Você pesquisou por y - Critical Care Science (CCS)

You searched for:"Thiago Domingos Corrêa"
We found (12) results for your search.Abstract
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 - 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 - 3) versus 5 (2 - 24) hours; p < 0.001].
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Abstract
Rev Bras Ter Intensiva. 2022;34(1):107-115
DOI 10.5935/0103-507X.20220005-en
To evaluate clinical practices and hospital resource organization during the early COVID-19 pandemic in Brazil.
This was a multicenter, cross-sectional survey. An electronic questionnaire was provided to emergency department and intensive care unit physicians attending COVID-19 patients. The survey comprised four domains: characteristics of the participants, clinical practices, COVID-19 treatment protocols and hospital resource organization.
Between May and June 2020, 284 participants [median (interquartile ranges) age 39 (33 - 47) years, 56.3% men] responded to the survey; 33% were intensivists, and 9% were emergency medicine specialists. Half of the respondents worked in public hospitals. Noninvasive ventilation (89% versus 73%; p = 0.001) and highflow nasal cannula (49% versus 32%; p = 0.005) were reported to be more commonly available in private hospitals than in public hospitals. Mechanical ventilation was more commonly used in public hospitals than private hospitals (70% versus 50%; p = 0,024). In the Emergency Departments, positive endexpiratory pressure was most commonly adjusted according to SpO2, while in the intensive care units, positive end-expiratory pressure was adjusted according to the best lung compliance. In the Emergency Departments, 25% of the respondents did not know how to set positive end-expiratory pressure. Compared to private hospitals, public hospitals had a lower availability