-
Intensive care admission policies for critically ill cancer patients: time for a reappraisal
Rev Bras Ter Intensiva. 2006;18(3):217-218
-
Mechanical ventilation in Brazil: epidemiological aspects
Rev Bras Ter Intensiva. 2006;18(3):219-228
Abstract
Mechanical ventilation in Brazil: epidemiological aspects
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
Views1BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation’s causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Keywords:artificial respirationintensive care unit (ICU)mechanical ventilationrespiratory failureventilators modesSee moreViews1

Abstract
Mechanical ventilation in Brazil: epidemiological aspects
Rev Bras Ter Intensiva. 2006;18(3):219-228
DOI 10.1590/S0103-507X2006000300002
Views1BACKGROUND AND OBJECTIVES: There are few epidemiological studies in mechanical ventilation, and the aim of the study is to show how this procedure is being used in Brazil. METHODS: A 1-day point prevalence study was performed in 40 ICUs, with 390 patients; 217 of these patients were in mechanical ventilation. The results evaluated were the characteristics of ventilated patients, their distribution in Brazil, the mechanical ventilation’s causes, the main ventilatory modes, the more important ventilators settings, and the weaning stage of mechanical ventilation. RESULTS: The median age of the ventilated patients was 66 years old. The median APACHE II was 20, while the median time of mechanical ventilation was 11 days. Acute respiratory failure occurred in 71% of the patients, coma in 21.2%, acute exacerbation of chronic respiratory failure in 5.5%, and the neuromuscular disease in 2.3%. The volume-controlled ventilation (VCV) (30%), the pressure support ventilation (PSV) (29.5%), and the pressure-controlled ventilation (PCV) (18%) were the ventilatory modes most used; the PSV had been the main mode in weaning (63.5%). The median of tidal volume (8 mL/kg) was higher in VCV. The median of maximal inspiratory pression (30 cmH2O) and the median of positive end-expiration pressure (PEEP) (8 cmH2O) were higher in PCV. CONCLUSIONS: The predominance of ventilated patients in ICUs was marked by clinical severity of them, and a longer hospital stay time; acute respiratory failure was the principal mechanical ventilation cause; VCV and PSV ventilated more patients, with PSV being more used in weaning patients.
Keywords:artificial respirationintensive care unit (ICU)mechanical ventilationrespiratory failureventilators modesSee more -
Stress ulcer prophylaxis in intensive care units: an observational multicenter study
Rev Bras Ter Intensiva. 2006;18(3):229-233
Abstract
Stress ulcer prophylaxis in intensive care units: an observational multicenter study
Rev Bras Ter Intensiva. 2006;18(3):229-233
DOI 10.1590/S0103-507X2006000300003
Views0See moreBACKGROUND AND OBJECTIVES: Gastrointestinal bleeding due to stress ulcer (GB) complicates critical disease, and must be received prophylaxis based on defined criteria. To evaluate the GB prophylaxis in Intensive Care Units (ICU), and to compare with the guidelines. METHODS: We carried out a cross-sectional multicenter study in 21 medical-surgical ICU in Brazil to investigate this issue. For data analysis, these were distributed in 3 sub-groups (high, moderate and low risk for GB). RESULTS: 235 patients were evaluated, with mean age of 57.7 ± 19.5 years and days on ICU 13 ± 19.7. The more common admission ICU diagnoses were sepsis (26%) and postoperative (16.2%) patients. Seventy-three (73%) of the patients were GB high risk, 21.5% moderate and 5.5% low risk. Of the 187 high risk patients, 139 were receiving GB prophylaxis (60% with histamine blockers (HB2) and 39% with proton pump inhibitors (PPI). Of these patients, 25.7% did not receive GU prophylaxis, although indicated it. Of the 55 moderate risk patients, 70.9% wer e receiving GU prophylaxis (22 with HB2 and 17 with PPI). Of the 14 low risk patients, 71% were using GU prophylaxis (6 with HB2 and 4 with PPI). CONCLUSIONS: Almost 80% of the patients made use of GB prophylactic drugs, with no agreement GU risk stratification. This study demonstrated the no adequate GU prophylaxis in the Brazilian ICU.
Views0Abstract
Stress ulcer prophylaxis in intensive care units: an observational multicenter study
Rev Bras Ter Intensiva. 2006;18(3):229-233
DOI 10.1590/S0103-507X2006000300003
Views0See moreBACKGROUND AND OBJECTIVES: Gastrointestinal bleeding due to stress ulcer (GB) complicates critical disease, and must be received prophylaxis based on defined criteria. To evaluate the GB prophylaxis in Intensive Care Units (ICU), and to compare with the guidelines. METHODS: We carried out a cross-sectional multicenter study in 21 medical-surgical ICU in Brazil to investigate this issue. For data analysis, these were distributed in 3 sub-groups (high, moderate and low risk for GB). RESULTS: 235 patients were evaluated, with mean age of 57.7 ± 19.5 years and days on ICU 13 ± 19.7. The more common admission ICU diagnoses were sepsis (26%) and postoperative (16.2%) patients. Seventy-three (73%) of the patients were GB high risk, 21.5% moderate and 5.5% low risk. Of the 187 high risk patients, 139 were receiving GB prophylaxis (60% with histamine blockers (HB2) and 39% with proton pump inhibitors (PPI). Of these patients, 25.7% did not receive GU prophylaxis, although indicated it. Of the 55 moderate risk patients, 70.9% wer e receiving GU prophylaxis (22 with HB2 and 17 with PPI). Of the 14 low risk patients, 71% were using GU prophylaxis (6 with HB2 and 4 with PPI). CONCLUSIONS: Almost 80% of the patients made use of GB prophylactic drugs, with no agreement GU risk stratification. This study demonstrated the no adequate GU prophylaxis in the Brazilian ICU.
