-
Editorial
The inclusion of RBTI in the Scielo
Rev Bras Ter Intensiva. 2006;18(2):113-113
Abstract
Views0

-
Artigo Original
Referred medical patients not admitted to the Intensive Care Unit: prevalence, clinical characteristics and prognosis
Rev Bras Ter Intensiva. 2006;18(2):114-120
Abstract
Artigo OriginalReferred medical patients not admitted to the Intensive Care Unit: prevalence, clinical characteristics and prognosis
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
Views0See moreBACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
Views0Abstract
Artigo OriginalReferred medical patients not admitted to the Intensive Care Unit: prevalence, clinical characteristics and prognosis
Rev Bras Ter Intensiva. 2006;18(2):114-120
DOI 10.1590/S0103-507X2006000200002
Views0See moreBACKGROUND AND OBJECTIVES: Information on the outcomes of patients who were refused to the ICU is limited. The aims of this study were to compare the clinical characteristics of patients who were admitted with those of patients who were refused to the ICU and to identify clinical parameters associated with triage procedures. METHODS: Observational prospective cohort study. The following data were collected using a standard questionnaire: comorbidities, acute illness, vital status, laboratory data and APACHE II score. The end-points of interest were admission to the ICU and vital status at hospital discharge. RESULTS: A total of 455 patients were studied; 254 (56%) were admitted and 201 (44%) were not. The main reason for the refuse of admission was the lack of ICU beds (82%). Patients who were not admitted had a higher mortality (85% vs. 61%; p < 0.001). In multivariable analysis, the following variables were associated to non-admission [odds ratio, (95% confidence interval)]: metastatic cancer [5.6(1.7-18.7)], arterial systolic pressure < 90 mmHg [5.2(3.0-8.8)], age > 70 years [4.0(2.4-6.5)], hepatic cirrhosis [3.7(1.8-7.6)], and Glasgow coma scale < 5 [3.6(1.9-6.9)]. The variables associated with ICU admission were: mechanical ventilation [0.5(0.3-0.7)] and acute coronary syndromes [0.1(0.03-0.6)]. CONCLUSIONS: Refusal of ICU admission is frequent and generally as a consequence of ICU beds shortage. Patients who were not admitted had a higher mortality. Clinical characteristics associated with the refusal of admission were identified suggesting that they are used in clinical decision-making for ICU triage.
-
Artigo Original
Evaluation of T tube trial as a strategy of weaning from mechanical ventilation
Rev Bras Ter Intensiva. 2006;18(2):121-125
Abstract
Artigo OriginalEvaluation of T tube trial as a strategy of weaning from mechanical ventilation
Rev Bras Ter Intensiva. 2006;18(2):121-125
DOI 10.1590/S0103-507X2006000200003
Views0See moreBACKGROUND AND OBJECTIVES: Weaning from mechanical ventilation (MV) is an important strategy to reduce morbidity and mortality in critical care patients. In this setting, this study aimed at evaluation of T-tube trial (TT) in weaning from MV. METHODS: Patient admitted in the ICU were included if they present the following inclusion criteria: MV > 24 hours, no neuromuscular disorders, PaO2/FiO2 ratio >200, hemodynamic stability, reversion of the cause of respiratory failure, adequate respiratory drive. All were submitted to TT. Failure was defined by the presence of one of these symptoms: RR > 30 ipm, hypoxemia, tachycardia, arrhythmia, hypertension or hypotension. After two hours of TT, patients without failure criteria were extubated. After 48 hours of adequate spontaneous respiration the patient was considered successful weaned. Results were considered significant if p < 0.05. RESULTS: Forty-nine patients were included with a mean age 51.8 ± 21.7 years. The incidence of ARDS and septic shock were 26.5% and 32.7% and mean duration of MV was 11.9 ± 13 days. Discontinuation of MV occurred in 79.2%, reintubation in 31.6%, in a mean time of 13 ± 8.7 hours and in 75% of the cases it was due to respiratory failure. There was no correlation between success in TT and hemoglobin levels, PaO2/FiO2 ratio, age, gender, prior ARDS or septic shock. Weaning success was not correlated with none of the above variables. CONCLUSIONS: TT was adequated for weaning from mechanical ventilation in the majority of the cases. However, reintubation rate was high. Possible causes are the long period of TT, prior mechanical ventilation or the failure in the criteria used to indicate extubation.
Views0Abstract
Artigo OriginalEvaluation of T tube trial as a strategy of weaning from mechanical ventilation
Rev Bras Ter Intensiva. 2006;18(2):121-125
DOI 10.1590/S0103-507X2006000200003
Views0See moreBACKGROUND AND OBJECTIVES: Weaning from mechanical ventilation (MV) is an important strategy to reduce morbidity and mortality in critical care patients. In this setting, this study aimed at evaluation of T-tube trial (TT) in weaning from MV. METHODS: Patient admitted in the ICU were included if they present the following inclusion criteria: MV > 24 hours, no neuromuscular disorders, PaO2/FiO2 ratio >200, hemodynamic stability, reversion of the cause of respiratory failure, adequate respiratory drive. All were submitted to TT. Failure was defined by the presence of one of these symptoms: RR > 30 ipm, hypoxemia, tachycardia, arrhythmia, hypertension or hypotension. After two hours of TT, patients without failure criteria were extubated. After 48 hours of adequate spontaneous respiration the patient was considered successful weaned. Results were considered significant if p < 0.05. RESULTS: Forty-nine patients were included with a mean age 51.8 ± 21.7 years. The incidence of ARDS and septic shock were 26.5% and 32.7% and mean duration of MV was 11.9 ± 13 days. Discontinuation of MV occurred in 79.2%, reintubation in 31.6%, in a mean time of 13 ± 8.7 hours and in 75% of the cases it was due to respiratory failure. There was no correlation between success in TT and hemoglobin levels, PaO2/FiO2 ratio, age, gender, prior ARDS or septic shock. Weaning success was not correlated with none of the above variables. CONCLUSIONS: TT was adequated for weaning from mechanical ventilation in the majority of the cases. However, reintubation rate was high. Possible causes are the long period of TT, prior mechanical ventilation or the failure in the criteria used to indicate extubation.
