nutrition assessment Archives - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2019;31(4):504-510
DOI 10.5935/0103-507X.20190067
To evaluate the risk factors for protein-caloric inadequacy in critically ill patients.
Prospective cohort study of patients hospitalized in an adult intensive care unit between February and November 2017. Patients were followed for 7 days. The conditional probability of inadequacy was calculated using the Kaplan-Meier method and the 95% log-rank test. To assess the risk of inadequacy, crude and adjusted hazard ratios (HR) were calculated using Cox regression with a 95% confidence interval.
Of the 130 patients, 63.8% were male, 73.8% were <60 years of age, and 49.2% were diagnosed with trauma. The mean APACHE II score was 24 points, and 70.0% of the patients had a protein-caloric adequacy >80%. In the univariate analysis, the significant variables for inadequacy were use of vasoactive drugs, interruptions of diet and failure to initiate nutrition early. In the final model, patients who presented with vomiting/gastric residue (adjusted HR = 22.5; 95%CI 5.14 - 98.87) and fasting for extubation (adjusted HR = 14.75; 95%CI 3.59 - 60.63) and for examinations and interventions (adjusted HR = 12.46; 95%CI 4.52 - 34.36) had a higher risk of not achieving protein-caloric adequacy.
Achievement of nutritional goals > 80.0% occurred in 70.0% of patients. The risk factors for protein-caloric inadequacy were nutritional interruptions, especially due to vomiting/gastric residue and fasting for extubation, exams and surgical procedures.
Abstract
Rev Bras Ter Intensiva. 2019;31(4):504-510
DOI 10.5935/0103-507X.20190067
To evaluate the risk factors for protein-caloric inadequacy in critically ill patients.
Prospective cohort study of patients hospitalized in an adult intensive care unit between February and November 2017. Patients were followed for 7 days. The conditional probability of inadequacy was calculated using the Kaplan-Meier method and the 95% log-rank test. To assess the risk of inadequacy, crude and adjusted hazard ratios (HR) were calculated using Cox regression with a 95% confidence interval.
Of the 130 patients, 63.8% were male, 73.8% were <60 years of age, and 49.2% were diagnosed with trauma. The mean APACHE II score was 24 points, and 70.0% of the patients had a protein-caloric adequacy >80%. In the univariate analysis, the significant variables for inadequacy were use of vasoactive drugs, interruptions of diet and failure to initiate nutrition early. In the final model, patients who presented with vomiting/gastric residue (adjusted HR = 22.5; 95%CI 5.14 - 98.87) and fasting for extubation (adjusted HR = 14.75; 95%CI 3.59 - 60.63) and for examinations and interventions (adjusted HR = 12.46; 95%CI 4.52 - 34.36) had a higher risk of not achieving protein-caloric adequacy.
