Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
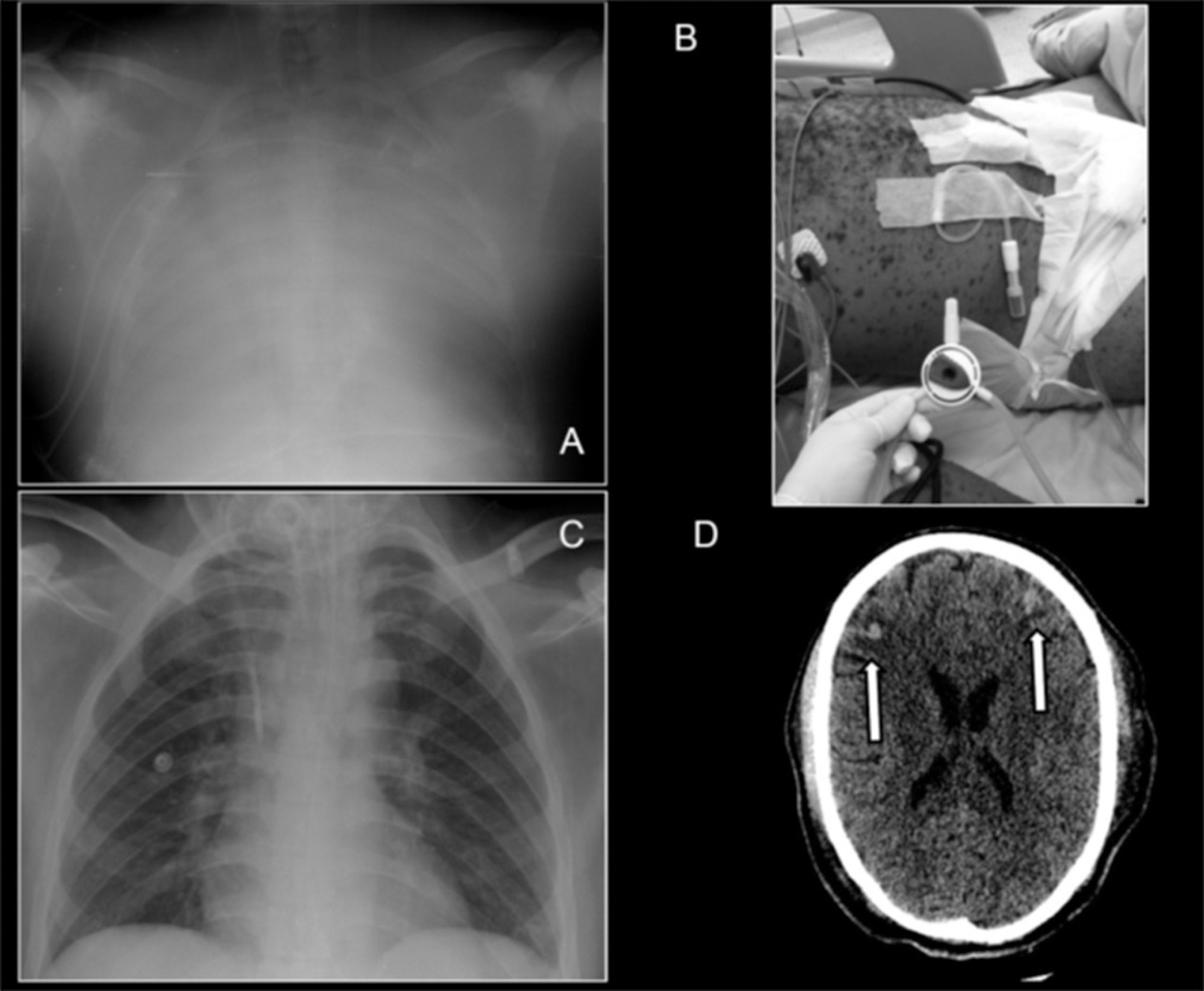
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):410-415
DOI 10.5935/0103-507X.20140063
A case of a 30 year-old man presenting with severe systemic chickenpox with refractory hypoxemia, central nervous system vasculitis and anuric renal failure is described. Ambulance transportation and support using veno-venous extracorporeal membrane oxygenation were necessary until the patient