-
Influence of the breathing time increase in the pulmonary ventilation of patients submitted to mechanical ventilation in controlled pressure mode
Rev Bras Ter Intensiva. 2006;18(2):126-130
Abstract
Influence of the breathing time increase in the pulmonary ventilation of patients submitted to mechanical ventilation in controlled pressure mode
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
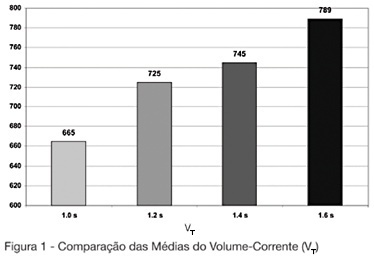
Views0See moreBACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.
Views0Abstract
Influence of the breathing time increase in the pulmonary ventilation of patients submitted to mechanical ventilation in controlled pressure mode
Rev Bras Ter Intensiva. 2006;18(2):126-130
DOI 10.1590/S0103-507X2006000200004
Views0See moreBACKGROUND AND OBJECTIVES: The mechanical ventilator support is one of the main used modalities of support in intensive therapy. In the modality of predetermined pressure, the maximum pressure is regulated, but the current volume (V T) is a complex function of the applied pressure and its speed to reach the pressure-target, of the available breathing time and the resistance to the breath. This paper has as objective to evaluate the influences of the increment of the breathing time in the pulmonary ventilation. METHODS: The study was carried through in the Adult ICU of the Regional Hospital of Mato Grosso do Sul, located in Campo Grande. They had been enclosed individuals adult, both genders, between 16 and 84 years, submitted to the mechanical ventilation in controlled pressure mode or in controlled-watched mode. The breathing time was adjusted in 1 sec, developing in 0.2 sec until the boundary-value of 1.6 sec. The tidal volume (V T) and the volume minute (V E) had been evaluated of 13 patients in the breathing times of 1s; 1.2s; 1.4s and 1.6s. RESULTS: In the mean of V T and V E an increasing increase was observed after-increment of the breathing time. We did not find in consulted literature, data which correlated the breathing time with alterations in the current volume. CONCLUSIONS: The increment of the breathing time in the ventilation for pressure control can have influence in the determination of the current volume offered to the patient.
-
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
Abstract
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
Views0See moreBACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
Views0Abstract
Standardization of weaning of the mechanical ventilation in a Intensive Care Unit: results afterwards one year
Rev Bras Ter Intensiva. 2006;18(2):131-136
DOI 10.1590/S0103-507X2006000200005
Views0See moreBACKGROUND AND OBJECTIVES: The weaning of mechanical ventilation is the process of transition from mechanical ventilation to spontaneous. The actual practice weaning reveals that the empirism is insufficient and inadequate. On the other side, the standardization of the weaning provides best conductions in the process. The objective of this study was to evaluate the effects of the application of a weaning protocol in an intensive care unit. METHODS: Method: It was included in this study all the patients in program of liberation from the mechanical ventilation, in which the evolution of the weaning was followed by the utilization of a pre-establish protocol and publicated by the service. RESULTS: It was studied 127 patients. In 91% (115) of the patients we had success in the weaning and unsuccess in 9% (12). The non-invasive ventilation after the extubation was utilized in 19% (24) of them. None obit was observed. Comparing the group of the patients that had success with the failed group, there were no statistically significant variations observed in sex (p = 0.96), APACHE II (19.5 versus 18.6 p = 0.75), risk of obit (29% versus 22% p = 0.54), MIP (38 versus 32 cmH2O p = 0.17), duration of mechanical ventilation (6 versus 7 days p = 0.70), PaO2/FiO2 relation (324 versus 312 p = 0.83), weaning modality (PSV or T Tube p = 0.29). There were statistically significant variations observed in rapid shallow respiratory index (59 versus 77 p = 0.02) and duration of the weaning (1 versus 30 hours p < 0.001). CONCLUSIONS: The weaning of the ventilation realized following the standardization brought improvement in its conduction, maintaining the high success index with low mortality.
-
Variability in interventions with pulmonary artery catheter data: Brazilian experience
Rev Bras Ter Intensiva. 2006;18(2):137-142
Abstract
Variability in interventions with pulmonary artery catheter data: Brazilian experience
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
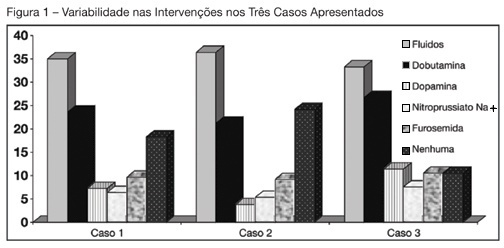
Views0See moreBACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
Views0Abstract
Variability in interventions with pulmonary artery catheter data: Brazilian experience
Rev Bras Ter Intensiva. 2006;18(2):137-142
DOI 10.1590/S0103-507X2006000200006
Views0See moreBACKGROUND AND OBJECTIVES: Use of Pulmonary Artery Catheter (PAC) is still a debatable issue, mainly due to questions raised about its security and efficacy. This study reproduced in a sample of Brazilian physicians, another one conducted amidst American doctors, in which was pointed out the heterogeneity of clinical decisions guided by data obtained from PAC. METHODS: During the Brazilian Congress of Intensive Care Medicine (Curitiba 2004), doctors were asked to answer a survey form with three vignettes. Each of them contained PAC data and one half of the surveys contained echocardiographic information. Every doctor was asked to select one of six interventions for each vignette. A homogeneous answer was considered when it was selected by at least 80% of the respondents. RESULTS: Two hundred and thirty seven doctors answered the questionnaires. They selected completely different therapeutic interventions in all three vignettes and none of the interventions achieved more than 80% agreement. Variability persisted with the choices guided by echocardiography. CONCLUSIONS: As in the original study, we observed total heterogeneity of therapeutic interventions guided by CAP and echocardiography. These results could be caused by lack of knowledge about basic pathophysiologic concepts and maybe we had to improve its teaching at the medical school benches.
