias and enhance the utility of the reported results.
ClinicalTrials.gov number, NCT01374022.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms "variable ventilation" OR "noisy ventilation" OR "biologically variable ventilation".
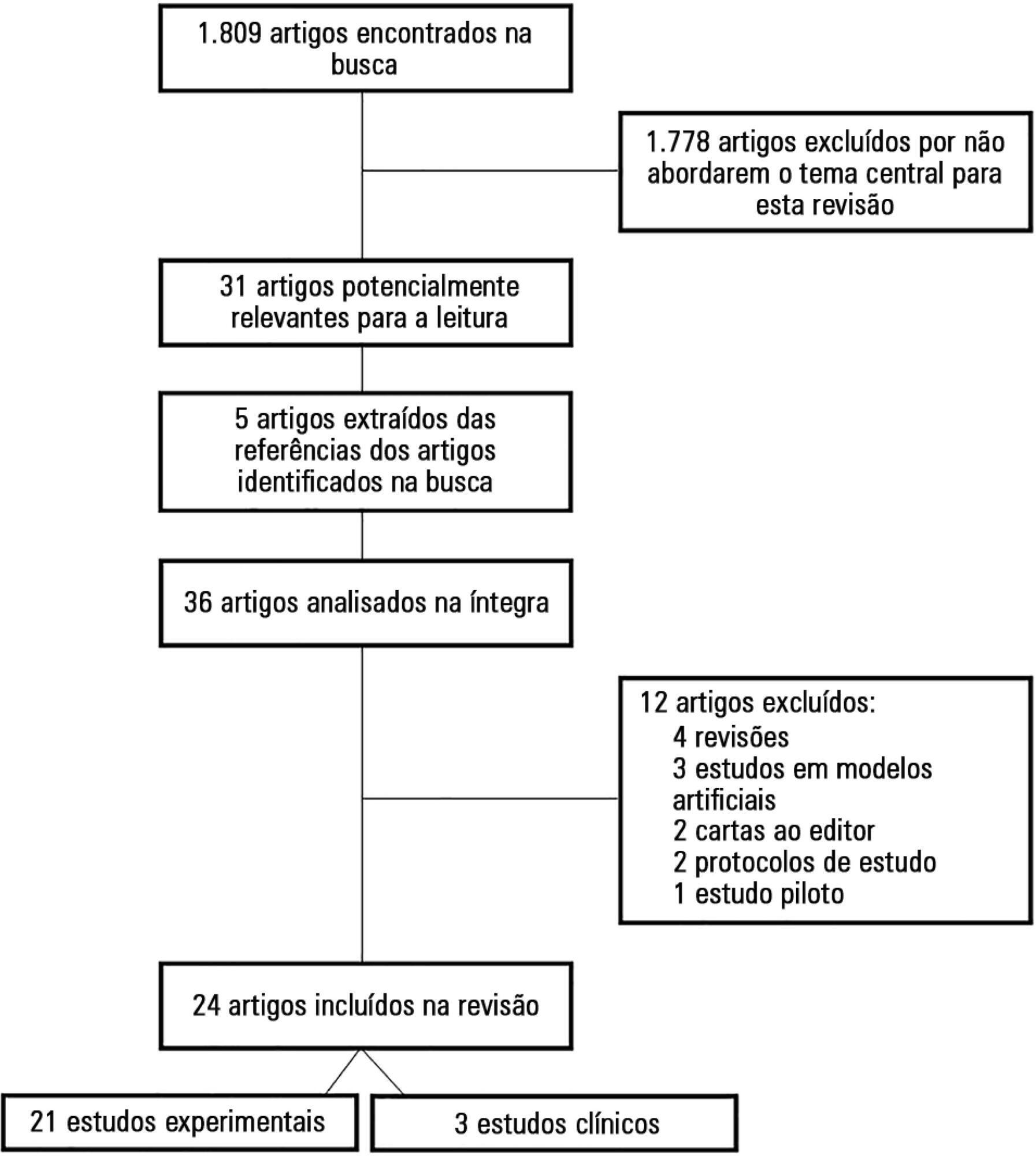
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2017;29(1):77-86
DOI 10.5935/0103-507X.20170012
To review the literature on the use of variable mechanical ventilation and the main outcomes of this technique.