recovered. Ultimately, the potential use of extracorporeal membrane oxygenation support in low-middle income countries to manage common diseases is discussed.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
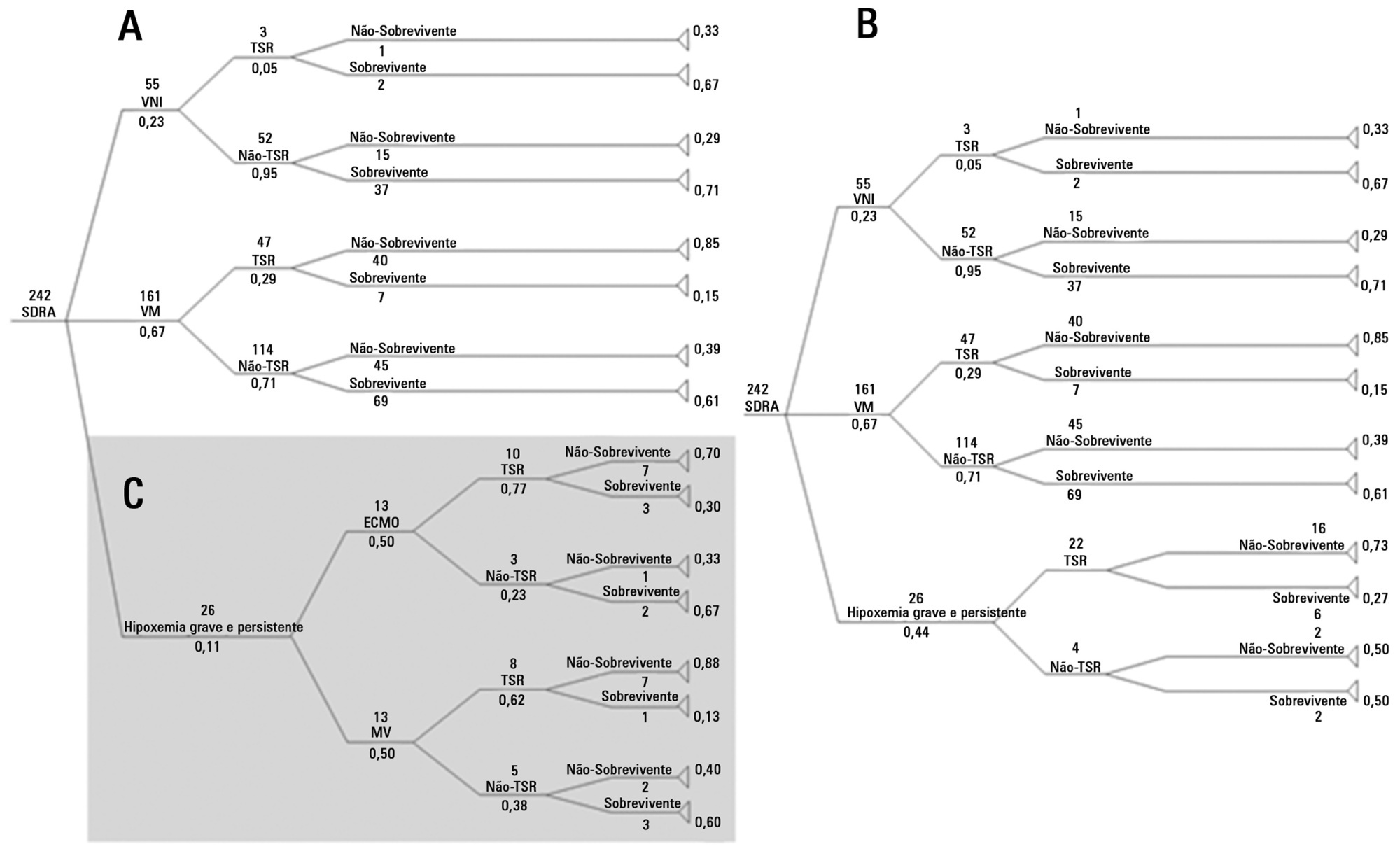
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):253-262
DOI 10.5935/0103-507X.20140036
To analyze the cost-utility of using extracorporeal oxygenation for patients with severe acute respiratory distress syndrome in Brazil.