-
Cardiac arrest and cardiopulmonary resuscitation knowledge of Critical Care Nursing
Rev Bras Ter Intensiva. 2006;18(2):143-147
Abstract
Cardiac arrest and cardiopulmonary resuscitation knowledge of Critical Care Nursing
Rev Bras Ter Intensiva. 2006;18(2):143-147
DOI 10.1590/S0103-507X2006000200007
Views0See moreBACKGROUND AND OBJECTIVES: In general, as ICU nursing staff is always close from the patients, their members most commonly identify the cardiac arrest and begin the cardiac and pulmonary resuscitation (CPR). The objective of this study was to evaluate the critical care nursing staff theoretical knowledge about cardiac arrest and CPR, as a basis for an in-service training. METHODS: Descriptive research with quantitative approach developed in an ICU, of general hospital at state of Santa Catarina – Brazil. The population was composed of nurses, nursing technicians and nursing assistants. The data were collected with a structured questionnaire with questions about the theme. The results were analyzed based on medical and nursing bibliographies about cardiac arrest and cardiopulmonary resuscitation. RESULTS: Twenty-six professionals answered the questionnaire, fifty four percent worked for more than two years in the ICU. The cardiac arrest signals were identified correctly by only 15.4% of the professionals. The main causes of cardiac arrest were mentioned correctly by 53.8% of participants. Answered correctly the most used medications in a CPR 65.4% of the participants. CONCLUSIONS: The work time of the nursing professionals in ICU and their professional category had influenced positively the knowledge about CPR and cardiac arrest. The fact that the majority of the participants (84.6%) do not identify correctly cardiac arrest and 34.6% do not recognize the medications used, may compromise the beginning, organization and quickness of the maneuvers. The study may present some basis for the theoretical approach of an in-service training program for the ICU nursing staff of the hospital where the study was held.
Views0Abstract
Cardiac arrest and cardiopulmonary resuscitation knowledge of Critical Care Nursing
Rev Bras Ter Intensiva. 2006;18(2):143-147
DOI 10.1590/S0103-507X2006000200007
Views0See moreBACKGROUND AND OBJECTIVES: In general, as ICU nursing staff is always close from the patients, their members most commonly identify the cardiac arrest and begin the cardiac and pulmonary resuscitation (CPR). The objective of this study was to evaluate the critical care nursing staff theoretical knowledge about cardiac arrest and CPR, as a basis for an in-service training. METHODS: Descriptive research with quantitative approach developed in an ICU, of general hospital at state of Santa Catarina – Brazil. The population was composed of nurses, nursing technicians and nursing assistants. The data were collected with a structured questionnaire with questions about the theme. The results were analyzed based on medical and nursing bibliographies about cardiac arrest and cardiopulmonary resuscitation. RESULTS: Twenty-six professionals answered the questionnaire, fifty four percent worked for more than two years in the ICU. The cardiac arrest signals were identified correctly by only 15.4% of the professionals. The main causes of cardiac arrest were mentioned correctly by 53.8% of participants. Answered correctly the most used medications in a CPR 65.4% of the participants. CONCLUSIONS: The work time of the nursing professionals in ICU and their professional category had influenced positively the knowledge about CPR and cardiac arrest. The fact that the majority of the participants (84.6%) do not identify correctly cardiac arrest and 34.6% do not recognize the medications used, may compromise the beginning, organization and quickness of the maneuvers. The study may present some basis for the theoretical approach of an in-service training program for the ICU nursing staff of the hospital where the study was held.
-
Risk factors for early-onset neonatal sepsis in Brazilian public hospital short-title: early-onset neonatal sepsis
Rev Bras Ter Intensiva. 2006;18(2):148-153
Abstract
Risk factors for early-onset neonatal sepsis in Brazilian public hospital short-title: early-onset neonatal sepsis
Rev Bras Ter Intensiva. 2006;18(2):148-153
DOI 10.1590/S0103-507X2006000200008
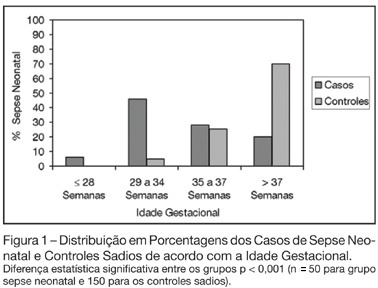
Views0See moreBACKGROUND AND OBJECTIVES: The determination of the risk factors to early-onset neonatal sepsis in our country is essential to prevent and reduce the mortality associated with this syndrome. Thus, the objective of this study was to determine the frequency and associated risk factors to early-onset neonatal sepsis in public hospital in Southern Brazil. METHODS: Observational, case-control study. Were included neonates with diagnostic of early-onset neonatal sepsis and as controls, neonates without neonatal infection. Were included 50 cases and 3 controls for each case resulting in a total sample of 200 patients. Associations were considered significant when p < 0.05. RESULTS: The sepsis frequency was 50.3 per 1000 born-alive. Risk factors associated to the development of neonatal sepsis were prematurity (OR 9.33; p < 0.001), low birth weight (OR 11.74; p < 0.001), maternal infection (OR 2.28; p = 0.009), mother with history of previous infant with neonatal sepsis (OR 6.43; p = 0.035) and rupture of the membranes more than 18 hours before delivery (OR 9.33; p = 0.001). CONCLUSIONS: Neonatal sepsis was very frequent in the study. Prematurity, low birth weight, maternal infection and mother’s having had a previous infant with neonatal sepsis are risk factors for early-onset neonatal sepsis.