Achievement of nutritional goals > 80.0% occurred in 70.0% of patients. The risk factors for protein-caloric inadequacy were nutritional interruptions, especially due to vomiting/gastric residue and fasting for extubation, exams and surgical procedures.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
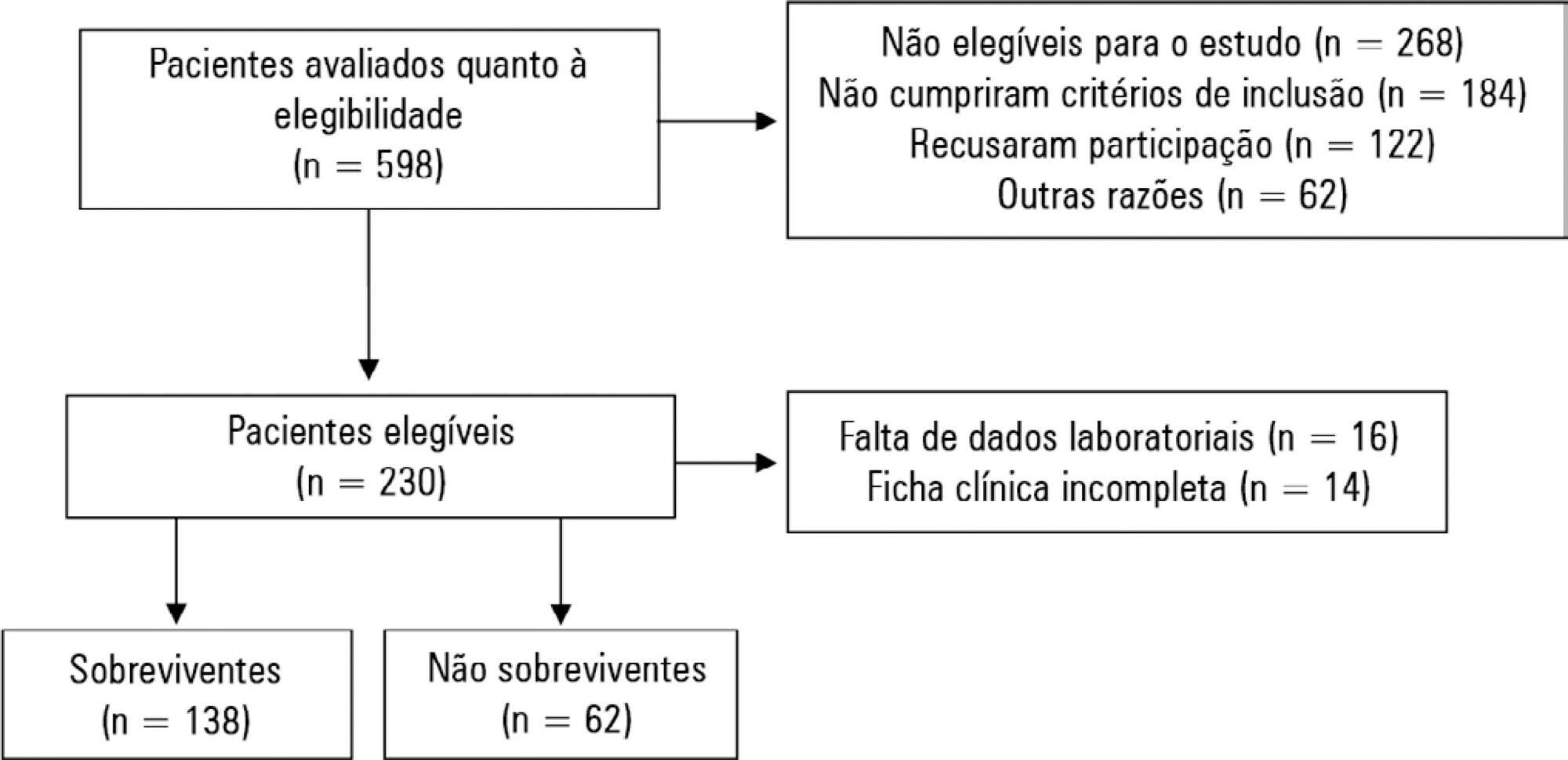
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients' medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 - 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 - 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 - 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 - 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 - 6.44; p < 0.001).
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):326-332
DOI 10.5935/0103-507X.20190041
To evaluate possible associations between nutritional risk and the clinical outcomes of critical patients admitted to an intensive care unit.
A prospective study was carried out with a cohort comprising 200 patients admitted to a university hospital intensive care unit. Nutritional risk was assessed with the NRS-2002 and NUTRIC scores. Patients with scores ≥ 5 were considered at high nutritional risk. Clinical data and outcome measures were obtained from patients' medical records. Multiple logistic regression analysis was used to calculate odds ratios and their respective 95% confidence intervals (for clinical outcomes).
This sample of critical patients had a mean age of 59.4 ± 16.5 years and 53.5% were female. The proportions at high nutritional risk according to NRS-2002 and NUTRIC were 55% and 36.5%, respectively. Multiple logistic regression models adjusted for gender and type of admission indicated that high nutritional risk assessed by the NRS-2002 was positively associated with use of mechanical ventilation (OR = 2.34; 95%CI 1.31 - 4.19; p = 0.004); presence of infection (OR = 2.21; 95%CI 1.24 - 3.94; p = 0.007), and death (OR = 1.86; 95%CI 1.01 - 3.41; p = 0.045). When evaluated by NUTRIC, nutritional risk was associated with renal replacement therapy (OR = 2.10; 95%CI 1.02 - 4.15; p = 0.040) and death (OR = 3.48; 95%CI 1.88 - 6.44; p < 0.001).
In critically ill patients, high nutritional risk was positively associated with an increased risk of clinical outcomes including hospital death.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):379-385
DOI 10.5935/0103-507X.20190061
To collect data on the use of The Nutrition Risk in Critically Ill (NUTRIC) score.