A decision tree was constructed using databases from previously published studies. Costs were taken from the average price paid by the Brazilian Unified Health System (Sistema Único de Saúde; SUS) over three months in 2011. Using the data of 10,000,000 simulated patients with predetermined outcomes and costs, an analysis was performed of the ratio between cost increase and years of life gained, adjusted for quality (cost-utility), with survival rates of 40 and 60% for patients using extracorporeal membrane oxygenation.
The decision tree resulted in 16 outcomes with different life support techniques. With survival rates of 40 and 60%, respectively, the increased costs were R$=-301.00/-14.00, with a cost of R$=-30,913.00/-1,752.00 paid per six-month quality-adjusted life-year gained and R$=-2,386.00/-90.00 per quality-adjusted life-year gained until the end of life, when all patients with severe ARDS were analyzed. Analyzing only patients with severe hypoxemia (i.e., a ratio of partial oxygen pressure in the blood to the fraction of inspired oxygen <100mmHg), the increased cost was R$=-5,714.00/272.00, with a cost per six-month quality-adjusted life-year gained of R$=-9,521.00/293.00 and a cost of R$=-280.00/7.00 per quality-adjusted life-year gained.
The cost-utility ratio associated with the use of extracorporeal membrane oxygenation in Brazil is potentially acceptable according to this hypothetical study.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):347-354
DOI 10.5935/0103-507X.20140053
To assess the diagnostic and prognostic efficacy of urine neutrophil gelatinase-associated lipocalin in patients admitted to an intensive care unit.
Longitudinal, prospective cohort study conducted in a cardiology intensive care unit. The participants were divided into groups with and without acute kidney injury and were followed from admission to the intensive care unit until hospital discharge or death. Serum creatinine, urine output and urine neutrophil gelatinase-associated lipocalin were measured 24 and 48 hours after admission.
A total of 83 patients admitted to the intensive care unit for clinical reasons were assessed, most being male (57.8%). The participants were divided into groups without acute kidney injury (N=18), with acute kidney injury (N=28) and with severe acute kidney injury (N=37). Chronic diseases, mechanical ventilation and renal replacement therapy were more common in the groups with acute kidney injury and severe acute kidney injury, and those groups exhibited longer intensive care unit stay and hospital stay and higher mortality. Serum creatinine did not change significantly in the group with acute kidney injury within the first 24 hours of admission to the intensive care unit, although, urine neutrophil gelatinase-associated lipocalin was high in the groups with acute kidney injury and severe acute kidney injury (p<0.001). Increased urine neutrophil gelatinase-associated lipocalin was associated with death.
An increase in urine neutrophil gelatinase-associated lipocalin precedes variations in serum creatinine in patients with acute kidney injury and may be associated with death.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):347-354
DOI 10.5935/0103-507X.20140053
To assess the diagnostic and prognostic efficacy of urine neutrophil gelatinase-associated lipocalin in patients admitted to an intensive care unit.
Longitudinal, prospective cohort study conducted in a cardiology intensive care unit. The participants were divided into groups with and without acute kidney injury and were followed from admission to the intensive care unit until hospital discharge or death. Serum creatinine, urine output and urine neutrophil gelatinase-associated lipocalin were measured 24 and 48 hours after admission.