Views0Abstract
Risk factors for early-onset neonatal sepsis in Brazilian public hospital short-title: early-onset neonatal sepsis
Rev Bras Ter Intensiva. 2006;18(2):148-153
DOI 10.1590/S0103-507X2006000200008
Views0See moreBACKGROUND AND OBJECTIVES: The determination of the risk factors to early-onset neonatal sepsis in our country is essential to prevent and reduce the mortality associated with this syndrome. Thus, the objective of this study was to determine the frequency and associated risk factors to early-onset neonatal sepsis in public hospital in Southern Brazil. METHODS: Observational, case-control study. Were included neonates with diagnostic of early-onset neonatal sepsis and as controls, neonates without neonatal infection. Were included 50 cases and 3 controls for each case resulting in a total sample of 200 patients. Associations were considered significant when p < 0.05. RESULTS: The sepsis frequency was 50.3 per 1000 born-alive. Risk factors associated to the development of neonatal sepsis were prematurity (OR 9.33; p < 0.001), low birth weight (OR 11.74; p < 0.001), maternal infection (OR 2.28; p = 0.009), mother with history of previous infant with neonatal sepsis (OR 6.43; p = 0.035) and rupture of the membranes more than 18 hours before delivery (OR 9.33; p = 0.001). CONCLUSIONS: Neonatal sepsis was very frequent in the study. Prematurity, low birth weight, maternal infection and mother’s having had a previous infant with neonatal sepsis are risk factors for early-onset neonatal sepsis.
-
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
Abstract
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
DOI 10.1590/S0103-507X2006000200009
Views0See moreBACKGROUND AND OBJECTIVES: The main cardiovascular function is to maintain the adequate perfusion e oxygen delivery to the cells. Physiologically, this is controlled by the cellular metabolic rate. The critically ill patients are in high danger of tissue hipoperfusion and this is directly related to cellular injury and organ dysfunction. Therefore, the tissue perfusion monitoring makes part and is indissociated of hemodynamic evaluation of the critically ill patient and is indicated to all this patients. The objective was to define recommendations about clinical utility of different tolls to bedside perfusion monitoring. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MedLine in the period from 1996 to 2004. RESULTS: Recommendations were done about the utility of clinical monitoring of tissue perfusion, temperature gradient and transcutaneous oxygen monitoring, serum lactate, base excess, SvO² and ScvO², gastric and sublingual capnometry, CO² venous-arterial gradient and Orthogonal Polarization Spectral (OPS). CONCLUSIONS: The homodynamic compensation of a critically ill patient isn’t complete unless the tissue perfusion is corrected. Many different methods of monitoring is available and are useful in clinical practice, however, none has accuracy and effectiveness characteristics to be used independently of clinical context.
Views0Abstract
Brazilian consensus of monitoring and hemodynamic support – Part IV: tissue perfusion evaluation
Rev Bras Ter Intensiva. 2006;18(2):154-160
DOI 10.1590/S0103-507X2006000200009
Views0See moreBACKGROUND AND OBJECTIVES: The main cardiovascular function is to maintain the adequate perfusion e oxygen delivery to the cells. Physiologically, this is controlled by the cellular metabolic rate. The critically ill patients are in high danger of tissue hipoperfusion and this is directly related to cellular injury and organ dysfunction. Therefore, the tissue perfusion monitoring makes part and is indissociated of hemodynamic evaluation of the critically ill patient and is indicated to all this patients. The objective was to define recommendations about clinical utility of different tolls to bedside perfusion monitoring. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MedLine in the period from 1996 to 2004. RESULTS: Recommendations were done about the utility of clinical monitoring of tissue perfusion, temperature gradient and transcutaneous oxygen monitoring, serum lactate, base excess, SvO² and ScvO², gastric and sublingual capnometry, CO² venous-arterial gradient and Orthogonal Polarization Spectral (OPS). CONCLUSIONS: The homodynamic compensation of a critically ill patient isn’t complete unless the tissue perfusion is corrected. Many different methods of monitoring is available and are useful in clinical practice, however, none has accuracy and effectiveness characteristics to be used independently of clinical context.