-
Transfusion practices in brazilian Intensive Care Units (pelo FUNDO-AMIB)
Rev Bras Ter Intensiva. 2006;18(3):234-241
Abstract
Transfusion practices in brazilian Intensive Care Units (pelo FUNDO-AMIB)
Rev Bras Ter Intensiva. 2006;18(3):234-241
DOI 10.1590/S0103-507X2006000300004
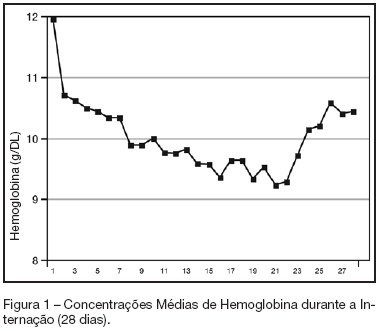
Views0See moreBACKGROUND AND OBJECTIVES: Anemia of critical illness is a multifactorial condition caused by blood loss, frequent phlebotomies and inadequate production of red blood cells (RBC). Controversy surrounds the most appropriate hemoglobin concentration “trigger” for transfusion of RBC. We aimed to evaluate transfusion practices in Brazilian ICUs. METHODS: A prospective study throughout a 2-week period in 19 Brazilian ICUs. Hemoglobin (Hb) level, transfusion rate, organ dysfunction assessment and 28-day mortality were evaluated. Primary indication for transfusion and pretransfusion hemoglobin level were collected for each transfusion. RESULTS: Two hundred thirty-one patients with an ICU length of stay longer than 48h were included. An Hb level lower than 10 g/dL was found in 33% on admission in the ICU. A total of 348 RBC units were transfused in 86 patients (36.5%). The mean pretransfusion hemoglobin level was 7.7 ± 1.1 g/dL. Transfused-patients had significantly higher SOFA score (7.9 ± 4.6 vs 5.6 ± 3.8, p < 0.05, respectively), days on mechanical ventilation (10.7 ± 8.2 vs 7.2 ± 6.4, p < 0.05) and days on vasoactive drugs (6.7 ± 6.4 vs 4.2 ± 4.0, p < 0.05) than non-transfused patients despite similar APACHE II scores (15.2 ± 8.1 vs 14.2 ± 8.1, NS). Transfused patients had higher mortality rate (43.5%) than non-transfused patients (36.3%) (RR 0.60-1.15, NS). Only one patient (0.28%) had febrile non-hemolytic transfusion and urticarial reactions. CONCLUSIONS: Anemia is common in critically ill patients.It seems from the present study that transfusion practices in Brazil have had a more restrictive approach with a lower limit "transfusion trigger".
Views0Abstract
Transfusion practices in brazilian Intensive Care Units (pelo FUNDO-AMIB)
Rev Bras Ter Intensiva. 2006;18(3):234-241
DOI 10.1590/S0103-507X2006000300004
Views0See moreBACKGROUND AND OBJECTIVES: Anemia of critical illness is a multifactorial condition caused by blood loss, frequent phlebotomies and inadequate production of red blood cells (RBC). Controversy surrounds the most appropriate hemoglobin concentration “trigger” for transfusion of RBC. We aimed to evaluate transfusion practices in Brazilian ICUs. METHODS: A prospective study throughout a 2-week period in 19 Brazilian ICUs. Hemoglobin (Hb) level, transfusion rate, organ dysfunction assessment and 28-day mortality were evaluated. Primary indication for transfusion and pretransfusion hemoglobin level were collected for each transfusion. RESULTS: Two hundred thirty-one patients with an ICU length of stay longer than 48h were included. An Hb level lower than 10 g/dL was found in 33% on admission in the ICU. A total of 348 RBC units were transfused in 86 patients (36.5%). The mean pretransfusion hemoglobin level was 7.7 ± 1.1 g/dL. Transfused-patients had significantly higher SOFA score (7.9 ± 4.6 vs 5.6 ± 3.8, p < 0.05, respectively), days on mechanical ventilation (10.7 ± 8.2 vs 7.2 ± 6.4, p < 0.05) and days on vasoactive drugs (6.7 ± 6.4 vs 4.2 ± 4.0, p < 0.05) than non-transfused patients despite similar APACHE II scores (15.2 ± 8.1 vs 14.2 ± 8.1, NS). Transfused patients had higher mortality rate (43.5%) than non-transfused patients (36.3%) (RR 0.60-1.15, NS). Only one patient (0.28%) had febrile non-hemolytic transfusion and urticarial reactions. CONCLUSIONS: Anemia is common in critically ill patients.It seems from the present study that transfusion practices in Brazil have had a more restrictive approach with a lower limit "transfusion trigger".