A total of 83 patients admitted to the intensive care unit for clinical reasons were assessed, most being male (57.8%). The participants were divided into groups without acute kidney injury (N=18), with acute kidney injury (N=28) and with severe acute kidney injury (N=37). Chronic diseases, mechanical ventilation and renal replacement therapy were more common in the groups with acute kidney injury and severe acute kidney injury, and those groups exhibited longer intensive care unit stay and hospital stay and higher mortality. Serum creatinine did not change significantly in the group with acute kidney injury within the first 24 hours of admission to the intensive care unit, although, urine neutrophil gelatinase-associated lipocalin was high in the groups with acute kidney injury and severe acute kidney injury (p<0.001). Increased urine neutrophil gelatinase-associated lipocalin was associated with death.
An increase in urine neutrophil gelatinase-associated lipocalin precedes variations in serum creatinine in patients with acute kidney injury and may be associated with death.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):355-359
DOI 10.5935/0103-507X.20140054
To assess adherence to a ventilator care bundle in an intensive care unit and to determine the impact of adherence on the rates of ventilatorassociated pneumonia.
A total of 198 beds were assessed for 60 days using a checklist that consisted of the following items: bed head elevation to 30 to 45º; position of the humidifier filter; lack of fluid in the ventilator circuit; oral hygiene; cuff pressure; and physical therapy. Next, an educational lecture was delivered, and 235 beds were assessed for the following 60 days. Data were also collected on the incidence of ventilator-acquired pneumonia.
Adherence to the following ventilator care bundle items increased: bed head elevation from 18.7% to 34.5%; lack of fluid in the ventilator circuit from 55.6% to 72.8%; oral hygiene from 48.5% to 77.8%; and cuff pressure from 29.8% to 51.5%. The incidence of ventilator-associated pneumonia was statistically similar before and after intervention (p=0.389).
The educational intervention performed in this study increased the adherence to the ventilator care bundle, but the incidence of ventilator-associated pneumonia did not decrease in the small sample that was assessed.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):355-359
DOI 10.5935/0103-507X.20140054
To assess adherence to a ventilator care bundle in an intensive care unit and to determine the impact of adherence on the rates of ventilatorassociated pneumonia.
A total of 198 beds were assessed for 60 days using a checklist that consisted of the following items: bed head elevation to 30 to 45º; position of the humidifier filter; lack of fluid in the ventilator circuit; oral hygiene; cuff pressure; and physical therapy. Next, an educational lecture was delivered, and 235 beds were assessed for the following 60 days. Data were also collected on the incidence of ventilator-acquired pneumonia.
Adherence to the following ventilator care bundle items increased: bed head elevation from 18.7% to 34.5%; lack of fluid in the ventilator circuit from 55.6% to 72.8%; oral hygiene from 48.5% to 77.8%; and cuff pressure from 29.8% to 51.5%. The incidence of ventilator-associated pneumonia was statistically similar before and after intervention (p=0.389).
The educational intervention performed in this study increased the adherence to the ventilator care bundle, but the incidence of ventilator-associated pneumonia did not decrease in the small sample that was assessed.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):367-372
DOI 10.5935/0103-507X.20140056
To test the effectiveness of using a cuff pressure relief valve technique to maintain cuff pressure levels within the normal in vitro range (Phase 1) in patients admitted to the intensive care unit (Phase 2) and to test the reproducibility of the technique using different syringes.