Search, selection, and analysis of all original articles on variable ventilation, without restriction on the period of publication and language, available in the electronic databases LILACS, MEDLINE®, and PubMed, by searching the terms "variable ventilation" OR "noisy ventilation" OR "biologically variable ventilation".
A total of 36 studies were selected. Of these, 24 were original studies, including 21 experimental studies and three clinical studies.
Several experimental studies reported the beneficial effects of distinct variable ventilation strategies on lung function using different models of lung injury and healthy lungs. Variable ventilation seems to be a viable strategy for improving gas exchange and respiratory mechanics and preventing lung injury associated with mechanical ventilation. However, further clinical studies are necessary to assess the potential of variable ventilation strategies for the clinical improvement of patients undergoing mechanical ventilation.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):231-237
DOI 10.5935/0103-507X.20170032
Overdistention and intratidal alveolar recruitment have been advocated as the main physical mechanisms responsible for ventilator-induced lung injury. Limiting tidal volume has a demonstrated survival benefit in patients with acute respiratory distress syndrome and is recognized as the cornerstone of protective ventilation. In contrast, the use of high positive end-expiratory pressure levels in clinical trials has yielded conflicting results and remains controversial. In the present review, we will discuss the benefits and limitations of the open lung approach and will discuss some recent experimental and clinical trials on the use of high versus low/moderate positive end-expiratory pressure levels. We will also distinguish dynamic (tidal volume) from static strain (positive end-expiratory pressure and mean airway pressure) and will discuss their roles in inducing ventilator-induced lung injury. High positive end-expiratory pressure strategies clearly decrease refractory hypoxemia in patients with acute respiratory distress syndrome, but they also increase static strain, which in turn may harm patients, especially those with lower levels of lung recruitability. In patients with severe respiratory failure, titrating positive end-expiratory pressure against the severity of hypoxemia, or providing it in a decremental fashion after a recruitment maneuver, is recommended. If high plateau, driving or mean airway pressures are observed, prone positioning or ultraprotective ventilation may be indicated to improve oxygenation without additional stress and strain in the lung.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):231-237
DOI 10.5935/0103-507X.20170032
Overdistention and intratidal alveolar recruitment have been advocated as the main physical mechanisms responsible for ventilator-induced lung injury. Limiting tidal volume has a demonstrated survival benefit in patients with acute respiratory distress syndrome and is recognized as the cornerstone of protective ventilation. In contrast, the use of high positive end-expiratory pressure levels in clinical trials has yielded conflicting results and remains controversial. In the present review, we will discuss the benefits and limitations of the open lung approach and will discuss some recent experimental and clinical trials on the use of high versus low/moderate positive end-expiratory pressure levels. We will also distinguish dynamic (tidal volume) from static strain (positive end-expiratory pressure and mean airway pressure) and will discuss their roles in inducing ventilator-induced lung injury. High positive end-expiratory pressure strategies clearly decrease refractory hypoxemia in patients with acute respiratory distress syndrome, but they also increase static strain, which in turn may harm patients, especially those with lower levels of lung recruitability. In patients with severe respiratory failure, titrating positive end-expiratory pressure against the severity of hypoxemia, or providing it in a decremental fashion after a recruitment maneuver, is recommended. If high plateau, driving or mean airway pressures are observed, prone positioning or ultraprotective ventilation may be indicated to improve oxygenation without additional stress and strain in the lung.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):266-273
DOI 10.5935/0103-507X.20150035
Acute respiratory distress syndrome is a disease of acute onset characterized by hypoxemia and infiltrates on chest radiographs that affects both adults and children of all ages. It is an important cause of respiratory failure in pediatric intensive care units and is associated with significant morbidity and mortality. Nevertheless, until recently, the definitions and diagnostic criteria for acute respiratory distress syndrome have focused on the adult population. In this article, we review the evolution of the definition of acute respiratory distress syndrome over nearly five decades, with a special focus on the new pediatric definition. We also discuss recommendations for the implementation of mechanical ventilation strategies in the treatment of acute respiratory distress syndrome in children and the use of adjuvant therapies.
