Shock, septic Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(4):392-396
DOI 10.5935/0103-507X.20140060
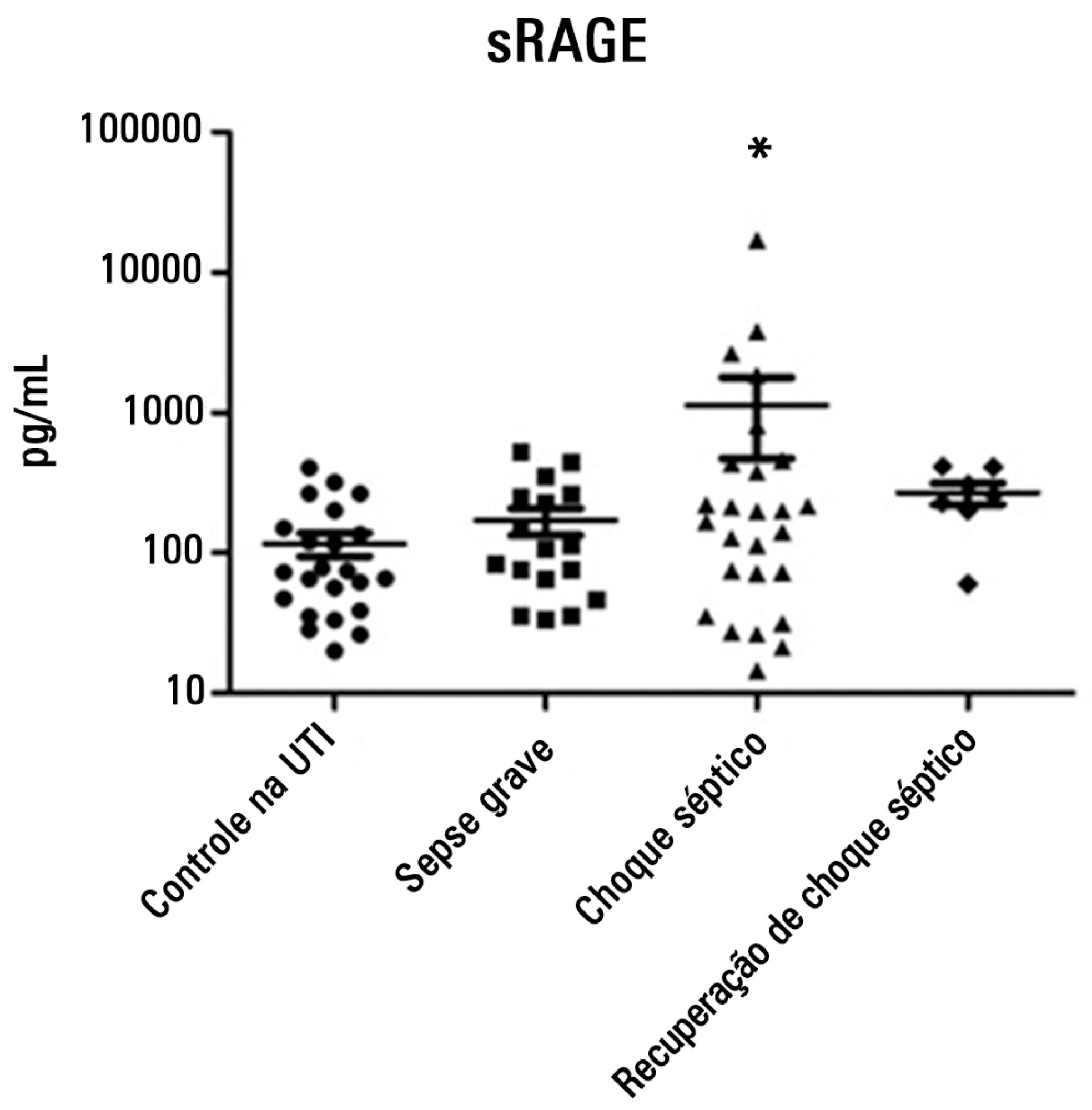
To evaluate and understand the clinical implications of the plasma levels of a soluble isoform of a receptor for advanced glycation end products (sRAGE) in different stages of sepsis.
Serum sRAGE values in patients who were divided into intensive care unit control, severe sepsis, septic shock and recovery from septic shock groups were statistically analyzed to assess quantity (Kruskal-Wallis), variability (Levine test) and correlation (Spearman rank test) with certain inflammatory mediators (IL-1 α, IL-6, IL-8, IL-10, IP-10, G-CSF, MCP-1, IFN-γ and TNF-α).