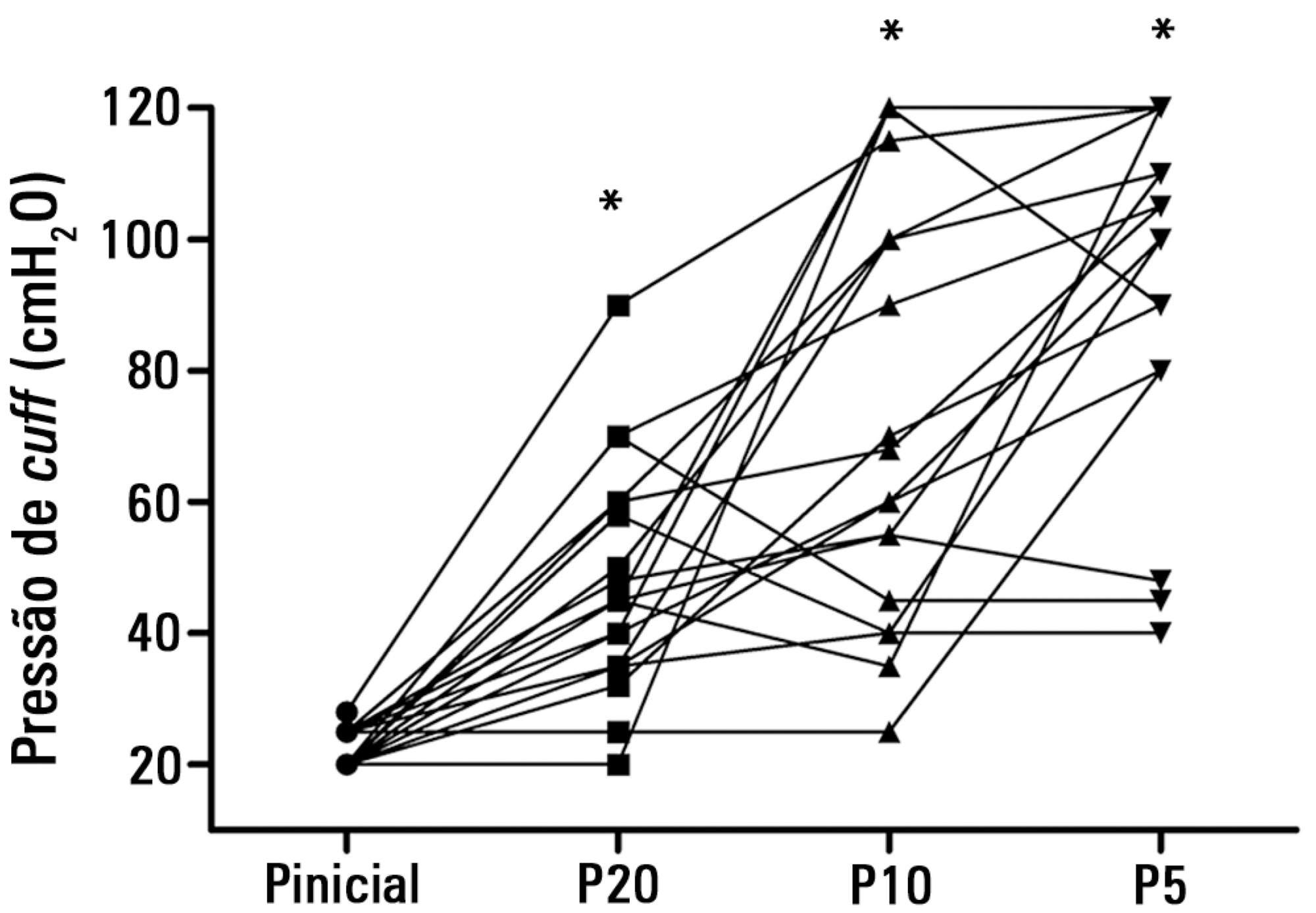
In Phase 1, a tracheal tube was inserted into a trachea model. Ten- and 20mL syringes were used to inflate the cuff through the tracheal tube. The cuff was slowly and steadily inflated until the syringe plunger would move in the opposite direction of the application. After the plunger stopped, the cuff pressures were recorded. In Phase 2, the same maneuvers for inflating the cuff were performed on 20 patients using 5, 10, and 20mL syringes and were compared with manometer measurements. The intraclass correlation coefficient and Bland-Altman analysis were employed to determine the reproducibility and agreement between syringes. Data were expressed as medians (interquartile range).