of protocols for personal protection equipment during tracheal intubation (82% versus 94%; p = 0.005), managing mechanical ventilation [64% versus 75%; p = 0.006] and weaning patients from mechanical ventilation [34% versus 54%; p = 0.002]. Finally, patients spent less time in the emergency department before being transferred to the intensive care unit in private hospitals than in public hospitals [2 (1 - 3) versus 5 (2 - 24) hours; p < 0.001].
This survey revealed significant heterogeneity in the organization of hospital resources, clinical practices and treatments among physicians during the early COVID-19 pandemic in Brazil.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
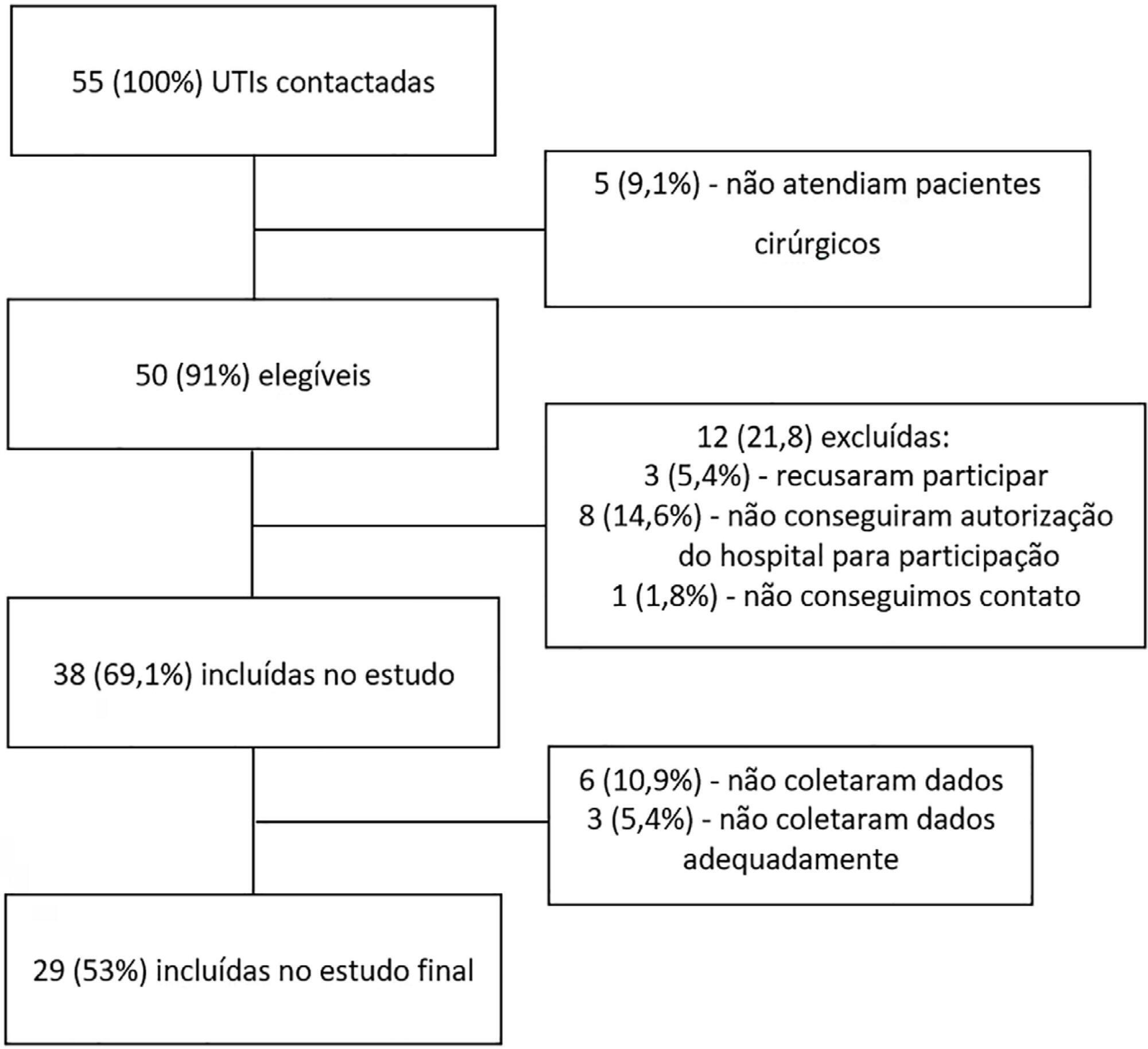
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
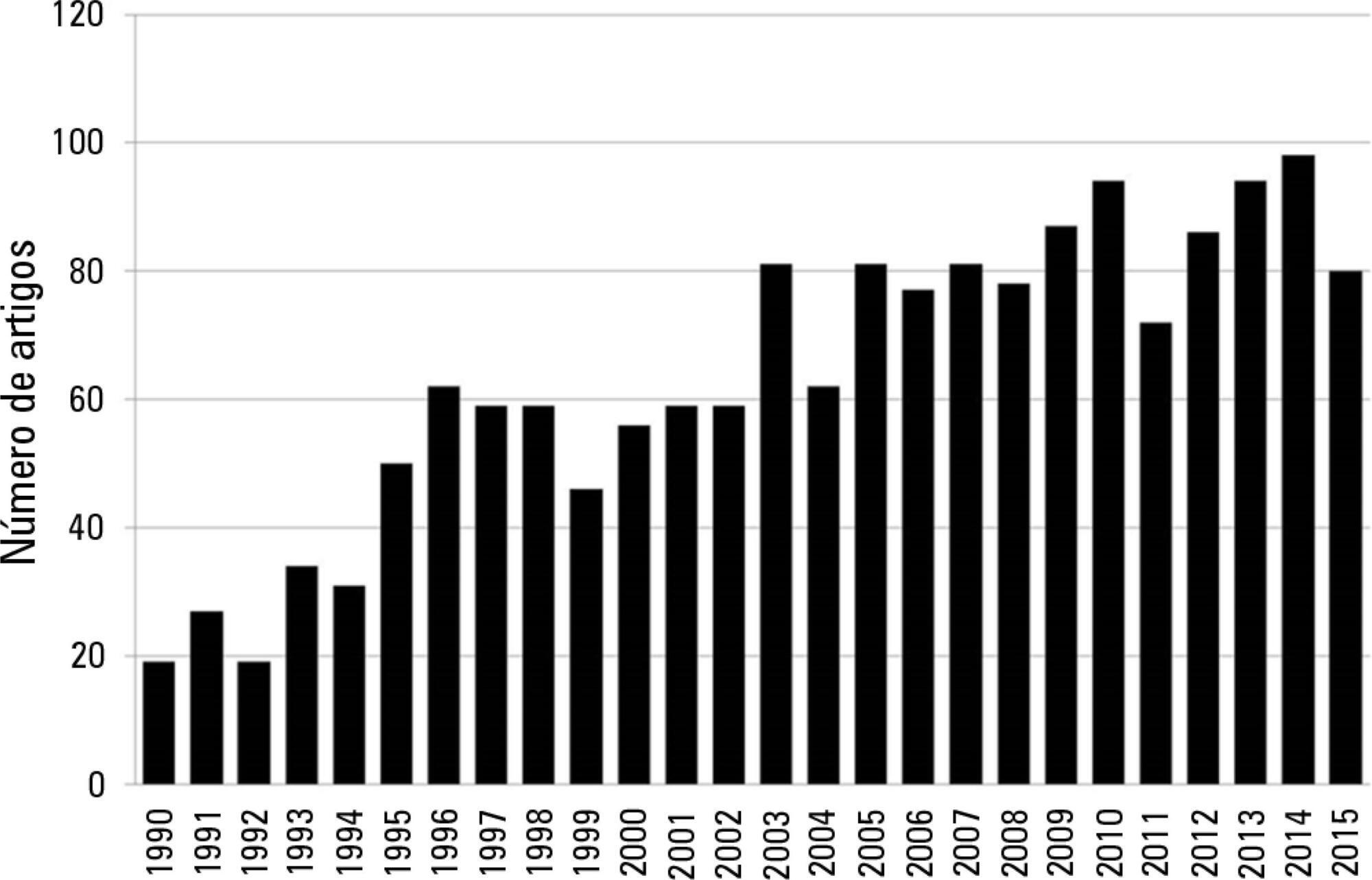
BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Abstract
Rev Bras Ter Intensiva. 2008;20(2):197-204
DOI 10.1590/S0103-507X2008000200014
BACKGROUND AND OBJECTIVES: Acute coronary syndromes result from a disruption of a vulnerable coronary plaque complicated by intraluminal thrombus formation, embolisation, and variable degrees of coronary obstruction. Patients with total occlusion may present with acute ST Elevation Myocardial Infarction (STEMI). Partial vessel obstruction may result in Non-ST-Elevation Acute Myocardial Infarction (NSTEMI) or unstable angina (UA). Clinical symptoms and electrocardiographic changes are the main components of identification of ACS. The rapid and effective triage of such patients regarding presence or absence of ST-segment elevation is critical to dictate further therapeutic strategies. The objective of this chapter was to review current evidence and recommendations for the evaluation and early treatment of acute coronary syndromes. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1990 to September 2007. CONCLUSIONS: Reperfusion of the infarct-related artery is the cornerstone of therapy for STEMI. Fibrinolysis and percutaneous coronary intervention are both well established as effective options. Management of UA/NSTEMI patients requires early risk stratification. High-risk patients should undergo an early invasive strategy that consists in performance of cardiac catheterization in the first 24 to 48 hours of presentation.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):216-220
DOI 10.1590/S0103-507X2007000200013
BACKGROUND AND OBJECTIVES: Myocardial contusion is often associated with blunt chest trauma. Its diagnosis is challenging to the professionals who work in emergency department due to nonspecific symptoms and the lack of auxiliary exams with enough accuracy to diagnose. Among the available diagnostic tools, the biomarkers of myocardial injury troponin I and troponin T have stood out. Troponins are proteins of the citocellular apparatus, released into the bloodstream only after the disruption of myocytes cellular membrane. Therefore they are highly specific to detect myocardial injuries. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1980 to November 2006 about the importance of a serial measurement of troponin I and T as a diagnostic tool as well as predictor of unfavorable clinical outcome in patients with myocardial contusion after a blunt chest trauma. CONCLUSIONS: Although troponins I and T are more specific than usual biomarkers CKMB and CK, these two first biomarkers show a low sensitivity and positive predictive value to diagnosis myocardial contusion. Patients with ECG abnormalities, troponins elevations or both should remain in an intensive care unit (ICU) for at least 24 hours, period in which they cam develop most of the complications related to myocardial contusion.