-
Blood transfusion in intensive care: an epidemiological observational study
Rev Bras Ter Intensiva. 2006;18(3):242-250
Abstract
Blood transfusion in intensive care: an epidemiological observational study
Rev Bras Ter Intensiva. 2006;18(3):242-250
DOI 10.1590/S0103-507X2006000300005
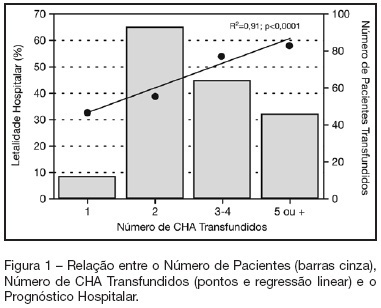
Views0See moreBACKGROUND AND OBJECTIVES: Packed red blood cell (PRBC) transfusion is frequent in intensive care unit (ICU). However, the consequences of anemia in ICU patients are poorly understood. Our aim was to evaluate the prevalence, indications, pre-transfusion hematocrit and hemoglobin levels, and outcomes of ICU patients transfused with PRBC. METHODS: Prospective cohort study conducted at a medical-surgical ICU of a teaching hospital during a 16-month period. Patients’ demographic, clinical, laboratory and transfusion-related data were collected. Logistic regression was used after univariate analyses. RESULTS: A total of 698 patients were evaluated and 244 (35%) received PRBC, mainly within the first four days of ICU (82.4%). Transfusion was more frequent in medical and emergency surgical patients. The mean pre-transfusion hematocrit and hemoglobin were 22.8% ± 4.5% and 7.9 ± 1.4 g/dL, respectively. Transfused patients received 4.4 ± 3.7 PRBC during ICU stay and 2.2 ± 1 PRBC at each transfusion. The ICU (39.8% versus 13.2%; p < 0.0001) and hospital (48.8% versus 20.3%; p < 0.0001) mortality rates were higher in transfused patients. Mortality increased as the number of transfused PRBC increased (R² = 0.91). In logistic regression, predictive factors for PRBC transfusion were hepatic cirrhosis, mechanical ventilation (MV), type and duration of ICU admission, and hematocrit. The independent factors associated to hospital mortality were MV, transfusions of more than five PRBC and SAPS II score. CONCLUSIONS: PRBC transfusions are frequent in ICU patients, especially in those with medical and emergency surgical complications, longer ICU stay, and hepatic cirrhosis and in need of MV. Pre-transfusion hemoglobin levels were lower than those previously reported. In our study, PRBC transfusion was associated with increased mortality.
Views0Abstract
Blood transfusion in intensive care: an epidemiological observational study
Rev Bras Ter Intensiva. 2006;18(3):242-250
DOI 10.1590/S0103-507X2006000300005
Views0See moreBACKGROUND AND OBJECTIVES: Packed red blood cell (PRBC) transfusion is frequent in intensive care unit (ICU). However, the consequences of anemia in ICU patients are poorly understood. Our aim was to evaluate the prevalence, indications, pre-transfusion hematocrit and hemoglobin levels, and outcomes of ICU patients transfused with PRBC. METHODS: Prospective cohort study conducted at a medical-surgical ICU of a teaching hospital during a 16-month period. Patients’ demographic, clinical, laboratory and transfusion-related data were collected. Logistic regression was used after univariate analyses. RESULTS: A total of 698 patients were evaluated and 244 (35%) received PRBC, mainly within the first four days of ICU (82.4%). Transfusion was more frequent in medical and emergency surgical patients. The mean pre-transfusion hematocrit and hemoglobin were 22.8% ± 4.5% and 7.9 ± 1.4 g/dL, respectively. Transfused patients received 4.4 ± 3.7 PRBC during ICU stay and 2.2 ± 1 PRBC at each transfusion. The ICU (39.8% versus 13.2%; p < 0.0001) and hospital (48.8% versus 20.3%; p < 0.0001) mortality rates were higher in transfused patients. Mortality increased as the number of transfused PRBC increased (R² = 0.91). In logistic regression, predictive factors for PRBC transfusion were hepatic cirrhosis, mechanical ventilation (MV), type and duration of ICU admission, and hematocrit. The independent factors associated to hospital mortality were MV, transfusions of more than five PRBC and SAPS II score. CONCLUSIONS: PRBC transfusions are frequent in ICU patients, especially in those with medical and emergency surgical complications, longer ICU stay, and hepatic cirrhosis and in need of MV. Pre-transfusion hemoglobin levels were lower than those previously reported. In our study, PRBC transfusion was associated with increased mortality.
-
Cancer disease should not be a limitative factor for admission of high risk surgical patients to an intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):251-255
Abstract
Cancer disease should not be a limitative factor for admission of high risk surgical patients to an intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):251-255
DOI 10.1590/S0103-507X2006000300006
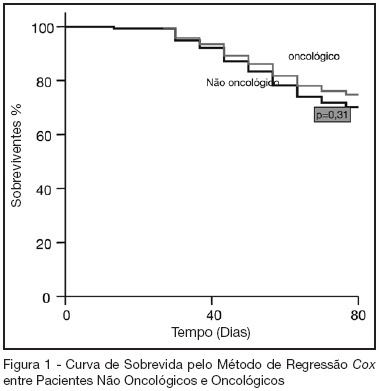
Views0See moreBACKGROUND AND OBJECTIVES: Oncologic diseases are conditions that have influence in the treatment offered to affected patients. The aim of this study was to compare hospitalar outcome of oncologic and non oncologic patients submitted to high risk elective surgery. METHODS: Prospective, observational cohort study realized in an ICU of a tertiary hospital during the period between 04/01/2005 and 07/31/2005. Demographic data, APACHE II and MODS scores and laboratorial and hemodynamic variables were collected and complications like re-intervention need for mechanical ventilation, red blood cell transfusions and pulmonary artery catheter use during the post-operative period were evaluated. All patients were followed until hospital discharge or death. T student and Mann Whitney tests were used to compare numerical variables. Chi-square test was used to compare categorical variables. A p < 0.05 was considered as significant. RESULTS: 119 patients were included in the study. 43 were oncologic and 76 were non-oncologic. 52.9% were female. Mean age was 65.1 ± 14.1 years. Mean APACHE II score was 16.5 ± 5.8 and MODS median was 3 (2-6). Median length of surgery was 5 (3.3-7) hours and ICU and hospital mortality were 10.9% and 25.2%, respectively. Oncologic patients had greater length of hospital stay and length of stay before surgery. These results were statistically significant. Hospital mortality of oncologic patients was not greater than non-oncologic patients (22.4% versus 30.2%, p = 0.32). CONCLUSIONS: In this series, oncologic patients submitted to high risk surgery had the same mortality rate as non-onconlogic patients with similar disease severity.