There was no reproducibility between syringes with an intraclass correlation coefficient ranging between -0.33 and 0.8 (p>0.05). The pressures generated with the syringes were higher than the pressures generated using a standard manometer: the 5mL syringe pressure was 105cmH2O (82.5-120cmH2O), the 10mL syringe pressure was 69cmH2O (47.5-111.3cmH2O), and the 20mL syringe pressure was 45cmH2O (35-59.5cmH2O). The Bland-Altman analysis confirmed the large bias and variability between the syringes used, compared with the manometer.
The use of syringes is not an effective technique for determining the cuff pressure in patients admitted to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):367-372
DOI 10.5935/0103-507X.20140056
To test the effectiveness of using a cuff pressure relief valve technique to maintain cuff pressure levels within the normal in vitro range (Phase 1) in patients admitted to the intensive care unit (Phase 2) and to test the reproducibility of the technique using different syringes.
In Phase 1, a tracheal tube was inserted into a trachea model. Ten- and 20mL syringes were used to inflate the cuff through the tracheal tube. The cuff was slowly and steadily inflated until the syringe plunger would move in the opposite direction of the application. After the plunger stopped, the cuff pressures were recorded. In Phase 2, the same maneuvers for inflating the cuff were performed on 20 patients using 5, 10, and 20mL syringes and were compared with manometer measurements. The intraclass correlation coefficient and Bland-Altman analysis were employed to determine the reproducibility and agreement between syringes. Data were expressed as medians (interquartile range).
There was no reproducibility between syringes with an intraclass correlation coefficient ranging between -0.33 and 0.8 (p>0.05). The pressures generated with the syringes were higher than the pressures generated using a standard manometer: the 5mL syringe pressure was 105cmH2O (82.5-120cmH2O), the 10mL syringe pressure was 69cmH2O (47.5-111.3cmH2O), and the 20mL syringe pressure was 45cmH2O (35-59.5cmH2O). The Bland-Altman analysis confirmed the large bias and variability between the syringes used, compared with the manometer.
The use of syringes is not an effective technique for determining the cuff pressure in patients admitted to the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):373-378
DOI 10.5935/0103-507X.20140057
The objective of this study was to translate and culturally adapt the Behavioral Pain Scale to Brazilian Portuguese and to evaluate the psychometric properties of this scale.
This study was conducted in two phases: the Behavioral Pain Scale was translated and culturally adapted to Brazilian Portuguese and the psychometric properties of this scale were subsequently assessed (reliability and clinical utility). The study sample consisted of 100 patients who were older than 18 years of age, admitted to an intensive care unit, intubated, mechanically ventilated, and subjected or not to sedation and analgesia from July 2012 to December 2012. Pediatric and non-intubated patients were excluded. The study was conducted at a large private hospital that was situated in the city of São Paulo (SP).
Regarding reproducibility, the results revealed that the observed agreement between the two evaluators was 92.08% for the pain descriptor “adaptation to mechanical ventilation”, 88.1% for “upper limbs”, and 90.1% for “facial expression”. The kappa coefficient of agreement for “adaptation to mechanical ventilation” assumed a value of 0.740. Good agreement was observed between the evaluators with an intraclass correlation coefficient of 0.807 (95% confidence interval: 0.727-0.866).
The Behavioral Pain Scale was easy to administer and reproduce. Additionally, this scale had adequate internal consistency. The Behavioral Pain Scale was satisfactorily adapted to Brazilian Portuguese for the assessment of pain in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):373-378
DOI 10.5935/0103-507X.20140057
The objective of this study was to translate and culturally adapt the Behavioral Pain Scale to Brazilian Portuguese and to evaluate the psychometric properties of this scale.
This study was conducted in two phases: the Behavioral Pain Scale was translated and culturally adapted to Brazilian Portuguese and the psychometric properties of this scale were subsequently assessed (reliability and clinical utility). The study sample consisted of 100 patients who were older than 18 years of age, admitted to an intensive care unit, intubated, mechanically ventilated, and subjected or not to sedation and analgesia from July 2012 to December 2012. Pediatric and non-intubated patients were excluded. The study was conducted at a large private hospital that was situated in the city of São Paulo (SP).
