acute respiratory distress syndrome Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2009;21(4):404-415
DOI 10.1590/S0103-507X2009000400011
Acute respiratory distress syndrome is characterized by a diffuse inflammatory reaction of lung parenchyma induced by a direct insult to the alveolar epithelium (pulmonary acute respiratory distress syndrome) or an indirect lesion through the vascular endothelium (extrapulmonary acute respiratory distress syndrome). The main therapeutic strategy for acute respiratory distress syndrome is the ventilatory support. However, mechanical ventilation can worsen lung injury. In this context, a protective ventilatory strategy with low tidal volume has been proposed. The use of low tidal volume reduced the mortality rate of acute respiratory distress syndrome patients, but result in hypercapnic acidosis. The current article presents a review of literature on the effects of permissive hypercapnia in acute respiratory distress syndrome. To that end, we carried out a systematic review of scientific literature based on established criteria for documental analysis including clinical and experimental articles, using as data bases MedLine, LILACS, SciELO, PubMed, Cochrane. Hypercapnic acidosis has been considered by some authors as a modulator of the inflammatory process of acute respiratory distress syndrome. However, clinical and experimental studies on the effects of hypercapnic acidosis have shown controversial results. Therefore it is important to better elucidate the role of hypercapnic acidosis in acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2009;21(4):404-415
DOI 10.1590/S0103-507X2009000400011
Acute respiratory distress syndrome is characterized by a diffuse inflammatory reaction of lung parenchyma induced by a direct insult to the alveolar epithelium (pulmonary acute respiratory distress syndrome) or an indirect lesion through the vascular endothelium (extrapulmonary acute respiratory distress syndrome). The main therapeutic strategy for acute respiratory distress syndrome is the ventilatory support. However, mechanical ventilation can worsen lung injury. In this context, a protective ventilatory strategy with low tidal volume has been proposed. The use of low tidal volume reduced the mortality rate of acute respiratory distress syndrome patients, but result in hypercapnic acidosis. The current article presents a review of literature on the effects of permissive hypercapnia in acute respiratory distress syndrome. To that end, we carried out a systematic review of scientific literature based on established criteria for documental analysis including clinical and experimental articles, using as data bases MedLine, LILACS, SciELO, PubMed, Cochrane. Hypercapnic acidosis has been considered by some authors as a modulator of the inflammatory process of acute respiratory distress syndrome. However, clinical and experimental studies on the effects of hypercapnic acidosis have shown controversial results. Therefore it is important to better elucidate the role of hypercapnic acidosis in acute respiratory distress syndrome.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):174-182
DOI 10.1590/S0103-507X2009000200010
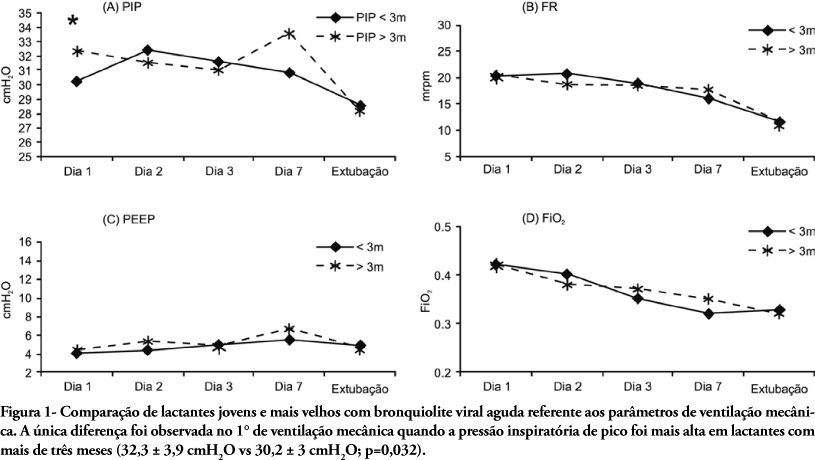
OBJECTIVE: To describe the characteristics and the outcome of infants with acute viral bronchiolitis submitted to mechanical ventilation. METHODS: We performed a retrospective study enrolling all infants (less than 12 months old) admitted with the diagnosis of acute viral bronchiolitis and submitted to mechanical ventilation in an university affiliated Brazilian pediatric intensive care unit between March, 2004 and September, 2006 (3 consecutives winters). The mechanical ventilation parameters' employed on 1st, 2nd, 3rd, 7th day and before extubation were evaluated as well as the evolution (mortality rate, presence of acute respiratory distress syndrome and the prevalence of complications). The groups were compared using the Student t test, the Mann-Whitney U test and the Chi-square test. RESULTS: Fifty-nine infants were included (3.8 ± 2.7 months old, 59% male), with 9.0 ± 9.4 days on mechanical ventilation. Prior mechanical ventilation, non invasive ventilation was instituted in 71% of children. Anemia was observed in 78% of the sample. In 51 infants (86.5%) the lower airway obstructive pattern was maintained up to tracheal extubation with a nil mortality and low prevalence of pneumothorax (7.8%). Acute respiratory distress syndrome occurred in 8 infants (13.5%), with higher mortality and a higher prevalence of pneumothorax (62.5%). CONCLUSIONS: The declining mortality in acute viral bronchiolitis is observed even in non developed regions, involving children with high rates of anemia and premature labor. The low mortality is associated with the maintenance of the lower airway obstructive pattern during the period on mechanical ventilation. The development of acute respiratory distress syndrome is associated with increased mortality and higher prevalence of complications, representing the actual challenge in the management of children with severe acute viral bronchiolitis.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):174-182