Abstract
Rev Bras Ter Intensiva. 2015;27(3):266-273
DOI 10.5935/0103-507X.20150035
Acute respiratory distress syndrome is a disease of acute onset characterized by hypoxemia and infiltrates on chest radiographs that affects both adults and children of all ages. It is an important cause of respiratory failure in pediatric intensive care units and is associated with significant morbidity and mortality. Nevertheless, until recently, the definitions and diagnostic criteria for acute respiratory distress syndrome have focused on the adult population. In this article, we review the evolution of the definition of acute respiratory distress syndrome over nearly five decades, with a special focus on the new pediatric definition. We also discuss recommendations for the implementation of mechanical ventilation strategies in the treatment of acute respiratory distress syndrome in children and the use of adjuvant therapies.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):134-140
DOI 10.5935/0103-507X.20150024
The development of the extracorporeal membrane oxygenation in Latin America represents a challenge in this specialty field. The objective of this article was to describe the results of a new extracorporeal membrane oxygenation program in an intensive care unit.
This retrospective cohort study included 22 patients who required extracorporeal membrane oxygenation and were treated from January 2011 to June 2014. The baseline characteristics, indications, duration of the condition, days on mechanical ventilation, days in the intensive care unit, complications, and hospital mortality were evaluated.
Fifteen patients required extracorporeal membrane oxygenation after lung transplantation, and seven patients required oxygenation due to acute respiratory distress. All transplanted patients were weaned from extracorporeal membrane oxygenation with a median duration of 3 days (Interquartile range - IQR: 2 - 5), were on mechanical ventilation for a median of 15.5 days (IQR: 3 - 25), and had an intensive care unit stay of 31.5 days (IQR: 19 - 53) and a median hospital stay of 60 days (IQR: 36 - 89) with 20% mortality. Patients with acute respiratory distress had a median oxygenation membrane duration of 9 days (IQR: 3 - 14), median mechanical ventilation time of 25 days (IQR: 13 - 37), a 31 day stay in therapy (IQR: 11 - 38), a 32 day stay in the hospital (IQR: 11 - 41), and 57% mortality. The main complications were infections (80%), acute kidney failure (43%), bleeding at the surgical site and at the site of cannula placement (22%), plateletopenia (60%), and coagulopathy (30%).
In spite of the steep learning curve, we considered this experience to be satisfactory, with results and complications comparable to those reported in the literature.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.
Abstract
Rev Bras Ter Intensiva. 2015;27(2):178-184
DOI 10.5935/0103-507X.20150030
To analyze the correlations of the blood flow/pump rotation ratio and the transmembrane pressure, CO2 and O2 transfer during the extracorporeal respiratory support.
Five animals were instrumented and submitted to extracorporeal membrane oxygenation in a five-step protocol, including abdominal sepsis and lung injury.
This study showed that blood flow/pump rotations ratio variations are dependent on extracorporeal membrane oxygenation blood flow in a positive logarithmic fashion. Blood flow/pump rotation ratio variations are negatively associated with transmembrane pressure (R2 = 0.5 for blood flow = 1500mL/minute and R2 = 0.4 for blood flow = 3500mL/minute, both with p < 0.001) and positively associated with CO2 transfer variations (R2 = 0.2 for sweep gas flow ≤ 6L/minute, p < 0.001, and R2 = 0.1 for sweep gas flow > 6L/minute, p = 0.006), and the blood flow/pump rotation ratio is not associated with O2 transfer variations (R2 = 0.01 for blood flow = 1500mL/minute, p = 0.19, and R2 = - 0.01 for blood flow = 3500 mL/minute, p = 0.46).
Blood flow/pump rotation ratio variation is negatively associated with transmembrane pressure and positively associated with CO2 transfer in this animal model. According to the clinical situation, a decrease in the blood flow/pump rotation ratio can indicate artificial lung dysfunction without the occurrence of hypoxemia.

