Intensive care units Archives - Page 3 of 26 - Critical Care Science (CCS)

Abstract
Rev Bras Ter Intensiva. 2020;32(2):268-276
DOI 10.5935/0103-507X.20200043
To conduct a national survey of intensive care professionals to identify the practices for promoting sleep in adult intensive care units in Brazil and describe the professionals’ perceptions of the importance of sleep for patients.
An electronic questionnaire was distributed by the clinical research cooperation network of the Associação de Medicina Intensiva Brasileira and by the Brazilian Research in Intensive Care Network to physicians and nurses registered with the association. The questionnaire evaluated the profile of the respondents, the profile of their intensive care units, whether protocols for promoting sleep were present, the pharmacological and nonpharmacological measures typically employed in the unit, and the professionals’ perceptions regarding sleep in critically ill patients.
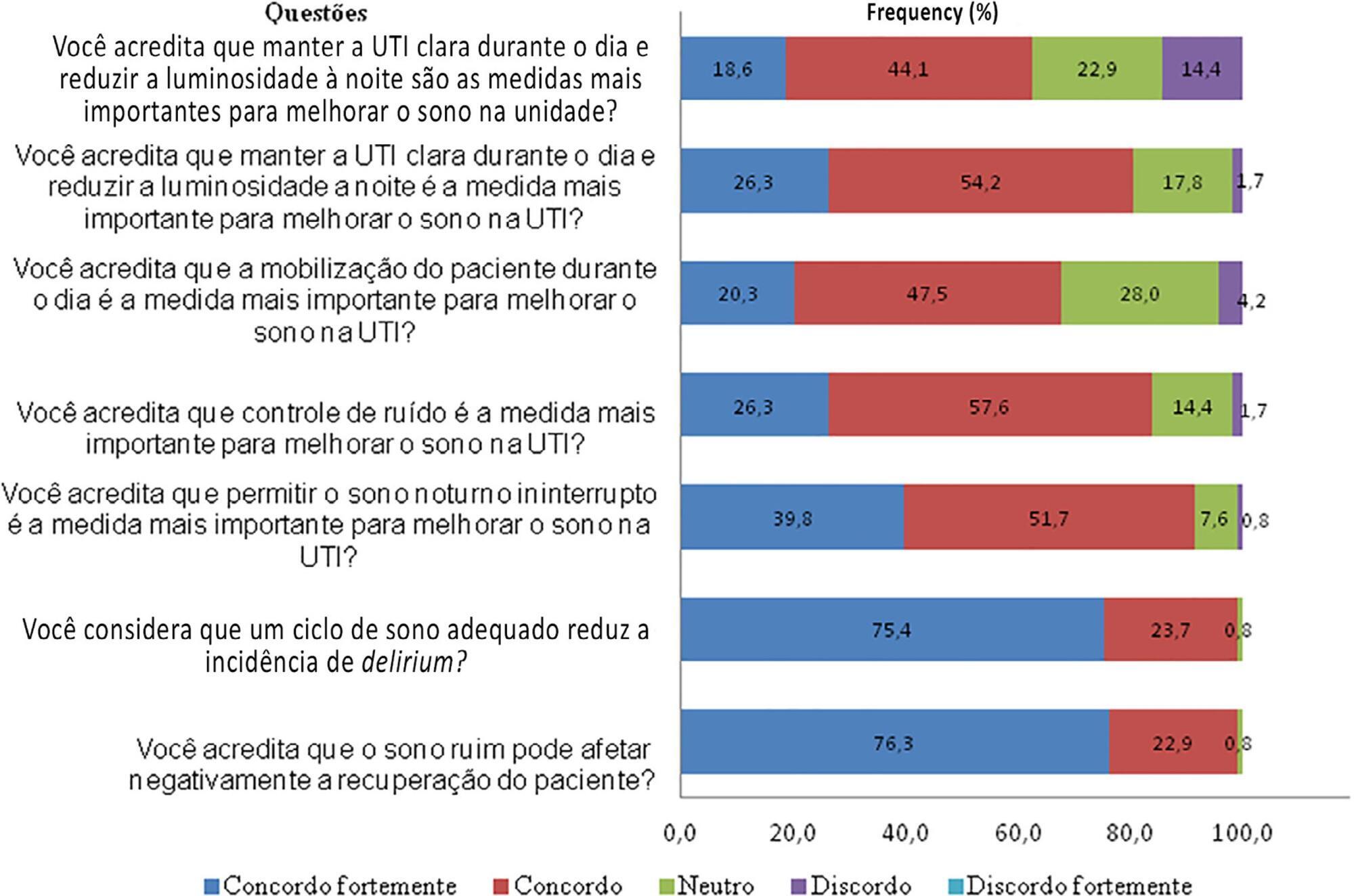
A total of 118 questionnaires were evaluated. The Southeast region of the country was the most represented (50 questionnaires, 42.4%). The majority of units had a clinical-surgical profile (93 questionnaires; 78.8%), and 26 had a continuous visitation policy (22.0%). Only 18 intensive care units (15.3%) reported having protocols for promoting sleep. The most cited measure for sleep promotion was reducing light during the night (95 questionnaires; 80.5%), which was more often performed in private intensive care units. Almost all of the responders (99%) believed that poor-quality sleep has a negative impact on patient recovery.
