
You searched for:"Márcio Soares"
We found (32) results for your search.-
Review Articles
The importance of delirium monitoring in the intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):274-279
Abstract
Review ArticlesThe importance of delirium monitoring in the intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):274-279
DOI 10.1590/S0103-507X2010000300010
Views0See moreDelirium is an acute confusional state associated with increased mortality in the intensive care unit and long-term impaired functional recovery. Despite its elevated incidence and major impact in the outcomes of critically ill patients, delirium remains under-diagnosed. Presently, there are validated instruments to diagnose and monitor delirium, allowing the detection of early organ dysfunction and treatment initiation. Beyond patient’s non-modifiable risk factors, there are modifiable clinical and environmental aspects that should be accessed to reduce the occurrence and severity of delirium. As recent studies demonstrate that interventions aiming to reduce sedative exposure and to improve patients’ orientation associated with early mobility have proved to reduce delirium, a low incidence of delirium should be targeted and considered as a measure of quality of care in the intensive care unit (ICU).
Views0

Abstract
Review ArticlesThe importance of delirium monitoring in the intensive care unit
Rev Bras Ter Intensiva. 2010;22(3):274-279
DOI 10.1590/S0103-507X2010000300010
Views0See moreDelirium is an acute confusional state associated with increased mortality in the intensive care unit and long-term impaired functional recovery. Despite its elevated incidence and major impact in the outcomes of critically ill patients, delirium remains under-diagnosed. Presently, there are validated instruments to diagnose and monitor delirium, allowing the detection of early organ dysfunction and treatment initiation. Beyond patient’s non-modifiable risk factors, there are modifiable clinical and environmental aspects that should be accessed to reduce the occurrence and severity of delirium. As recent studies demonstrate that interventions aiming to reduce sedative exposure and to improve patients’ orientation associated with early mobility have proved to reduce delirium, a low incidence of delirium should be targeted and considered as a measure of quality of care in the intensive care unit (ICU).
-
Original Articles
Outcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
Abstract
Original ArticlesOutcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
Views0See moreOBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
Views0Abstract
Original ArticlesOutcome of patients with cirrhosis admitted to intensive care
Rev Bras Ter Intensiva. 2010;22(1):11-18
DOI 10.1590/S0103-507X2010000100004
Views0See moreOBJECTIVE: This study aimed to evaluate the outcome of cirrhotic patients admitted to Intensive Care Unit. METHODS: We conducted a prospective cohort of cirrhotic patients admitted to two intensive care unit between June 1999 to September 2004. We collected demographic, comorbid conditions, diagnosis, vital signs, laboratory data, prognostic scores and evolution in intensive care unit and hospital. The patients were divided in groups: non surgical, non liver surgery, surgery for portal hypertension, liver surgery, liver transplantation, and urgent surgery. RESULTS: We studied 304 patients, which 190 (62.5%) were male. The median of age was 54 (47-61) years. The mortality rate in intensive care unit and hospital were 29.3 and 39.8%, respectively, more elevated than in the other patients admitted critically ill patients (19.6 and 28.3%; p<0.001). Non surgical patients and those submitted to urgent surgery presented high mortality rate in the intensive care unit (64.3 and 65.4%) and in the hospital (80.4 and 76.9%). The variables related to hospital mortality were [Odds ratio (confidence interval 95%)]: mean arterial pressure [0.985 (0.974-0.997)]; mechanical ventilation in the first 24 h [4.080 (1.990-8.364)]; confirmed infection in the first 24 h [7.899 (2.814-22.175)]; acute renal failure [5.509 (1.708-17.766)] and APACHE II score (points) [1.078 (1.017-1.143)]. CONCLUSIONS: Cirrhotic patients had higher mortality rate compared to non cirrhotic critically ill patients. Those admitted after urgent surgery and non surgical had higher mortality rate.
-
Review Articles
Understanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
Views0A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Keywords:Intensive careMultiple organ failureOutcome and process assessmentPrognosisRisk assessmentSepsisSee moreViews0Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – part 2
Rev Bras Ter Intensiva. 2010;22(1):64-68
DOI 10.1590/S0103-507X2010000100011
Views0A sepsis staging system focused on predisposition, insult, host response and organ failure may provide a useful basis for risk stratification. Knowledge on interactions among predisposing factors, insult characteristics and host response might help us to improve our understanding on sepsis pathophysiology and allow more individual therapeutic approach. Recent clinical studies documented the clinical importance of PIRO approach for severity stratification in septic patients in intensive care unit, and also for specific conditions such as community acquired pneumonia and ventilator associated pneumonia , with a good performance for outcome prediction. In this review we describe how this new concept can be used in clinical practice and provide some insights on its usefulness to facilitate the stratification and potential for enrollment in clinical trials of sepsis therapies.