Views0Abstract
Cancer disease should not be a limitative factor for admission of high risk surgical patients to an intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):251-255
DOI 10.1590/S0103-507X2006000300006
Views0See moreBACKGROUND AND OBJECTIVES: Oncologic diseases are conditions that have influence in the treatment offered to affected patients. The aim of this study was to compare hospitalar outcome of oncologic and non oncologic patients submitted to high risk elective surgery. METHODS: Prospective, observational cohort study realized in an ICU of a tertiary hospital during the period between 04/01/2005 and 07/31/2005. Demographic data, APACHE II and MODS scores and laboratorial and hemodynamic variables were collected and complications like re-intervention need for mechanical ventilation, red blood cell transfusions and pulmonary artery catheter use during the post-operative period were evaluated. All patients were followed until hospital discharge or death. T student and Mann Whitney tests were used to compare numerical variables. Chi-square test was used to compare categorical variables. A p < 0.05 was considered as significant. RESULTS: 119 patients were included in the study. 43 were oncologic and 76 were non-oncologic. 52.9% were female. Mean age was 65.1 ± 14.1 years. Mean APACHE II score was 16.5 ± 5.8 and MODS median was 3 (2-6). Median length of surgery was 5 (3.3-7) hours and ICU and hospital mortality were 10.9% and 25.2%, respectively. Oncologic patients had greater length of hospital stay and length of stay before surgery. These results were statistically significant. Hospital mortality of oncologic patients was not greater than non-oncologic patients (22.4% versus 30.2%, p = 0.32). CONCLUSIONS: In this series, oncologic patients submitted to high risk surgery had the same mortality rate as non-onconlogic patients with similar disease severity.
-
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
Abstract
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
Views0BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients’ level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Keywords:consciousness disturbancesmaximum inspiratory pressuremechanical ventilationunidirectional valveWeaningSee moreViews0Abstract
Comparison of two methods for measurement of maximal inspiratory pressure in patients with and without alterations of the conscience’s level
Rev Bras Ter Intensiva. 2006;18(3):256-262
DOI 10.1590/S0103-507X2006000300007
Views0BACKGROUND AND OBJECTIVES: There is no literature consensus about the time of airway occlusion sufficient enough to get a true PImax during weaning from mechanical ventilation (MV). So, the main objectives of the present study were to compare two methods PImax measurement and to evaluate the influence of patients’ level of conscience on them. METHODS: The population was composed by 28 general ICU patients, with MV > 48h, in a weaning process, divided into two groups according to Glasgow coma scale score: with (GCS < 15) and without (GCS = 15) alterations of conscience level. The airway was occluded by using an unidirectional valve for 20s (PImaxT20), or for a maximum time of one minute if a plateau of inspiratory pressure was not observed during three consecutive inspirations (PImaxTid). RESULTS: PImaxT20 (mean ± SD, cmH2O) values were similar in both groups (44 ± 16 vs42 ± 15, p = 0.52). However, PImaxTid values, as long as the time needed to their attainment, were greater in GCS < 15 group (65 ± 24 vs 47 ± 23cmH2O and 37 ± 10 vs24 ± 8s, p = 0.04 and 0.0019, respectively). CONCLUSIONS: The method commonly used of 20s airway occlusion seems to be inadequate to get the true PImax in patients with alterations of the level of conscience. Additional studies, now in a more homogeneous group (e. g.: patients with structural brain lesion), are needed to clarify these findings.
Keywords:consciousness disturbancesmaximum inspiratory pressuremechanical ventilationunidirectional valveWeaningSee more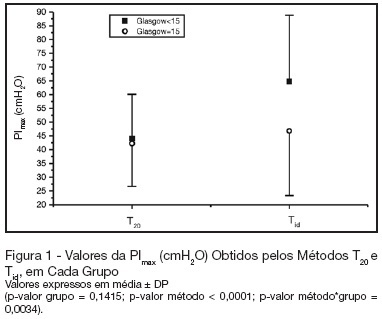
-
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
Abstract
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
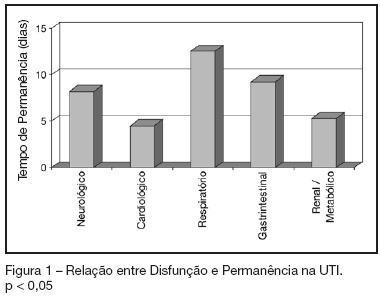
Views0See moreBACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
Views0Abstract
Morbidity and mortality of elderly patients admitted to an Intensive Care Unit of a University Hospital in Fortaleza
Rev Bras Ter Intensiva. 2006;18(3):263-267
DOI 10.1590/S0103-507X2006000300008
Views0See moreBACKGROUND AND OBJECTIVES: To identify the severity of elderly patients admitted to the intensive care unit (ICU) in a university hospital, relating it to the in-ICU mortality. METHODS: Retrospective study, with analysis of 130 patients admitted to ICU from March 2004 to July 2005. RESULTS: Of the 130 patients, there was a predominance of women, and mean 72.2 ± 7.3 years. There were more patients between 65 and 74 years old. More than 80% of the patients had come from the university hospital itself. The main dysfunctions were from the cardiocirculatory and respiratory systems. Sepsis caused 23.8% of the admissions. Length of stay in ICU was 8.2 ± 7.6 days. The mean of APACHE II was 18.2 ± 7.2. Lesser values of APACHE II, length of stay and mortality were observed in patients with cardiocirculatory dysfunction. The in-ICU mortality was 33.9%, 6.2% before 48 hours. The standardized mortality ratio (SMR) was 0.988. CONCLUSIONS: The age groups did not determine difference between values of APACHE II. They were related neither to higher mortality rate, nor to higher ICU length of stay. Patients with cardiocirculatory dysfunctions had lesser values of APACHE II, ICU length of stay and in-ICU mortality.