The responses to this Brazilian survey revealed that few intensive care units had a program for promoting sleep, although almost all participants recognized the importance of sleep in patient recovery.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):268-276
DOI 10.5935/0103-507X.20200043
To conduct a national survey of intensive care professionals to identify the practices for promoting sleep in adult intensive care units in Brazil and describe the professionals’ perceptions of the importance of sleep for patients.
An electronic questionnaire was distributed by the clinical research cooperation network of the Associação de Medicina Intensiva Brasileira and by the Brazilian Research in Intensive Care Network to physicians and nurses registered with the association. The questionnaire evaluated the profile of the respondents, the profile of their intensive care units, whether protocols for promoting sleep were present, the pharmacological and nonpharmacological measures typically employed in the unit, and the professionals’ perceptions regarding sleep in critically ill patients.
A total of 118 questionnaires were evaluated. The Southeast region of the country was the most represented (50 questionnaires, 42.4%). The majority of units had a clinical-surgical profile (93 questionnaires; 78.8%), and 26 had a continuous visitation policy (22.0%). Only 18 intensive care units (15.3%) reported having protocols for promoting sleep. The most cited measure for sleep promotion was reducing light during the night (95 questionnaires; 80.5%), which was more often performed in private intensive care units. Almost all of the responders (99%) believed that poor-quality sleep has a negative impact on patient recovery.
The responses to this Brazilian survey revealed that few intensive care units had a program for promoting sleep, although almost all participants recognized the importance of sleep in patient recovery.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):284-294
DOI 10.5935/0103-507X.20200045
To identify the relationship of patient-ventilator asynchrony with the level of sedation and hemogasometric and clinical results.
This was a prospective study of 122 patients admitted to the intensive care unit who underwent > 24 hours of invasive mechanical ventilation with inspiratory effort. In the first 7 days of ventilation, patient-ventilator asynchrony was evaluated daily for 30 minutes. Severe patient-ventilator asynchrony was defined as an asynchrony index > 10%.
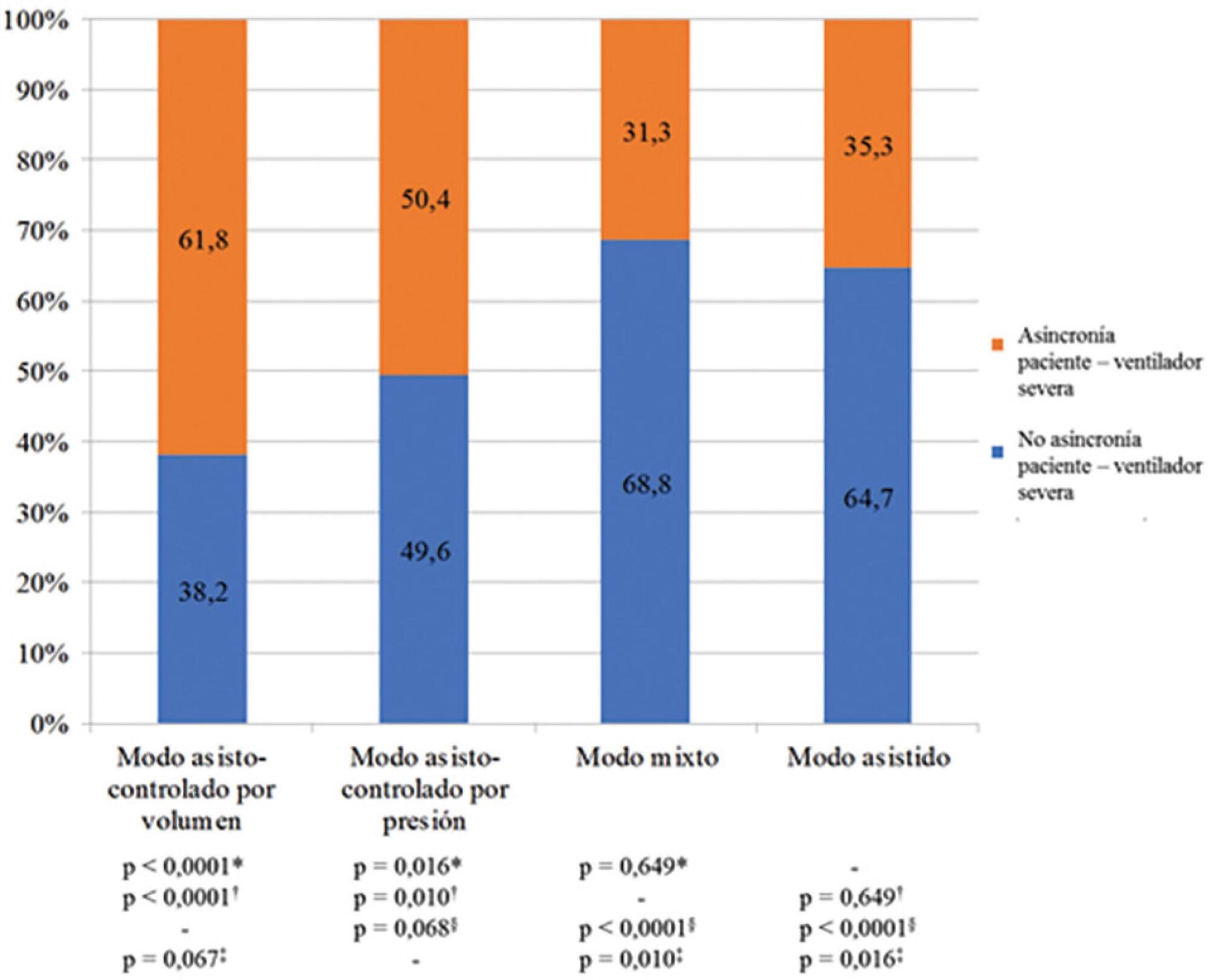
A total of 339,652 respiratory cycles were evaluated in 504 observations. The mean asynchrony index was 37.8% (standard deviation 14.1 - 61.5%). The prevalence of severe patient-ventilator asynchrony was 46.6%. The most frequent patient-ventilator asynchronies were ineffective trigger (13.3%), autotrigger (15.3%), insufficient flow (13.5%), and delayed cycling (13.7%). Severe patient-ventilator asynchrony was related to the level of sedation (ineffective trigger: p = 0.020; insufficient flow: p = 0.016; premature cycling: p = 0.023) and the use of midazolam (p = 0.020). Severe patient-ventilator asynchrony was also associated with hemogasometric changes. The persistence of severe patient-ventilator asynchrony was an independent risk factor for failure of the spontaneous breathing test, ventilation time, ventilator-associated pneumonia, organ dysfunction, mortality in the intensive care unit, and length of stay in the intensive care unit.