No changes in sRAGE levels were observed among the groups; however, the septic shock group showed differences in the variability of sRAGE compared to the other groups. A positive correlation with all the inflammatory mediators was reported in the septic shock group.
sRAGE levels are associated with worse outcomes in patients with septic shock. However, a statistical correlation analysis with other proinflammatory cytokines indicated that the pathways leading to those outcomes are different depending on the sRAGE levels. Future studies to elucidate the pathophysiological mechanisms involving sRAGE in models of sepsis are of great clinical importance for the safe handling of this biomarker.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):392-396
DOI 10.5935/0103-507X.20140060
To evaluate and understand the clinical implications of the plasma levels of a soluble isoform of a receptor for advanced glycation end products (sRAGE) in different stages of sepsis.
Serum sRAGE values in patients who were divided into intensive care unit control, severe sepsis, septic shock and recovery from septic shock groups were statistically analyzed to assess quantity (Kruskal-Wallis), variability (Levine test) and correlation (Spearman rank test) with certain inflammatory mediators (IL-1 α, IL-6, IL-8, IL-10, IP-10, G-CSF, MCP-1, IFN-γ and TNF-α).
No changes in sRAGE levels were observed among the groups; however, the septic shock group showed differences in the variability of sRAGE compared to the other groups. A positive correlation with all the inflammatory mediators was reported in the septic shock group.
sRAGE levels are associated with worse outcomes in patients with septic shock. However, a statistical correlation analysis with other proinflammatory cytokines indicated that the pathways leading to those outcomes are different depending on the sRAGE levels. Future studies to elucidate the pathophysiological mechanisms involving sRAGE in models of sepsis are of great clinical importance for the safe handling of this biomarker.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
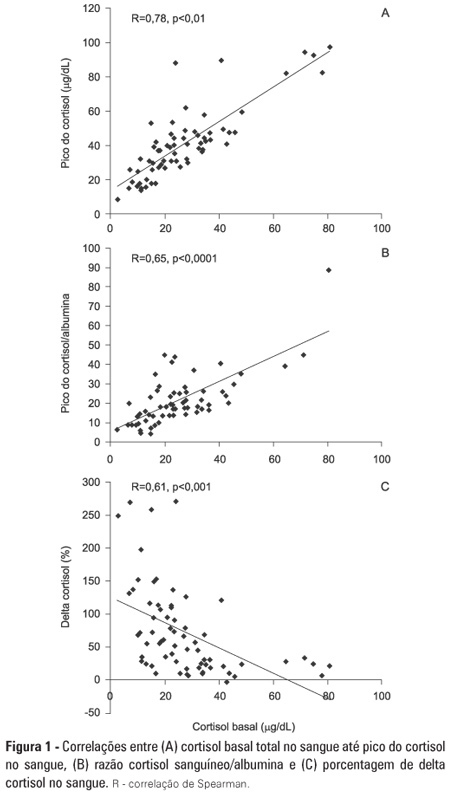
OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Abstract
Rev Bras Ter Intensiva. 2012;24(4):362-368
DOI 10.1590/S0103-507X2012000400012
OBJECTIVE: To evaluate if cortisol responses to 250 µg of intravenously administered adrenocorticotropic hormone are related to disease severity and, hence, mortality. METHODS: This is a retrospective study in a medical-surgical intensive care unit of a university hospital. We studied 69 consecutive patients with septic shock over a 1-yr period; these patients underwent a short 250-µg adrenocorticotropic hormone test because they exhibited >6 hours of progressive hemodynamic instability requiring repeated fluid challenges and vasopressor treatment to maintain blood pressure. The test was performed by intravenously injecting 250 µg of synthetic adrenocorticotropic hormone and measuring cortisol immediately before injection, 30 minutes post-injection and 60 minutes post-injection. RESULTS: The mean APACHE II score was 22±7. The intensive care unit mortality rate at day 28 was 55%. Median baseline cortisol levels (19 [11-27] µg/dL versus 24 [18-34] µg/dL, p=0.047) and median baseline cortisol/albumin ratios (7.6 [4.6-12.3] versus 13.9 [8.8-18.5]; p=0.01) were lower in survivors than in non-survivors. Responders and non-responders had similar baseline clinical data and outcomes. The variables that were significantly correlated with outcome based on the area under the ROC curves (AUC) were APACHE II (AUC=0.67 [0.535 to 0.781]), baseline cortisol (µg/dl) (AUC=0.662 [0.536 to 0.773], peak cortisol (µg/dl) (AUC=0.642 [0.515 to 0.755]) and baseline cortisol/albumin (AUC=0.75 [0.621 to 0.849]). CONCLUSIONS: Increased basal cortisol is associated with mortality and disease severity. Cortisol responses upon adrenocorticotropic hormone stimulation were not related to outcome. The cortisol/albumin ratio does not predict unfavorable outcomes better than total cortisol levels or help to improve the accuracy of the adrenocorticotropic hormone test.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