Regarding reproducibility, the results revealed that the observed agreement between the two evaluators was 92.08% for the pain descriptor “adaptation to mechanical ventilation”, 88.1% for “upper limbs”, and 90.1% for “facial expression”. The kappa coefficient of agreement for “adaptation to mechanical ventilation” assumed a value of 0.740. Good agreement was observed between the evaluators with an intraclass correlation coefficient of 0.807 (95% confidence interval: 0.727-0.866).
The Behavioral Pain Scale was easy to administer and reproduce. Additionally, this scale had adequate internal consistency. The Behavioral Pain Scale was satisfactorily adapted to Brazilian Portuguese for the assessment of pain in critically ill patients.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):379-383
DOI 10.5935/0103-507X.20140058
To describe the oral health status of patients hospitalized in an intensive care unit.
Clinical assessment of the oral cavity was performed in 35 patients at two time-points (up to 48 hours after admission and 72 hours after the first assessment) and recorded in data collection forms. The following data were collected: plaque index, condition of the mucosa, presence or absence of dental prosthesis, number of teeth present, and tongue coating index.
The prevalence of nosocomial infection was 22% (eight patients), with 50% respiratory tract infections. All patients exhibited oral biofilm, and 20 (57%) showed biofilm visible to the naked eye; tongue coating was present on more than two thirds of the tongue in 24 patients (69%) and was thick in most cases. A significant increase in plaque index (p=0.007) occurred after 72 hours, although the tongue coating index was p<0.001 regarding the area and p=0.5 regarding the thickness.
The plaque and tongue coating indices increased with the length of hospital stay at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(4):379-383
DOI 10.5935/0103-507X.20140058
To describe the oral health status of patients hospitalized in an intensive care unit.
Clinical assessment of the oral cavity was performed in 35 patients at two time-points (up to 48 hours after admission and 72 hours after the first assessment) and recorded in data collection forms. The following data were collected: plaque index, condition of the mucosa, presence or absence of dental prosthesis, number of teeth present, and tongue coating index.
The prevalence of nosocomial infection was 22% (eight patients), with 50% respiratory tract infections. All patients exhibited oral biofilm, and 20 (57%) showed biofilm visible to the naked eye; tongue coating was present on more than two thirds of the tongue in 24 patients (69%) and was thick in most cases. A significant increase in plaque index (p=0.007) occurred after 72 hours, although the tongue coating index was p<0.001 regarding the area and p=0.5 regarding the thickness.
The plaque and tongue coating indices increased with the length of hospital stay at the intensive care unit.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients' condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.
Abstract
Rev Bras Ter Intensiva. 2014;26(3):292-298
DOI 10.5935/0103-507X.20140041
The nursing workload consists of the time spent by the nursing staff to perform the activities for which they are responsible, whether directly or indirectly related to patient care. The aim of this study was to evaluate the nursing workload in an adult intensive care unit at a university hospital using the Nursing Activities Score (NAS) instrument.
A longitudinal, prospective study that involved the patients admitted to the intensive care unit of a university hospital between March and December 2008. The data were collected daily to calculate the NAS, the Acute Physiology and Chronic Health Evaluation (APACHE II), the Sequential Organ Failure Assessment (SOFA) and the Therapeutic Intervention Scoring System (TISS-28) of patients until they left the adult intensive care unit or after 90 days of hospitalization. The level of significance was set at 5%.
In total, 437 patients were evaluated, which resulted in an NAS of 74.4%. The type of admission, length of stay in the intensive care unit and the patients' condition when leaving the intensive care unit and hospital were variables associated with differences in the nursing workload. There was a moderate correlation between the mean NAS and APACHE II severity score (r=0.329), the mean organic dysfunction SOFA score (r=0.506) and the mean TISS-28 score (r=0.600).
We observed a high nursing workload in this study. These results can assist in planning the size of the staff required. The workload was influenced by clinical characteristics, including an increased workload required for emergency surgical patients and patients who died.