SARS-CoV-2 Archives - Critical Care Science (CCS)

Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
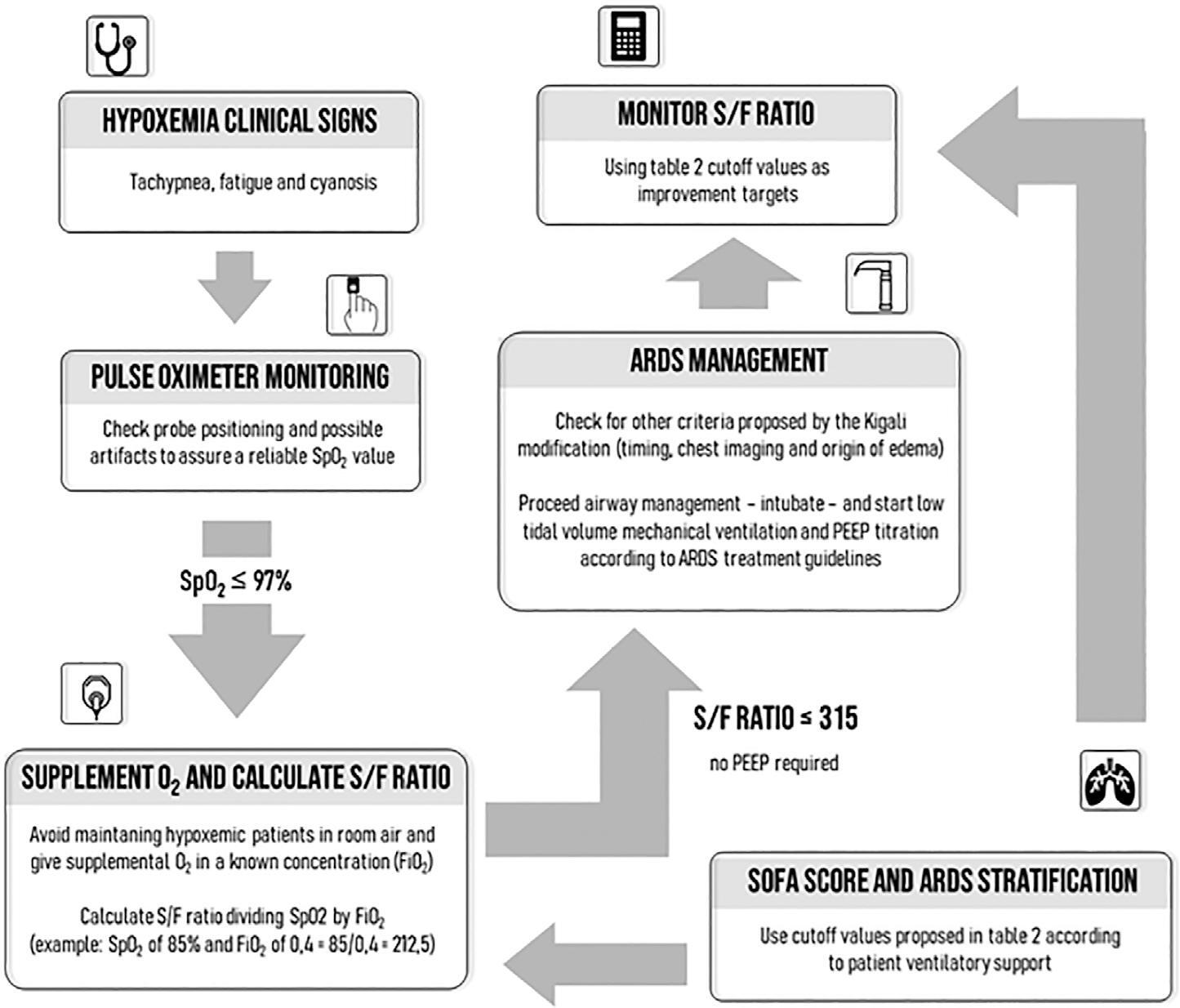
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Revista Brasileira de Terapia Intensiva. 2022;34(1):185-196
DOI 10.5935/0103-507X.20220013-en
Although the PaO 2/FiO 2 derived from arterial blood gas analysis remains the gold standard for the diagnosis of acute respiratory failure, the SpO2/FiO2 has been investigated as a potential substitute. The current narrative review presents the state of the preclinical and clinical literature on the SpO2/FiO2 as a possible substitute for PaO2/FiO2 and for use as a diagnostic and prognostic marker; provides an overview of pulse oximetry and its limitations, and assesses the utility of SpO2/ FiO2 as a surrogate for PaO2/FiO2 in COVID-19 patients. Overall, 49 studies comparing SpO2/FiO2 and PaO2/FiO2 were found according to a minimal search strategy. Most were conducted on neonates, some were conducted on adults with acute respiratory distress syndrome, and a few were conducted in other clinical scenarios (including a very few on COVID-19 patients). There is some evidence that the SpO2/ FiO2 criteria can be a surrogate for PaO2/FiO2 in different clinical scenarios. This is reinforced by the fact that unnecessary invasive procedures should be avoided in patients with acute respiratory failure. It is undeniable that pulse oximeters are becoming increasingly widespread and can provide costless monitoring. Hence, replacing PaO2/FiO2 with SpO2/FiO2may allow resourcelimited facilities to objectively diagnose acute respiratory failure.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):487-536
DOI 10.5935/0103-507X.0103-507X-rbti-20210080
The Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group have previously issued health service and management recommendations for critically ill patients with COVID-19. Due to the evolution of knowledge, the panel of experts was again convened to review the current evidence and issue updated recommendations.