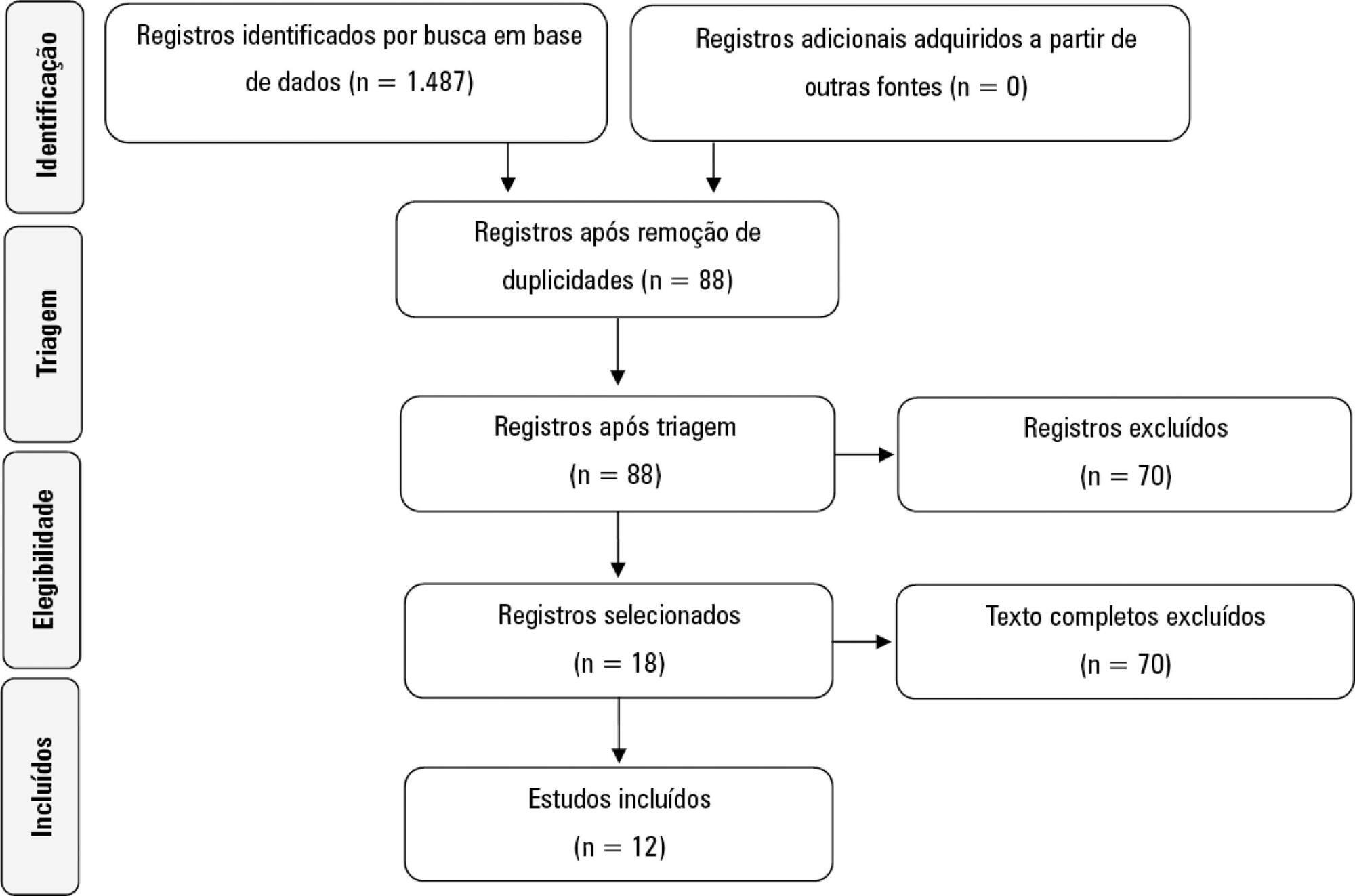
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Reviews, abstracts, dissertations, protocols and case reports were excluded from this review; to be included in the review, studies needed to specifically evaluate the NUTRIC score and to have been published in English, Spanish or Portuguese.
We included 12 (0.8%) studies from our search in this review. Ten studies (83.3%) were observational, 1 was a pilot study (8.3%) and 1 was a randomized control trial (8.3%). All of the included studies (100%) chose not to use IL-6 and considered a high nutritional risk cutoff point ≥ 5. There were 11 (91.7%) English language studies versus 1 (8.3%) Spanish language study. Mechanical ventilation and a high NUTRIC score were significantly correlated in four studies. The association between intensive care unit or hospital length of stay and nutritional high risk was significant in three studies. Seven studies found a statistically significant association between the NUTRIC score and mortality.
The NUTRIC score is related to clinical outcomes, such as length of hospital stay, and is appropriate for use in critically ill patients in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2019;31(3):379-385
DOI 10.5935/0103-507X.20190061
To collect data on the use of The Nutrition Risk in Critically Ill (NUTRIC) score.