DOI 10.1590/S0103-507X2009000200010
OBJECTIVE: To describe the characteristics and the outcome of infants with acute viral bronchiolitis submitted to mechanical ventilation. METHODS: We performed a retrospective study enrolling all infants (less than 12 months old) admitted with the diagnosis of acute viral bronchiolitis and submitted to mechanical ventilation in an university affiliated Brazilian pediatric intensive care unit between March, 2004 and September, 2006 (3 consecutives winters). The mechanical ventilation parameters' employed on 1st, 2nd, 3rd, 7th day and before extubation were evaluated as well as the evolution (mortality rate, presence of acute respiratory distress syndrome and the prevalence of complications). The groups were compared using the Student t test, the Mann-Whitney U test and the Chi-square test. RESULTS: Fifty-nine infants were included (3.8 ± 2.7 months old, 59% male), with 9.0 ± 9.4 days on mechanical ventilation. Prior mechanical ventilation, non invasive ventilation was instituted in 71% of children. Anemia was observed in 78% of the sample. In 51 infants (86.5%) the lower airway obstructive pattern was maintained up to tracheal extubation with a nil mortality and low prevalence of pneumothorax (7.8%). Acute respiratory distress syndrome occurred in 8 infants (13.5%), with higher mortality and a higher prevalence of pneumothorax (62.5%). CONCLUSIONS: The declining mortality in acute viral bronchiolitis is observed even in non developed regions, involving children with high rates of anemia and premature labor. The low mortality is associated with the maintenance of the lower airway obstructive pattern during the period on mechanical ventilation. The development of acute respiratory distress syndrome is associated with increased mortality and higher prevalence of complications, representing the actual challenge in the management of children with severe acute viral bronchiolitis.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2009;21(1):96-103
DOI 10.1590/S0103-507X2009000100014
This article intends to review literature on high frequency oscillatory ventilation and describe its main clinical applications for children and neonates. Articles from the last 15 years were selected using MedLine and SciElo databases. The following key words were used: high frequency oscillatory ventilation, mechanical ventilation, acute respiratory distress syndrome, children, and new-born. The review describes high frequency oscillatory ventilation in children with acute respiratory distress syndrome, air leak syndrome, and obstructive lung disease. Respiratory distress syndrome, bronchopulmonary dysplasia, intracranial hemorrhage, periventricular leukomalacia, and air leak syndrome were reviewed in neonates. Transition from conventional mechanical ventilation to high frequency ventilation and its adjustments relating to oxygenation, CO2 elimination, chest radiography, suctioning, sedatives and use of neuromuscular blocking agents were described. Weaning and complications were also reported. For children, high frequency oscillatory ventilation is a therapeutic option, particularly in acute respiratory distress syndrome, and should be used as early as possible. It may be also useful in the air leak syndrome and obstructive pulmonary disease. Evidence that, in neonates, high frequency oscillatory ventilation is superior to conventional mechanical ventilation is lacking. However there is evidence that better results are only achieved with this ventilatory mode to manage the air leak syndrome.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):407-411
DOI 10.1590/S0103-507X2006000400015
BACKGROUND AND OBJECTIVE: The objective of this study was to review the literature on inhaled nitric oxide to children with acute respiratory distress syndrome. CONTENTS: A review of literature and selection of the most important publications on inhaled nitric oxide, using the MedLine and Cochrane Systematic Review Databases. This review was organized as follows: introduction; metabolism and biological effects; clinical applications; dosage, gas administration and weaning process; warnings and side-effects. Inhaled nitric oxide use was described in acute respiratory distress syndrome. CONCLUSIONS: Inhaled nitric oxide as the first vasodilator to produce selective pulmonary vasodilation has beneficial effects on gas exchange and ventilation, improving outcome in children with severe hypoxia. It is safe when administered in intensive care units under strict surveillance and monitoring. Further studies should be concentrated on early treatment, when acute respiratory distress syndrome is potentially reversible.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):407-411
DOI 10.1590/S0103-507X2006000400015