-
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
Abstract
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
Views0See moreBACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
Views0Abstract
Brazilian consensus of monitoring and hemodynamic support – Part V: hemodynamic support
Rev Bras Ter Intensiva. 2006;18(2):161-176
DOI 10.1590/S0103-507X2006000200010
Views0See moreBACKGROUND AND OBJECTIVES: Shock occurs when the circulatory system cannot maintain adequate cellular perfusion. If this condition is not reverted irreversible cellular injury establishes. Shock treatment has as its initial priority the fast and vigorous correction of mean arterial pressure and cardiac output to maintain life and avoid or lessen organic dysfunctions. Fluid challenge and vasoactive drugs are necessary to warrant an adequate tissue perfusion and maintenance of function of different organs and systems, always guided by cardiovascular monitorization. The recommendations built in this consensus are aimed to guide hemodynamic support needed to maintain adequate tisular perfusion. METHODS: Modified Delphi methodology was used to create and quantify the consensus between the participants. AMIB indicated a coordinator who invited more six experts in the area of monitoring and hemodynamic support to constitute the Consensus Advisory Board. Twenty five physician and two nurses selected from different regions of the country completed the expert panel, which reviewed the pertinent bibliography listed at the MEDLINE in the period from 1996 to 2004. RESULTS: Recommendations were made answering 17 questions about hemodynamic support with focus on fluid challenge, red blood cell transfusions, vasoactive drugs and perioperative hemodynamic optimization. CONCLUSIONS: Hemodynamic monitoring by itself does not reduce the mortality of critically ill patients, however, we believe that the correct interpretation of the data obtained by the hemodynamic monitoring and the use of hemodynamic support protocols based on well defined tissue perfusion goals can improve the outcome of these patients.
-
Update on cardiopulmonary resuscitation: what changed with the new guidelines
Rev Bras Ter Intensiva. 2006;18(2):177-185
Abstract
Update on cardiopulmonary resuscitation: what changed with the new guidelines
Rev Bras Ter Intensiva. 2006;18(2):177-185
DOI 10.1590/S0103-507X2006000200011
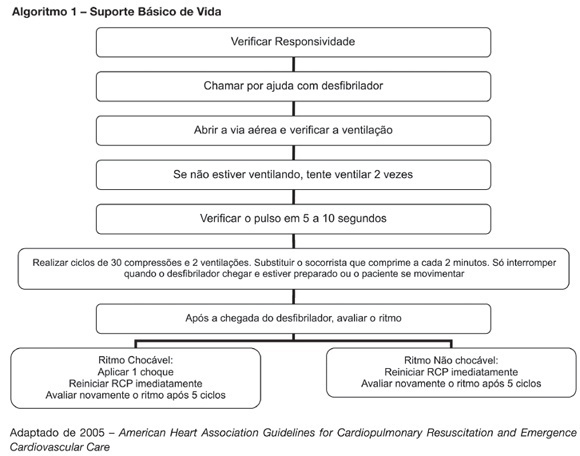
Views1See moreBACKGROUND AND OBJECTIVES: New resuscitation guidelines contain significant changes intended to improve resuscitation practice and survival from cardiac arrest. This article provides an overview of the key changes on resuscitation for healthcare provider. CONTENTS: There are several new recommendations on cardiopulmonary resuscitation (CPR), the major are intended to provide good circulation during cardiac arrest. The most important change is the emphasis on high-quality chest compressions with minimal interruptions. The universal 30:2 ratio is recommended to simplify training, to achieve optimal compression rates and to reduce the frequency of interruptions. Only one shock is delivered when indicated, followed immediately by CPR. This shock should be of 120-200J on a biphasic wave or 360J on a monophasic wave. Rescuers should not interrupt chest compressions to check rhythm until after about 5 cycles or approximately 2 minutes of CPR. After this period, if an organized rhythm is present, the healthcare provider should check for a pulse. There are several little changes about the drugs administrated during CPR according to the rhythm. Given the lack of documented effect of drug therapy in improving long-term outcome from cardiac arrest, the sequence for CPR deemphasizes drug administration and reemphasizes basic life support. CONCLUSIONS: The update on the new resuscitation guidelines is important to improve the quality of resuscitation and achieve better survival rates from our critical care patients.
Views1Abstract
Update on cardiopulmonary resuscitation: what changed with the new guidelines
Rev Bras Ter Intensiva. 2006;18(2):177-185
DOI 10.1590/S0103-507X2006000200011
Views1See moreBACKGROUND AND OBJECTIVES: New resuscitation guidelines contain significant changes intended to improve resuscitation practice and survival from cardiac arrest. This article provides an overview of the key changes on resuscitation for healthcare provider. CONTENTS: There are several new recommendations on cardiopulmonary resuscitation (CPR), the major are intended to provide good circulation during cardiac arrest. The most important change is the emphasis on high-quality chest compressions with minimal interruptions. The universal 30:2 ratio is recommended to simplify training, to achieve optimal compression rates and to reduce the frequency of interruptions. Only one shock is delivered when indicated, followed immediately by CPR. This shock should be of 120-200J on a biphasic wave or 360J on a monophasic wave. Rescuers should not interrupt chest compressions to check rhythm until after about 5 cycles or approximately 2 minutes of CPR. After this period, if an organized rhythm is present, the healthcare provider should check for a pulse. There are several little changes about the drugs administrated during CPR according to the rhythm. Given the lack of documented effect of drug therapy in improving long-term outcome from cardiac arrest, the sequence for CPR deemphasizes drug administration and reemphasizes basic life support. CONCLUSIONS: The update on the new resuscitation guidelines is important to improve the quality of resuscitation and achieve better survival rates from our critical care patients.