-
Assessment of effectiveness and safety of Yale insulin infusion protocol in a brazilian medical and surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(3):268-275
Abstract
Assessment of effectiveness and safety of Yale insulin infusion protocol in a brazilian medical and surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(3):268-275
DOI 10.1590/S0103-507X2006000300009
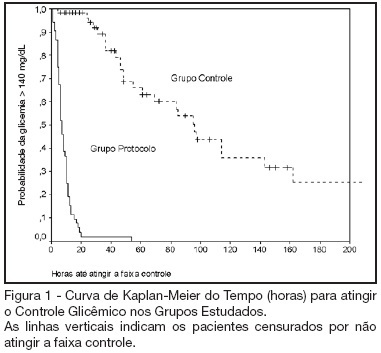
Views0See moreBACKGROUND AND OBJECTIVES: Actually tight glycemic control is a major concern in critical care. The objective of this study was to evaluate effectiveness and safety of Yale insulin infusion protocol in a Brazilian medical and surgical intensive care unit. METHODS: Retrospective, before-after cohort study. Selected end-points were mean blood glucose levels, time-to-reach target range of 80 – 140 mg/dL, and percent of blood glucose in target range and hypoglycemia incidence. RESULTS: Were studied 112 patients: 60 in control group (CG) and 52 in protocol group (PG). Bedside blood glucose was measured 5392 times for a mean value of 131.2 ± 14.7 mg/dL in the PG versus 2485 times for a mean value of 181.7 ± 36.1 mg/dL in the CG. Blood glucose values were in the target range 65% and 32% of the times, respectively for PG and CG groups (p < 0.001). The median time to reach glucose target range was 7 h (range 4 -10 h) for PG and 96 hr (range 46 - 278 h) for CG (p < 0.001). Incidence of severe hypoglycemia did not reach difference statistically significant: 4 patients in PG versus 2 patients in CG. CONCLUSIONS: Yale insulin infusion protocol was effective and safe to improve blood glucose control in a Brazilian medical and surgical intensive care unit.
Views0Abstract
Assessment of effectiveness and safety of Yale insulin infusion protocol in a brazilian medical and surgical Intensive Care Unit
Rev Bras Ter Intensiva. 2006;18(3):268-275
DOI 10.1590/S0103-507X2006000300009
Views0See moreBACKGROUND AND OBJECTIVES: Actually tight glycemic control is a major concern in critical care. The objective of this study was to evaluate effectiveness and safety of Yale insulin infusion protocol in a Brazilian medical and surgical intensive care unit. METHODS: Retrospective, before-after cohort study. Selected end-points were mean blood glucose levels, time-to-reach target range of 80 – 140 mg/dL, and percent of blood glucose in target range and hypoglycemia incidence. RESULTS: Were studied 112 patients: 60 in control group (CG) and 52 in protocol group (PG). Bedside blood glucose was measured 5392 times for a mean value of 131.2 ± 14.7 mg/dL in the PG versus 2485 times for a mean value of 181.7 ± 36.1 mg/dL in the CG. Blood glucose values were in the target range 65% and 32% of the times, respectively for PG and CG groups (p < 0.001). The median time to reach glucose target range was 7 h (range 4 -10 h) for PG and 96 hr (range 46 - 278 h) for CG (p < 0.001). Incidence of severe hypoglycemia did not reach difference statistically significant: 4 patients in PG versus 2 patients in CG. CONCLUSIONS: Yale insulin infusion protocol was effective and safe to improve blood glucose control in a Brazilian medical and surgical intensive care unit.
-
Severity indexes in an adult intensive care unit: clinical evaluation and nursing work
Rev Bras Ter Intensiva. 2006;18(3):276-281
Abstract
Severity indexes in an adult intensive care unit: clinical evaluation and nursing work
Rev Bras Ter Intensiva. 2006;18(3):276-281
DOI 10.1590/S0103-507X2006000300010
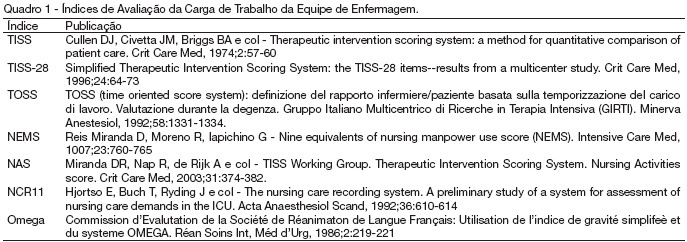
Views4See moreBACKGROUND AND OBJECTIVES: ICU is the hospital sectors that have interrupt assistance. Assistance with quality is a challenge for those who run human resources. It is also important to know the risk of the patient to the better use of resources. The aim of this study is to identify most used severity indexes in intensive care and classify them according with their finality METHODS: Library research (medline), using the key words: “Scoring systems and ICU”. The articles were selected in the period from March to May 2005. Books and thesis were also used. RESULTS: We identify seven indexes evaluating nursing workload: TISS, TISS-28, TOSS, NEMS, NAS, NCR11, and Omega. We identify 21 indexes evaluating clinical status: Killip Glasgow CRI APACHE II e III, Ransom, SS, SSS, SAPS, MLR, MPM, LIS, ARPI, SAPS (II), MPM II, ODIN, Ontario, MODS, SOFA, LOD, and PSI). CONCLUSIONS: Although indexes evaluating nursing workload are in a lower number, they are also fundamental to preview the need for material and human resources.