A national panel of experts who declared that they had no conflicts of interest regarding the development of the recommendations was assembled. Operational questions were developed based on the PICO methodology, and a rapid systematic review was conducted by consulting different bibliographic sources. The panel determined the direction and strength of the recommendations using two Delphi rounds, conducted in accordance with the principles of the GRADE system. A strong recommendation received the wording “is recommended”, and a weak recommendation was written as “is suggested.”
A total of 48 recommendations and 30 suggestions were issued, covering the following topics: diagnosis of SARS-CoV-2 infection, coinfection and superinfection; criteria for admission, cure and suspension of isolation; organization of services; personal protective equipment; and respiratory support and other specific therapies (antivirals, immunomodulators and anticoagulation).
These recommendations, specifically oriented to the Portuguese reality but that may also apply to Portuguese-speaking African countries and East Timor, aim to support health professionals in the management of critically ill patients with COVID-19. They will be continuously reviewed to reflect the progress of our understanding and the treatment of this pathology.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(4):487-536
DOI 10.5935/0103-507X.0103-507X-rbti-20210080
The Sociedade Portuguesa de Cuidados Intensivos and the Infection and Sepsis Group have previously issued health service and management recommendations for critically ill patients with COVID-19. Due to the evolution of knowledge, the panel of experts was again convened to review the current evidence and issue updated recommendations.
A national panel of experts who declared that they had no conflicts of interest regarding the development of the recommendations was assembled. Operational questions were developed based on the PICO methodology, and a rapid systematic review was conducted by consulting different bibliographic sources. The panel determined the direction and strength of the recommendations using two Delphi rounds, conducted in accordance with the principles of the GRADE system. A strong recommendation received the wording “is recommended”, and a weak recommendation was written as “is suggested.”
A total of 48 recommendations and 30 suggestions were issued, covering the following topics: diagnosis of SARS-CoV-2 infection, coinfection and superinfection; criteria for admission, cure and suspension of isolation; organization of services; personal protective equipment; and respiratory support and other specific therapies (antivirals, immunomodulators and anticoagulation).