Abstract
Rev Bras Ter Intensiva. 2007;19(2):216-220
DOI 10.1590/S0103-507X2007000200013
BACKGROUND AND OBJECTIVES: Myocardial contusion is often associated with blunt chest trauma. Its diagnosis is challenging to the professionals who work in emergency department due to nonspecific symptoms and the lack of auxiliary exams with enough accuracy to diagnose. Among the available diagnostic tools, the biomarkers of myocardial injury troponin I and troponin T have stood out. Troponins are proteins of the citocellular apparatus, released into the bloodstream only after the disruption of myocytes cellular membrane. Therefore they are highly specific to detect myocardial injuries. CONTENTS: We performed a clinical review using the electronic databases MedLine and LILACS from January 1980 to November 2006 about the importance of a serial measurement of troponin I and T as a diagnostic tool as well as predictor of unfavorable clinical outcome in patients with myocardial contusion after a blunt chest trauma. CONCLUSIONS: Although troponins I and T are more specific than usual biomarkers CKMB and CK, these two first biomarkers show a low sensitivity and positive predictive value to diagnosis myocardial contusion. Patients with ECG abnormalities, troponins elevations or both should remain in an intensive care unit (ICU) for at least 24 hours, period in which they cam develop most of the complications related to myocardial contusion.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):238-247
DOI 10.5935/0103-507X.20170033
Parameters related to macrocirculation, such as the mean arterial pressure, central venous pressure, cardiac output, mixed venous saturation and central oxygen saturation, are commonly used in the hemodynamic assessment of critically ill patients. However, several studies have shown that there is a dissociation between these parameters and the state of microcirculation in this group of patients. Techniques that allow direct viewing of the microcirculation are not completely disseminated, nor are they incorporated into the clinical management of patients in shock. The numerous techniques developed for microcirculation assessment include clinical assessment (e.g., peripheral perfusion index and temperature gradient), laser Doppler flowmetry, tissue oxygen assessment electrodes, videomicroscopy (orthogonal polarization spectral imaging, sidestream dark field imaging or incident dark field illumination) and near infrared spectroscopy. In the near future, the monitoring and optimization of tissue perfusion by direct viewing and microcirculation assessment may become a goal to be achieved in the hemodynamic resuscitation of critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2017;29(2):238-247
DOI 10.5935/0103-507X.20170033
Parameters related to macrocirculation, such as the mean arterial pressure, central venous pressure, cardiac output, mixed venous saturation and central oxygen saturation, are commonly used in the hemodynamic assessment of critically ill patients. However, several studies have shown that there is a dissociation between these parameters and the state of microcirculation in this group of patients. Techniques that allow direct viewing of the microcirculation are not completely disseminated, nor are they incorporated into the clinical management of patients in shock. The numerous techniques developed for microcirculation assessment include clinical assessment (e.g., peripheral perfusion index and temperature gradient), laser Doppler flowmetry, tissue oxygen assessment electrodes, videomicroscopy (orthogonal polarization spectral imaging, sidestream dark field imaging or incident dark field illumination) and near infrared spectroscopy. In the near future, the monitoring and optimization of tissue perfusion by direct viewing and microcirculation assessment may become a goal to be achieved in the hemodynamic resuscitation of critically ill patients.