Views4Abstract
Severity indexes in an adult intensive care unit: clinical evaluation and nursing work
Rev Bras Ter Intensiva. 2006;18(3):276-281
DOI 10.1590/S0103-507X2006000300010
Views4See moreBACKGROUND AND OBJECTIVES: ICU is the hospital sectors that have interrupt assistance. Assistance with quality is a challenge for those who run human resources. It is also important to know the risk of the patient to the better use of resources. The aim of this study is to identify most used severity indexes in intensive care and classify them according with their finality METHODS: Library research (medline), using the key words: “Scoring systems and ICU”. The articles were selected in the period from March to May 2005. Books and thesis were also used. RESULTS: We identify seven indexes evaluating nursing workload: TISS, TISS-28, TOSS, NEMS, NAS, NCR11, and Omega. We identify 21 indexes evaluating clinical status: Killip Glasgow CRI APACHE II e III, Ransom, SS, SSS, SAPS, MLR, MPM, LIS, ARPI, SAPS (II), MPM II, ODIN, Ontario, MODS, SOFA, LOD, and PSI). CONCLUSIONS: Although indexes evaluating nursing workload are in a lower number, they are also fundamental to preview the need for material and human resources.
-
Renal protection in a surgical intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):282-291
Abstract
Renal protection in a surgical intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):282-291
DOI 10.1590/S0103-507X2006000300011
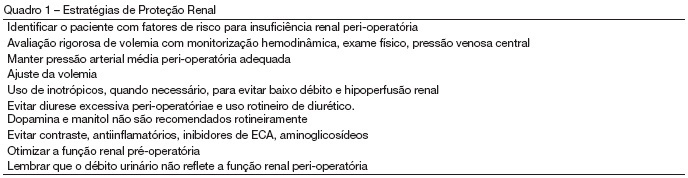
Views0See moreBACKGROUND AND OBJECTIVES: Perioperative renal dysfunction is an important cause of morbidity and mortality. With increase of life expectancy, older patients with more co-morbidity are being submitted to high risk surgical procedures, what make clinical practice related to organ protection possible modifier of short and long term survival. This review about renal protection in surgical intensive care unit points risk factors and discusses scientific evidence related to reduction of renal dysfunction in perioperative. CONTENTS: Although low extraction and adequate renal reserve of oxygen, the kidney is extremely sensible to hypoperfusion being renal acute insufficiency a frequent complication of hemodynamic instability. This apparent paradox, high oxygen content and reduced extraction with high incidence of renal damage to hypotension reflects the intra-renal gradient of oxygen, what makes renal medulla highly susceptible to ischemia. Factors associated with renal lesion are observed in all fases of perioperative period: fasting, contrast use, hypovolemia, hypotension, catecholamine and cytokine release, extracorporeal circulation, trauma, rabdomiolisys and aortic clamp. CONCLUSIONS: Management of renal damage is based in principals of perioperative renal physiology and glomerular hemodynamic. Clinical practice directed to organic protection should be implemented to minimize the impact this dysfunction.
Views0Abstract
Renal protection in a surgical intensive care unit
Rev Bras Ter Intensiva. 2006;18(3):282-291
DOI 10.1590/S0103-507X2006000300011
Views0See moreBACKGROUND AND OBJECTIVES: Perioperative renal dysfunction is an important cause of morbidity and mortality. With increase of life expectancy, older patients with more co-morbidity are being submitted to high risk surgical procedures, what make clinical practice related to organ protection possible modifier of short and long term survival. This review about renal protection in surgical intensive care unit points risk factors and discusses scientific evidence related to reduction of renal dysfunction in perioperative. CONTENTS: Although low extraction and adequate renal reserve of oxygen, the kidney is extremely sensible to hypoperfusion being renal acute insufficiency a frequent complication of hemodynamic instability. This apparent paradox, high oxygen content and reduced extraction with high incidence of renal damage to hypotension reflects the intra-renal gradient of oxygen, what makes renal medulla highly susceptible to ischemia. Factors associated with renal lesion are observed in all fases of perioperative period: fasting, contrast use, hypovolemia, hypotension, catecholamine and cytokine release, extracorporeal circulation, trauma, rabdomiolisys and aortic clamp. CONCLUSIONS: Management of renal damage is based in principals of perioperative renal physiology and glomerular hemodynamic. Clinical practice directed to organic protection should be implemented to minimize the impact this dysfunction.
-
Stevens-Johnson syndrome and toxical epidermal necrolysis in intensive care medicine
Rev Bras Ter Intensiva. 2006;18(3):292-297
Abstract
Stevens-Johnson syndrome and toxical epidermal necrolysis in intensive care medicine
Rev Bras Ter Intensiva. 2006;18(3):292-297
DOI 10.1590/S0103-507X2006000300012
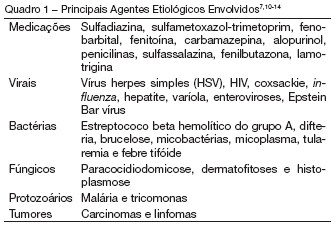
Views0See moreBACKGROUND AND OBJECTIVES: The Stevens Johnson Syndrome (SJS) and Toxical Epidermal Necrolisys (TEN) are important skin and mucosal lesions that need intensive care treatment. The aim of this article is to show a literature review about SJS and TEN. CONTENTS: This article reviews the concepts, diagnostic topics, clinical presentation and the principle of basic treatment in Intensive Care Unit for SJS and TEN. CONCLUSIONS: These illnesses are characterized as dermatological emergencies and its adequate management and cares must be part of the routine knowledge of the intensive care doctors.
Views0Abstract
Stevens-Johnson syndrome and toxical epidermal necrolysis in intensive care medicine
Rev Bras Ter Intensiva. 2006;18(3):292-297
DOI 10.1590/S0103-507X2006000300012
Views0See moreBACKGROUND AND OBJECTIVES: The Stevens Johnson Syndrome (SJS) and Toxical Epidermal Necrolisys (TEN) are important skin and mucosal lesions that need intensive care treatment. The aim of this article is to show a literature review about SJS and TEN. CONTENTS: This article reviews the concepts, diagnostic topics, clinical presentation and the principle of basic treatment in Intensive Care Unit for SJS and TEN. CONCLUSIONS: These illnesses are characterized as dermatological emergencies and its adequate management and cares must be part of the routine knowledge of the intensive care doctors.