-
Sedation in intensive care unit: the use of remifentanil in clinical practice
Rev Bras Ter Intensiva. 2006;18(2):186-189
Abstract
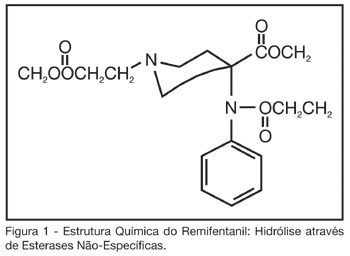
Sedation in intensive care unit: the use of remifentanil in clinical practice
Rev Bras Ter Intensiva. 2006;18(2):186-189
DOI 10.1590/S0103-507X2006000200012
Views0See moreBACKGROUND AND OBJECTIVES: Critically ill patients frequently need to use sedative and analgesic drugs, as part of their treatment or during several procedures. It is a challenge for all intensive care providers to determine the best drug to be used for each patient, with less collateral effects. The objective of this study is to describe the background to give the use of remifentanil in intensive care clinical practice. CONTENTS: Remifentanil is a short acting opioid agonist little used in intensive care medicine. Several studies have been published, showing that remifentanil is a safe drug to be used for the sedation and analgesia for intensive care patients, still needing more information regardless to septic shock patients. CONCLUSIONS: Because remifentanil is a relatively new drug, it is not yet part of the routine drugs used for intensive care providers, although solid evidences of its safety and efficiency for critically ill patients.
Views0Abstract
Sedation in intensive care unit: the use of remifentanil in clinical practice
Rev Bras Ter Intensiva. 2006;18(2):186-189
DOI 10.1590/S0103-507X2006000200012
Views0See moreBACKGROUND AND OBJECTIVES: Critically ill patients frequently need to use sedative and analgesic drugs, as part of their treatment or during several procedures. It is a challenge for all intensive care providers to determine the best drug to be used for each patient, with less collateral effects. The objective of this study is to describe the background to give the use of remifentanil in intensive care clinical practice. CONTENTS: Remifentanil is a short acting opioid agonist little used in intensive care medicine. Several studies have been published, showing that remifentanil is a safe drug to be used for the sedation and analgesia for intensive care patients, still needing more information regardless to septic shock patients. CONCLUSIONS: Because remifentanil is a relatively new drug, it is not yet part of the routine drugs used for intensive care providers, although solid evidences of its safety and efficiency for critically ill patients.
-
Delirium in the critically ill patient
Rev Bras Ter Intensiva. 2006;18(2):190-195
Abstract
Delirium in the critically ill patient
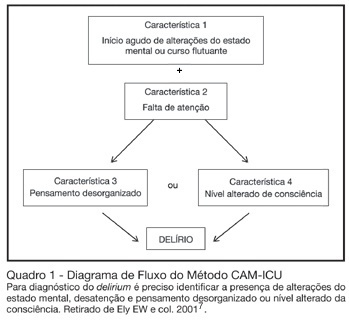
Rev Bras Ter Intensiva. 2006;18(2):190-195
DOI 10.1590/S0103-507X2006000200013
Views0See moreBACKGROUND AND OBJECTIVES: Delirium is a frequent finding in the critically ill patient. Although it is associated with increased morbidity and mortality, it is often not recognized by intensive care doctors. This review will address the main issues regarding delirium in critically ill patients. CONTENTS: Definition, incidence, mortality, risk factors, diagnosis, and treatment of delirium in the critically ill. CONCLUSIONS: Deliriumis defined as a disturbance of consciousness, attention, cognition and perception that occurs frequently in critically ill patients. It occurs in as many as 80% of mechanically ventilated ICU patients. Risk factors for delirium include acute systemic illnesses, older age, pre-existing cognitive impairment, sleep deprivation, and medications with anticholinergic activity. Although new assessment tools are available for rapidly and accurately measuring deliriumin critically ill patients, healthcare professionals still do not regularly monitor for this condition. In recent years, the emphasis in the approach to delirium has shifted to systematic screening and prevention. Haloperidol remains the standard treatment for delirium, but there is some evidence for the efficacy of risperidone.
Views0Abstract
Delirium in the critically ill patient
Rev Bras Ter Intensiva. 2006;18(2):190-195
DOI 10.1590/S0103-507X2006000200013
Views0See moreBACKGROUND AND OBJECTIVES: Delirium is a frequent finding in the critically ill patient. Although it is associated with increased morbidity and mortality, it is often not recognized by intensive care doctors. This review will address the main issues regarding delirium in critically ill patients. CONTENTS: Definition, incidence, mortality, risk factors, diagnosis, and treatment of delirium in the critically ill. CONCLUSIONS: Deliriumis defined as a disturbance of consciousness, attention, cognition and perception that occurs frequently in critically ill patients. It occurs in as many as 80% of mechanically ventilated ICU patients. Risk factors for delirium include acute systemic illnesses, older age, pre-existing cognitive impairment, sleep deprivation, and medications with anticholinergic activity. Although new assessment tools are available for rapidly and accurately measuring deliriumin critically ill patients, healthcare professionals still do not regularly monitor for this condition. In recent years, the emphasis in the approach to delirium has shifted to systematic screening and prevention. Haloperidol remains the standard treatment for delirium, but there is some evidence for the efficacy of risperidone.
-
Terlipressin as a new therapeutic agent in septic shock
Rev Bras Ter Intensiva. 2006;18(2):196-199
Abstract
Terlipressin as a new therapeutic agent in septic shock
Rev Bras Ter Intensiva. 2006;18(2):196-199
DOI 10.1590/S0103-507X2006000200014
Views0See moreBACKGROUND AND OBJECTIVES: The hemodynamic support of sepsis is now formulated trying to insert terlipressin as salvage drug in catecholamine resistant shock, justifying a broad critical analysis. CONTENTS: The analysis included hemodynamic therapies with defined specific goals and new recommendations for fluid resuscitation, vasopressor therapy, and inotropic therapy of septic in adult and pediatric patients. CONCLUSIONS: Terlipressin appears as a new but controversial alternative for vasopressor therapy in sepsis.