Abstract
Crit Care Sci. 2023;35(3):256-265
DOI 10.5935/2965-2774.20230129-pt
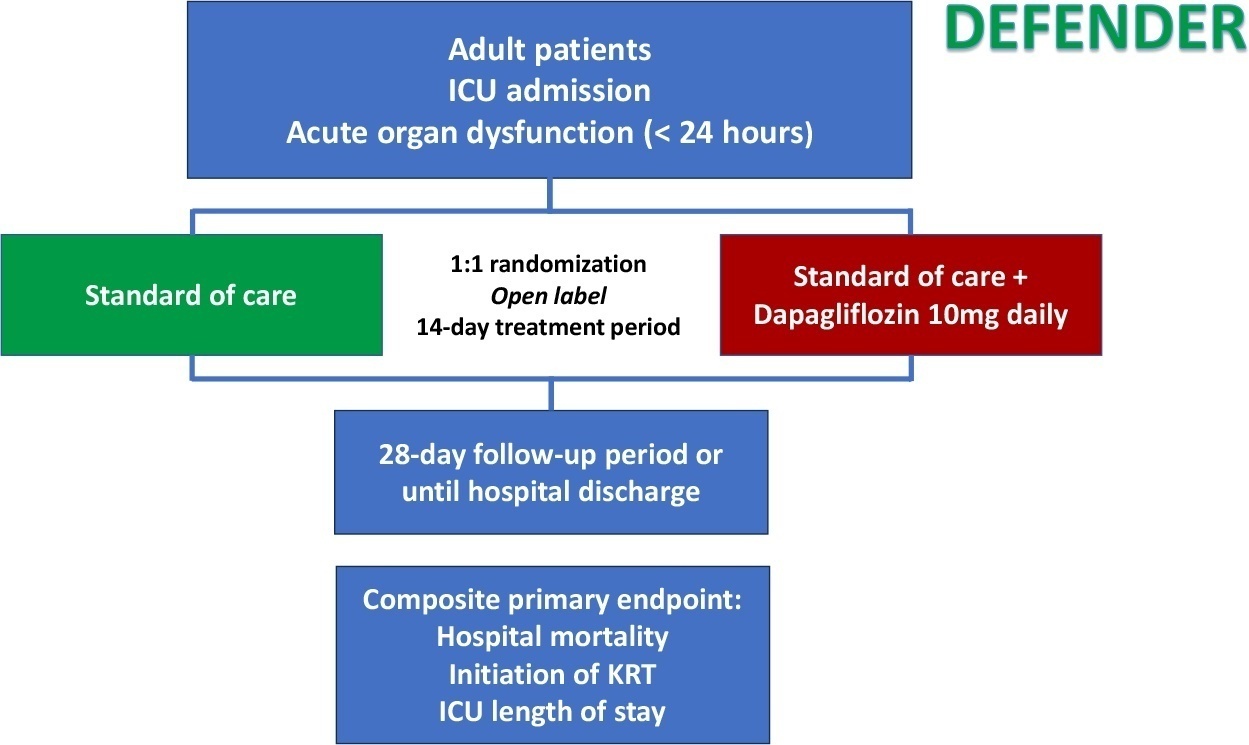
Critical illness is a major ongoing health care burden worldwide and is associated with high mortality rates. Sodium-glucose cotransporter-2 inhibitors have consistently shown benefits in cardiovascular and renal outcomes. The effects of sodium-glucose cotransporter-2 inhibitors in acute illness have not been properly investigated.
DEFENDER is an investigator-initiated, multicenter, randomized, open-label trial designed to evaluate the efficacy and safety of dapagliflozin in 500 adult participants with acute organ dysfunction who are hospitalized in the intensive care unit. Eligible participants will be randomized 1:1 to receive dapagliflozin 10mg plus standard of care for up to 14 days or standard of care alone. The primary outcome is a hierarchical composite of hospital mortality, initiation of kidney replacement therapy, and intensive care unit length of stay, up to 28 days. Safety will be strictly monitored throughout the study.