Patient-ventilator asynchrony is a frequent disorder in critically ill patients with inspiratory effort. The patient’s interaction with the ventilator should be optimized to improve hemogasometric parameters and clinical results. Further studies are required to confirm these results.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):284-294
DOI 10.5935/0103-507X.20200045
To identify the relationship of patient-ventilator asynchrony with the level of sedation and hemogasometric and clinical results.
This was a prospective study of 122 patients admitted to the intensive care unit who underwent > 24 hours of invasive mechanical ventilation with inspiratory effort. In the first 7 days of ventilation, patient-ventilator asynchrony was evaluated daily for 30 minutes. Severe patient-ventilator asynchrony was defined as an asynchrony index > 10%.
A total of 339,652 respiratory cycles were evaluated in 504 observations. The mean asynchrony index was 37.8% (standard deviation 14.1 - 61.5%). The prevalence of severe patient-ventilator asynchrony was 46.6%. The most frequent patient-ventilator asynchronies were ineffective trigger (13.3%), autotrigger (15.3%), insufficient flow (13.5%), and delayed cycling (13.7%). Severe patient-ventilator asynchrony was related to the level of sedation (ineffective trigger: p = 0.020; insufficient flow: p = 0.016; premature cycling: p = 0.023) and the use of midazolam (p = 0.020). Severe patient-ventilator asynchrony was also associated with hemogasometric changes. The persistence of severe patient-ventilator asynchrony was an independent risk factor for failure of the spontaneous breathing test, ventilation time, ventilator-associated pneumonia, organ dysfunction, mortality in the intensive care unit, and length of stay in the intensive care unit.
Patient-ventilator asynchrony is a frequent disorder in critically ill patients with inspiratory effort. The patient’s interaction with the ventilator should be optimized to improve hemogasometric parameters and clinical results. Further studies are required to confirm these results.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):301-307
DOI 10.5935/0103-507X.20200047
To evaluate the hypothesis that the Modified Early Warning Score (MEWS) at the time of intensive care unit discharge is associated with readmission and to identify the MEWS that most reliably predicts intensive care unit readmission within 48 hours of discharge.