A systematic literature search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Reviews, abstracts, dissertations, protocols and case reports were excluded from this review; to be included in the review, studies needed to specifically evaluate the NUTRIC score and to have been published in English, Spanish or Portuguese.
We included 12 (0.8%) studies from our search in this review. Ten studies (83.3%) were observational, 1 was a pilot study (8.3%) and 1 was a randomized control trial (8.3%). All of the included studies (100%) chose not to use IL-6 and considered a high nutritional risk cutoff point ≥ 5. There were 11 (91.7%) English language studies versus 1 (8.3%) Spanish language study. Mechanical ventilation and a high NUTRIC score were significantly correlated in four studies. The association between intensive care unit or hospital length of stay and nutritional high risk was significant in three studies. Seven studies found a statistically significant association between the NUTRIC score and mortality.
The NUTRIC score is related to clinical outcomes, such as length of hospital stay, and is appropriate for use in critically ill patients in intensive care units.
Abstract
Rev Bras Ter Intensiva. 2013;25(1):25-31
DOI 10.1590/S0103-507X2013000100006
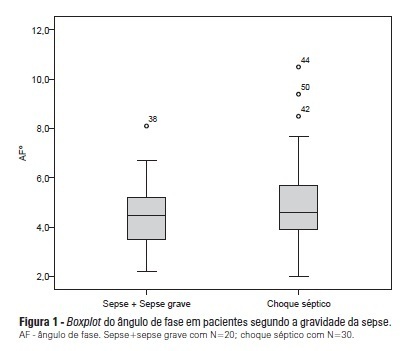
OBJECTIVE: To calculate the values of the phase angle of septic patients using bioelectrical impedance analysis, correlate the values with clinical and biochemical variables, and compare them to reference values. METHODS: Cohort study conducted with 50 septic patients aged ≥18 years old, admitted to intensive care units, and assessed according to prognostic indexes (APACHE II and SOFA), clinical progression (mortality, severity of sepsis, length of stay in intensive care unit), biochemical parameters (albumin and C-reactive protein), and the phase angle. RESULTS: The average age of the sample was 65.6±16.5 years. Most patients were male (58%) and suffering from septic shock (60%). The average APACHE II and SOFA scores were 22.98±7.1 and 7.5±3.4, respectively. The patients who survived stayed nine days on average (five to 13) in the intensive care unit, and the mortality rate was 30%. The average value of the phase angle was 5.4±2.6° in the total sample and was smaller among the females compared with the males (p=0.01). The phase angle measures did not exhibit an association with the severity of the sepsis, mortality, gender, and age or correlate with the length of hospitalization or the biochemical parameters. The participants' phase angle values adjusted per gender and age were 1.1 to 1.9 times lower compared with the values for a normal population. CONCLUSION: The average value of the phase angle of septic patients was lower compared with the reference values for a healthy population. The phase angle measures did not exhibit association with the clinical and biochemical variables, which might be explained by the sample homogeneity.
Abstract
Rev Bras Ter Intensiva. 2013;25(1):25-31
DOI 10.1590/S0103-507X2013000100006
OBJECTIVE: To calculate the values of the phase angle of septic patients using bioelectrical impedance analysis, correlate the values with clinical and biochemical variables, and compare them to reference values. METHODS: Cohort study conducted with 50 septic patients aged ≥18 years old, admitted to intensive care units, and assessed according to prognostic indexes (APACHE II and SOFA), clinical progression (mortality, severity of sepsis, length of stay in intensive care unit), biochemical parameters (albumin and C-reactive protein), and the phase angle. RESULTS: The average age of the sample was 65.6±16.5 years. Most patients were male (58%) and suffering from septic shock (60%). The average APACHE II and SOFA scores were 22.98±7.1 and 7.5±3.4, respectively. The patients who survived stayed nine days on average (five to 13) in the intensive care unit, and the mortality rate was 30%. The average value of the phase angle was 5.4±2.6° in the total sample and was smaller among the females compared with the males (p=0.01). The phase angle measures did not exhibit an association with the severity of the sepsis, mortality, gender, and age or correlate with the length of hospitalization or the biochemical parameters. The participants' phase angle values adjusted per gender and age were 1.1 to 1.9 times lower compared with the values for a normal population. CONCLUSION: The average value of the phase angle of septic patients was lower compared with the reference values for a healthy population. The phase angle measures did not exhibit association with the clinical and biochemical variables, which might be explained by the sample homogeneity.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2008;20(3):286-295
DOI 10.1590/S0103-507X2008000300012