Abstract
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
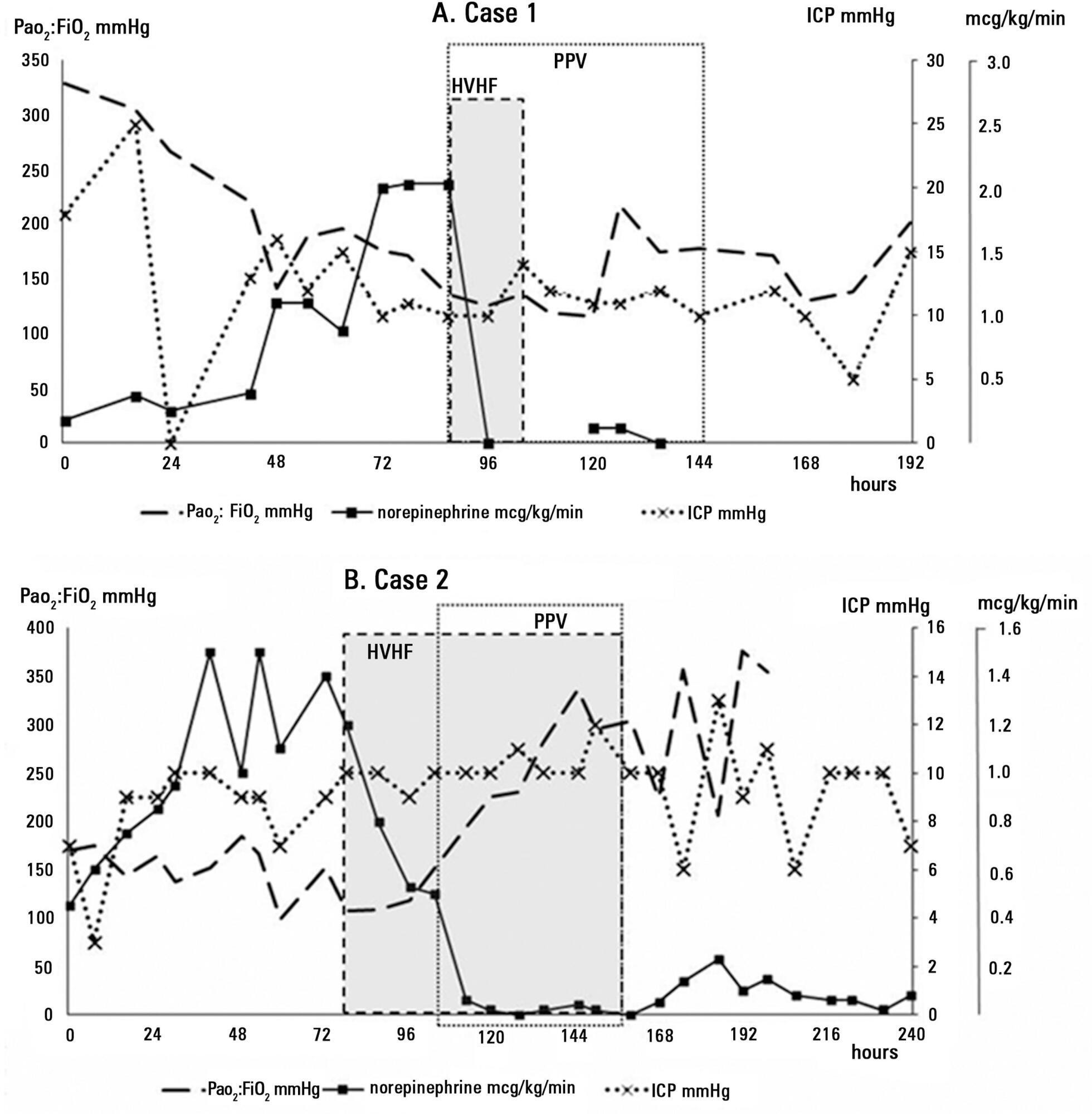
We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Abstract
Rev Bras Ter Intensiva. 2014;26(2):193-199
DOI 10.5935/0103-507X.20140028
We report the successful treatment of two patients with aneurismal subarachnoid hemorrhage complicated by severe respiratory failure and refractory septic shock using simultaneous prone position ventilation and high-volume hemofiltration. These rescue therapies allowed the patients to overcome the critical situation without associated complications and with no detrimental effects on the intracranial and cerebral perfusion pressures. Prone position ventilation is now an accepted therapy for severe acute respiratory distress syndrome, and high-volume hemofiltration is a non-conventional hemodynamic support that has several potential mechanisms for improving septic shock. In this manuscript, we briefly review these therapies and the related evidence. When other conventional treatments are insufficient for providing safe limits of oxygenation and perfusion as part of basic neuroprotective care in subarachnoid hemorrhage patients, these rescue therapies should be considered on a case-by-case basis by an experienced critical care team.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
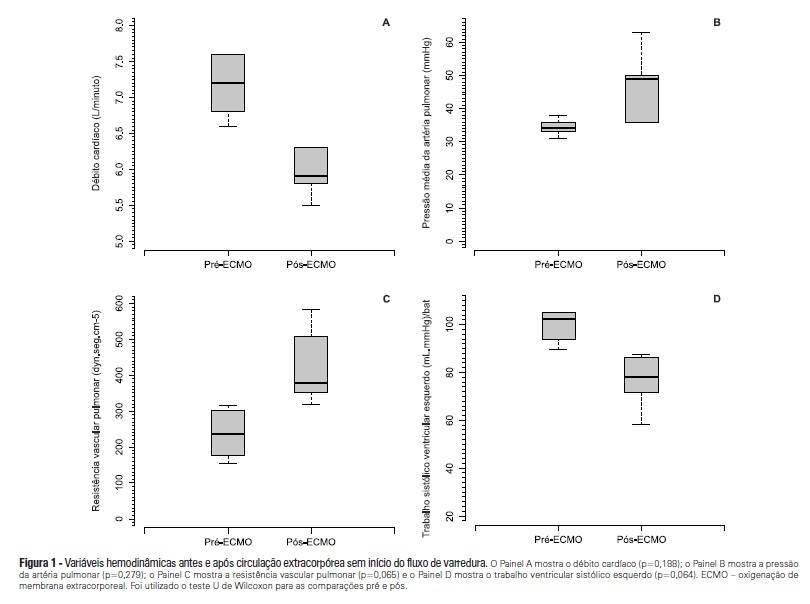
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.
Abstract