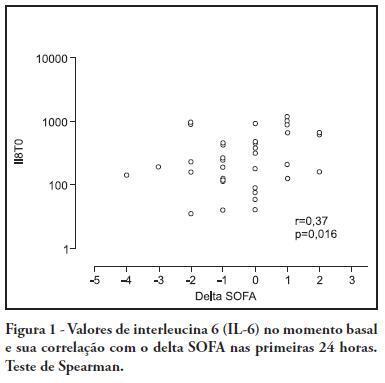
OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Abstract
Rev Bras Ter Intensiva. 2011;23(4):426-433
DOI 10.1590/S0103-507X2011000400006
OBJECTIVE: To investigate the correlation of organ dysfunction and its progression with inflammatory response during the early phases of septic shock by assessing baseline cytokine concentrations. METHODS: This study included patients over 18 years old with septic shock within the first 48 hours after the onset of organ dysfunction. Interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10) and C-reactive protein levels were assessed at inclusion and after 24 hours, and the differences between these values were calculated. The progression of organ dysfunction was assessed using the Sequential Organ Failure Assessment (SOFA) score upon admission and 24 hours later for a delta-SOFA determination and were categorized as either worsened or improved. The results were expressed as means + standard deviation or median (25-75% percentiles). Values with descriptive p values of 0.05 or less were considered significant. RESULTS: Overall, we included 41 patients with median SOFA scores of 8.0 (6.5-10.0) upon admission (T0) and 8.0 (6.0-10.0) 24 hours later (T1). Worsened, improved or unchanged SOFA scores were observed in 11 (Group 1), 17 (Group 2) and 13 (Group 3) patients, respectively. For Group 1, the baseline IL-6, IL-8 and IL-10 values were higher, and a significant increase of IL-8 levels was found after 24 hours. The change in the SOFA score after 24 hours was significantly, although weakly, correlated with baseline IL-6 and IL-8 concentrations. CONCLUSIONS: Higher baseline IL-6, IL-8 and IL-10 levels are associated with unfavorable organ dysfunction outcomes. Increased IL-8 levels within the first 24 hours are correlated with a worsening dysfunction.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):403-412
DOI 10.1590/S0103-507X2010000400015
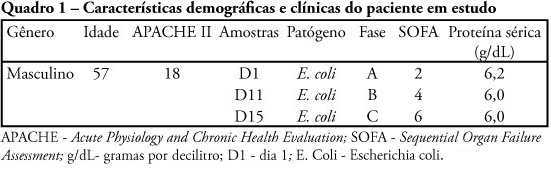
Gene expression is disrupted by sepsis. Genetic markers can only reveal a patient's genotype, and they are not affected by environmental biological processes. These processes are expressed by proteins. This study was aimed to advance the insight into the molecular foundations of sepsis. It employed proteomic techniques to identify and analyze differential serum protein expressions taken from a patient throughout the stages of sepsis (sepsis, severe sepsis and septic shock). Serum samples were collected at each stage of sepsis and submitted to one-dimensional electrophoresis, on gradient strips of immobilized pH, followed by two-dimensional 12.5% polyacrylamide gel electrophoresis. The gels obtained were stained, scanned and analyzed by the ImageMasterPlatinum program. Proteins that were differentially expressed in the gels were excised, digested with trypsin and identified through mass spectrometry. Fourteen differentially expressed proteins were identified throughout the stages of sepsis, as well as a protein that was not expressed in all stages, suggesting the potential existence of a biomarker. The differentially expressed proteins identified were: serum amyloid A, apolipoprotein A-1 (2 isoforms), zinc finger protein 222, human albumin, PRO 2619, immunoglobulin kappa light chain VLJ region, monoclonal immunoglobulin M cold agglutinin, 7 proteinase inhibitors - alpha-1 antitrypsin. The findings of this pilot study demonstrate the involvement of the complement and coagulation pathways, of the lipid metabolism and of genetic information in sepsis. The vast majority of proteins identified are involved in the immune system and the proteinase inhibitor proteins are predominant.