These recommendations, specifically oriented to the Portuguese reality but that may also apply to Portuguese-speaking African countries and East Timor, aim to support health professionals in the management of critically ill patients with COVID-19. They will be continuously reviewed to reflect the progress of our understanding and the treatment of this pathology.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):320-324
DOI 10.5935/0103-507X.20210041
We report a case of Influenza B infection and Kawasaki disease in an adolescent, diagnosed during the COVID-19 pandemic. An asthmatic female adolescent presented with fever and flu-like symptoms for 7 days and was admitted with acute respiratory failure requiring mechanical ventilation. She progressed with hemodynamic instability responsive to vasoactive drugs. Antibiotic therapy and support measures were introduced, showing progressive hemodynamics and respiratory improvement, however with persistent fever and increased inflammatory markers. During the hospitalization, she developed bilateral non-purulent conjunctivitis, hand and feet desquamation, strawberry tongue, and cervical adenopathy, and was diagnosed with Kawasaki disease. She was prescribed intravenous immunoglobulin and, due to the refractory clinical conditions, corticosteroid therapy was added; 24 hours later, the patient was afebrile. No coronary changes were found. A full viral panel including COVID-19 C-reactive protein and serology could only isolate the Influenza B virus. During the hospitalization, she was diagnosed with pulmonary thromboembolism; coagulopathies were investigated, and she was diagnosed with heterozygous factor V Leiden mutation. There is a potential association between Kawasaki disease and infection with Influenza B or with other viruses such as coronavirus. Therefore, this association should be considered in pediatric patients, adolescents included, with prolonged febrile conditions.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):320-324
DOI 10.5935/0103-507X.20210041
We report a case of Influenza B infection and Kawasaki disease in an adolescent, diagnosed during the COVID-19 pandemic. An asthmatic female adolescent presented with fever and flu-like symptoms for 7 days and was admitted with acute respiratory failure requiring mechanical ventilation. She progressed with hemodynamic instability responsive to vasoactive drugs. Antibiotic therapy and support measures were introduced, showing progressive hemodynamics and respiratory improvement, however with persistent fever and increased inflammatory markers. During the hospitalization, she developed bilateral non-purulent conjunctivitis, hand and feet desquamation, strawberry tongue, and cervical adenopathy, and was diagnosed with Kawasaki disease. She was prescribed intravenous immunoglobulin and, due to the refractory clinical conditions, corticosteroid therapy was added; 24 hours later, the patient was afebrile. No coronary changes were found. A full viral panel including COVID-19 C-reactive protein and serology could only isolate the Influenza B virus. During the hospitalization, she was diagnosed with pulmonary thromboembolism; coagulopathies were investigated, and she was diagnosed with heterozygous factor V Leiden mutation. There is a potential association between Kawasaki disease and infection with Influenza B or with other viruses such as coronavirus. Therefore, this association should be considered in pediatric patients, adolescents included, with prolonged febrile conditions.

Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):196-205
DOI 10.5935/0103-507X.20210027
To identify more severe COVID-19 presentations.
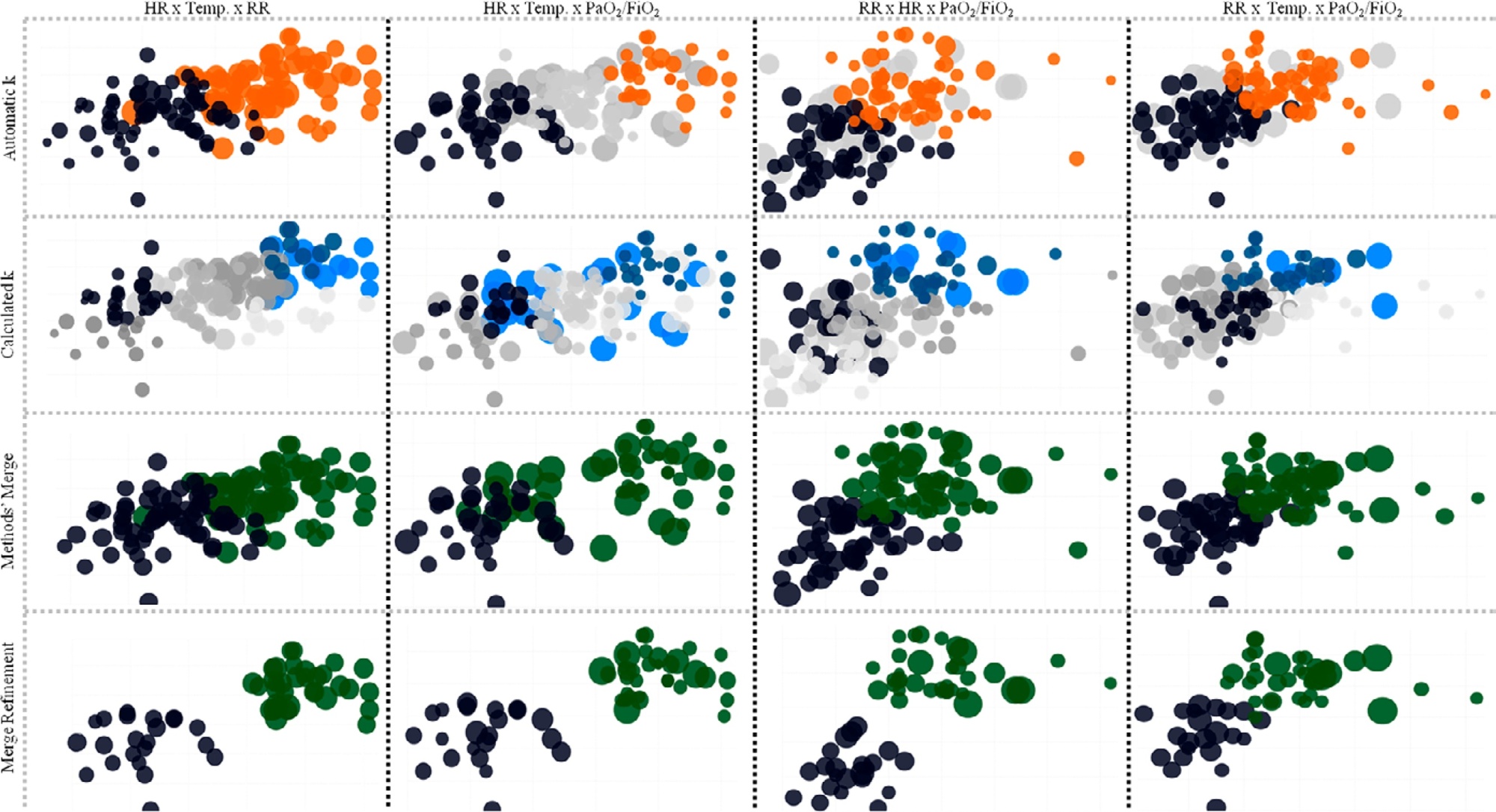
Consecutive intensive care unit-admitted patients were subjected to a stepwise clustering method.
Data from 147 patients who were on average 56 ± 16 years old with a Simplified Acute Physiological Score 3 of 72 ± 18, of which 103 (70%) needed mechanical ventilation and 46 (31%) died in the intensive care unit, were analyzed. From the clustering algorithm, two well-defined groups were found based on maximal heart rate [Cluster A: 104 (95%CI 99 - 109) beats per minute versus Cluster B: 159 (95%CI 155 - 163) beats per minute], maximal respiratory rate [Cluster A: 33 (95%CI 31 - 35) breaths per minute versus Cluster B: 50 (95%CI 47 - 53) breaths per minute], and maximal body temperature [Cluster A: 37.4 (95%CI 37.1 - 37.7)°C versus Cluster B: 39.3 (95%CI 39.1 - 39.5)°C] during the intensive care unit stay, as well as the oxygen partial pressure in the blood over the oxygen inspiratory fraction at intensive care unit admission [Cluster A: 116 (95%CI 99 - 133) mmHg versus Cluster B: 78 (95%CI 63 - 93) mmHg]. Subphenotypes were distinct in inflammation profiles, organ dysfunction, organ support, intensive care unit length of stay, and intensive care unit mortality (with a ratio of 4.2 between the groups).
Our findings, based on common clinical data, revealed two distinct subphenotypes with different disease courses. These results could help health professionals allocate resources and select patients for testing novel therapies.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):196-205
DOI 10.5935/0103-507X.20210027
To identify more severe COVID-19 presentations.
Consecutive intensive care unit-admitted patients were subjected to a stepwise clustering method.
Data from 147 patients who were on average 56 ± 16 years old with a Simplified Acute Physiological Score 3 of 72 ± 18, of which 103 (70%) needed mechanical ventilation and 46 (31%) died in the intensive care unit, were analyzed. From the clustering algorithm, two well-defined groups were found based on maximal heart rate [Cluster A: 104 (95%CI 99 - 109) beats per minute versus Cluster B: 159 (95%CI 155 - 163) beats per minute], maximal respiratory rate [Cluster A: 33 (95%CI 31 - 35) breaths per minute versus Cluster B: 50 (95%CI 47 - 53) breaths per minute], and maximal body temperature [Cluster A: 37.4 (95%CI 37.1 - 37.7)°C versus Cluster B: 39.3 (95%CI 39.1 - 39.5)°C] during the intensive care unit stay, as well as the oxygen partial pressure in the blood over the oxygen inspiratory fraction at intensive care unit admission [Cluster A: 116 (95%CI 99 - 133) mmHg versus Cluster B: 78 (95%CI 63 - 93) mmHg]. Subphenotypes were distinct in inflammation profiles, organ dysfunction, organ support, intensive care unit length of stay, and intensive care unit mortality (with a ratio of 4.2 between the groups).