Rev Bras Ter Intensiva. 2012;24(2):137-142
DOI 10.1590/S0103-507X2012000200007
OBJECTIVE: To investigate the hemodynamic, respiratory and metabolic impact of blood contact with a priming volume and extracorporeal membrane oxygenation circuit, before the initiation of oxygenation and ventilation METHODS: Five animals were instrumented and submitted to extracorporeal membrane oxygenation. Data were collected at the baseline and 30 minutes after starting extracorporeal circulation, without membrane ventilatory (sweeper) flow. RESULTS: After starting extracorporeal membrane oxygenation, there was a non-significant elevation in pulmonary vascular resistance from 235 (178,303) to 379 (353,508) dyn.seg.(cm5)-1 (P=0.065), associated with an elevation in the alveolar arterial oxygen gradient from 235 (178,303) to 379 (353,508) mmHg (P=0.063). We also observed a reduction in the left ventricle stroke work from 102 (94,105) to 78 (71,87) (mL.mmHg)/beat (P=0.064), in addition to a reduction in cardiac output from 7.2 (6.8,7.6) to 5.9 (5.8,6.3) L/min (P=0.188). The right ventricle stroke work was counterbalanced between the pulmonary vascular resistance increment and the cardiac output reduction, maintaining a similar value. CONCLUSIONS: We presented an experimental model that is feasible and safe. Blood contact with the priming volume and extracorporeal membrane oxygenation circuit resulted in non-significant systemic or metabolic changes.