-
Nutritional assessment of the critical ill patient
Rev Bras Ter Intensiva. 2006;18(3):298-306
Abstract
Nutritional assessment of the critical ill patient
Rev Bras Ter Intensiva. 2006;18(3):298-306
DOI 10.1590/S0103-507X2006000300013
Views0BACKGROUND AND OBJECTIVES: Nutritional state of patients affects them in their clinical evolution. Protein-caloric malnutrition contributes to the increase of morbidity and mortality in critical care. Regardless all the parameters available to assessment, there is no standard in hospital centers. In this review, we were looking for a method to nutrition assessment (NA) in critical patient that allow more adequate assessment and contribute to improvement in critical care. CONTENTS: In order to compare methods in NA in critical patient, search was performed in scientific papers aboutthis area. The keywords usedwere nutritional assessment, critical patient, critical care, hospital undernourishment and anthropometry. CONCLUSIONS: There are restrictions to different anthropometric parameters for NA when referring to critical patients. There is no consensus within authors about the best method for these patients and they no advise to choose only one parameter. We suggest for practice clinical in NA, one tool that include objective and subjective aspects in critical patients and identify those that are either undernourishments or in nutritional risks (Appendix 1).
Keywords:anthropometrycritical patienthospital undernourishmentintensive therapynutritional assessmentSee moreViews0Abstract
Nutritional assessment of the critical ill patient
Rev Bras Ter Intensiva. 2006;18(3):298-306
DOI 10.1590/S0103-507X2006000300013
Views0BACKGROUND AND OBJECTIVES: Nutritional state of patients affects them in their clinical evolution. Protein-caloric malnutrition contributes to the increase of morbidity and mortality in critical care. Regardless all the parameters available to assessment, there is no standard in hospital centers. In this review, we were looking for a method to nutrition assessment (NA) in critical patient that allow more adequate assessment and contribute to improvement in critical care. CONTENTS: In order to compare methods in NA in critical patient, search was performed in scientific papers aboutthis area. The keywords usedwere nutritional assessment, critical patient, critical care, hospital undernourishment and anthropometry. CONCLUSIONS: There are restrictions to different anthropometric parameters for NA when referring to critical patients. There is no consensus within authors about the best method for these patients and they no advise to choose only one parameter. We suggest for practice clinical in NA, one tool that include objective and subjective aspects in critical patients and identify those that are either undernourishments or in nutritional risks (Appendix 1).
Keywords:anthropometrycritical patienthospital undernourishmentintensive therapynutritional assessmentSee more -
Artigos de Revisão
Polyneuropathy in the critical ill patient: a common diagnosis in intensive care medicine?
Rev Bras Ter Intensiva. 2006;18(3):307-310
Abstract
Artigos de RevisãoPolyneuropathy in the critical ill patient: a common diagnosis in intensive care medicine?
Rev Bras Ter Intensiva. 2006;18(3):307-310
DOI 10.1590/S0103-507X2006000300014
Views0See moreBACKGROUND AND OBJECTIVES: The diffuse axonal polyneuropathy, more commonly known as Critical Illness Polyneuropathy (CIP), has been discussed by authors by decades; however, it has only been deeply studied over the last thirty years, becoming more important as an important cause of long term dependence on mechanical ventilation by seriously ill patients in intensive care medicine. CONTENTS: A significant reason for such interest is due to the importance of the CIP as complication of the septic shock and in patients with multiple organ failure, as much as responsible for the prolonging hospitalization in the Intensive Care Unit, as for the gradual reduction of the chance of survival. It has been suggested that the polyneuropathy is related with cytokines and other mediators which would increase the permeability of the vases, resulting in endoneural edema and causing the axonal injury. It is difficult to do the initial diagnostic, which, in general, are only possibly recognized when the sepsis complications or the multiple organs failure have been satisfactorily controlled. The diagnosis is made through the eletroneuromiography exam, and although there is still no effective drug treatment other than the control of the basic illness, it is consensus among multidisciplinary team that the development of the CIP does not have to be understood as a way to reduce the intensity of treatment. CONCLUSIONS: Spit of your prevalence, it is still unknown the mainly factors which are physiopathology associated as soon as your correct therapy.
Views0Abstract
Artigos de RevisãoPolyneuropathy in the critical ill patient: a common diagnosis in intensive care medicine?
Rev Bras Ter Intensiva. 2006;18(3):307-310
DOI 10.1590/S0103-507X2006000300014
Views0See moreBACKGROUND AND OBJECTIVES: The diffuse axonal polyneuropathy, more commonly known as Critical Illness Polyneuropathy (CIP), has been discussed by authors by decades; however, it has only been deeply studied over the last thirty years, becoming more important as an important cause of long term dependence on mechanical ventilation by seriously ill patients in intensive care medicine. CONTENTS: A significant reason for such interest is due to the importance of the CIP as complication of the septic shock and in patients with multiple organ failure, as much as responsible for the prolonging hospitalization in the Intensive Care Unit, as for the gradual reduction of the chance of survival. It has been suggested that the polyneuropathy is related with cytokines and other mediators which would increase the permeability of the vases, resulting in endoneural edema and causing the axonal injury. It is difficult to do the initial diagnostic, which, in general, are only possibly recognized when the sepsis complications or the multiple organs failure have been satisfactorily controlled. The diagnosis is made through the eletroneuromiography exam, and although there is still no effective drug treatment other than the control of the basic illness, it is consensus among multidisciplinary team that the development of the CIP does not have to be understood as a way to reduce the intensity of treatment. CONCLUSIONS: Spit of your prevalence, it is still unknown the mainly factors which are physiopathology associated as soon as your correct therapy.