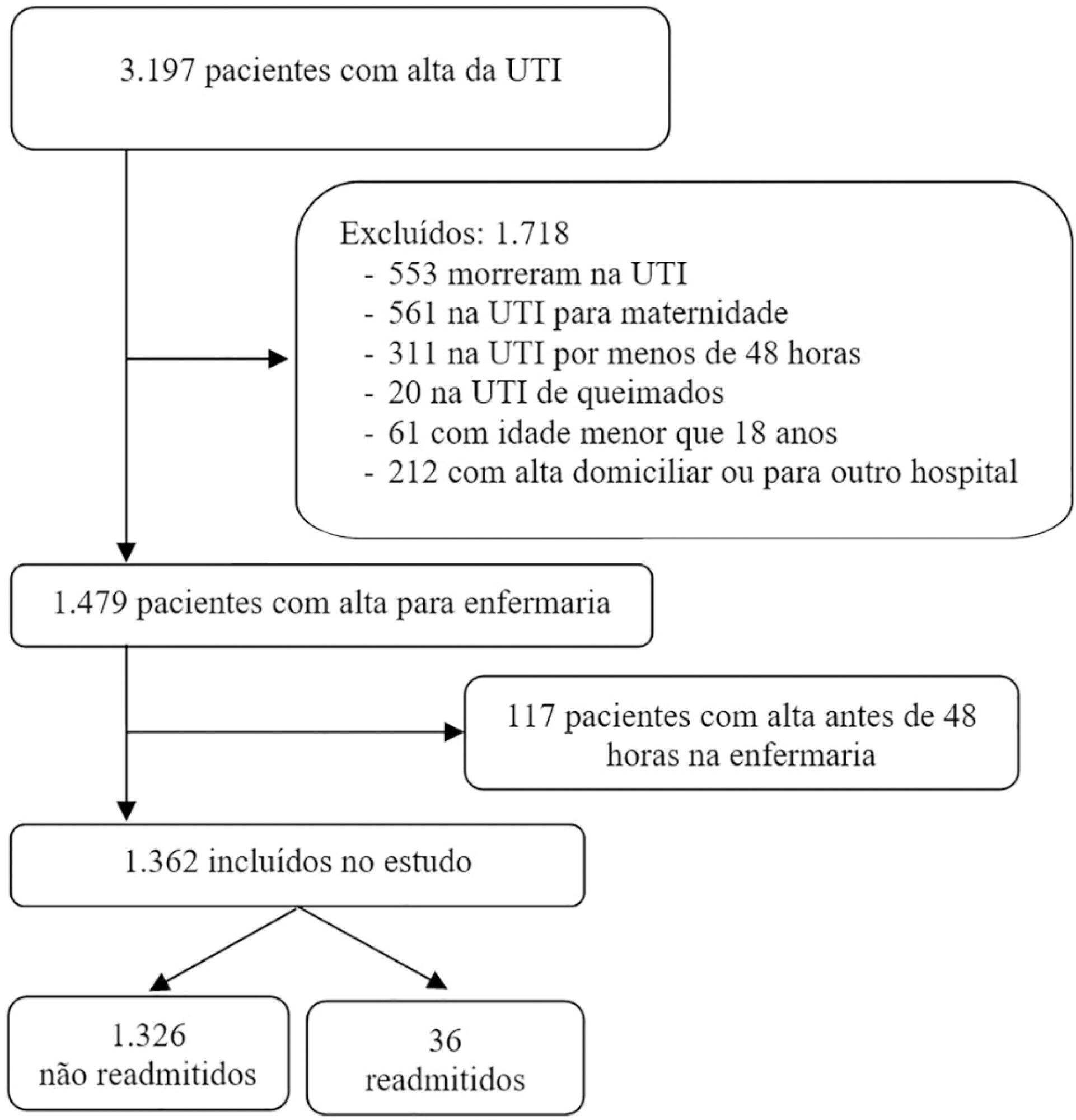
This was a retrospective observational study of the MEWSs of discharged patients from the intensive care unit. We compared the demographics, severity scores, critical illness characteristics, and MEWSs of readmitted and non-readmitted patients, identified factors associated with readmission in a logistic regression model, constructed a Receiver Operating Characteristic (ROC) curve of the MEWS in predicting the probability of readmission, and presented the optimum criterion with the highest sensitivity and specificity.
The readmission rate was 2.6%, and the MEWS was a significant predictor of readmission, along with intensive care unit length of stay > 10 days and tracheostomy. The ROC curve of the MEWS in predicting the readmission probability had an AUC of 0.82, and a MEWS > 6 carried a sensitivity of 0.78 (95%CI 0.66 - 0.9) and specificity of 0.9 (95%CI 0.87 - 0.93).
The MEWS is associated with intensive care unit readmission, and a score > 6 has excellent accuracy as a prognostic predictor.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):301-307
DOI 10.5935/0103-507X.20200047
To evaluate the hypothesis that the Modified Early Warning Score (MEWS) at the time of intensive care unit discharge is associated with readmission and to identify the MEWS that most reliably predicts intensive care unit readmission within 48 hours of discharge.
This was a retrospective observational study of the MEWSs of discharged patients from the intensive care unit. We compared the demographics, severity scores, critical illness characteristics, and MEWSs of readmitted and non-readmitted patients, identified factors associated with readmission in a logistic regression model, constructed a Receiver Operating Characteristic (ROC) curve of the MEWS in predicting the probability of readmission, and presented the optimum criterion with the highest sensitivity and specificity.
The readmission rate was 2.6%, and the MEWS was a significant predictor of readmission, along with intensive care unit length of stay > 10 days and tracheostomy. The ROC curve of the MEWS in predicting the readmission probability had an AUC of 0.82, and a MEWS > 6 carried a sensitivity of 0.78 (95%CI 0.66 - 0.9) and specificity of 0.9 (95%CI 0.87 - 0.93).