Abstract
Rev Bras Ter Intensiva. 2010;22(4):403-412
DOI 10.1590/S0103-507X2010000400015
Gene expression is disrupted by sepsis. Genetic markers can only reveal a patient's genotype, and they are not affected by environmental biological processes. These processes are expressed by proteins. This study was aimed to advance the insight into the molecular foundations of sepsis. It employed proteomic techniques to identify and analyze differential serum protein expressions taken from a patient throughout the stages of sepsis (sepsis, severe sepsis and septic shock). Serum samples were collected at each stage of sepsis and submitted to one-dimensional electrophoresis, on gradient strips of immobilized pH, followed by two-dimensional 12.5% polyacrylamide gel electrophoresis. The gels obtained were stained, scanned and analyzed by the ImageMasterPlatinum program. Proteins that were differentially expressed in the gels were excised, digested with trypsin and identified through mass spectrometry. Fourteen differentially expressed proteins were identified throughout the stages of sepsis, as well as a protein that was not expressed in all stages, suggesting the potential existence of a biomarker. The differentially expressed proteins identified were: serum amyloid A, apolipoprotein A-1 (2 isoforms), zinc finger protein 222, human albumin, PRO 2619, immunoglobulin kappa light chain VLJ region, monoclonal immunoglobulin M cold agglutinin, 7 proteinase inhibitors - alpha-1 antitrypsin. The findings of this pilot study demonstrate the involvement of the complement and coagulation pathways, of the lipid metabolism and of genetic information in sepsis. The vast majority of proteins identified are involved in the immune system and the proteinase inhibitor proteins are predominant.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):280-290
DOI 10.1590/S0103-507X2010000300011
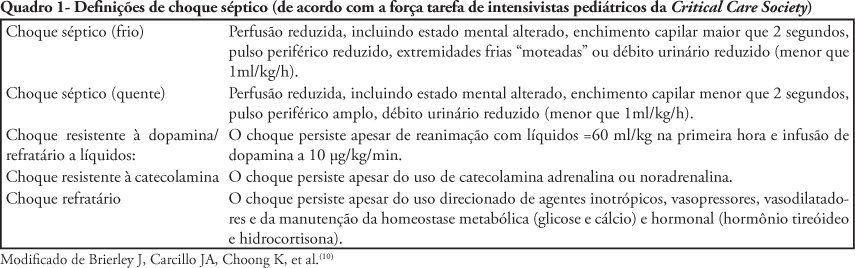
The nonspecific presentation of neonatal sepsis and systemic inflammatory response syndrome preceding septic shock delay the early diagnosis of septic shock and increase its mortality rate. Early diagnosis involves suspecting septic shock in every newborn with tachycardia, respiratory distress, difficult feeding, altered tonus and skin coloration, tachypnea and reduced perfusion, specially in case of maternal peripartum infection, chorioamnionitis or long-term membranes rupture. This article aims to review current knowledge on neonatal period peculiarities, fetal circulation dynamics, and the pregnancy age variable. Newborn septic shock is not just a small adult shock. In the newborn, the septic shock is predominantly cold and characterized by reduced cardiac output and increased systemic vascular resistance (vasoconstriction). Time is fundamental for septic shock reversion. The indexed-databases literature review provides subside for the newborn management.