Our findings, based on common clinical data, revealed two distinct subphenotypes with different disease courses. These results could help health professionals allocate resources and select patients for testing novel therapies.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):325-325
DOI 10.5935/0103-507X.20210042
COVID-19 was declared a pandemic by the World Health Organization on March 11, 2020. The clinical presentation is predominantly respiratory symptoms; however, in the current literature, several neurological manifestations associated with SARS-CoV-2 infection have been described. The authors present the clinical case of a 45-year-old man hospitalized for pneumonia with a positive test result for SARS-CoV-2, without a neurological history, who, on the sixteenth day of hospitalization, presented a sudden change in his state of consciousness accompanied by conjugated right gaze deviation and myoclonus of the face and thoracic region to the left, followed by generalized tonic-clonic seizures associated with persistent left hemiparesis. The present study highlights a positive RT-PCR test for SARS-CoV-2 in cerebrospinal fluid. The patient progressed with gradual improvement, and the outcome was favorable.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(2):325-325
DOI 10.5935/0103-507X.20210042
COVID-19 was declared a pandemic by the World Health Organization on March 11, 2020. The clinical presentation is predominantly respiratory symptoms; however, in the current literature, several neurological manifestations associated with SARS-CoV-2 infection have been described. The authors present the clinical case of a 45-year-old man hospitalized for pneumonia with a positive test result for SARS-CoV-2, without a neurological history, who, on the sixteenth day of hospitalization, presented a sudden change in his state of consciousness accompanied by conjugated right gaze deviation and myoclonus of the face and thoracic region to the left, followed by generalized tonic-clonic seizures associated with persistent left hemiparesis. The present study highlights a positive RT-PCR test for SARS-CoV-2 in cerebrospinal fluid. The patient progressed with gradual improvement, and the outcome was favorable.