BACKGROUND AND OBJECTIVE: The objective of this study was to review the literature on inhaled nitric oxide to children with acute respiratory distress syndrome. CONTENTS: A review of literature and selection of the most important publications on inhaled nitric oxide, using the MedLine and Cochrane Systematic Review Databases. This review was organized as follows: introduction; metabolism and biological effects; clinical applications; dosage, gas administration and weaning process; warnings and side-effects. Inhaled nitric oxide use was described in acute respiratory distress syndrome. CONCLUSIONS: Inhaled nitric oxide as the first vasodilator to produce selective pulmonary vasodilation has beneficial effects on gas exchange and ventilation, improving outcome in children with severe hypoxia. It is safe when administered in intensive care units under strict surveillance and monitoring. Further studies should be concentrated on early treatment, when acute respiratory distress syndrome is potentially reversible.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):44-52
DOI 10.1590/S0103-507X2007000100006
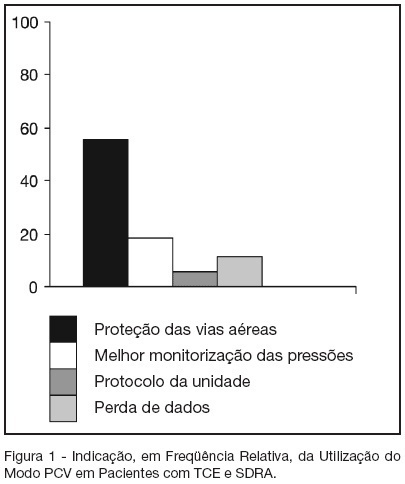
BACKGROUND AND OBJECTIVES: The traumatic brain injury (TBI) is a healthy-world problem, some of his patients develop respiratory failure, requiring intubation and mechanical ventilation, and the most common complications are the acute respiratory distress syndrome (ARDS). In this way, this study has the objective describe the daily clinical practice of respiratory care in this patients submit mechanical ventilation. METHODS: The methods and ventilatories parameters used to ventilate the patients with TBI and ARDS has been evaluated by a sample of physiotherapists from the city of Salvador, BA, from a descriptive study. The data were collected by face-to-face interviews in the period of October 2005 to March 2006. For in such way a half structuralized questionnaire was elaborated contends changeable social-demographic, about the hospital profile and the applied ventilatory strategy in patients with TBI that come to develop ARDS. RESULTS: The sample was composed by 70 physiotherapists, 41 (58.6%) was female, with mean of age of 31.2 ± 6.4 (24-49) years-old and graduated time 7.7 ± 6.4 (1-27) years, which 37 (52.9%) works on public hospital; 67 (95.7%) has any specialization. Sixty four physiotherapists affirm the usage of the pressure controlled ventilation mode. The peak pressure and the plateau pressure wanted to ventilate the patients with TBI and ARDS were in mean 35.6 ± 5,3 (25-50) and 28,4 ± 5,8 (15-35) cmH2O respectively. Forty eighty (68.6%) of the interviewed wants a PaCO2 in 30-35 mmHg. Thirty one (44.3%) of the interviewed finds the ideal PEEP through the best SpO2 with minor FiO2. CONCLUSIONS: It's incontestable that the ventilatory strategy of a patient with severe TBI that become to develop ALI or ARDS is an authentic challenge; a predilection for PCV mode is observed due to the already known protective ventilation strategy.
Abstract
Rev Bras Ter Intensiva. 2007;19(1):44-52
DOI 10.1590/S0103-507X2007000100006
BACKGROUND AND OBJECTIVES: The traumatic brain injury (TBI) is a healthy-world problem, some of his patients develop respiratory failure, requiring intubation and mechanical ventilation, and the most common complications are the acute respiratory distress syndrome (ARDS). In this way, this study has the objective describe the daily clinical practice of respiratory care in this patients submit mechanical ventilation. METHODS: The methods and ventilatories parameters used to ventilate the patients with TBI and ARDS has been evaluated by a sample of physiotherapists from the city of Salvador, BA, from a descriptive study. The data were collected by face-to-face interviews in the period of October 2005 to March 2006. For in such way a half structuralized questionnaire was elaborated contends changeable social-demographic, about the hospital profile and the applied ventilatory strategy in patients with TBI that come to develop ARDS. RESULTS: The sample was composed by 70 physiotherapists, 41 (58.6%) was female, with mean of age of 31.2 ± 6.4 (24-49) years-old and graduated time 7.7 ± 6.4 (1-27) years, which 37 (52.9%) works on public hospital; 67 (95.7%) has any specialization. Sixty four physiotherapists affirm the usage of the pressure controlled ventilation mode. The peak pressure and the plateau pressure wanted to ventilate the patients with TBI and ARDS were in mean 35.6 ± 5,3 (25-50) and 28,4 ± 5,8 (15-35) cmH2O respectively. Forty eighty (68.6%) of the interviewed wants a PaCO2 in 30-35 mmHg. Thirty one (44.3%) of the interviewed finds the ideal PEEP through the best SpO2 with minor FiO2. CONCLUSIONS: It's incontestable that the ventilatory strategy of a patient with severe TBI that become to develop ALI or ARDS is an authentic challenge; a predilection for PCV mode is observed due to the already known protective ventilation strategy.