Abstract
Rev Bras Ter Intensiva. 2010;22(3):280-290
DOI 10.1590/S0103-507X2010000300011
The nonspecific presentation of neonatal sepsis and systemic inflammatory response syndrome preceding septic shock delay the early diagnosis of septic shock and increase its mortality rate. Early diagnosis involves suspecting septic shock in every newborn with tachycardia, respiratory distress, difficult feeding, altered tonus and skin coloration, tachypnea and reduced perfusion, specially in case of maternal peripartum infection, chorioamnionitis or long-term membranes rupture. This article aims to review current knowledge on neonatal period peculiarities, fetal circulation dynamics, and the pregnancy age variable. Newborn septic shock is not just a small adult shock. In the newborn, the septic shock is predominantly cold and characterized by reduced cardiac output and increased systemic vascular resistance (vasoconstriction). Time is fundamental for septic shock reversion. The indexed-databases literature review provides subside for the newborn management.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):113-123
DOI 10.1590/S0103-507X2009000200001
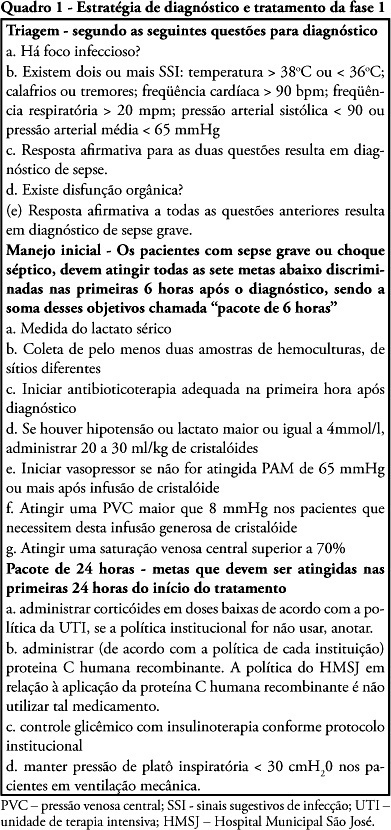
OBJECTIVE: To evaluate the impact of implementing an institutional policy for detection of severe sepsis and septic shock. METHODS: Study before (stage I), after (stage II) with prospective data collection in a 195 bed public hospital.. Stage I: Patients with severe sepsis or septic shock were included consecutively over 15 months and treated according to the Surviving Sepsis Campaign guidelines. Stage II: In the 10 subsequent months, patients with severe sepsis or septic shock were enrolled based on an active search for signs suggesting infection (SSI) in hospitalized patients. The two stages were compared for demographic variables, time needed for recognition of at least two signs suggesting infection (SSI-Δt), compliance to the bundles of 6 and 24 hours and mortality. RESULTS: We identified 124 patients with severe sepsis or septic shock, 68 in stage I and 56 in stage II. The demographic variables were similar in both stages. The Δt-SSI was 34 ± 54 hours in stage I and 7 ± 8.4 hours in stage II (p <0.001). There was no difference in compliance to the bundles. In parallel there was significant reduction of mortality rates at 28 days (54.4% versus 30%, p <0.02) and hospital (67.6% versus 41%, p <0.003). CONCLUSION: The strategy used helped to identify early risk of sepsis and resulted in decreased mortality associated with severe sepsis and septic shock.
Abstract
Rev Bras Ter Intensiva. 2009;21(2):113-123
DOI 10.1590/S0103-507X2009000200001
OBJECTIVE: To evaluate the impact of implementing an institutional policy for detection of severe sepsis and septic shock. METHODS: Study before (stage I), after (stage II) with prospective data collection in a 195 bed public hospital.. Stage I: Patients with severe sepsis or septic shock were included consecutively over 15 months and treated according to the Surviving Sepsis Campaign guidelines. Stage II: In the 10 subsequent months, patients with severe sepsis or septic shock were enrolled based on an active search for signs suggesting infection (SSI) in hospitalized patients. The two stages were compared for demographic variables, time needed for recognition of at least two signs suggesting infection (SSI-Δt), compliance to the bundles of 6 and 24 hours and mortality. RESULTS: We identified 124 patients with severe sepsis or septic shock, 68 in stage I and 56 in stage II. The demographic variables were similar in both stages. The Δt-SSI was 34 ± 54 hours in stage I and 7 ± 8.4 hours in stage II (p <0.001). There was no difference in compliance to the bundles. In parallel there was significant reduction of mortality rates at 28 days (54.4% versus 30%, p <0.02) and hospital (67.6% versus 41%, p <0.003). CONCLUSION: The strategy used helped to identify early risk of sepsis and resulted in decreased mortality associated with severe sepsis and septic shock.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):267-277
DOI 10.1590/S0103-507X2008000300010
The present review discusses the hemodynamic and immune-modulatory effects of hypertonic saline in experimental shock and in patients with sepsis. We comment on the mechanisms of action of hypertonic saline, calling upon data in hemorrhagic and septic shock. Specific actions of hypertonic saline applicable to severe sepsis and septic shock are highlighted. Data available support potential benefits of hypertonic saline infusion in various aspects of the pathophysiology of sepsis, including tissue hypoperfusion, decreased oxygen consumption, endothelial dysfunction, cardiac depression, and the presence of a broad array of pro-inflammatory cytokines and various oxidant species. A therapy that simultaneously blocks the damaging components of sepsis will have an impact on the management of sepsis. Proper designed prospective studies may prove a beneficial role for hypertonic saline solution in the future.