DEFENDER is the first study designed to investigate the use of a sodium-glucose cotransporter-2 inhibitor in general intensive care unit patients with acute organ dysfunction. It will provide relevant information on the use of drugs of this promising class in critically ill patients.
NCT05558098
Abstract
Crit Care Sci. 2023;35(3):256-265
DOI 10.5935/2965-2774.20230129-pt
Critical illness is a major ongoing health care burden worldwide and is associated with high mortality rates. Sodium-glucose cotransporter-2 inhibitors have consistently shown benefits in cardiovascular and renal outcomes. The effects of sodium-glucose cotransporter-2 inhibitors in acute illness have not been properly investigated.
DEFENDER is an investigator-initiated, multicenter, randomized, open-label trial designed to evaluate the efficacy and safety of dapagliflozin in 500 adult participants with acute organ dysfunction who are hospitalized in the intensive care unit. Eligible participants will be randomized 1:1 to receive dapagliflozin 10mg plus standard of care for up to 14 days or standard of care alone. The primary outcome is a hierarchical composite of hospital mortality, initiation of kidney replacement therapy, and intensive care unit length of stay, up to 28 days. Safety will be strictly monitored throughout the study.
DEFENDER is the first study designed to investigate the use of a sodium-glucose cotransporter-2 inhibitor in general intensive care unit patients with acute organ dysfunction. It will provide relevant information on the use of drugs of this promising class in critically ill patients.
NCT05558098
Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2022;34(2):287-294
DOI 10.5935/0103-507X.20220027-en
Ketamine is unique among anesthetics and analgesics. The drug is a rapid-acting general anesthetic that produces an anesthetic state characterized by profound analgesia, preserved pharyngeal-laryngeal reflexes, normal or slightly enhanced skeletal muscle tone, cardiovascular and respiratory stimulation, and occasionally a transient and minimal respiratory depression. Research has demonstrated the efficacy of its use on anesthesia, pain, palliative care, and intensive care. Recently, it has been used for postoperative and chronic pain, as