Keywords:Intensive careMultiple organ failureOutcome and process assessmentPrognosisRisk assessmentSepsisSee more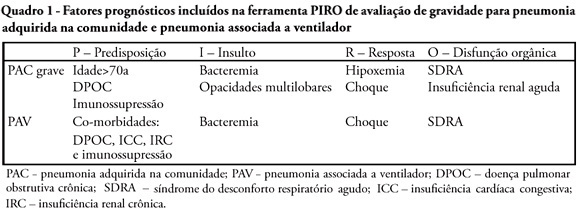
-
Review Articles
Understanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
DOI 10.1590/S0103-507X2009000400013
Views0Despite recent advances in diagnosis and care of critically ill patients sepsis related mortality rate remains unacceptably high. Therefore, new methods of evaluation are necessary to provide an earlier and more accurate characterization of septic patients. Based on the (oncologic) TNM system, the PIRO concept was introduced as a new staging system for sepsis in order to assess risk and predict prognosis, with potential to assist in inclusion of patients in clinical studies and estimate the probability of response of patients to specific therapeutic interventions.
Keywords:Intensive careMultiple organ failureOutcome and process assessment (Health Care)PrognosisRisk assessmentSepsisSee moreViews0Abstract
Review ArticlesUnderstanding the PIRO concept: from theory to clinical practice – Part 1
Rev Bras Ter Intensiva. 2009;21(4):425-431
DOI 10.1590/S0103-507X2009000400013
Views0Despite recent advances in diagnosis and care of critically ill patients sepsis related mortality rate remains unacceptably high. Therefore, new methods of evaluation are necessary to provide an earlier and more accurate characterization of septic patients. Based on the (oncologic) TNM system, the PIRO concept was introduced as a new staging system for sepsis in order to assess risk and predict prognosis, with potential to assist in inclusion of patients in clinical studies and estimate the probability of response of patients to specific therapeutic interventions.
Keywords:Intensive careMultiple organ failureOutcome and process assessment (Health Care)PrognosisRisk assessmentSepsisSee more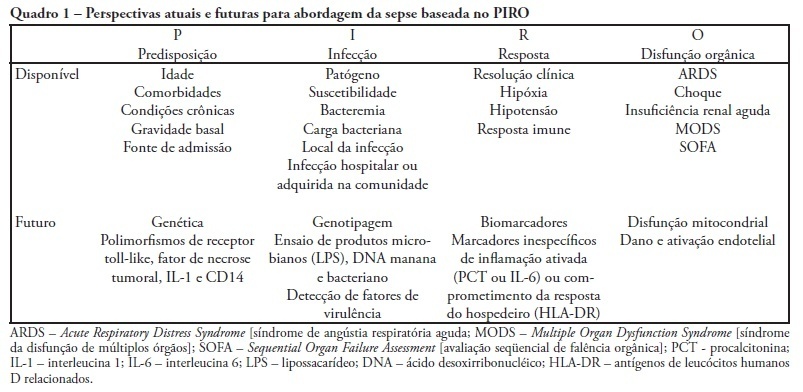
-
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
Abstract
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
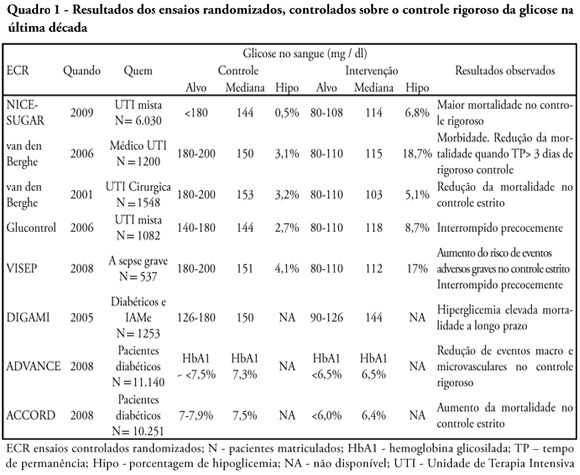
Views0See moreGlucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient’s safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
Views0Abstract
Glucose control in critically ill patients in 2009: no alarms and no surprises
Rev Bras Ter Intensiva. 2009;21(3):310-314
DOI 10.1590/S0103-507X2009000300012
Views0See moreGlucose control is a major issue in critical care since landmark publications from the last decade leading to widespread use of strict glucose control in the clinical practice. Subsequent trials showed discordant results that lead to several questions and concerns about benefits and risks of implementing an intensive glucose control protocol. In the midst of all recent controversy, we propose that a new glycemic target -150mg/dl) should be aimed. This target glucose level could offer protection against the deleterious effects of hyperglycemia and at the same time keep patient’s safety avoiding hypoglicemia. The article presents a critical review of the current literature on intensive insulin therapy in critically ill patients.