The MEWS is associated with intensive care unit readmission, and a score > 6 has excellent accuracy as a prognostic predictor.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):308-311
DOI 10.5935/0103-507X.20200033
The disease pandemic caused by the novel coronavirus has triggered significant changes in the medical decision-making process relating to critically ill patients. Admissions to intensive care units have suddenly increased, but many of these patients do not present with clinical manifestations related to the viral infection but rather exacerbation of preexisting diseases. In this context, we must prevent intuitive decision-making and insecurity from leading us to exhaust the available critical-care beds before they are truly necessary, while still recognizing the importance of rapid decision-making in emergency situations. One of the best ways to achieve this goal may be by practicing metacognition and establishing ways for regular feedback to be provided to professionals engaged in inherently rapid decision-making processes.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
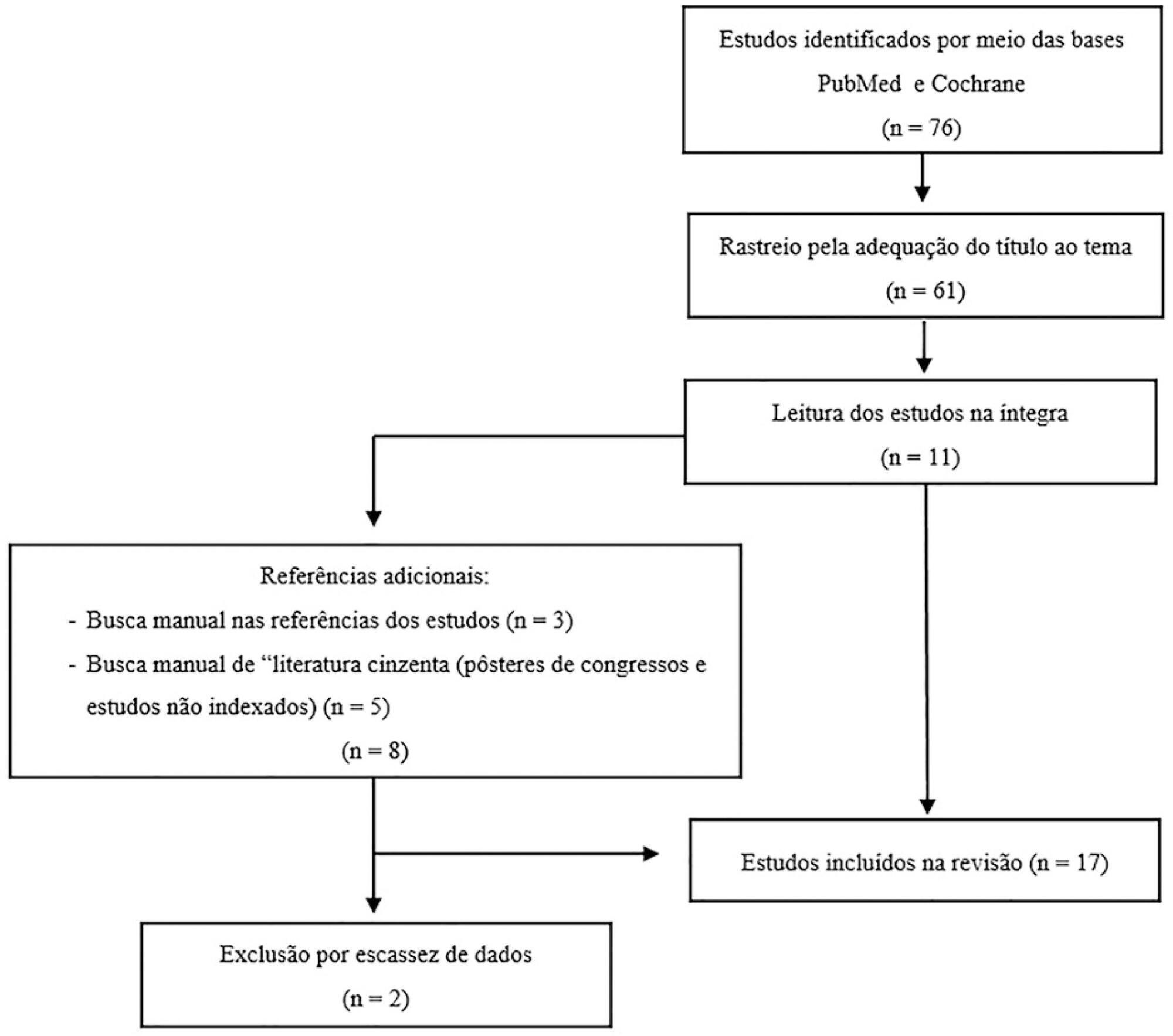
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 - 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 - 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Abstract
Rev Bras Ter Intensiva. 2020;32(2):312-318
DOI 10.5935/0103-507X.20200048
Among the potential complications of extracorporeal membrane oxygenation, neurological dysfunctions, including brain death, are not negligible. In Brazil, the diagnostic process of brain death is regulated by Federal Council of Medicine resolution 2,173 of 2017. Diagnostic tests for brain death include the apnea test, which assesses the presence of a ventilatory response to hypercapnic stimulus. However, gas exchange, including carbon dioxide removal, is maintained under extracorporeal membrane oxygenation, making the test challenging. In addition to the fact that the aforementioned resolution