an adjunct in psychotherapy, as a treatment for depression and posttraumatic stress disorder, as a procedural sedative, and as a treatment for respiratory and/or neurologic clinical conditions. Despite being a safe and widely used drug, many physicians, such as intensivists and those practicing in emergency care, are not aware of the current clinical applications of ketamine. The objective of this narrative literature review is to present the theoretical and practical aspects of clinical applications of ketamine in intensive care unit and emergency department settings.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
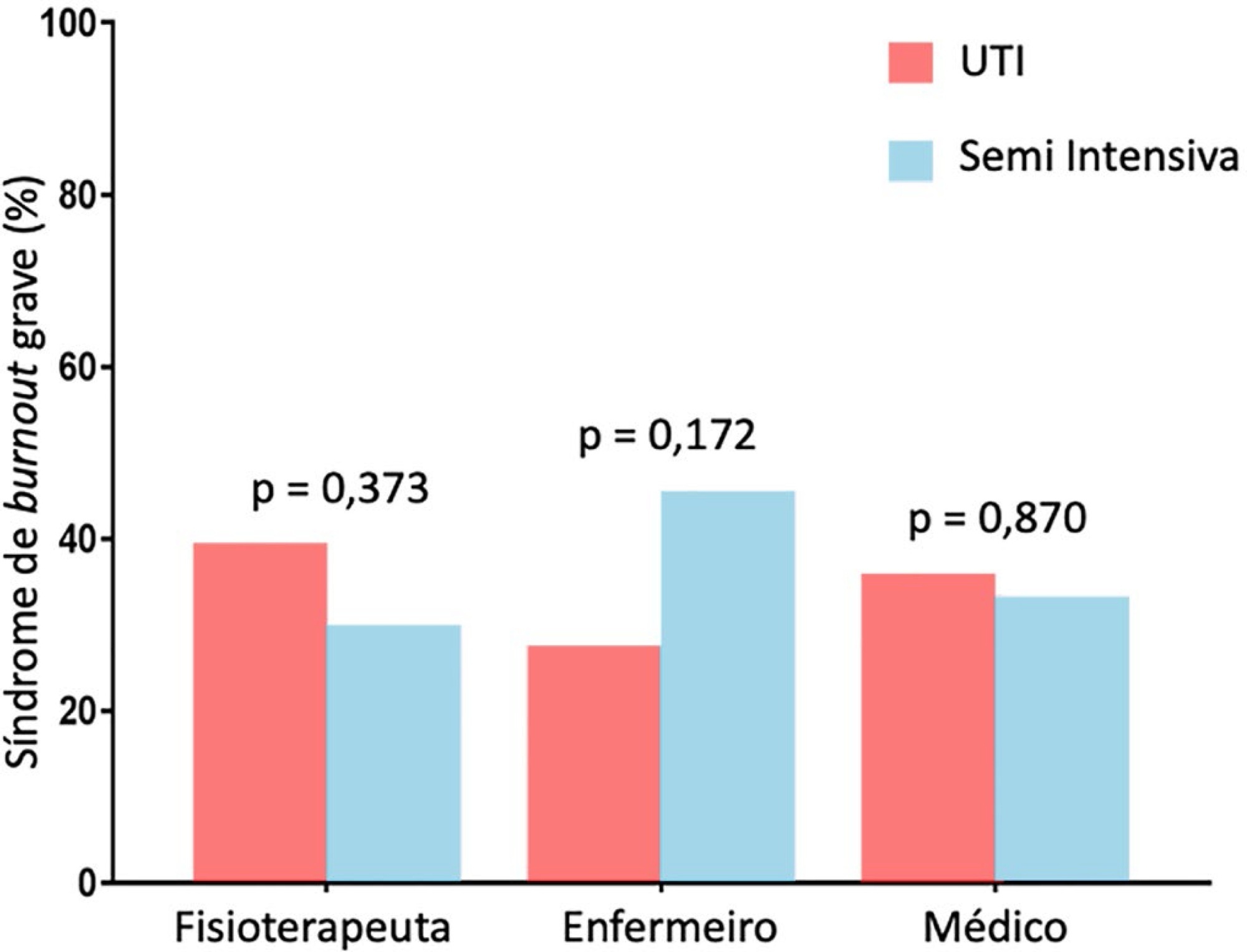
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 - 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 - 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.
Abstract
Rev Bras Ter Intensiva. 2020;32(3):381-390
DOI 10.5935/0103-507X.20200066
To evaluate the frequency of severe burnout syndrome among critical care providers and to correlate it with work engagement.
A self-administered survey including the Maslach Burnout Inventory, Depression Anxiety and Stress Scales, and Gallup questionnaire was distributed. All analyses were stratified by setting (intensive care unit or step-down unit) and by professional group (nurses versus physicians versus physiotherapists).
Between February 2017 and June 2017, 206 out of 325 invited professionals (63.4%) answered the questionnaires. Of these, 55 were physicians (26.7%), 88 were physiotherapists (42.7%) and 63 were nurses (30.6%). The frequency of severe burnout was 34.3% (27.9 - 41.4%), and no difference was found between professional groups or settings. The frequency of severe or very severe cases of depression, anxiety or stress was 12.9%, 11.4% and 10.5%, respectively. The median (interquartile range) score observed on the Gallup questionnaire was 41 (34 - 48), and no differences were found between professional groups or settings. There was a negative correlation between burnout and work engagement (r = -0.148; p = 0.035).
There is a high frequency of severe burnout among critical care providers working in the intensive care unit and step-down unit. There was a negative correlation between burnout and work engagement.