Views0Abstract
Terlipressin as a new therapeutic agent in septic shock
Rev Bras Ter Intensiva. 2006;18(2):196-199
DOI 10.1590/S0103-507X2006000200014
Views0See moreBACKGROUND AND OBJECTIVES: The hemodynamic support of sepsis is now formulated trying to insert terlipressin as salvage drug in catecholamine resistant shock, justifying a broad critical analysis. CONTENTS: The analysis included hemodynamic therapies with defined specific goals and new recommendations for fluid resuscitation, vasopressor therapy, and inotropic therapy of septic in adult and pediatric patients. CONCLUSIONS: Terlipressin appears as a new but controversial alternative for vasopressor therapy in sepsis.
-
Growth hormone therapy in pediatric hypercatabolic state: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2006;18(2):200-203
Abstract
Growth hormone therapy in pediatric hypercatabolic state: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2006;18(2):200-203
DOI 10.1590/S0103-507X2006000200015
Views0See moreBACKGROUND AND OBJECTIVES: To assess the use of recombinant human growth hormone (rhGH) in pediatric patients with hypercatabolic state in the pediatric intensive care unit. METHODS: We searched the databases of MedLine (1990 to 2005), LILACS (1990 to 2005), OVID (1990 to 2006) and EMBASE (1990 to 2005). Randomized controlled trials in pediatric patients using rhGH for hypercatabolic state (burns, sepsis) were selected. Intervention included rhGH therapy versus placebo. Data were extracted in duplicate and independently. Meta-analyses were performed using the software Review Manager statistic tools, with Mantel-Haenzel method for dichotomous outcomes and inverse variance method for continuous. RESULTS: There were evidences that rhGH in burned pediatric patients can reduce exogenous albumin requirement, with a improvement in Lean Body Mass, and accelerate site-donor wound healing, with no effects on mortality. Possibly can reduce the length of hospital stay. Hyperglycemia was the most frequently reported adverse event. CONCLUSIONS: This review suggests that the early application of rhGH to standard treatment in pediatric severe burned patients has the potential to improve some aspects from outcome. At this time, although the literature does not support routine rhGH for pediatric burn patients, consideration should be given to its use in this group, at least as an aim for further research. For use in septic patients, no proper statement can be done.
Views0Abstract
Growth hormone therapy in pediatric hypercatabolic state: a systematic review and meta-analysis
Rev Bras Ter Intensiva. 2006;18(2):200-203
DOI 10.1590/S0103-507X2006000200015
Views0See moreBACKGROUND AND OBJECTIVES: To assess the use of recombinant human growth hormone (rhGH) in pediatric patients with hypercatabolic state in the pediatric intensive care unit. METHODS: We searched the databases of MedLine (1990 to 2005), LILACS (1990 to 2005), OVID (1990 to 2006) and EMBASE (1990 to 2005). Randomized controlled trials in pediatric patients using rhGH for hypercatabolic state (burns, sepsis) were selected. Intervention included rhGH therapy versus placebo. Data were extracted in duplicate and independently. Meta-analyses were performed using the software Review Manager statistic tools, with Mantel-Haenzel method for dichotomous outcomes and inverse variance method for continuous. RESULTS: There were evidences that rhGH in burned pediatric patients can reduce exogenous albumin requirement, with a improvement in Lean Body Mass, and accelerate site-donor wound healing, with no effects on mortality. Possibly can reduce the length of hospital stay. Hyperglycemia was the most frequently reported adverse event. CONCLUSIONS: This review suggests that the early application of rhGH to standard treatment in pediatric severe burned patients has the potential to improve some aspects from outcome. At this time, although the literature does not support routine rhGH for pediatric burn patients, consideration should be given to its use in this group, at least as an aim for further research. For use in septic patients, no proper statement can be done.
-
Acute nitrogen intoxication by patient inhalation with breathing insufficiency and coma: case report
Rev Bras Ter Intensiva. 2006;18(2):204-206
Abstract
Acute nitrogen intoxication by patient inhalation with breathing insufficiency and coma: case report
Rev Bras Ter Intensiva. 2006;18(2):204-206
DOI 10.1590/S0103-507X2006000200016
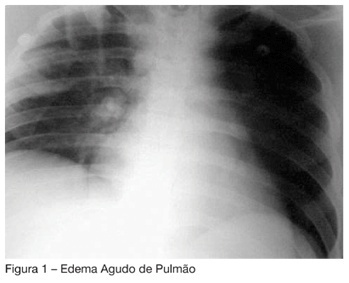
Views0See moreBACKGROUND AND OBJECTIVES: To present the first case reported in the Brazilian literature of liquid nitrogen intoxication. The objective of this report was to present a case of severe intoxication by liquid nitrogen, with acute lung edema and ischemic encephalopathy, which a good outcome, due to a fast diligence and a proper therapy administration. CASE REPORT: Male patient, 26 years, unconscious for one hour, in a close room with a machine to keep frozen the ice-roller ring. There was evidence of gastric aspiration and laryngeal edema. The intubation was difficult. The patient developed acute lung edema and brain edema due to hypoxia. There was a slow lung resolution with a protective ventilatory strategy for ARDS (VT 5 mL/kg, PEEP de 15 cmH2O) and corticotherapy with hydrocortisone (200 mg) every 6 h to treat bronchospasm. CONCLUSIONS: This the first case published in Brazil of nitrogen intoxication. In the international literature there are several reports of similar cases occurred in gymnasiums for hockey game. There are reports of bronchospasm exacerbations in people after the matches, even up to 10h after exposal to the gases riches in nitrogen.