does not consider the specificities of the diagnostic process under extracorporeal membrane oxygenation, studies on the subject are scarce. This review aims to identify case studies (and/or case series) published in the PubMed® and Cochrane databases describing the process of brain death diagnosis. A total of 17 publications (2011 - 2019) were identified. The practical strategies described were to provide pretest supplemental oxygenation via mechanical ventilation and extracorporeal membrane oxygenation (fraction of inspired oxygen = 1.0) and, at the beginning of the test, titrate the sweep flow (0.5 - 1.0L/minute) to minimize carbon dioxide removal. It is also recommended to increase blood flow and/or sweep flow in the presence of hypoxemia and/or hypotension, which may be combined with fluid infusion and/or the escalation of inotropic/vasoactive drugs. If the partial pressure of carbon dioxide threshold is not reached, repeating the test under supplementation of carbon dioxide exogenous to the circuit is an alternative. Last, in cases of venoarterial extracorporeal membrane oxygenation, to measure gas variation and exclude differential hypoxia, blood samples of the native and extracorporeal (post-oxygenator) circulations are recommended.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
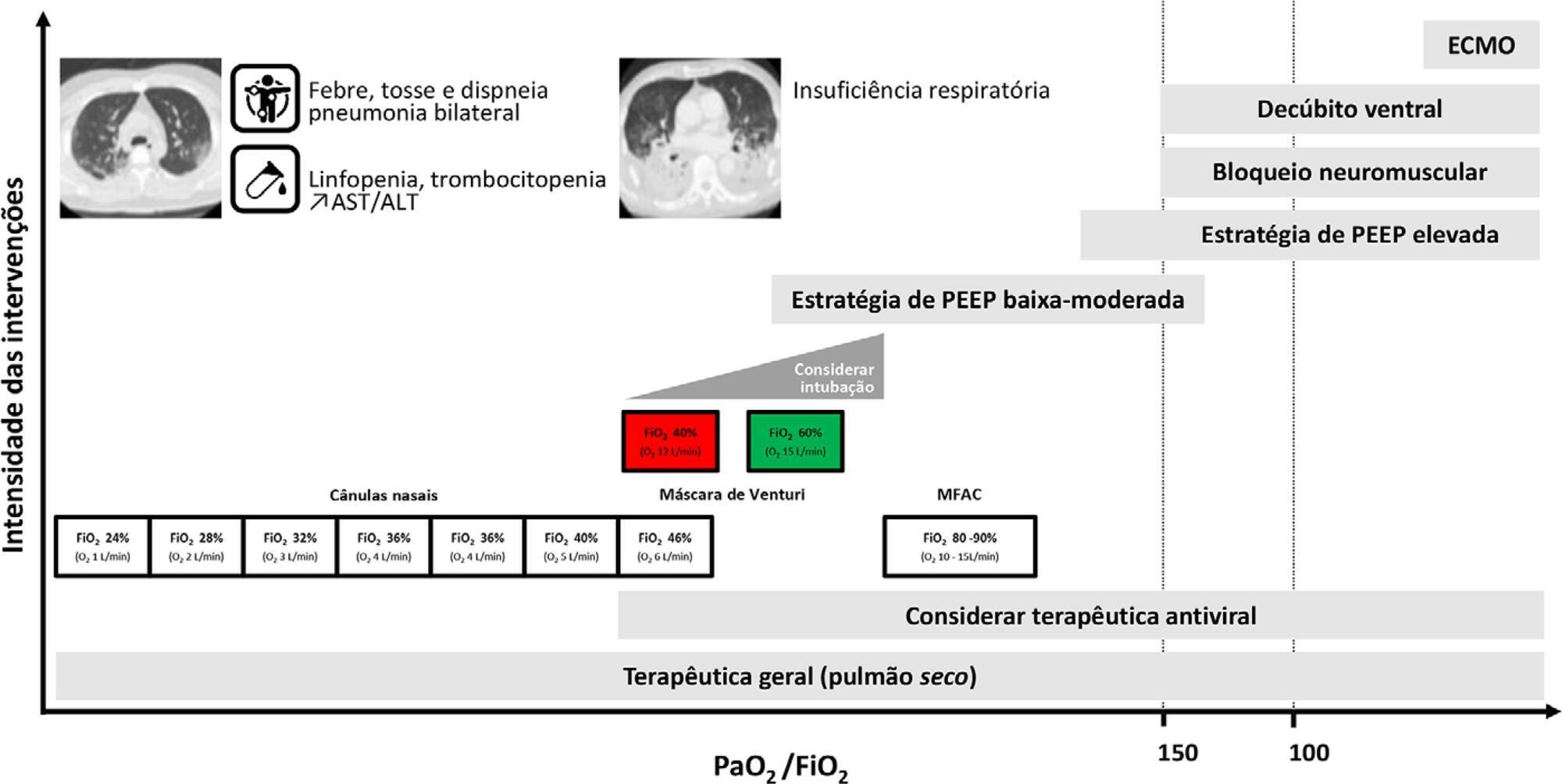
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):2-10
DOI 10.5935/0103-507X.20200002
Current COVID-19 epidemics was declared on December 31, 2019 at the Wuhan city seafood market, rapidly spreading throughout China, and later reaching several countries (mainly South Korea, Japan, Italy and Iran) and, since March 1, reaching Portugal. Most of the infected patients present with mild symptoms, not requiring hospitalization. Among those admitted to the hospital, 6% to 10% require admission to the intensive care unit. These recommendations are aimed to support the organization of intensive care services to respond COVID-19, providing optimized care to the patient and protection for healthcare professionals.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