-
Letters to the Editor
Drotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
DOI 10.1590/S0103-507X2008000300018
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See moreViews0Abstract
Letters to the EditorDrotrecogin alfa (activated) in clinical practice and current evidences: reply
Rev Bras Ter Intensiva. 2008;20(3):323-324
DOI 10.1590/S0103-507X2008000300018
Views0LETTER TO THE EDITOR Drotrecogin alfa (activated) in clinical practice and current evidences[…]See more -
Review Articles
Drotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
Abstract
Review ArticlesDrotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
Views0See moreBACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
Views0Abstract
Review ArticlesDrotrecogin alfa activated in clinical practice and the current evidences
Rev Bras Ter Intensiva. 2008;20(2):173-177
DOI 10.1590/S0103-507X2008000200010
Views0See moreBACKGROUND AND OBJECTIVES: The debate on efficacy and patient safety related to the use of drotrecogin alfa (DrotAA) is timely, principally due to the negative results observed in clinical studies performed after the PROWESS study, and the economic cost-related impact of the drug on the healthcare system. The aim of this study was to review the main studies on the use of DrotAA in patients with severe sepsis. The focus was on drug efficacy-and patient safety-related issues. CONTENTS: Articles were selected by a MedLine search for studies on the use of DrotAA in patients with sepsis using the following key words: activated protein C; drotrecogin alfa; sepsis; septic shock; Xigris®. Additional references were retrieved from the studies initially selected. CONCLUSIONS: Mortality and bleeding complications associated with the use of DrotAA were more frequent in large observational studies than those reported in randomized trials. In the light of the current knowledge, routine use of DrotAA should be reevaluated until well-designed confirmatory clinical trials can clarify the true efficacy and safety of the drug and help identify the subgroup of patients that can benefit from use of DrotAA. Physicians should be cautious with the rapid transfer of evidences not well-documented, to the guidelines and recommendations practiced in the care and treatment of patients with severe sepsis.
-
Original Articles
Performance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
Abstract
Original ArticlesPerformance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
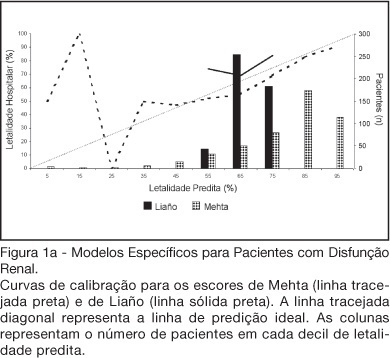
Views0See moreBACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Views0Abstract
Original ArticlesPerformance of six prognostic scores in critically ILL patients receiving renal replacement therapy
Rev Bras Ter Intensiva. 2008;20(2):115-123
DOI 10.1590/S0103-507X2008000200001
Views0See moreBACKGROUND AND OBJECTIVES: There is no consensus about prognostic scores for use in patients with acute kidney injury (AKI). The aim of this study was to evaluate the performance of six prognostic scores in predicting hospital mortality in patients with AKI and need for renal replacement therapy (RRT). METHODS: Prospective cohort of patients admitted to the intensive care units (ICU) of three tertiary care hospitals that required RRT for AKI over a 32-month period. Patients with end-stage renal disease and those with ICU stay < 24h were excluded. Data from the first 24h of ICU admission were used to calculate SAPS II and APACHE II scores, and data from the first 24h of RRT were used in the calculation of LOD, ODIN, Liaño and Mehta scores. Discrimination was evaluated using the area under ROC curve (AUROC) and calibration using the Hosmer-Lemeshow goodness-of-fit test. The hospital mortality was the end-point of interest. RESULTS: 467 patients were evaluated. Hospital mortality rate was 75%. Mean SAPS II and APACHE II scores were 48.5 ±11.2 and 27.4 ± 6.3 points, and median LOD score was 7 (5-8) points. Except for Mehta score (p = 0.001), calibration was appropriate in all models. However, discrimination was uniformly unsatisfactory; AUROC ranged from 0.60 for ODIN to 0.72 for SAPS II and Mehta scores. In addition, except for Mehta, all models tended to underestimate hospital mortality. CONCLUSIONS: Organ dysfunction, general and renal-specific severity-of-illness scores were inaccurate in predicting outcome in ICU patients in need for RRT.
Search
Search in:
KEY WORDS
Case reports Child Coronavirus infections COVID-19 Critical care Critical illness Extracorporeal membrane oxygenation Infant, newborn Intensive care Intensive care units Intensive care units, pediatric mechanical ventilation Mortality Physical therapy modalities Prognosis Respiration, artificial Respiratory insufficiency risk factors SARS-CoV-2 Sepsis