Abstract
. ;
Abstract
. ;
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(1):68-74
DOI 10.5935/0103-507X.20210006
To analyze whether changes in medical care due to the application of COVID-19 protocols affected clinical outcomes in patients without COVID-19 during the pandemic.
This was a retrospective, observational cohort study carried out in a thirty-eight-bed surgical and medical intensive care unit of a high complexity private hospital. Patients with respiratory failure admitted to the intensive care unit during March and April 2020 and the same months in 2019 were selected. We compared interventions and outcomes of patients without COVID-19 during the pandemic with patients admitted in 2019. The main variables analyzed were intensive care unit respiratory management, number of chest tomography scans and bronchoalveolar lavages, intensive care unit complications, and status at hospital discharge.
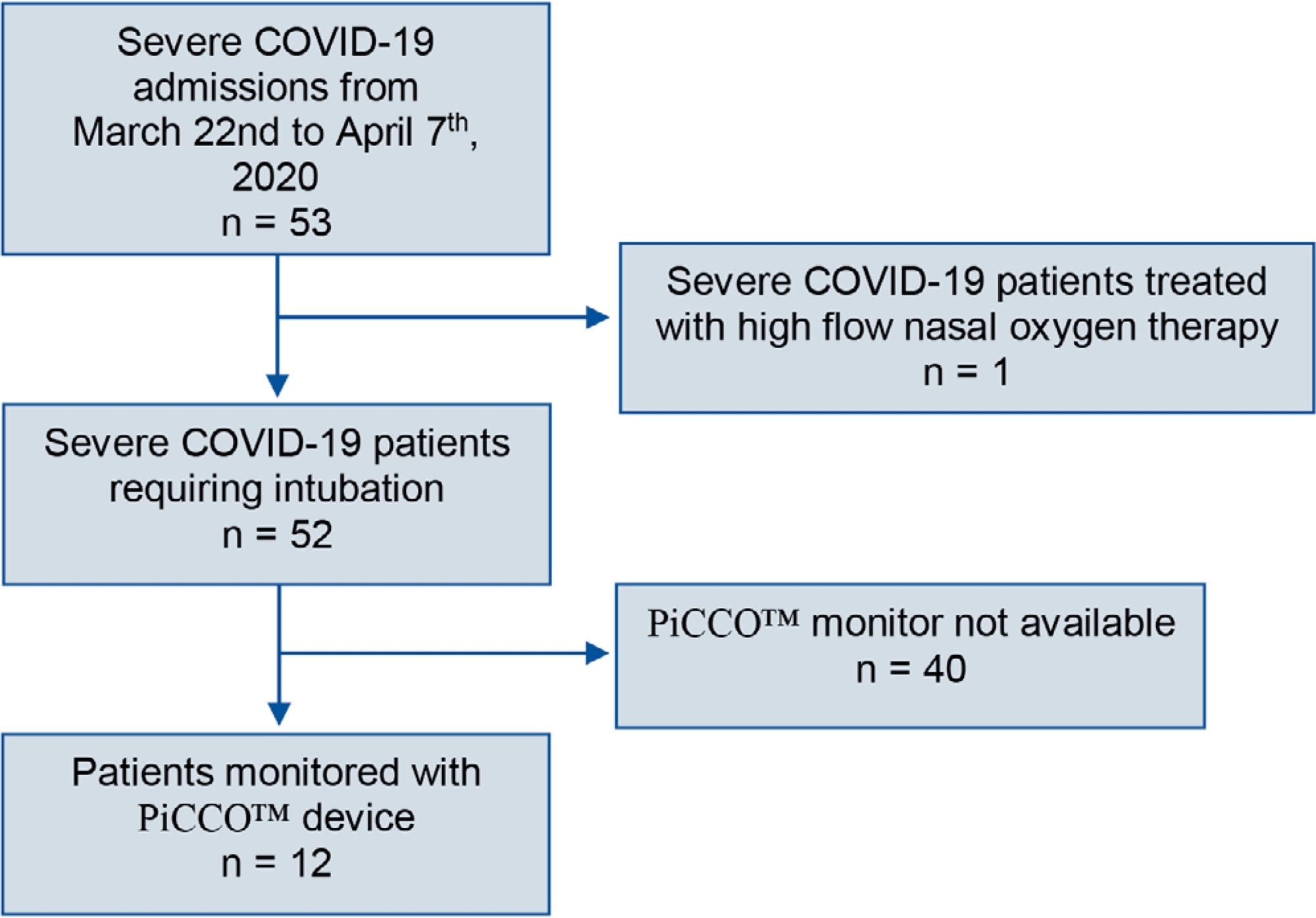
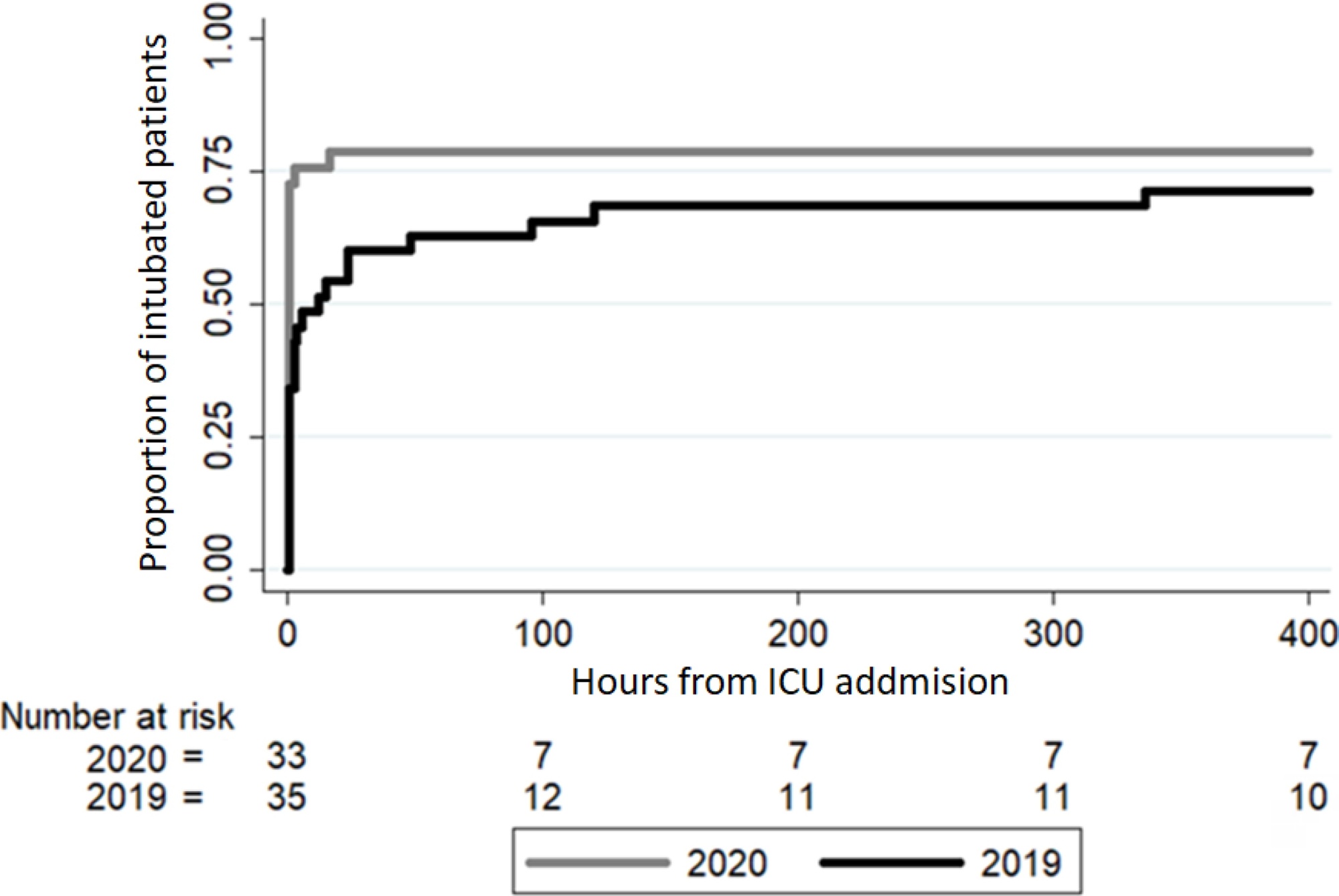
In 2020, a significant reduction in the use of a high-flow nasal cannula was observed: 14 (42%) in 2019 compared to 1 (3%) in 2020. Additionally, in 2020, a significant increase was observed in the number of patients under mechanical ventilation admitted to the intensive care unit from the emergency department, 23 (69%) compared to 11 (31%) in 2019. Nevertheless, the number of patients with mechanical ventilation after 5 days of admission was similar in both years: 24 (69%) in 2019 and 26 (79%) in 2020.
Intensive care unit protocols based on international recommendations for the COVID-19 pandemic have produced a change in non-COVID-19 patient management. We observed a reduction in the use of a high-flow nasal cannula and an increased number of tracheal intubations in the emergency department. However, no changes in the percentage of intubated patients in the intensive care unit, the number of mechanical ventilation days or the length of stay in intensive care unit.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(1):68-74