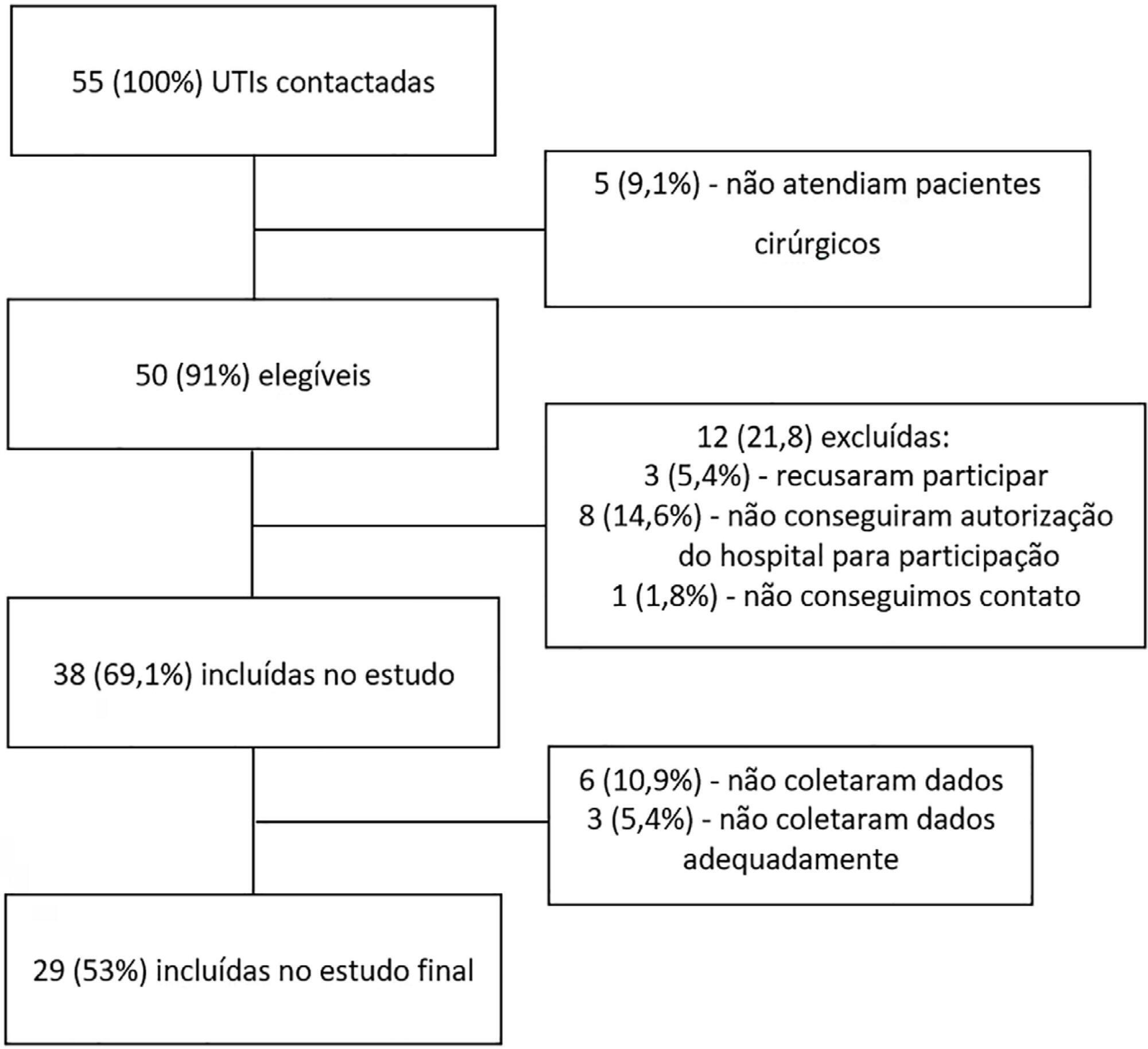
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):17-27
DOI 10.5935/0103-507X.20200005
To define the epidemiological profile and the main determinants of morbidity and mortality in noncardiac high surgical risk patients in Brazil.
This was a prospective, observational and multicenter study. All noncardiac surgical patients admitted to intensive care units, i.e., those considered high risk, within a 1-month period were evaluated and monitored daily for a maximum of 7 days in the intensive care unit to determine complications. The 28-day postoperative, intensive care unit and hospital mortality rates were evaluated.
Twenty-nine intensive care units participated in the study. Surgeries were performed in 25,500 patients, of whom 904 (3.5%) were high-risk (95% confidence interval - 95%CI 3.3% - 3.8%) and were included in the study. Of the participating patients, 48.3% were from private intensive care units, and 51.7% were from public intensive care units. The length of stay in the intensive care unit was 2.0 (1.0 - 4.0) days, and the length of hospital stay was 9.5 (5.4 - 18.6) days. The complication rate was 29.9% (95%CI 26.4 - 33.7), and the 28-day postoperative mortality rate was 9.6% (95%CI 7.4 - 12.1). The independent risk factors for complications were the Simplified Acute Physiology Score 3 (SAPS 3; odds ratio - OR = 1.02; 95%CI 1.01 - 1.03) and Sequential Organ Failure Assessment Score (SOFA) on admission to the intensive care unit (OR = 1.17; 95%CI 1.09 - 1.25), surgical time (OR = 1.001, 95%CI 1.000 - 1.002) and emergency surgeries (OR = 1.93, 95%CI, 1.10 - 3.38). In addition, there were associations with 28-day mortality (OR = 1.032; 95%CI 1.011 - 1.052), SAPS 3 (OR = 1.041; 95%CI 1.107 - 1.279), SOFA (OR = 1.175, 95%CI 1.069 - 1.292) and emergency surgeries (OR = 2.509; 95%CI 1.040 - 6.051).