-
Artigos de Revisão
Gas embolism
Rev Bras Ter Intensiva. 2006;18(3):311-315
Abstract
Artigos de RevisãoGas embolism
Rev Bras Ter Intensiva. 2006;18(3):311-315
DOI 10.1590/S0103-507X2006000300015
Views0See moreBACKGROUND AND OBJECTIVES: Gas embolism is an iatrogenic injury that has high morbidity and mortality. It’s a complication of clinical-surgical procedures, and it’s necessary that the health professionals know this entity. The aim of this study was to realize a review of the gas embolism, considering its pathophysiology, diagnosis and therapeutics aspects. CONTENTS: This article revises conceptually the gas embolism, dividing it in arterial and venous. Relate the mains physiopathology, diagnosis and therapeutics characteristics of the arterial and venous embolism. In addition, it’s also approach the paradoxical embolism, event that occurs by conversion of a venous embolism to an arterial embolism. CONCLUSIONS: Gas embolism is an important complication, and it’s present in many medical specialties. Knowledge about its physiopathology, and its diagnosis and therapeutic methods is essential to guarantee higher safety to the patients.
Views0Abstract
Artigos de RevisãoGas embolism
Rev Bras Ter Intensiva. 2006;18(3):311-315
DOI 10.1590/S0103-507X2006000300015
Views0See moreBACKGROUND AND OBJECTIVES: Gas embolism is an iatrogenic injury that has high morbidity and mortality. It’s a complication of clinical-surgical procedures, and it’s necessary that the health professionals know this entity. The aim of this study was to realize a review of the gas embolism, considering its pathophysiology, diagnosis and therapeutics aspects. CONTENTS: This article revises conceptually the gas embolism, dividing it in arterial and venous. Relate the mains physiopathology, diagnosis and therapeutics characteristics of the arterial and venous embolism. In addition, it’s also approach the paradoxical embolism, event that occurs by conversion of a venous embolism to an arterial embolism. CONCLUSIONS: Gas embolism is an important complication, and it’s present in many medical specialties. Knowledge about its physiopathology, and its diagnosis and therapeutic methods is essential to guarantee higher safety to the patients.
-
Artigos de Revisão
Challenges in prevention venous thromboembolism: critical ill patient approach
Rev Bras Ter Intensiva. 2006;18(3):316-319
Abstract
Artigos de RevisãoChallenges in prevention venous thromboembolism: critical ill patient approach
Rev Bras Ter Intensiva. 2006;18(3):316-319
DOI 10.1590/S0103-507X2006000300016
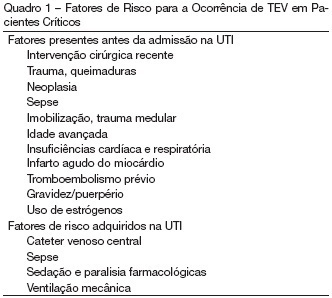
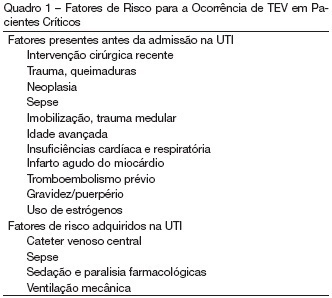
Views0See moreBACKGROUND AND OBJECTIVES: Venous thromboembolism (VTE), with includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common complication in critically ill patients, resulting in high morbidity and mortality. CONTENTS: Most patients treated in intensive care units (ICU) face a high risk of thromboembolic complications. Despite these considerations, the prevention of VTE may not be as high a priority in ICU patients as it is in other high-risk patient groups. Low molecular weight heparin (LMWH) may be the optimal prophylaxis in most ICU patients, but there is a lack of sufficient data including the paucity of VTE consensus and guidelines documents pertaining to critically ill patients. CONCLUSIONS: This article reviews background, current options, and recommendations regarding VTE in intensive care population emphasizing special diagnostic and treatment considerations in the ICU setting.
Views0Abstract
Artigos de RevisãoChallenges in prevention venous thromboembolism: critical ill patient approach
Rev Bras Ter Intensiva. 2006;18(3):316-319
DOI 10.1590/S0103-507X2006000300016
Views0See moreBACKGROUND AND OBJECTIVES: Venous thromboembolism (VTE), with includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common complication in critically ill patients, resulting in high morbidity and mortality. CONTENTS: Most patients treated in intensive care units (ICU) face a high risk of thromboembolic complications. Despite these considerations, the prevention of VTE may not be as high a priority in ICU patients as it is in other high-risk patient groups. Low molecular weight heparin (LMWH) may be the optimal prophylaxis in most ICU patients, but there is a lack of sufficient data including the paucity of VTE consensus and guidelines documents pertaining to critically ill patients. CONCLUSIONS: This article reviews background, current options, and recommendations regarding VTE in intensive care population emphasizing special diagnostic and treatment considerations in the ICU setting.
-
Rev Bras Ter Intensiva. 2006;18(3):320-320
Abstract
Rev Bras Ter Intensiva. 2006;18(3):320-320
DOI 10.1590/S0103-507X2006000300017
Views0Errata No resumo do trabalho “Dosagem do fator anti XA como marcador de eficácia da enoxaparina sódica em pacientes críticos” publicado na RBTI, 2006;Supl.:92, houve uma supressão de texto. […]See moreViews0Abstract
Rev Bras Ter Intensiva. 2006;18(3):320-320
DOI 10.1590/S0103-507X2006000300017
Views0Errata No resumo do trabalho “Dosagem do fator anti XA como marcador de eficácia da enoxaparina sódica em pacientes críticos” publicado na RBTI, 2006;Supl.:92, houve uma supressão de texto. […]See more
Volume Articles - Critical Care Science (CCS)