DOI 10.5935/0103-507X.20210006
To analyze whether changes in medical care due to the application of COVID-19 protocols affected clinical outcomes in patients without COVID-19 during the pandemic.
This was a retrospective, observational cohort study carried out in a thirty-eight-bed surgical and medical intensive care unit of a high complexity private hospital. Patients with respiratory failure admitted to the intensive care unit during March and April 2020 and the same months in 2019 were selected. We compared interventions and outcomes of patients without COVID-19 during the pandemic with patients admitted in 2019. The main variables analyzed were intensive care unit respiratory management, number of chest tomography scans and bronchoalveolar lavages, intensive care unit complications, and status at hospital discharge.
In 2020, a significant reduction in the use of a high-flow nasal cannula was observed: 14 (42%) in 2019 compared to 1 (3%) in 2020. Additionally, in 2020, a significant increase was observed in the number of patients under mechanical ventilation admitted to the intensive care unit from the emergency department, 23 (69%) compared to 11 (31%) in 2019. Nevertheless, the number of patients with mechanical ventilation after 5 days of admission was similar in both years: 24 (69%) in 2019 and 26 (79%) in 2020.
Intensive care unit protocols based on international recommendations for the COVID-19 pandemic have produced a change in non-COVID-19 patient management. We observed a reduction in the use of a high-flow nasal cannula and an increased number of tracheal intubations in the emergency department. However, no changes in the percentage of intubated patients in the intensive care unit, the number of mechanical ventilation days or the length of stay in intensive care unit.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