Higher prognostic scores, elderly patients, longer surgical times and emergency surgeries were strongly associated with higher 28-day mortality and more complications during the intensive care unit stay.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV - pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
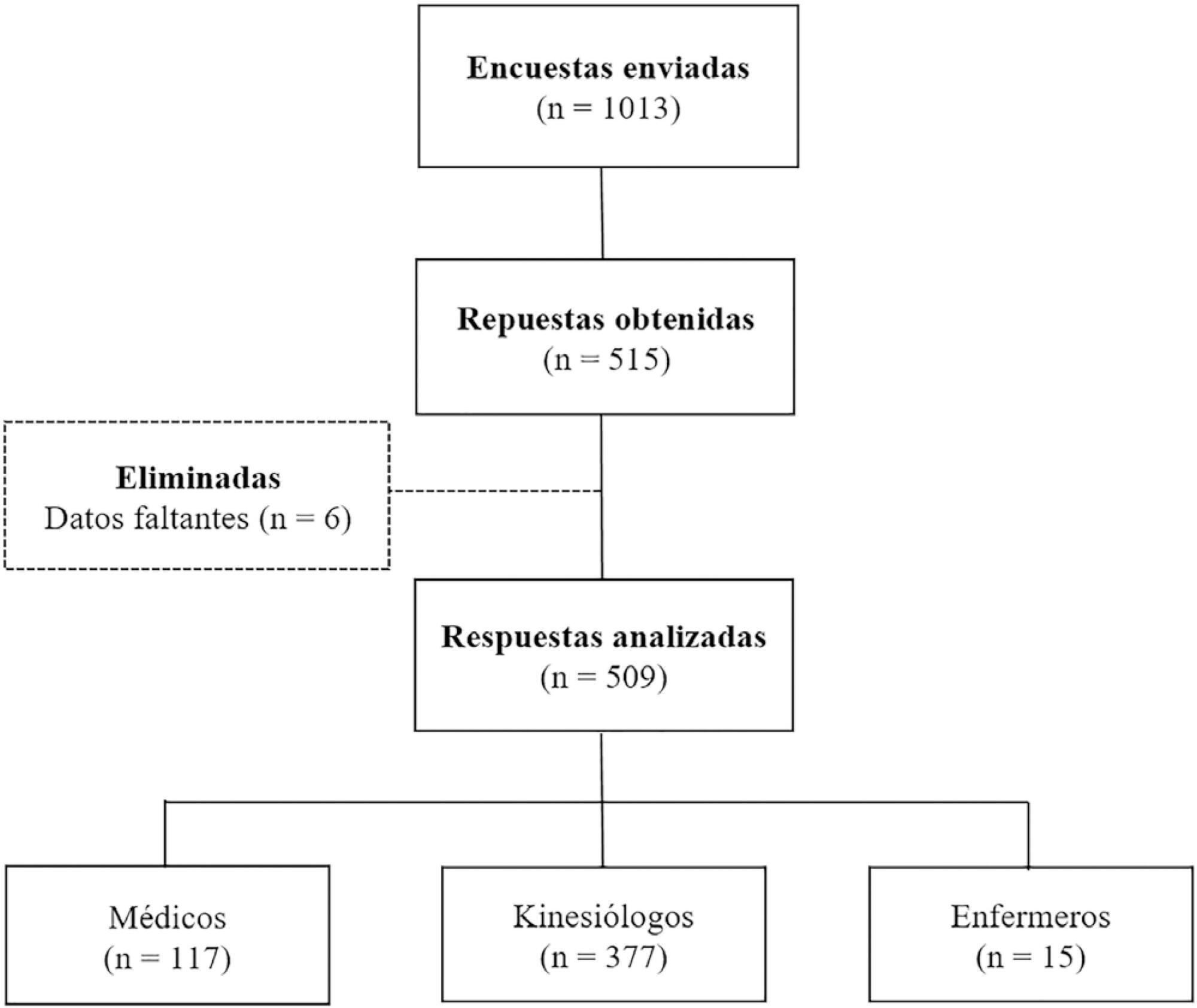
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.
Abstract
Rev Bras Ter Intensiva. 2020;32(1):81-91
DOI 10.5935/0103-507X.20200013
To identify common practices related to the use and titration of pressure-support ventilation (PC-CSV - pressure control-continuous spontaneous ventilation) in patients under mechanical ventilation and to analyze diagnostic criteria for over-assistance and under-assistance. The secondary objective was to compare the responses provided by physician, physiotherapists and nurses related to diagnostic criteria for over-assistance and under-assistance.
An online survey was conducted using the Survey Monkey tool. Physicians, nurses and physiotherapists from Argentina with access to PC-CSV in their usual clinical practice were included.
A total of 509 surveys were collected from October to December 2018. Of these, 74.1% were completed by physiotherapists. A total of 77.6% reported using PC-CSV to initiate the partial ventilatory support phase, and 43.8% of respondents select inspiratory pressure support level based on tidal volume. The main objective for selecting positive end-expiratory pressure (PEEP) level was to decrease the work of breathing. High tidal volume was the primary variable for detecting over-assistance, while the use of accessory respiratory muscles was the most commonly chosen for under-assistance. Discrepancies were observed between physicians and physiotherapists in relation to the diagnostic criteria for over-assistance.
The most commonly used mode to initiate the partial ventilatory support phase was PC-CSV. The most frequently selected variable to guide the titration of inspiratory pressure support level was tidal volume, and the main objective of PEEP was to decrease the work of breathing. Over-assistance was detected primarily by high tidal volume, while under-assistance by accessory respiratory muscles activation. Discrepancies were observed among professions in relation to the diagnostic criteria for over-assistance, but not for under-assistance.