Considering the importance and the difficulties inherent to nutritional state assessment, as well as the results interpretation and the inexistence of specific and validated guidelines related to applied methods to the severely ill patient, the present revision aims to contribute to the analysis and recommendation of efficient methods, which are suitable to use and reliable in terms of interpretation in the context of the severely ill patient. The presence of edema and unspecific alterations in the plasmatic concentrations of proteins; altered anthropometrics variables reflecting more the rearrangement of the total body water than the nutritional state changes; inconclusive studies with electric bioimpedance; absence of data related to the application of the global subjective assessment to severely ill patients; altered biochemical markers as a consequence of the metabolic changes that, among others, indicate several method limitations to these patients. Notwithstanding the lack of studies to validate the various methods, recommendations based on clinical evidences, observation and physiopathology alterations are available. Independent from the methods, clinical observation by the health staff at all stages is mandatory. It is crucial to dedicate more efforts to identify methods and their specificity to detection, risk assessment or monitoring.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):331-337
DOI 10.1590/S0103-507X2006000400003
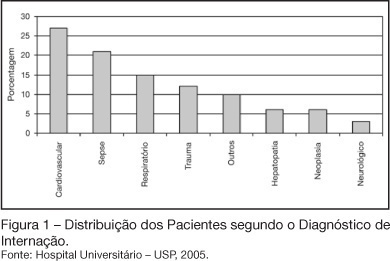
BACKGROUND AND OBJECTIVES: In critically ill patients nutritional deficiency is common. Considering this fact, the diary monitoring of energy delivered is extremely important. The objective of this study is to assess the adequacy of enteral nutrition (EN) in an Intensive Care Unit (ICU) and identify the reasons for interruptions in feeding. METHODS: Prospective study of adult patients admitted to ICU in period of 53 days. Patients receiving continuous enteral tube feeding (22 hours/day) exclusively and post-pyloric tube feeding position were followed. The feeding volume started at 25 mL/h and was increased until nutritional goal, guided by a feeding protocol. RESULTS: 33 patients between 18 and 85 years old were studied. 58% were male. The main admission diagnoses were cardiovascular diseases (27%) and septic shock (21%). The mean time to feeding was 25.3 hours after the patient admission and nutritional goal was achieved in a mean time of 32 hours. The total volume prescribed per day was sufficient to guarantee a mean of 26.1 kcal/kg of body weight and 1.04 g of protein/kg of body weight. Patients received a mean of 19.5 kcal/kg of body weight and 0.8 g of protein/kg of body weight, which correspond a 74% of adequacy. Interruptions of feeding for routine procedures related to patients accounted for 40.6% of the total reasons. CONCLUSIONS: The nutritional support is adequate considering the literature for these patients, who clinical instability causes gastrointestinal intolerance. The effective participation of the Nutrition Therapy Team can contribute positively on nutritional therapy.
Abstract
Rev Bras Ter Intensiva. 2006;18(4):331-337
DOI 10.1590/S0103-507X2006000400003
BACKGROUND AND OBJECTIVES: In critically ill patients nutritional deficiency is common. Considering this fact, the diary monitoring of energy delivered is extremely important. The objective of this study is to assess the adequacy of enteral nutrition (EN) in an Intensive Care Unit (ICU) and identify the reasons for interruptions in feeding. METHODS: Prospective study of adult patients admitted to ICU in period of 53 days. Patients receiving continuous enteral tube feeding (22 hours/day) exclusively and post-pyloric tube feeding position were followed. The feeding volume started at 25 mL/h and was increased until nutritional goal, guided by a feeding protocol. RESULTS: 33 patients between 18 and 85 years old were studied. 58% were male. The main admission diagnoses were cardiovascular diseases (27%) and septic shock (21%). The mean time to feeding was 25.3 hours after the patient admission and nutritional goal was achieved in a mean time of 32 hours. The total volume prescribed per day was sufficient to guarantee a mean of 26.1 kcal/kg of body weight and 1.04 g of protein/kg of body weight. Patients received a mean of 19.5 kcal/kg of body weight and 0.8 g of protein/kg of body weight, which correspond a 74% of adequacy. Interruptions of feeding for routine procedures related to patients accounted for 40.6% of the total reasons. CONCLUSIONS: The nutritional support is adequate considering the literature for these patients, who clinical instability causes gastrointestinal intolerance. The effective participation of the Nutrition Therapy Team can contribute positively on nutritional therapy.