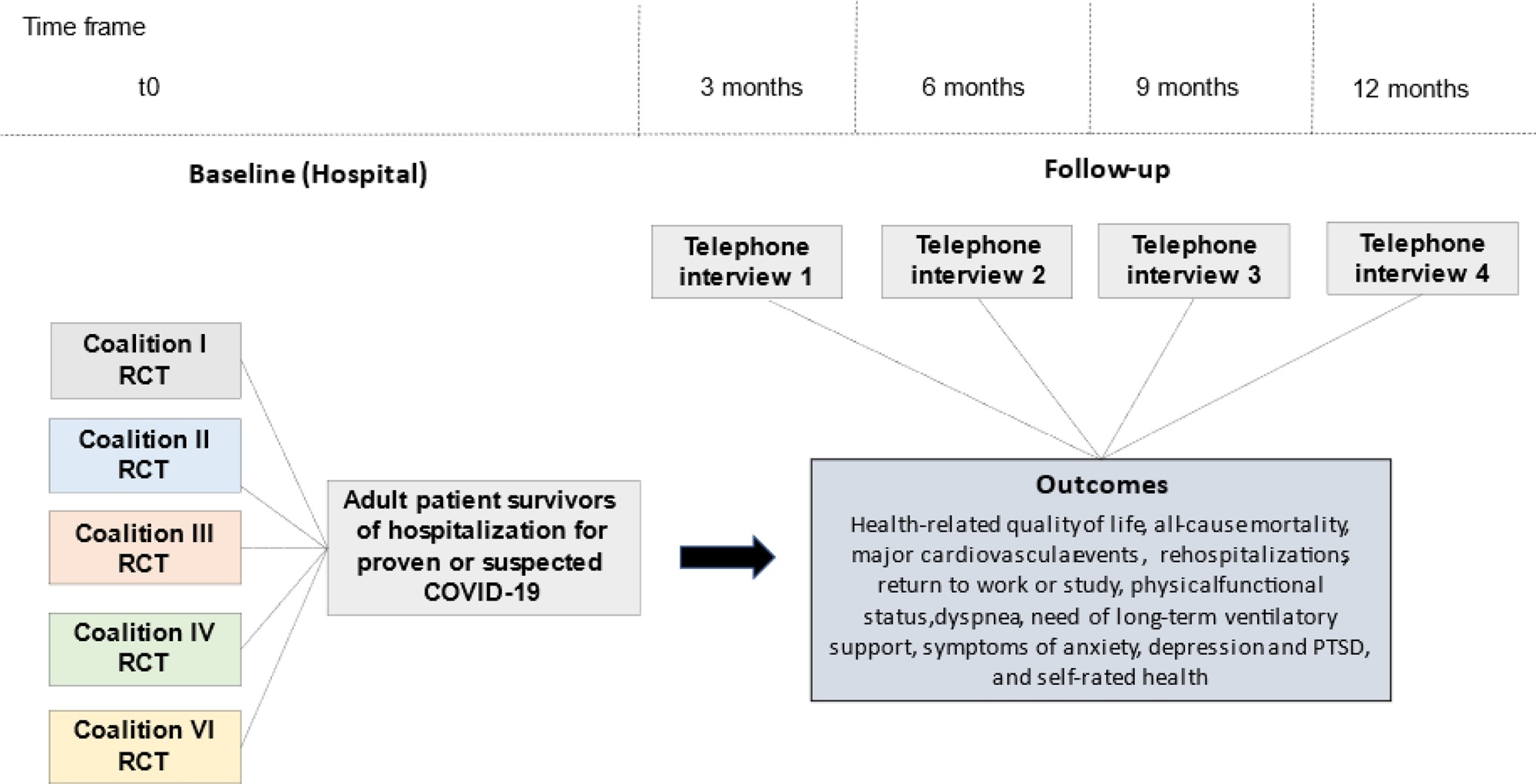
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.
Abstract
Revista Brasileira de Terapia Intensiva. 2021;33(1):31-37
DOI 10.5935/0103-507X.20210003
The long-term effects caused by COVID-19 are unknown. The present study aims to assess factors associated with health-related quality of life and long-term outcomes among survivors of hospitalization for COVID-19 in Brazil.
This is a multicenter prospective cohort study nested in five randomized clinical trials designed to assess the effects of specific COVID-19 treatments in over 50 centers in Brazil. Adult survivors of hospitalization due to proven or suspected SARS-CoV-2 infection will be followed-up for a period of 1 year by means of structured telephone interviews. The primary outcome is the 1-year utility score of health-related quality of life assessed by the EuroQol-5D3L. Secondary outcomes include all-cause mortality, major cardiovascular events, rehospitalizations, return to work or study, physical functional status assessed by the Lawton-Brody Instrumental Activities of Daily Living, dyspnea assessed by the modified Medical Research Council dyspnea scale, need for long-term ventilatory support, symptoms of anxiety and depression assessed by the Hospital Anxiety and Depression Scale, symptoms of posttraumatic stress disorder assessed by the Impact of Event Scale-Revised, and self-rated health assessed by the EuroQol-5D3L Visual Analog Scale. Generalized estimated equations will be performed to test the association between five sets of variables (1- demographic characteristics, 2- premorbid state of health, 3- characteristics of acute illness, 4- specific COVID-19 treatments received, and 5- time-updated postdischarge variables) and outcomes.
The study protocol was approved by the Research Ethics Committee of all participant institutions. The results will be disseminated through conferences and peer-reviewed journals.