Views0Abstract
Acute nitrogen intoxication by patient inhalation with breathing insufficiency and coma: case report
Rev Bras Ter Intensiva. 2006;18(2):204-206
DOI 10.1590/S0103-507X2006000200016
Views0See moreBACKGROUND AND OBJECTIVES: To present the first case reported in the Brazilian literature of liquid nitrogen intoxication. The objective of this report was to present a case of severe intoxication by liquid nitrogen, with acute lung edema and ischemic encephalopathy, which a good outcome, due to a fast diligence and a proper therapy administration. CASE REPORT: Male patient, 26 years, unconscious for one hour, in a close room with a machine to keep frozen the ice-roller ring. There was evidence of gastric aspiration and laryngeal edema. The intubation was difficult. The patient developed acute lung edema and brain edema due to hypoxia. There was a slow lung resolution with a protective ventilatory strategy for ARDS (VT 5 mL/kg, PEEP de 15 cmH2O) and corticotherapy with hydrocortisone (200 mg) every 6 h to treat bronchospasm. CONCLUSIONS: This the first case published in Brazil of nitrogen intoxication. In the international literature there are several reports of similar cases occurred in gymnasiums for hockey game. There are reports of bronchospasm exacerbations in people after the matches, even up to 10h after exposal to the gases riches in nitrogen.
-
Gastric rupture following cardiopulmonary resuscitation: case report
Rev Bras Ter Intensiva. 2006;18(2):207-211
Abstract
Gastric rupture following cardiopulmonary resuscitation: case report
Rev Bras Ter Intensiva. 2006;18(2):207-211
DOI 10.1590/S0103-507X2006000200017
Views0See moreBACKGROUND AND OBJECTIVES: Gastric rupture is a rare complication from cardiopulmonary resuscitation (CPR), with a reported incidence of 0.1%. Unawareness of this possible complication during these maneuvers delays its recognition and reduces the patient’s surviving chance. The aim of this report is to describe a case of acute abdomen due to gastric rupture following CPR maneuvers that was promptly diagnosed and treated. CASE REPORT: We report a case of a 76-year-old patient that was admitted to the hospital with pneumonia and also to rule out a possible brain vascular accident (BVA). In the first day after admission she developed acute respiratory failure and cardiac arrest, being successfully resuscitated and subsequently transferred to the intensive care unit (ICU) by the medical ward team. Despite successful CPR, adequate volume resuscitation, vasopressor support and respiratory function improvement she remained with significant hemodynamic instability. Physical examination hours after CPR showed a hypertimpanic liver percussion, abdominal distension, tachycardia and hypotension. Chest X-Ray revealed pneumoperitoneum, and gastric perforation was identified by an exploratory laparotomy. Histopathology confirmed traumatic gastric injury. CONCLUSIONS: We report a rare case of traumatic gastric rupture after CPR maneuvers in which prompt diagnosis and emergent treatment lead to a favorable outcome. This case brings out the need to increase awareness of this life-threatening complication with emphasis on the importance of a thorough physical examination after CPR maneuvers. Reinforcement of appropriate CPR technique is crucial to avoid incorrect maneuvers through continued medical education.
Views0Abstract
Gastric rupture following cardiopulmonary resuscitation: case report
Rev Bras Ter Intensiva. 2006;18(2):207-211
DOI 10.1590/S0103-507X2006000200017
Views0See moreBACKGROUND AND OBJECTIVES: Gastric rupture is a rare complication from cardiopulmonary resuscitation (CPR), with a reported incidence of 0.1%. Unawareness of this possible complication during these maneuvers delays its recognition and reduces the patient’s surviving chance. The aim of this report is to describe a case of acute abdomen due to gastric rupture following CPR maneuvers that was promptly diagnosed and treated. CASE REPORT: We report a case of a 76-year-old patient that was admitted to the hospital with pneumonia and also to rule out a possible brain vascular accident (BVA). In the first day after admission she developed acute respiratory failure and cardiac arrest, being successfully resuscitated and subsequently transferred to the intensive care unit (ICU) by the medical ward team. Despite successful CPR, adequate volume resuscitation, vasopressor support and respiratory function improvement she remained with significant hemodynamic instability. Physical examination hours after CPR showed a hypertimpanic liver percussion, abdominal distension, tachycardia and hypotension. Chest X-Ray revealed pneumoperitoneum, and gastric perforation was identified by an exploratory laparotomy. Histopathology confirmed traumatic gastric injury. CONCLUSIONS: We report a rare case of traumatic gastric rupture after CPR maneuvers in which prompt diagnosis and emergent treatment lead to a favorable outcome. This case brings out the need to increase awareness of this life-threatening complication with emphasis on the importance of a thorough physical examination after CPR maneuvers. Reinforcement of appropriate CPR technique is crucial to avoid incorrect maneuvers through continued medical education.

-
Erratas
Rev Bras Ter Intensiva. 2006;18(2):212-212
Abstract
Erratas
Rev Bras Ter Intensiva. 2006;18(2):212-212
DOI 10.1590/S0103-507X2006000200018
Views0ERRATAS No artigo “Sepse Brasil: Estudo Epidemiológico da Sepse em Unidades de Terapia Intensiva Brasileiras” publicado na RBTI, 2006;18:9-17, houve uma inversão dos nomes dos autores na capa e no sumário.[…]See moreViews0Abstract
Erratas
Rev Bras Ter Intensiva. 2006;18(2):212-212
DOI 10.1590/S0103-507X2006000200018
Views0ERRATAS No artigo “Sepse Brasil: Estudo Epidemiológico da Sepse em Unidades de Terapia Intensiva Brasileiras” publicado na RBTI, 2006;18:9-17, houve uma inversão dos nomes dos autores na capa e no sumário.[…]See more
Volume Articles - Critical Care Science (CCS)
